

The rs2682826 Polymorphism of the NOS1 Gene Is Associated with the Degree of Disability of Erectile Dysfunction

 , and
, and
Abstract
:Simple Summary
Abstract
1. Introduction
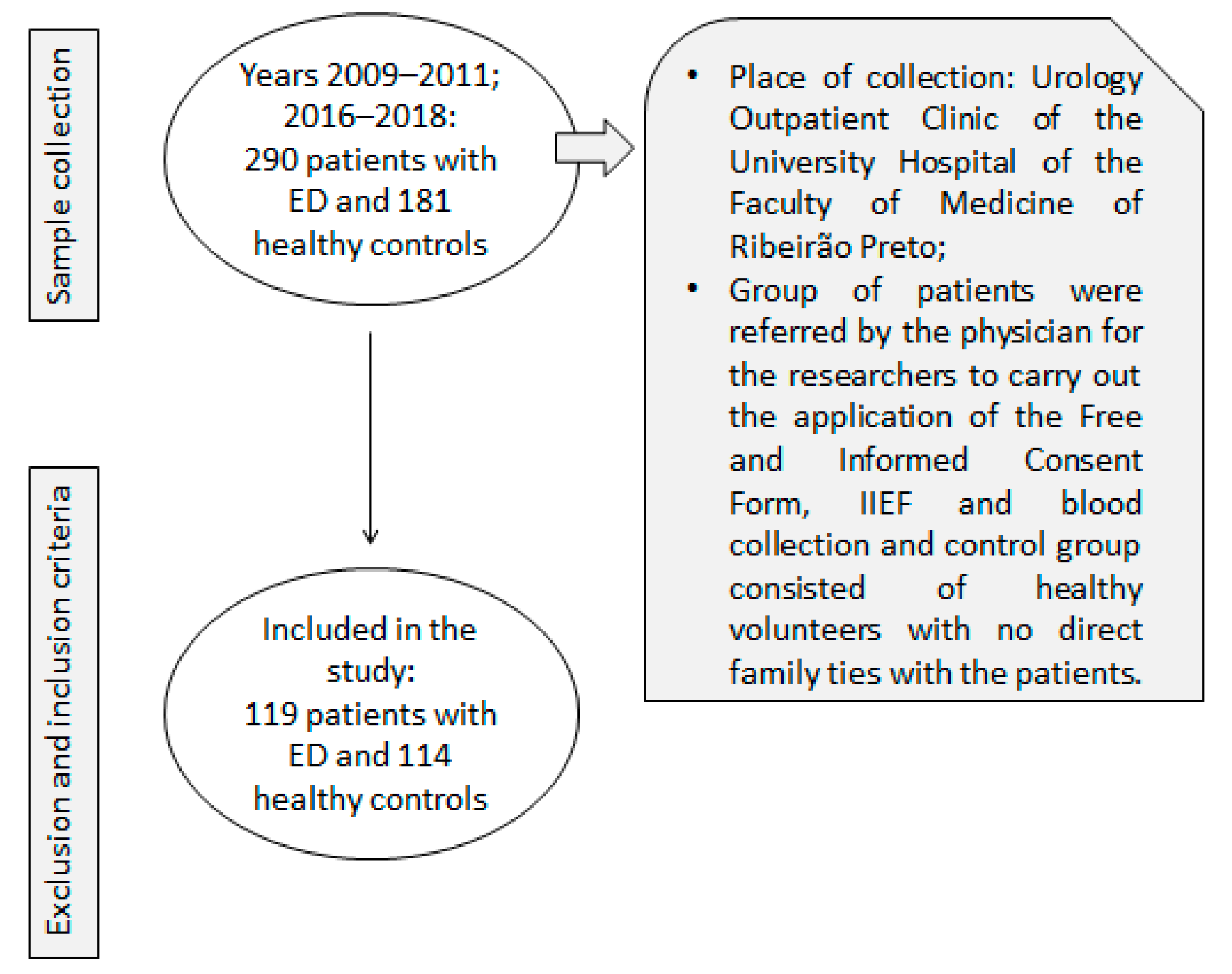
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- MacDonald, S.M.; Burnett, A.L. Physiology of Erection and Pathophysiology of Erectile Dysfunction. Urol. Clin. N. Am. 2021, 48, 513–525. [Google Scholar] [CrossRef]
- Salonia, A.; Bettocchi, C.; Boeri, L.; Capogrosso, P.; Carvalho, J.; Cilesiz, N.C.; Cocci, A.; Corona, G.; Dimitropoulos, K.; Gül, M.; et al. European Association of Urology Guidelines on Sexual and Reproductive Health-2021 Update: Male Sexual Dysfunction. Eur. Urol. 2021, 80, 333–357. [Google Scholar] [CrossRef] [PubMed]
- Burnett, A.L.; Nehra, A.; Breau, R.H.; Culkin, D.J.; Faraday, M.M.; Hakim, L.S.; Heidelbaugh, J.; Khera, M.; McVary, K.T.; Miner, M.M.; et al. Erectile Dysfunction: AUA Guideline. J. Urol. 2018, 200, 633–641. [Google Scholar] [CrossRef] [PubMed]
- Rosen, R.C.; Riley, A.; Wagner, G.; Osterloh, I.H.; Kirkpatrick, J.; Mishra, A. The International Index of Erectile Function (IIEF): A Multidimensional Scale for Assessment of Erectile Dysfunction. Urology 1997, 49, 822–830. [Google Scholar] [CrossRef]
- Gonzáles, A.I.; Sties, S.W.; Wittkopf, P.G.; Mara, L.S.; Ulbrich, A.Z.; Cardoso, F.L.; Carvalho, T. Validation of the International Index of Erectile Function (IIFE) for use in Brazil. Arq. Bras. Cardiol. 2013, 101, 176–182. [Google Scholar] [CrossRef]
- Terentes-Printzios, D.; Ioakeimidis, N.; Rokkas, K.; Vlachopoulos, C. Interactions between erectile dysfunction, cardiovascular disease and cardiovascular drugs. Nat. Rev. Cardiol. 2022, 19, 59–74. [Google Scholar] [CrossRef]
- De Oliveira, A.A.; Nunes, K.P. Hypertension and Erectile Dysfunction: Breaking Down the Challenges. Am. J. Hypertens. 2021, 34, 134–142. [Google Scholar] [CrossRef] [PubMed]
- Inman, B.A.; Sauver, J.L.; Jacobson, D.J.; McGree, M.E.; Nehra, A.; Lieber, M.M.; Roger, V.L.; Jacobsen, S.J. A population-based, longitudinal study of erectile dysfunction and future coronary artery disease. Mayo. Clin. Proc. 2009, 84, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Bocchio, M.; Scarpelli, P.; Necozione, S.; Pelliccione, F.; Mhialca, R.; Spartera, C.; Francavilla, F.; Francavilla, S. Intima-media thickening of common carotid arteries is a risk factor for severe erectile dysfunction in men with vascular risk factors but no clinical evidence of atherosclerosis. J. Urol. 2005, 173, 526–529. [Google Scholar] [CrossRef]
