
SH3YL1 Protein Predicts Renal Outcomes in Patients with Type 2 Diabetes
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Patients
2.2. Renal Outcome
2.3. Data Collection
2.4. Measurement of Plasma SH3YL1 and Urinary Albumin and SH3YL1
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics of the Study Population
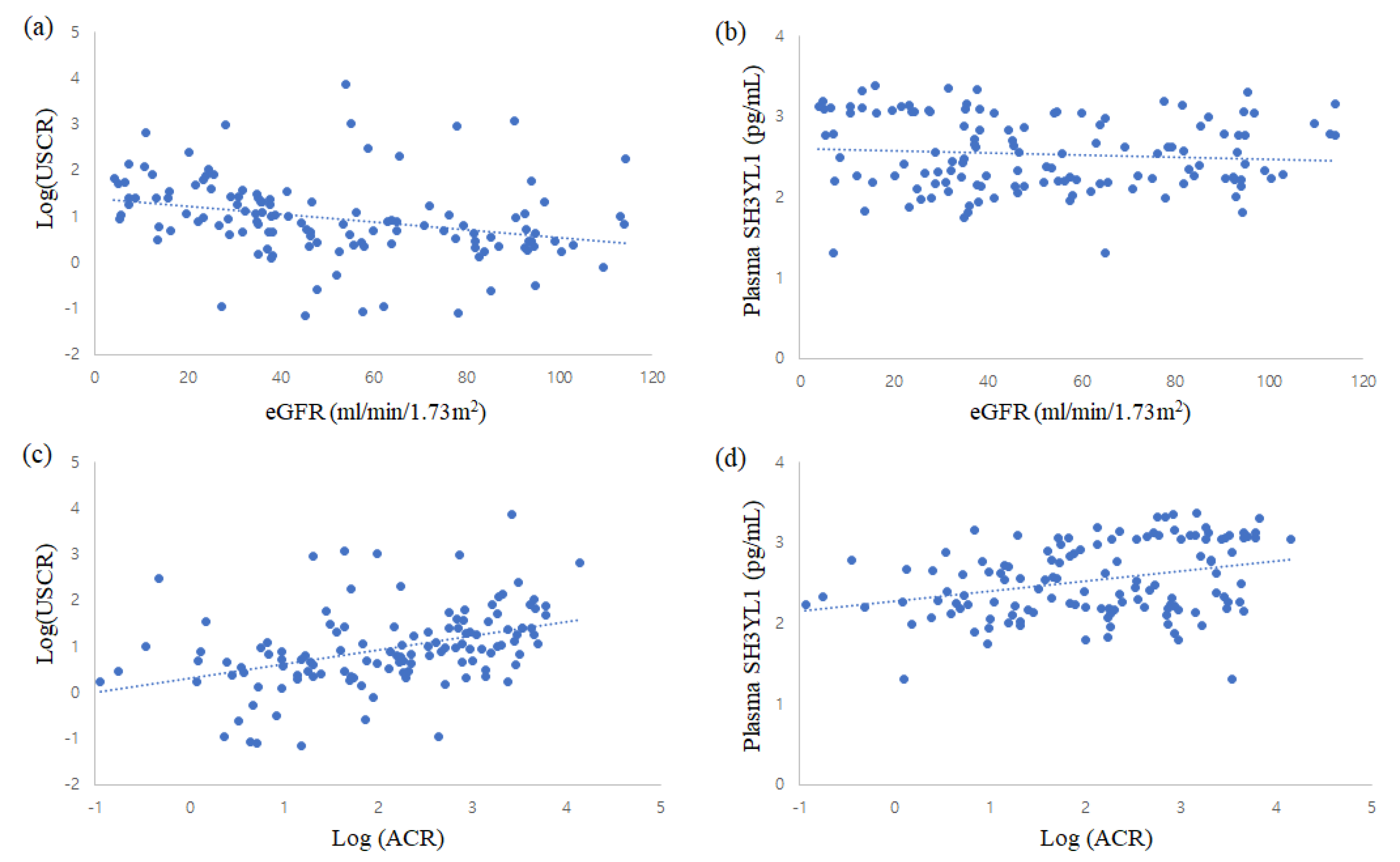
3.2. Plasma and Urinary Levels of SH3YL1
3.3. Prediction for Renal Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maruno, S.; Tanaka, T.; Nangaku, M. Exploring molecular targets in diabetic kidney disease. Kidney Res. Clin. Pract. 2022, 41, S33–S45. [Google Scholar] [CrossRef] [PubMed]
- Honda, T.; Hirakawa, Y.; Nangaku, M. The role of oxidative stress and hypoxia in renal disease. Kidney Res. Clin. Pract. 2019, 38, 414–426. [Google Scholar] [CrossRef] [Green Version]
- Jha, J.C.; Banal, C.; Chow, B.S.; Cooper, M.E.; Jandeleit-Dahm, K. Diabetes and Kidney Disease: Role of Oxidative Stress. Antioxid. Redox. Signal. 2016, 25, 657–684. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Araki, S.-I.; Haneda, M.; Koya, D.; Sugaya, T.; Isshiki, K.; Kume, S.; Kashiwagi, A.; Uzu, T.; Maegawa, H. Predictive effects of urinary liver-type fatty acid-binding protein for deteriorating renal function and incidence of cardiovascular disease in type 2 diabetic patients without advanced nephropathy. Diabetes Care 2013, 36, 1248–1253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nielsen, S.E.; Sugaya, T.; Hovind, P.; Baba, T.; Parving, H.H.; Rossing, P. Urinary liver-type fatty acid-binding protein predicts progression to nephropathy in type 1 diabetic patients. Diabetes Care 2010, 33, 1320–1324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, T.Q.; Tarnow, L.; Jorsal, A.; Oliver, N.; Roestenberg, P.; Ito, Y.; Parving, H.H.; Rossing, P.; Van Nieuwenhoven, F.A.; Goldschmeding, R. Plasma connective tissue growth factor is an independent predictor of end-stage renal disease and mortality in type 1 diabetic nephropathy. Diabetes Care 2008, 31, 1177–1182. [Google Scholar] [CrossRef] [Green Version]
