
Ageing People Living with HIV/AIDS, PLWHA; More Dental Challenges; the Romanian Dental Professional’s Point of View

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
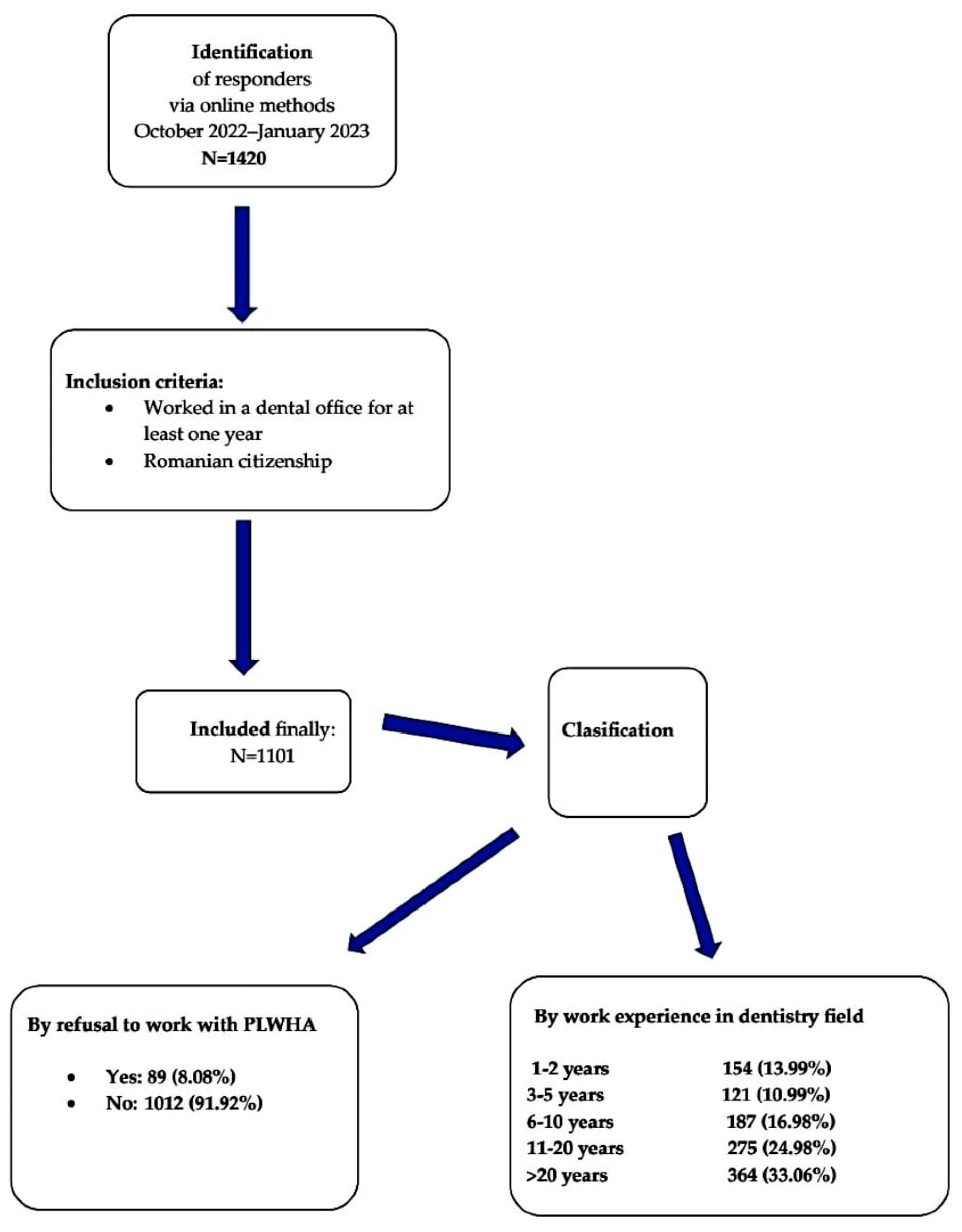
2.1. Study Design, Setting, and Participants
2.2. Survey Questionnaire and Data Collection
2.3. Ethical Approval
2.4. Statistical Analysis
3. Results
3.1. Genal Data of Responders
3.2. Attitudes towards, Knowledge about, Practice with, and Management of PLWHA
3.3. More Dental Challenges and Differences in Treating Aging PLWHA, According to Area of Provenience
3.4. Aging with HIV, More Dental Challenges, Fear of Working with PLWHA
4. Discussion
Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Abbreviations
| AIDS | acquired immunodeficiency syndrome |
| ARV | antiretroviral therapy |
| HAART | highly active anti-retroviral therapy |
| HIV | human immunodeficiency virus |
| HRQoL | health-related quality of life |
| OHRQoL | oral-health-related quality of life |
| PLHIV | people living with HIV |
| PLWHA | people living with HIV/AIDS |
References
- Global status of reported AIDS cases ranked across regions of the World Health Organization. Integration 1989, 60. Available online: https://pubmed.ncbi.nlm.nih.gov/12282145/ (accessed on 23 March 2023).