- Calzo, J.P.; Austin, S.B.; Charlton, B.M.; Missmer, S.A.; Kathrins, M.; Gaskins, A.J.; Chavarro, J.E. Erectile Dysfunction in a Sample of Sexually Active Young Adult Men from a U.S. Cohort: Demographic, Metabolic and Mental Health Correlates. J. Urol. 2021, 205, 539–544. [Google Scholar] [CrossRef]
- Nguyen, H.M.T.; Gabrielson, A.T.; Hellstrom, W.J.G. Erectile Dysfunction in Young Men-A Review of the Prevalence and Risk Factors. Sex. Med. Rev. 2017, 5, 508–520. [Google Scholar] [CrossRef] [PubMed]
- Lacchini, R.; Tanus-Santos, J.E. Pharmacogenetics of erectile dysfunction: Navigating into uncharted waters. Pharmacogenomics 2014, 15, 1519–1538. [Google Scholar] [CrossRef] [PubMed]
- Lacchini, R.; Muniz, J.J.; Nobre, Y.T.; Cologna, A.J.; Martins, A.C.; Tanus-Santos, J.E. nNOS polymorphisms are associated with responsiveness to sildenafil in clinical and postoperative erectile dysfunction. Pharmacogenomics 2014, 15, 775–784. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.; Azadzoi, K.M.; Goldstein, I.; Saenz de Tejada, I. A nitric oxide-like factor mediates nonadrenergic-noncholinergic neurogenic relaxation of penile corpus cavernosum smooth muscle. J. Clin. Investig. 1991, 88, 112–118. [Google Scholar] [CrossRef] [PubMed]
- Silva, C.N.D.; Pedrosa, K.N.; Silva, G.C.D.; Cunha, P.D.S.; Diniz, T.F.; Maia, L.M.S.; Almeida, F.M.; Gomez, R.S.; Lemos, V.S.; Gomes, D.A.; et al. The synthetic peptide PnPP-19 potentiates erectile function via nNOS and iNOS. Nitric. Oxide 2021, 113, 23–30. [Google Scholar] [CrossRef]
- Kang, B.S.; Suh, S.W.; Yang, D.Y.; Choi, B.Y.; Lee, W.K. Expression and Distribution of Free Zinc in Penile Erectile Tissue. World J. Mens. Health 2023, 41, 155–163. [Google Scholar] [CrossRef]
- Gantner, B.N.; LaFond, K.M.; Bonini, M.G. Nitric oxide in cellular adaptation and disease. Redox Biol. 2020, 34, 101550. [Google Scholar] [CrossRef]
- Ignarro, L.J.; Buga, G.M.; Wood, K.S.; Byrns, R.E.; Chaudhuri, G. Endothelium-derived relaxing factor produced and released from artery and vein is nitric oxide. Proc. Natl. Acad. Sci. USA 1987, 84, 9265–9269. [Google Scholar] [CrossRef]
- Tenopoulou, M.; Doulias, P.T. Endothelial nitric oxide synthase-derived nitric oxide in the regulation of metabolism. F1000Res 2020, 9, 1190. [Google Scholar] [CrossRef]
- Ahmed, W.S.; Geethakumari, A.M.; Biswas, K.H. Phosphodiesterase 5 (PDE5): Structure-function regulation and therapeutic applications of inhibitors. Biomed. Pharmacother. 2021, 134, 111128. [Google Scholar] [CrossRef]
- Calamera, G.; Moltzau, L.R.; Levy, F.O.; Andressen, K.W. Phosphodiesterases and Compartmentation of cAMP and cGMP Signaling in Regulation of Cardiac Contractility in Normal and Failing Hearts. Int. J. Mol. Sci. 2022, 23, 2145. [Google Scholar] [CrossRef] [PubMed]
