
The Value of Indocyanine Green Image-Guided Surgery in Patients with Primary Liver Tumors and Liver Metastases

 , , , , ,
, , , , ,
Abstract
:1. Background
2. Materials and Methods
2.1. Study Design and Population
2.2. Ethical Approval
2.3. Procedure
2.4. Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Patients Characteristics
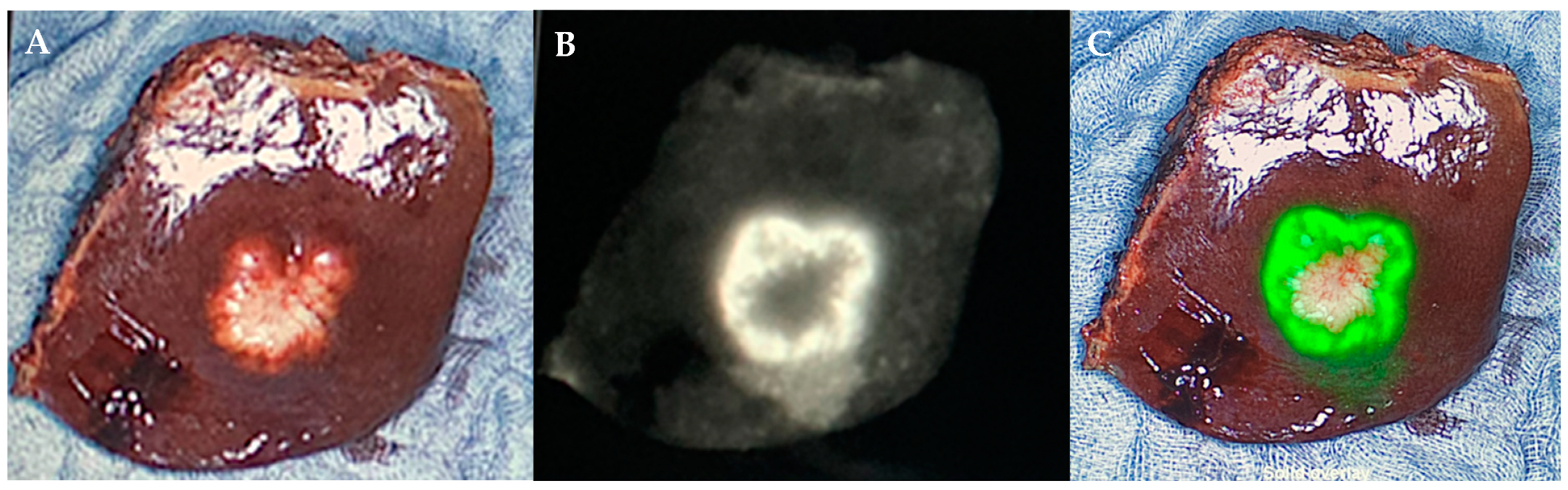
3.2. Intraoperative NIRF ICG Visualization
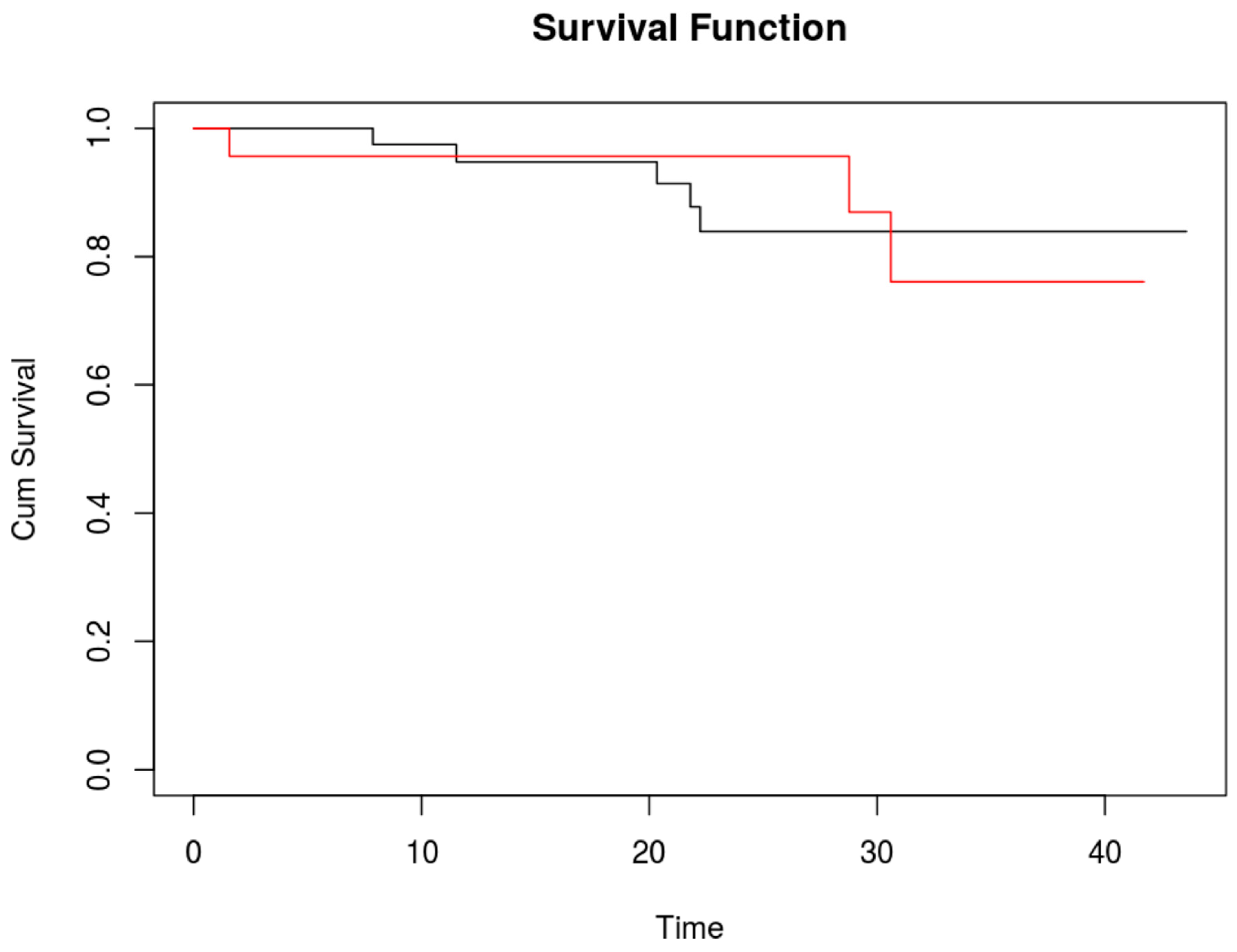
3.3. Survival
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ito, K.; Govindarajan, A.; Ito, H.; Fong, Y. Surgical treatment of hepatic colorectal metastasis: Evolving role in the setting of improving systemic therapies and ablative treatments in the 21st century. Cancer J. 2010, 16, 103–110. [Google Scholar] [CrossRef]
- Pulitanò, C.; Federico, C.; Luca, A.; Martin, B.; Rowan, W.P.; Gianfranco, F.; Stephen, J.W.; O James, G. What defines ‘cure’ after liver resection for colorectal metastases? Results after 10 years of follow-uHPB (Oxford). HPB 2010, 12, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Nikfarjam, M.; Shereef, S.; Kimchi, E.T.; Gusani, N.J.; Jiang, Y.; Avella, D.M.; Mahraj, R.P.; Staveley-O’carroll, K.F. Survival outcomes of patients with colorectal liver metastases following hepatic resection or ablation in the era of effective chemotherapy. Ann. Surg. Oncol. 2009, 16, 1860–1867. [Google Scholar] [CrossRef] [PubMed]
- Van der Pool, A.E.M.; Damhuis, R.A.; Ijzermans, J.N.M.; de Wilt, J.H.W.; Eggermont, A.M.M.; Kranse, R.; Verhoef, C. in incidence, treatment and survival of patients with stage IV colorectal cancer: A population-based series. Color. Dis. 2012, 14, 56–61. [Google Scholar] [CrossRef]
- Leung, U.; Gönen, M.; Allen, P.J.; Kingham, T.P.; DeMatteo, R.P.; Jarnagin, W.R.; D’angelica, M.I. Colorectal Cancer Liver Metastases and Concurrent Extrahepatic Disease Treated with Resection. Ann. Surg. 2017, 265, 158–165. [Google Scholar] [CrossRef] [PubMed]
- Rees, M.; Tekkis, P.P.; Welsh, F.K.; O’rourke, T.; John, T.G. Evaluation of long-term survival after hepatic resection for metastatic colorectal cancer: A multifactorial model of 929 patients. Ann. Surg. 2008, 247, 125–135. [Google Scholar] [CrossRef]
- Schmoll, H.J.; Van Cutsem, E.; Stein, A.; Valentini, V.; Glimelius, B.; Haustermans, K.; Nordlinger, B.; van de Velde, C.J.; Balmana, J.; Regula, J.; et al. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. a personalized approach to clinical decision making. Ann. Oncol. 2012, 23, 2479–2516. [Google Scholar] [CrossRef]