- Hersh, B.S.; Popovici, F.; Apetrei, R.C.; Zolotusca, L.; Beldescu, N.; Calomfirescu, A.; Jezek, Z.; Oxtoby, M.J.; Gromyko, A.; Heymann, D.L. Acquired immunodeficiency syndrome in Romania. Lancet 1991, 338, 645–649. [Google Scholar] [CrossRef]
- Manolescu, L.; Marinescu, P. Sex differences in HIV-1 viral load and absolute CD4 cell count in long term survivors HIV-1 infected patients from Giurgiu, Romania. Rom. Rev. Lab. Med. 2013, 21, 217–224. [Google Scholar] [CrossRef]
- Temereanca, A.; Ene, L.; Mehta, S.; Manolescu, L.; Duiculescu, D.; Ruta, S. Transmitted HIV drug resistance in treatment-naive Romanian patients. J. Med. Virol. 2013, 85, 1139–1147. [Google Scholar] [CrossRef]
- Marinescu, P.; Manolescu, L.S.C. Association of hepatitis B infection in patients with HIV Encephalopathy. Rom. Biotechnol. Lett. 2012, 17, 7817–7824. [Google Scholar]
- Manolescu, L.; Temereanca, A.; Diaconu, C.C.; Ruta, S. Correlation between resistance profile and immunosuppression in heavily treated HIV-1 infected Romanian patients. Rom. Biotechnol. Lett. 2011, 16, 6439–6449. [Google Scholar]
- Department for Monitoring and Evaluation of HIV/AIDS in Romania, National Institute of Infectious Diseases “Prof. Dr. Matei Balș”. Available online: https://www.cnlas.ro/index.php/date-statistice (accessed on 8 February 2023).
- Preda, M.; Manolescu, L.C.S. Romania, a Harbour of HIV-1 Subtype F1: Where Are We after 33 Years of HIV-1 Infection? Viruses 2022, 14, 2081. [Google Scholar] [CrossRef]
- McGettrick, P.; Barco, E.A.; Mallon, P.W.G. Ageing with HIV. Healthcare 2018, 6, 17. [Google Scholar] [CrossRef]
- So-Armah, K.; Benjamin, L.A.; Bloomfield, G.S.; Feinstein, M.J.; Hsue, P.; Njuguna, B.; Freiberg, M.S. HIV and cardiovascular disease. Lancet HIV 2020, 7, e279–e293. [Google Scholar] [CrossRef]
- Javadi, S.; Menias, C.O.; Karbasian, N.; Shaaban, A.; Shah, K.; Osman, A.; Jensen, C.T.; Lubner, M.G.; Gaballah, A.H.; Elsayes, K.M. HIV-related Malignancies and Mimics: Imaging Findings and Management. Radiographics 2018, 38, 2051–2068. [Google Scholar] [CrossRef]
- Winston, A.; Spudich, S. Cognitive disorders in people living with HIV. Lancet HIV 2020, 7, e504–e513. [Google Scholar] [CrossRef]
- Chisati, E.M.; Constantinou, D.; Lampiao, F. Management of Reduced Bone Mineral Density in HIV: Pharmacological Challenges and the Role of Exercise. Front. Physiol. 2018, 9, 1074. [Google Scholar] [CrossRef]
- Maina, E.K.; Adan, A.A.; Mureithi, H.; Muriuki, J.; Lwembe, R.M. A Review of Current Strategies Towards the Elimination of Latent HIV-1 and Subsequent HIV-1 Cure. Curr. HIV Res. 2021, 19, 14–26. [Google Scholar] [CrossRef]