- Wobst, J.; Schunkert, H.; Kessler, T. Genetic alterations in the NO-cGMP pathway and cardiovascular risk. Nitric Oxide 2018, 76, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Vasan, R.S.; Larson, M.G.; Aragam, J.; Wang, T.J.; Mitchell, G.F.; Kathiresan, S.; Newton-Cheh, C.; Vita, J.A.; Keyes, M.J.; O’Donnell, C.J.; et al. Genome-wide association of echocardiographic dimensions, brachial artery endothelial function and treadmill exercise responses in the Framingham Heart Study. BMC Med. Genet. 2007, 8, S2. [Google Scholar] [CrossRef]
- Hahn, W.H.; Suh, J.S.; Cho, B.S. Phosphodiesterase-5 gene (PDE5A) polymorphisms are associated with progression of childhood IgA nephropathy. Pediatr. Nephrol. 2010, 25, 1663–1671. [Google Scholar] [CrossRef] [PubMed]
- Hall, A.V.; Antoniou, H.; Wang, Y.; Cheung, A.H.; Arbus, A.M.; Olson, S.L.; Lu, W.C.; Kau, C.L.; Marsden, P.A. Structural organization of the human neuronal nitric oxide synthase gene (NOS1). J. Biol. Chem. 1994, 269, 33082–33090. [Google Scholar] [CrossRef]
- Roth, N.J.; Zipperich, S.; Kopf, J.; Deckert, J.; Reif, A. Influence of two functional polymorphisms in NOS1 on baseline cortisol and working memory in healthy subjects. Nitric Oxide 2019, 88, 45–49. [Google Scholar] [CrossRef]
- Chen, J.; Zhang, M.; Zhou, C.; Ding, Y.; Fan, N.; He, H. Association Analysis of Neuronal Nitric Oxide Synthase 1 Gene Polymorphism with Psychopathological Symptoms in Chronic Ketamine Users. Front. Psychiatry 2020, 11, 580771. [Google Scholar] [CrossRef]
- Singh, R.; Ghoshal, U.C.; Misra, A.; Mittal, B. Achalasia Is Associated With eNOS4a4a, iNOS22GA, and nNOS29TT Genotypes: A Case-control Study. J. Neurogastroenterol. Motil. 2015, 21, 380–389. [Google Scholar] [CrossRef]
- González-Castro, T.B.; Genis-Mendoza, A.D.; Tovilla-Zárate, C.A.; Juárez-Rojop, I.E.; López-Narvaez, M.L.; Pérez-Hernández, N.; Rodríguez-Pérez, J.M.; Martínez-Magaña, J.J. Association between polymorphisms of NOS1, NOS2 and NOS3 genes and suicide behavior: A systematic review and meta-analysis. Metab. Brain Dis. 2019, 34, 967–977. [Google Scholar] [CrossRef]
- Ahmed, S.S.S.J.; Akram Husain, R.S.; Suresh, K.; Ramakrishnan, V. Association Between NOS1 Gene Polymorphisms and Schizophrenia in Asian and Caucasian Populations: A Meta-Analysis. Neuromolecular. Med. 2017, 19, 452–461. [Google Scholar] [CrossRef]
- Rovný, R.; Marko, M.; Katina, S.; Murínová, J.; Roháriková, V.; Cimrová, B.; Repiská, G.; Minárik, G.; Riečanský, I. Association between genetic variability of neuronal nitric oxide synthase and sensorimotor gating in humans. Nitric Oxide 2018, 80, 32–36. [Google Scholar] [CrossRef]