- Astrup, A.S.; Tarnow, L.; Pietraszek, L.; Schalkwijk, C.G.; Stehouwer, C.D.; Parving, H.H.; Rossing, P. Markers of endothelial dysfunction and inflammation in type 1 diabetic patients with or without diabetic nephropathy followed for 10 years: Association with mortality and decline of glomerular filtration rate. Diabetes Care 2008, 31, 1170–1176. [Google Scholar] [CrossRef] [Green Version]
- Sharma, K.; Karl, B.; Mathew, A.V.; Gangoiti, J.A.; Wassel, C.L.; Saito, R.; Pu, M.; Sharma, S.; You, Y.-H.; Wang, L.; et al. Metabolomics reveals signature of mitochondrial dysfunction in diabetic kidney disease. J. Am. Soc. Nephrol. 2013, 24, 1901–1912. [Google Scholar] [CrossRef] [Green Version]
- Jha, J.C.; Gray, S.P.; Barit, D.; Okabe, J.; El-Osta, A.; Namikoshi, T.; Thallas-Bonke, V.; Wingler, K.; Szyndralewiez, C.; Heitz, F.; et al. Genetic targeting or pharmacologic inhibition of NADPH oxidase nox4 provides renoprotection in long-term diabetic nephropathy. J. Am. Soc. Nephrol. 2014, 25, 1237–1254. [Google Scholar] [CrossRef] [Green Version]
- Sedeek, M.; Callera, G.; Montezano, A.; Gutsol, A.; Heitz, F.; Szyndralewiez, C.; Page, P.; Kennedy, C.R.; Burns, K.D.; Touyz, R.M.; et al. Critical role of Nox4-based NADPH oxidase in glucose-induced oxidative stress in the kidney: Implications in type 2 diabetic nephropathy. Am. J. Physiol. Renal. Physiol. 2010, 299, F1348–F1358. [Google Scholar] [CrossRef]
- Bedard, K.; Krause, K.-H. The NOX family of ROSgenerating NADPH oxidases: Physiology and pathophysiology. Physiol. Rev. 2007, 87, 245–313. [Google Scholar] [CrossRef] [PubMed]
- Block, K.; Gorin, Y.; Abboud, H.E. Subcellular localization of Nox4 and regulation in diabetes. Proc. Natl. Acad. Sci. USA 2009, 106, 14385–14390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eid, A.A.; Gorin, Y.; Fagg, B.M.; Maalouf, R.; Barnes, J.L.; Block, K.; Abboud, H.E. Mechanisms of podocyte injury in diabetes: Role of cytochrome P450 and NADPH oxidases. Diabetes 2009, 58, 1201–1211. [Google Scholar] [CrossRef] [Green Version]
- Sedeek, M.; Nasrallah, R.; Touyz, R.M.; Hébert, R.L. NADPH oxidases, reactive oxygen species, and the kidney: Friend and foe. J. Am. Soc. Nephrol. 2013, 24, 1512–1518. [Google Scholar] [CrossRef] [Green Version]
- Vermot, A.; Petit-Härtlein, I.; Smith, S.M.E.; Fieschi, F. NADPH Oxidases (NOX): An Overview from Discovery, Molecular Mechanisms to Physiology and Pathology. Antioxidants 2021, 10, 890. [Google Scholar] [CrossRef]