- Campo-Trapero, J.; Cano-Sánchez, J.; Del Romero-Guerrero, J.; Moreno-López, L.A.; Cerero-Lapiedra, R.; Bascones-Martínez, A. Dental management of patients with human immunodeficiency virus. Quintessence Int. 2003, 34, 515–525. [Google Scholar]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Mehta, V.; Fiorillo, L.; Badnjević, A.; Cervino, G.; Cicciù, M. Gaucher: A Systematic Review on Oral and Radiological Aspects. Medicina 2023, 59, 670. [Google Scholar] [CrossRef]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Mehta, V.; Fiorillo, L.; Badnjević, A.; Cervino, G.; Cicciù, M. The Association between COVID-19 Related Anxiety, Stress, Depression, Temporomandibular Disorders, and Headaches from Childhood to Adulthood: A Systematic Review. Brain Sci. 2023, 13, 481. [Google Scholar] [CrossRef]
- Medar, C.; Cristache, C.M.; Mihut, T.; Marcov, E.C.; Furtunescu, F.L.; Burlibasa, M.; Burlibasa, L. Defensive dentistry from normal medical practice to safeguard from malpractice litigations. New rules in COVID-19 pandemic. Rom. J. Leg. Med. 2020, 28, 465–469. [Google Scholar] [CrossRef]
- Stetiu, A.A.; Stetiu, M.; Burlibasa, M.; Perieanu, V.S.; Tanase, G.; Marcov, N.; Andrei, O.C.; Costea, R.; Marcov, E.C.; Bodnar, D.C.; et al. FEM analysis of masticatory induced stresses over surrounding tissues of dental implant. Rom. Biotechnol. Lett. 2018, 24, 472–478. [Google Scholar] [CrossRef]
- Iacovou, E.; Vlastarakos, P.V.; Papacharalampous, G.; Kampessis, G.; Nikolopoulos, T.P. Diagnosis and treatment of HIV-associated manifestations in otolaryngology. Infect. Dis. Rep. 2012, 4, e9. [Google Scholar] [CrossRef]
- Beekmann, S.E.; Henderson, D.K. Managing occupational risks in the dental office: HIV and the dental professional. J. Am. Dent. Assoc. 1994, 125, 847–852. [Google Scholar] [CrossRef]
- Preda, M.; Dinu, R.S.; Prasacu, I.; Manolescu, L.S.C. SARS-CoV-2 Infection Anxiety, Knowledge and Attitudes in University Degree Pregnant Women from Romania—A Cross-Sectional Observational Survey in the First Two Pandemic Years. Vaccines 2023, 11, 35. [Google Scholar] [CrossRef]
- Pop-Tudose, M.E.; Popescu-Spineni, D.M.; Manolescu, L.S.C.; Radu, M.C.; Iancu, F.C.; Armean, S.M. Psychological Profile and Mood Disturbance of Women Who Gave Birth during the COVID-19 Pandemic in Romania. Midwifery 2022, 117, 103571. [Google Scholar] [CrossRef]
- Manolescu, L.S.C.; Zugravu, C.; Zaharia, C.N.; Dumitrescu, A.I.; Prasacu, I.; Radu, M.C.; Letiția, G.D.; Nita, I.; Cristache, C.M.; Gales, L.N. Barriers and Facilitators of Romanian HPV (Human Papillomavirus) Vaccination. Vaccines 2022, 10, 1722. [Google Scholar] [CrossRef]
- Otelea, M.R.; Zugravu, C.; Rascu, A.; Arghir, O.C.; Manolescu, L.S.C.; Mates, D. Coronasomnia in Employees without a Direct Contact with COVID-19 Infected Patients in Their Workplace. Healthcare 2022, 10, 1194. [Google Scholar] [CrossRef] [PubMed]
- Streinu-Cercel, A.; Ion, D.A.; Chivu, L.I.; Chivu, R.D. Lipodystrophy syndrome in HIV-infected patients. Clinical and diagnostic features. Rev. Med. Chir. Soc. Med. Nat. Iasi 2006, 110, 521–525. [Google Scholar] [PubMed]