- Bruenig, D.; Morris, C.P.; Mehta, D.; Harvey, W.; Lawford, B.; Young, R.M.; Voisey, J. Nitric oxide pathway genes (NOS1AP and NOS1) are involved in PTSD severity, depression, anxiety, stress and resilience. Gene 2017, 625, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Azevedo, A.M.M.; Brites-Anselmi, G.; Pinheiro, L.C.; Belo, V.D.; Coeli-Lacchini, F.B.; Molina, C.A.F.; de Andrade, M.F.; Tucci, S.; Hirsch, E.; Tanus-Santos, J.E.; et al. Relationship between asymmetric dimethylarginine, nitrite and genetic polymorphisms: Impact on erectile dysfunction therapy. Nitric Oxide-Biol. Chem. 2017, 71, 44–51. [Google Scholar] [CrossRef]
- Brites-Anselmi, G.; Azevedo, A.M.M.; Miyazaki, A.H.L.; Pinheiro, L.C.; Coeli-Lacchini, F.B.; de Andrade, M.F.; Molina, C.A.F.; Tucci, S., Jr.; Hirsch, E.; Tanus-Santos, J.E.; et al. DDAH1 and DDAH2 polymorphisms associate with asymmetrical dimethylarginine plasma levels in erectile dysfunction patients but not in healthy controls. Nitric Oxide 2019, 92, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Lacchini, R.; Muniz, J.J.; Nobre, Y.; Cologna, A.J.; Martins, A.C.P.; Tanus-Santos, J.E. Influence of arginase polymorphisms and arginase levels/activity on the response to erectile dysfunction therapy with sildenafil. Pharm. J. 2018, 18, 238–244. [Google Scholar] [CrossRef]
- Silva, P.S.; Fontana, V.; Luizon, M.R.; Lacchini, R.; Silva, W.A.; Biagi, C.; Tanus-Santos, J.E. eNOS and BDKRB2 genotypes affect the antihypertensive responses to enalapril. Eur. J. Clin. Pharmacol. 2013, 69, 167–177. [Google Scholar] [CrossRef] [PubMed]
- Menashe, I.; Rosenberg, P.S.; Chen, B.E. PGA: Power calculator for case-control genetic association analyses. BMC Genet. 2008, 9, 36. [Google Scholar] [CrossRef] [PubMed]
- Oliveira-Paula, G.H.; Luizon, M.R.; Lacchini, R.; Fontana, V.; Silva, P.S.; Biagi, C.; Tanus-Santos, J.E. Gene-Gene Interactions Among PRKCA, NOS3 and BDKRB2 Polymorphisms Affect the Antihypertensive Effects of Enalapril. Basic Clin. Pharmacol Toxicol. 2017, 120, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef]
- Lehnert, N.; Kim, E.; Dong, H.T.; Harland, J.B.; Hunt, A.P.; Manickas, E.C.; Oakley, K.M.; Pham, J.; Reed, G.C.; Alfaro, V.S. The Biologically Relevant Coordination Chemistry of Iron and Nitric Oxide: Electronic Structure and Reactivity. Chem. Rev. 2021, 121, 14682–14905. [Google Scholar] [CrossRef]
- Pautz, A.; Li, H.; Kleinert, H. Regulation of NOS expression in vascular diseases. Front. Biosci. 2021, 26, 85–101. [Google Scholar]