- Shaffer, E.; Hundal, R.S. Gallbladder cancer: Epidemiology and outcome. Clin. Epidemiol. 2014, 6, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Duffy, A.; Capanu, M.; Abou-Alfa, G.; Huitzil, D.; Jarnagin, W.; Fong, Y.; D’Angelica, M.; DeMatteo, R.; Blumgart, L.; O’Reilly, E. Gallbladder cancer (GBC): 10-year experience at Memorial Sloan-Kettering Cancer Centre (MSKCC). J. Surg. Oncol. 2008, 98, 485–489. [Google Scholar] [CrossRef]
- Bedikian, A.Y. Metastatic uveal melanoma therapy: Current options. Int. Ophthalmol. Clin. 2006, 46, 151–166. [Google Scholar] [CrossRef]
- Spagnolo, F.; Caltabiano, G.; Queirolo, P. Uveal melanoma. Cancer Treat. Rev. 2012, 38, 549–553. [Google Scholar] [CrossRef] [PubMed]
- Becker, J.C.; Terheyden, P.; Kämpgen, E.; Wagner, S.; Neumann, C.J.; Schadendorf, D.; Steinmann, A.; Wittenberg, G.; Lieb, W.E.; Bröcker, E.-B. Treatment of disseminated ocular melanoma with sequential fotemustine, interferon alpha, and interleukin 2. Br. J. Cancer 2002, 87, 840–845. [Google Scholar] [CrossRef] [PubMed]
- Xiong, L.; Gazyakan, E.; Yang, W.; Engel, H.; Hünerbein, M.; Kneser, U.; Hirche, C. Indocyanine green fluorescence-guided sentinel node biopsy: A meta-analysis on detection rate and diagnostic performance. Eur. J. Surg. Oncol. 2014, 40, 843–849. [Google Scholar] [CrossRef]
- Soltesz, E.G.; Kim, S.; Kim, S.-W.; Laurence, R.G.; De Grand, A.M.; Parungo, C.P.; Cohn, L.H.; Bawendi, M.G.; Frangioni, J.V. Sentinel lymph node mapping of the gastrointestinal tract by using invisible light. Ann. Surg. Oncol. 2006, 13, 386–396. [Google Scholar] [CrossRef] [PubMed]
- Verbeek, F.P.R.; Troyan, S.L.; Mieog, J.S.D.; Liefers, G.-J.; Moffitt, L.A.; Rosenberg, M.; Hirshfield-Bartek, J.; Gioux, S.; Van De Velde, C.J.H.; Vahrmeijer, A.L.; et al. Near-infrared fluorescence sentinel lymph node mapping in breast cancer: A multicenter experience. Breast Cancer Res. Treat. 2014, 143, 333–342. [Google Scholar] [CrossRef]
- Ishizawa, T.; Saiura, A.; Kokudo, N. Clinical application of indocyanine green-fluorescence imaging during hepatectomy. Hepatobiliary Surg. Nutr. 2016, 5, 322–328. [Google Scholar] [CrossRef]
- Lobbes, L.A.; Berns, S.; Warschkow, R.; Schmidt, L.R.; Schineis, C.; Strobel, R.M.; Lauscher, J.C.; Beyer, K.; Weixler, B. Perfusion Visualization during Ileal J-Pouch Formation-A Proposal for the Standardization of Intraoperative Imaging with Indocyanine Green Near-Infrared Fluorescence and a Postoperative Follow-Up in IBD Surgery. Life 2022, 12, 668. [Google Scholar] [CrossRef]