- Niță, I.; Nițipir, C.; Toma, S.A.; Limbău, A.M.; Pîrvu, E.; Bădărău, A.I.; Suciu, I.; Suciu, G.; Manolescu, L.S.C. Correlation between Androgen Receptor Expression and Immunohistochemistry Type as Prognostic Factors in a Cohort of Breast Cancer Patients: Result from a Single-Center, Cross Sectional Study. Healthcare 2021, 9, 277. [Google Scholar] [CrossRef] [PubMed]
- Niță, I.; Nițipir, C.; Toma, A.; Limbău, A.M.; Pîrvu, E.; Bădărău, I.A.; Suciu, I.; Suciu, G.; Manolescu, L.S.C. Histological Aspects and Quantitative Assessment of Ki67 as Prognostic Factors in Breast Cancer Patients: Result from a Single-Center, Cross Sectional Study. Medicina 2020, 56, 600. [Google Scholar] [CrossRef]
- Vidya, K.M.; Rao, U.K.; Nittayananta, W.; Liu, H.; Owotade, F.J. Oral mycoses and other opportunistic infections in HIV: Therapy and emerging problems—A workshop report. Oral Dis. 2016, 22, 158–165. [Google Scholar] [CrossRef]
- Parish, C.; Siegel, K.; Pereyra, M.; Liguori, T.; Metsch, L. Barriers and facilitators to dental care among HIV-Infected adults. Spéc. Care Dent. 2015, 35, 294–302. [Google Scholar] [CrossRef]
- Serb, P.; Yeung, S. HIV infection and the dentist. 1. The presence of HIV in saliva and its implications to dental practice. Aust. Dent. J. 1994, 39, 67–72. [Google Scholar] [CrossRef]
- Marcu, E.-A.; Dinescu, S.-N.; Pădureanu, V.; Dumitrescu, F.; Diaconu, R. Perinatal Exposure to HIV Infection: The Experience of Craiova Regional Centre, Romania. Healthcare 2022, 10, 308. [Google Scholar] [CrossRef] [PubMed]
- Katwal, D.; Rimal, J.; Prajapati, K. Knowledge, Attitude and Practice of Dental Students Regarding Treatment of Patients with HIV or AIDS in Nepal. Kathmandu Univ. Med. J. 2019, 17, 190–194. [Google Scholar]
- Wakayama, B.; Garbin, C.A.S.; Garbin, A.J.S.; Saliba Junior, O.A.; Garbin, A.J.I. The representation of HIV/AIDS and hepatitis B in the dentistry context. J. Infect. Dev. Ctries. 2021, 15, 979–988. [Google Scholar] [CrossRef]
- Rungsiyanont, S.; Vacharotayangul, P.; Lam-Ubol, A.; Ananworanich, J.; Phanuphak, P.; Phanuphak, N. Perceived dental needs and attitudes toward dental treatments in HIV-infected Thais. AIDS Care 2012, 24, 1584–1590. [Google Scholar] [CrossRef] [PubMed]
- Shaghaghian, S.; Saranjam, E.; Homayooni, M. Oral health-related quality of life in patients infected with HIV, Iran: A cross-sectional study. BMC Oral Health 2021, 21, 308. [Google Scholar] [CrossRef]
- Hardie, J. Problems associated with providing dental care to patients with HIV-infected and AIDS patients. Oral Surg. Oral Med. Oral Pathol. 1992, 73, 231–235. [Google Scholar] [CrossRef]
- Kall, M.; Fresán, U.; Guy, D.; Brown, G.; Burgui, C.; Castilla, J.; Grecu, V.I.; Dumitrescu, F.; Delpech, V.; Lazarus, J.V. Quality of life in people living with HIV in Romania and Spain. BMC Infect. Dis. 2021, 21, 898. [Google Scholar] [CrossRef]