- Schirar, A.; Bonnefond, C.; Meusnier, C.; Devinoy, E. Androgens modulate nitric oxide synthase messenger ribonucleic acid expression in neurons of the major pelvic ganglion in the rat. Endocrinology 1997, 138, 3093–3102. [Google Scholar] [CrossRef] [PubMed]
- Piras, I.; Falchi, A.; Moral, P.; Paoli, G.; Calò, C.M.; Vona, G.; Varesi, L. A gradient of NOS1 overproduction alleles in European and Mediterranean populations. Genet. Test. Mol. Biomarkers 2010, 1, 673–676. [Google Scholar] [CrossRef] [PubMed]
- Miura, P.; Sanfilippo, P.; Shenker, S.; Lai, E.C. Alternative polyadenylation in the nervous system: To what lengths will 3’ UTR extensions take us? Bioessays 2014, 36, 766–777. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.D.; Park, J.S.; Yun, D.H.; Kim, H.S.; Kim, S.K.; Kim, D.H.; Chon, J.; Je, G.; Kim, Y.S.; Chung, J.H.; et al. Polymorphism of Nitric Oxide Synthase 1 Affects the Clinical Phenotypes of Ischemic Stroke in Korean Population. Ann. Rehabil. Med. 2016, 40, 102–110. [Google Scholar] [CrossRef]
- Muniz, J.J.; Lacchini, R.; Rinaldi, T.O.; Nobre, Y.T.; Cologna, A.J.; Martins, A.C.; Tanus-Santos, J.E. Endothelial nitric oxide synthase genotypes and haplotypes modify the responses to sildenafil in patients with erectile dysfunction. Pharm. J. 2013, 13, 189–196. [Google Scholar] [CrossRef]
- Lacchini, R.; Muniz, J.J.; Nobre, Y.T.; Cologna, A.J.; Martins, A.C.; Tanus-Santos, J.E. VEGF genetic polymorphisms affect the responsiveness to sildenafil in clinical and postoperative erectile dysfunction. Pharm. J. 2013, 13, 437–442. [Google Scholar] [CrossRef]
- Saur, D.; Vanderwinden, J.M.; Seidler, B.; Schmid, R.M.; De Laet, M.H.; Allescher, H.D. Single-nucleotide promoter polymorphism alters transcription of neuronal nitric oxide synthase exon 1c in infantile hypertrophic pyloric stenosis. Proc. Natl. Acad. Sci. USA 2004, 101, 1662–1667. [Google Scholar] [CrossRef]
- Hidalgo-Tamola, J.; Chitaley, K. Review type 2 diabetes mellitus and erectile dysfunction. J. Sex. Med. 2009, 6, 916–926. [Google Scholar] [CrossRef]
- McMahon, C.N.; Smith, C.J.; Shabsigh, R. Treating erectile dysfunction when PDE5 inhibitors fail. BMJ 2006, 332, 589–592. [Google Scholar] [CrossRef]
- Israilov, S.; Shmuely, J.; Niv, E.; Engelstein, D.; Livne, P.; Boniel, J. Evaluation of a progressive treatment program for erectile dysfunction in patients with diabetes mellitus. Int. J. Impot. Res. 2005, 17, 431–436. [Google Scholar] [CrossRef] [PubMed]