- Weixler, B.; Rickenbacher, A.; Raptis, D.A.; Viehl, C.T.; Guller, U.; Rueff, J.; Zettl, A.; Zuber, M. Sentinel Lymph Node Mapping with Isosulfan Blue or Indocyanine Green in Colon Cancer Shows Comparable Results and Identifies Patients with Decreased Survival: A Prospective Single-Center Trial. World J. Surg. 2017, 41, 2378–2386. [Google Scholar] [CrossRef]
- Landsman, M.L.; Kwant, G.; Mook, G.A.; Zijlstra, W.G. Light-absorbing properties, stability, and spectral stabilization of indocyanine green. J. Appl. Physiol. 1976, 40, 575–583. [Google Scholar] [CrossRef]
- Boogerd, L.S.F.; Handgraaf, H.J.M.; Lam, H.-D.; Huurman, V.A.L.; Farina-Sarasqueta, A.; Frangioni, J.V.; van de Velde, C.J.H.; Braat, A.E.; Vahrmeijer, A.L. Laparoscopic detection and resection of occult liver tumors of multiple cancer types using real-time near-infrared fluorescence guidance. Surg. Endosc. 2017, 31, 952–961. [Google Scholar] [CrossRef]
- Kokudo, N.; Ishizawa, T. Clinical application of fluorescence imaging of liver cancer using indocyanine green. Liver Cancer 2012, 1, 15–21. [Google Scholar] [CrossRef]
- Tummers, Q.R.; Verbeek, F.P.; Prevoo, H.A.; Braat, A.E.; Baeten, C.I.; Frangioni, J.V.; Vahrmeijer, A.L. First experience on laparoscopic near-infrared fluorescence imaging of hepatic uveal melanoma metastases using indocyanine green. Surg. Innov. 2015, 22, 20–25. [Google Scholar] [CrossRef]
- De Graaf, W.; Häusler, S.; Heger, M.; Van Ginhoven, T.M.; Van Cappellen, G.; Bennink, R.J.; A Kullak-Ublick, G.; Hesselmann, R.; Van Gulik, T.M.; Stieger, B. Transporters involved in the hepatic uptake of (99 m)Tc-mebrofenin and indocyanine green. J. Hepatol. 2011, 54, 738–745. [Google Scholar] [CrossRef]
- van der Vorst, J.R.; Schaafsma, B.E.; Hutteman, M.; Verbeek, F.P.; Liefers, G.J.; Hartgrink, H.H.; Vahrmeijer, A.L. Near-infrared fluorescence-guided resection of colorectal liver metastases. Cancer 2013, 119, 3411–3418. [Google Scholar] [CrossRef] [PubMed]
- Gotoh, K.; Yamada, T.; Ishikawa, O.; Takahashi, H.; Eguchi, H.; Yano, M.; Imaoka, S. A novel image-guided surgery of hepatocellular carcinoma by indocyanine green fluorescence imaging navigation. J. Surg. Oncol. 2009, 100, 75–79. [Google Scholar] [CrossRef]
- Ishizawa, T.; Fukushima, N.; Shibahara, J.; Masuda, K.; Tamura, S.; Aoki, T.; Hasegawa, K.; Beck, Y.; Fukayama, M.; Kokudo, N. Real-time identification of liver cancers by using indocyanine green fluorescent imaging. Cancer 2009, 115, 2491–2504. [Google Scholar] [CrossRef]