- Dhanya, R.S.; Hegde, V.; Anila, S.; Sam, G.; Khajuria, R.R.; Singh, R. Knowledge, attitude, and practice towards HIV patients among dentists. J. Int. Soc. Prev. Commun. Dent. 2017, 7, 148–153. [Google Scholar] [CrossRef]
- Moodley, R.; Naidoo, S.; Van Wyk, J. The prevalence of occupational health-related problems in dentistry: A review of the literature. J. Occup. Health 2018, 60, 111–125. [Google Scholar] [CrossRef]
- Wiginton, J.M.; Maksut, J.L.; Murray, S.M.; Augustinavicius, J.L.; Kall, M.; Delpech, V.; Baral, S.D. Brief report: HIV-related healthcare stigma/discrimination and unmet needs among persons living with HIV in England and Wales. Prev. Med. Rep. 2021, 24, 101580. [Google Scholar] [CrossRef]
- Manolescu, L.S.C.; Zaharia, C.N.; Dumitrescu, A.I.; Prasacu, I.; Radu, M.C.; Boeru, A.C.; Boidache, L.; Nita, I.; Necsulescu, A.; Medar, C.; et al. COVID-19 Parental Vaccine Hesitancy in Romania: Nationwide Cross-Sectional Study. Vaccines 2022, 10, 493. [Google Scholar] [CrossRef]
- Preda, M.; Mihai, M.M.; Popa, L.I.; Dițu, L.-M.; Holban, A.M.; Manolescu, L.S.C.; Popa, G.-L.; Muntean, A.-A.; Gheorghe, I.; Chifiriuc, C.M.; et al. Phenotypic and genotypic virulence features of staphylococcal strains isolated from difficult-to-treat skin and soft tissue infections. PLoS ONE 2021, 16, e0246478. [Google Scholar] [CrossRef] [PubMed]
- Radu, M.C.; Boeru, C.; Marin, M.; Manolescu, L.S.C. SARS-CoV-2 Infection in Seven Childbearing Women at the Moment of Delivery, a Romanian Experience. Cureus 2021, 13, e12811. [Google Scholar] [CrossRef] [PubMed]
- Alali, F.M.; Tarakji, B.; Alqahtani, A.S.; Alqhtani, N.R.; Nabhan, A.B.; Alenzi, A.; Alrafedah, A.; Robaian, A.; Noushad, M.; Kujan, O.; et al. Assessment of Knowledge and Attitude of Dental Students towards HIV and Its Oral Manifestations in Saudi Arabia—A Cross-Sectional Study. Healthcare 2022, 10, 1379. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristic | Total Asked = 1101 | Total Asked = 1012 | Total Asked = 89 |
|---|---|---|---|
| age, median (min–max), years | 40 (19–75) | 40 (19–75) | 40(28–50) |
| rural residence (N) | 110 | 177 | 22 |
| P% | 9.9% | 17.49% | 24.72% |
| work experience in dentistry field | |||
| 1–2 years, (N) | 154 | 154 | 0 |
| P% | 13.99% | 15.22% | |
| 3–5 years, (N) | 121 | 121 | 0 |
| P% | 10.99% | 11.96% | |
| 6–10 years, (N) | 187 | 154 | 33 |
| P% | 16.98% | 15.22% | 37.08 |
| 11–20 years, (N) | 275 | 242 | 33 |
| P% | 24.98% | 23.91% | 37.08 |
| >20 years, (N) | 364 | 341 | 23 |
| P% | 33.06% | 33.70% | 25.84 |
| have worked with PLWHA, (N) | 363 | 319 | 67 |
| P% | 32.97% | 31.52% | 75.28 |
| knew of prophylaxis for general infectious diseases, (N) | 639 | 583 | 56 |
| P% | 58.04% | 57.60% | 62.92% |
| Total Asked = 1101 | Total Asked = 1012 | Total Asked = 89 | p Value | |