- Reif, A.; Herterich, S.; Strobel, A.; Ehlis, A.C.; Saur, D.; Jacob, C.P.; Wienker, T.; Töpner, T.; Fritzen, S.; Walter, U.; et al. A neuronal nitric oxide synthase (NOS-I) haplotype associated with schizophrenia modifies prefrontal cortex function. Mol. Psychiatry 2006, 11, 286–300. [Google Scholar] [CrossRef] [PubMed]
- Reif, A.; Schecklmann, M.; Eirich, E.; Jacob, C.P.; Jarczok, T.A.; Kittel-Schneider, S.; Lesch, K.P.; Fallgatter, A.J.; Ehlis, A.C. A functional promoter polymorphism of neuronal nitric oxide synthase moderates prefrontal functioning in schizophrenia. Int. J. Neuropsychopharmacol. 2011, 14, 887–897. [Google Scholar] [CrossRef]
- McCullough, A.R.; Hellstrom, W.G.; Wang, R.; Lepor, H.; Wagner, K.R.; Engel, J.D. Recovery of erectile function after nerve sparing radical prostatectomy and penile rehabilitation with nightly intraurethral alprostadil versus sildenafil citrate. J. Urol. 2010, 183, 2451–2456. [Google Scholar] [CrossRef] [PubMed]
- Cui, H.; Nishiguchi, N.; Yanagi, M.; Fukutake, M.; Mouri, K.; Kitamura, N.; Hashimoto, T.; Shirakawa, O.; Hishimoto, A. A putative cis-acting polymorphism in the NOS1 gene is associated with schizophrenia and NOS1 immunoreactivity in the postmortem brain. Schizophr. Res. 2010, 121, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Hancock, D.B.; Martin, E.R.; Vance, J.M.; Scott, W.K. Nitric oxide synthase genes and their interactions with environmental factors in Parkinson’s disease. Neurogenetics 2008, 9, 249–262. [Google Scholar] [CrossRef] [PubMed]
- Santos-Lobato, B.L.; Borges, V.; Ferraz, H.B.; Mata, I.F.; Zabetian, C.P.; Tumas, V. Association of a neuronal nitric oxide synthase gene polymorphism with levodopa-induced dyskinesia in Parkinson’s disease. Nitric Oxide 2018, 74, 86–90. [Google Scholar] [CrossRef]
- Black, M.; Wang, W. Ischemic Stroke: From Next Generation Sequencing and GWAS to Community Genomics? OMICS 2015, 19, 451–460. [Google Scholar] [CrossRef]
- Yanaka, N.; Kotera, J.; Ohtsuka, A.; Akatsuka, H.; Imai, Y.; Michibata, H.; Fujishige, K.; Kawai, E.; Takebayashi, S.; Okumura, K.; et al. Expression, structure and chromosomal localization of the human cGMP-binding cGMP-specific phosphodiesterase PDE5A gene. Eur. J. Biochem. 1998, 255, 391–399. [Google Scholar] [CrossRef]
- Marchal-Escalona, C.; Herrera-Imbroda, B.; Clemente-Postigo, M.; Alcaide-Torres, J.; Quiñonero, A.; Marchal, M.; Queipo-Ortuño, M.I.; Aragón, I.M.; Martín-Morales, A.; Laraet, M.F.; et al. PDE5A Polymorphisms Influence on Sildenafil Treatment Success. J. Sex. Med. 2016, 13, 1104–1110. [Google Scholar] [CrossRef]
- Stern, J.A.; Reina-Doreste, Y.; Chdid, L.; Meurs, K.M. Identification of PDE5A:E90K: A polymorphism in the canine phosphodiesterase 5A gene affecting basal cGMP concentrations of healthy dogs. J. Vet. Intern. Med. 2014, 28, 78–83. [Google Scholar] [CrossRef]