- Margonis, G.A.; Sergentanis, T.N.; Ntanasis-Stathopoulos, I.; Andreatos, N.; Tzanninis, I.G.; Sasaki, K.; Weiss, M.J. Impact of Surgical Margin Width on Recurrence and Overall Survival Following R0 Hepatic Resection of Colorectal Metastases: A Systematic Review and Meta-analysis. Ann. Surg. 2018, 267, 1047–1055. [Google Scholar] [CrossRef]
- Cloud Graphical User Interface for R Statistics and eLearning Platform. 2017. Available online: www.rbiostatistics.com (accessed on 6 October 2022).
- Benedetti Cacciaguerra, A.; Görgec, B.; Cipriani, F.; Aghayan, D.; Borelli, G.; Aljaiuossi, A.; Abu Hilal, M. Risk Factors of Positive Resection Margin in Laparoscopic and Open Liver Surgery for Colorectal Liver Metastases: A New Perspective in the Perioperative Assessment: A European Multicenter Study. Ann. Surg. 2022, 275, e213–e221. [Google Scholar] [CrossRef] [PubMed]
- Achterberg, F.B.; Mulder, B.G.S.; Meijer, R.P.J.; Bonsing, B.A.; Hartgrink, H.H.; Mieog, J.S.D.; Zlitni, A.; Park, S.-M.; Sarasqueta, A.F.; Vahrmeijer, A.L.; et al. Real-time surgical margin assessment using ICG-fluorescence during laparoscopic and robot-assisted resections of colorectal liver metastases. Ann. Transl. Med. 2020, 8, 1448. [Google Scholar] [CrossRef]
- Handgraaf, H.; Boogerd, L.; Höppener, D.; Peloso, A.; Mulder, B.S.; Hoogstins, C.; Hartgrink, H.; van de Velde, C.; Mieog, J.; Swijnenburg, R.; et al. Long-term follow-up after near-infrared fluorescence-guided resection of colorectal liver metastases: A retrospective multicenter analysis. Eur. J. Surg. Oncol. 2017, 43, 1463–1471. [Google Scholar] [CrossRef] [PubMed]
- Ishizawa, T.; Masuda, K.; Urano, Y.; Kawaguchi, Y.; Satou, S.; Kaneko, J.; Hasegawa, K.; Shibahara, J.; Fukayama, M.; Tsuji, S.; et al. Mechanistic background and clinical applications of indocyanine green fluorescence imaging of hepatocellular carcinoma. Ann. Surg. Oncol. 2014, 21, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Tummers, Q.R.J.G.; Hoogstins, C.E.S.; Peters, A.A.W.; De Kroon, C.D.; Trimbos, J.B.M.Z.; Van De Velde, C.J.H.; Frangioni, J.V.; Vahrmeijer, A.L.; Gaarenstroom, K. The Value of Intraoperative Near-Infrared Fluorescence Imaging Based on Enhanced Permeability and Retention of Indocyanine Green: Feasibility and False-Positives in Ovarian Cancer. PLoS ONE 2015, 10, e0129766. [Google Scholar] [CrossRef] [PubMed]