|---|---|---|---|---|
| HIV Attitude, knowledge, management | yes | yes | yes | |
| know of HIV pre-exposure prophylaxis methods, (N) | 913 | 858 | 55 | <0.05 |
| P% | 82.92% | 84.78% | 61.79% | |
| know of HIV post-exposure prophylaxis methods, (N) | 715 | 660 | 55 | >0.05 |
| P% | 64.94% | 65.21% | 61.79% | |
| have been exposed to HIV during dental practice, (N) | 254 | 187 | 67 | <0.05 |
| P% | 23.07% | 18.47% | 75.28% | |
| treat PLWHA differently according to HIV treatment or stage of disease, (N) | 396 | 352 | 44 | >0.05 |
| P% | 35.97% | 34.78% | 49.43% | |
| are afraid to get infected with HIV in the dental office, (N) | 594 | 528 | 66 | <0.05 |
| P% | 53.95% | 52.17% | 74.15% | |
| have taken ARV for HIV post-exposure prophylaxis, (N) | 33 | 11 | 22 | <0.05 |
| P% | 3% | 1.08% | 24.71% | |
| are using enhanced protective equipment when working with PLWHA, (N) | 660 | 583 | 77 | <0.05 |
| P% | 59.95% | 57.60% | 86.51% | |
| consider ageing PLWHA to need more dental care, (N) | 836 | 770 | 66 | >0.05 |
| P% | 75.93% | 76.08% | 74.15% | |
| are afraid to work with PLWHA, (N) | 429 | 363 | 66 | <0.05 |
| P% | 38.96% | 35.86% | 74.15% | |
| refuse to speak with PLWHA, (N) | 66 | 33 | 33 | <0.05 |
| P% | 5.99% | 3.26% | 37.07% |
| B | E.S. | Wald | p | OR | Lower CI 95% | Upper CI 95% | |
|---|---|---|---|---|---|---|---|
| area of residence of dental practice (urban vs. rural) | −1.181 | 0.308 | 14.735 | 0.000 | 0.307 | 0.168 | 0.561 |
| know of HIV post-exposure prophylaxis methods | −0.454 | 0.257 | 3.112 | 0.078 | 0.635 | 0.384 | 1.052 |
| previously exposed to HIV during dental practice | 2.671 | 0.268 | 99.698 | 0.000 | 14.456 | 8.557 | 24.420 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caministeanu, F.; Manolescu, L.S.C.; Malița, M.A.; Perieanu, V.Ș.; Marcov, E.C.; Babiuc, I.; Ionescu, C.; Pîrvu, C.F.; Costea, R.C.; Voinescu, I.; et al. Ageing People Living with HIV/AIDS, PLWHA; More Dental Challenges; the Romanian Dental Professional’s Point of View. Life 2023, 13, 1096. https://doi.org/10.3390/life13051096
Caministeanu F, Manolescu LSC, Malița MA, Perieanu VȘ, Marcov EC, Babiuc I, Ionescu C, Pîrvu CF, Costea RC, Voinescu I, et al. Ageing People Living with HIV/AIDS, PLWHA; More Dental Challenges; the Romanian Dental Professional’s Point of View. Life. 2023; 13(5):1096. https://doi.org/10.3390/life13051096
Chicago/Turabian StyleCaministeanu, Florentina, Loredana Sabina Cornelia Manolescu, Mădălina Adriana Malița, Viorel Ștefan Perieanu, Elena Cristina Marcov, Iuliana Babiuc, Camelia Ionescu, Cristina Florentina Pîrvu, Radu Catalin Costea, Ioana Voinescu, and et al. 2023. "Ageing People Living with HIV/AIDS, PLWHA; More Dental Challenges; the Romanian Dental Professional’s Point of View" Life 13, no. 5: 1096. https://doi.org/10.3390/life13051096