- Angulo, J.; Wright, H.M.; Cuevas, P.; González-Corrochano, R.; Fernández, A.; Cuevas, B.; La Fuente, J.M.; Gupta, S.; Sáenz de Tejada, I. Nebivolol dilates human penile arteries and reverses erectile dysfunction in diabetic rats through enhancement of nitric oxide signaling. J. Sex. Med. 2010, 7, 2681–2697. [Google Scholar] [CrossRef]
- Tuncayengin, A.; Biri, H.; Onaran, M.; Sen, I.; Tuncayengin, O.; Polat, F.; Erbaş, D.; Bozkirli, I. Cavernosal tissue nitrite, nitrate, malondialdehyde and glutathione levels in diabetic and non-diabetic erectile dysfunction. Int. J. Androl. 2003, 26, 250–254. [Google Scholar] [CrossRef] [PubMed]
- Sandrim, V.C.; Palei, A.C.; Metzger, I.F.; Cavalli, R.C.; Duarte, G.; Tanus-Santos, J.E. Interethnic differences in ADMA concentrations and negative association with nitric oxide formation in preeclampsia. Clin. Chim. Acta 2010, 411, 1457–1460. [Google Scholar] [CrossRef] [PubMed]
- Gebska, M.A.; Stevenson, B.K.; Hemnes, A.R.; Bivalacqua, T.J.; Haile, A.; Hesketh, G.G.; Murray, C.I.; Zaiman, A.L.; Halushka, M.K.; Krongkaew, N.; et al. Phosphodiesterase-5A (PDE5A) is localized to the endothelial caveolae and modulates NOS3 activity. Cardiovasc. Res. 2011, 90, 353–363. [Google Scholar] [CrossRef] [PubMed]
- Konstantinovsky, A.; Tamir, S.; Katz, G.; Tzischinsky, O.; Kuchersky, N.; Blum, N.; Blum, A. Erectile Dysfunction, Sleep Disorders, and Endothelial Function. Isr. Med. Assoc. J. 2019, 21, 408–411. [Google Scholar] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Control | Clinical ED | p | |
|---|---|---|---|
| n | 114 | 119 | - |
| Age (years) | 47 ± 9 | 56 ± 11 | <0.001 * |
| Ethnicity (White/non-White) | 61/53 | 56/63 | 0.325 |
| Waist circumference (cm) | 97 ± 11 | 100 ± 12 | 0.062 |
| BMI (kg m−2) | 28 ± 4 | 28 ± 5 | 0.643 |
| Smoking | |||
| Never smoker (n) | 66 | 43 | <0.001 * |
| Ex-smoker (n) | 28 | 61 | |
| Current smoker (n) | 20 | 15 | |
| Ethanol consumption | |||
| Current HD (> 30 g/day) | 11 | 5 | 0.009 * |
| Former HD (> 30 g/day) | 4 | 16 | |
| Low dose (<30 g/day) | 99 | 98 | |
| SBP (mm Hg) | 131 ± 19 | 139 ± 19 | 0.001 * |
| DBP (mm Hg) | 88 ± 13 | 89 ± 13 | 0.618 |
| HDL (mg dL−1) | 36 ± 11 | 41 ± 9 | <0.001 * |
| LDL (mg dL−1) | 127 ± 38 | 112 ± 35 | 0.002 * |
| Total cholesterol (mg dL−1) | 206 ± 46 | 181 ± 38 | <0.001 * |
| Triglycerides (mg dL−1) | 175 ± 106 | 161 ± 111 | 0.323 |
| Fasting glucose (mg dL−1) | 100 ± 40 | 127 ± 55 | <0.001 * |
| IIEF-5 score | 28 ± 2 | 10 ± 7 | <0.001 * |