- Liberale, G.; Bourgeois, P.; Larsimont, D.; Moreau, M.; Donckier, V.; Ishizawa, T. Indocyanine green fluorescence-guided surgery after IV injection in metastatic colorectal cancer: A systematic review. Eur. J. Surg. Oncol. 2017, 43, 1656–1667. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Patient Characteristics | n |
|---|---|
| Age | 65.5 years (IQR 58.7–73.9) |
| Sex | |
| Female | 27 (40.9%) |
| Male | 39 (59.1%) |
| Type of surgery | |
| Open | 48 (72.7%) |
| Laparoscopic | 18 (27.3%) |
| Type of operation | |
| Extended right | 11 |
| Extended left | 6 |
| Right hemihepatectomy | 7 |
| Left hemihepatectomy | 2 |
| Multiple segmentectomy | 7 |
| Segmentectomy | 13 |
| Wedge | 20 |
| Tumor type of metastases | |
| Rectal cancer | 28 |
| Colon cancer | 20 |
| Hepatocellular carcinoma | 5 |
| Uveal melanoma | 5 |
| Cholangiocarcinoma | 4 |
| Neuroendocrine tumor | 2 |
| Parotid carcinoma | 1 |
| Ovarian carcinoma | 1 |
| Patients with additional ICG-positive lesions | 23 |
| Additional ICG-positive lesions: | |
| Malignant no | 14 (71%) |
| Malignant yes | 9 (29%) |
| Child–Pugh Score | |
| No cirrhosis | 64 |
| B | 2 |
| ASA Score | |
| 1 | 3 |
| 2 | 27 |
| 3 | 36 |
| BMI | 23.7 (IQR 21.2–26.5) |
| Length of hospital stay | 9 days (IQR 6–17 days) |
| INR preoperative | 1.01 (IQR 0.96–1.06) |
| INR 24 h postoperative | 1.31 (IQR 1.14–1.41) |
| INR at discharge | 1.08 (IQR 1.02–1.16) |
| Postoperative complications (Clavien–Dindo) | |
| 0 | 27 |
| 1 | 7 |
| 2 | 8 |
| 3a | 6 |
| 3b | 12 |
| 4a | 2 |
| 5 | 4 |
| ICG-Positive Spots at Resection Margin on Liver Specimen | Type of Resection | ||
|---|---|---|---|
| R0 | R1 | R2 | |
| No | 93.9% | 6.1% | 0% |
| Yes | 64.3% | 21.4% | 14.3% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weixler, B.; Lobbes, L.A.; Scheiner, L.; Lauscher, J.C.; Staubli, S.M.; Zuber, M.; Raptis, D.A. The Value of Indocyanine Green Image-Guided Surgery in Patients with Primary Liver Tumors and Liver Metastases. Life 2023, 13, 1290. https://doi.org/10.3390/life13061290
Weixler B, Lobbes LA, Scheiner L, Lauscher JC, Staubli SM, Zuber M, Raptis DA. The Value of Indocyanine Green Image-Guided Surgery in Patients with Primary Liver Tumors and Liver Metastases. Life. 2023; 13(6):1290. https://doi.org/10.3390/life13061290
Chicago/Turabian StyleWeixler, Benjamin, Leonard A. Lobbes, Luis Scheiner, Johannes C. Lauscher, Sebastian M. Staubli, Markus Zuber, and Dimitri A. Raptis. 2023. "The Value of Indocyanine Green Image-Guided Surgery in Patients with Primary Liver Tumors and Liver Metastases" Life 13, no. 6: 1290. https://doi.org/10.3390/life13061290