| Source | Control | Clinical ED | ||
|---|---|---|---|---|
| R² = 0.11 | RMSE = 0.03 | R² = 0.14 | RMSE = 0.36 | |
| B | p | B | p | |
| Age (years) | −0.10 | 0.008 * | −1.11 | 0.006 * |
| Diabetes (yes) | +0.00 | 0.563 | −0.00 | 0.918 |
| Smoking Status | ||||
| Never Smoker | +0.00 | 0.837 | −0.01 | 0.878 |
| Ex Smoker | +0.00 | 0.379 | +0.10 | 0.047 * |
| Current Smoker | −0.01 | 0.336 | −0.09 | 0.173 |
| Ethanol Consumption (>30 g/day) | −0.00 | 0.634 | +0.04 | 0.664 |
| rs41279104 | ||||
| B | p | B | p | |
| CC | +0.00 | 0.662 | −0.01 | 0.728 |
| CT + TT | −0.00 | 0.662 | +0.01 | 0.728 |
| rs2682826 | ||||
| B | p | B | p | |
| CC | −0.01 | 0.122 | +0.07 | 0.033 * |
| CT + TT | +0.01 | 0.122 | −0.07 | 0.033 * |
| Source | Control | Clinical ED | ||
|---|---|---|---|---|
| R² = 0.09 | RMSE = 1.11 | R² = 0.14 | RMSE = 6.74 | |
| B | p | B | p | |
| Age (years) | −0.03 | 0.008 | −0.21 | <0.001 |
| Diabetes (yes) | −0.05 | 0.836 | −0.77 | 0.209 |
| Smoking Status | ||||
| Never Smoker | −0.17 | 0.277 | +0.97 | 0.281 |
| Ex Smoker | −0.09 | 0.643 | +0.94 | 0.292 |
| Current Smoker | +0.27 | 0.231 | −1.91 | 0.097 |
| Ethanol Consumption (>30 g/day) | −0.15 | 0.418 | −0.46 | 0.660 |
| Genotypes | ||||
| rs2389866 | B | p | B | p |
| TT | +0.06 | 0.706 | +0.48 | 0.542 |
| CT + CC | −0.06 | 0.706 | −0.48 | 0.542 |
| rs3733526 | B | p | B | p |
| GG | +0.13 | 0.621 | +0.01 | 0.997 |
| AG + AA | −0.13 | 0.621 | −0.01 | 0.997 |
| rs13124532 | ||||
| CC | +0.08 | 0.678 | −0.83 | 0.402 |
| CT + TT | −0.08 | 0.678 | +0.83 | 0.402 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Perticarrara Ferezin, L.; Kayzuka, C.; Rondon Pereira, V.C.; Ferreira de Andrade, M.; Molina, C.A.F.; Tucci, S., Jr.; Tanus-Santos, J.E.; Lacchini, R. The rs2682826 Polymorphism of the NOS1 Gene Is Associated with the Degree of Disability of Erectile Dysfunction. Life 2023, 13, 1082. https://doi.org/10.3390/life13051082
Perticarrara Ferezin L, Kayzuka C, Rondon Pereira VC, Ferreira de Andrade M, Molina CAF, Tucci S Jr., Tanus-Santos JE, Lacchini R. The rs2682826 Polymorphism of the NOS1 Gene Is Associated with the Degree of Disability of Erectile Dysfunction. Life. 2023; 13(5):1082. https://doi.org/10.3390/life13051082
Chicago/Turabian StylePerticarrara Ferezin, Leticia, Cezar Kayzuka, Vitória Carolina Rondon Pereira, Murilo Ferreira de Andrade, Carlos Augusto Fernandes Molina, Silvio Tucci, Jr., Jose Eduardo Tanus-Santos, and Riccardo Lacchini. 2023. "The rs2682826 Polymorphism of the NOS1 Gene Is Associated with the Degree of Disability of Erectile Dysfunction" Life 13, no. 5: 1082. https://doi.org/10.3390/life13051082