- Burtenshaw, D.; Hakimjavadi, R.; Redmond, E.M.; Cahill, P.A. Nox, Reactive Oxygen Species and Regulation of Vascular Cell Fate. Antioxidants 2017, 6, 90. [Google Scholar] [CrossRef] [Green Version]
- Xia, L.; Wang, H.; Munk, S.; Kwan, J.; Goldberg, H.J.; Fantus, I.G.; Whiteside, C.I. High glucose activates PKC-zeta and NADPH oxidase through autocrine TGF-beta1 signaling in mesangial cells. Am. J. Physiol. Renal. Physiol. 2008, 295, F1705–F1714. [Google Scholar] [CrossRef] [PubMed]
- Rajaram, R.; Dissard, R.; Jaquet, V.; de Seigneux, S. Potential benefits and harms of NADPH oxidase type 4 in the kidneys and cardiovascular system. Nephrol. Dial. Transplant. 2019, 34, 567–576. [Google Scholar] [CrossRef]
- Kawahara, T.; Ritsick, D.; Cheng, G.; Lambeth, J.D. Point mutations in the proline-rich region of p22phox are dominant in-hibitors of Nox1- and Nox2-dependent reactive oxygen generation. J. Biol. Chem. 2005, 280, 31859–31869. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.F.; Qiao, M.; Schröder, K.; Zhao, Q.; Asmis, R. Nox4 is a novel inducible source of reactive oxygen species in monocytes and macrophages and mediates oxidized low density lipoprotein-induced macrophage death. Circ. Res. 2010, 106, 1489–1497. [Google Scholar] [CrossRef] [Green Version]
- Yoo, J.Y.; Cha, D.R.; Kim, B.; An, E.J.; Lee, S.R.; Cha, J.J.; Kang, Y.S.; Ghee, J.Y.; Han, J.Y.; Bae, Y.S. LPS-Induced Acute Kidney Injury Is Mediated by Nox4-SH3YL1. Cell. Rep. 2020, 33, 108245. [Google Scholar] [CrossRef] [PubMed]
- Aoki, N.; Ito, K.; Ito, M. A novel mouse gene, Sh3yl1, is expressed in the anagen hair follicle. J. Investig. Dermatol. 2000, 114, 1050–1056. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koch, C.A.; Anderson, D.; Moran, M.F.; Ellis, C.; Pawson, T. SH2 and SH3 domains: Elements that control interactions of cyto-plasmic signaling proteins. Science 1991, 252, 668–674. [Google Scholar] [CrossRef] [PubMed]
- Shimomura, Y.; Aoki, N.; Ito, K.; Ito, M. Gene expression of Sh3d19, a novel adaptor protein with five Src homology 3 domains, in anagen mouse hair follicles. J. Dermatol. Sci. 2003, 31, 43–51. [Google Scholar] [CrossRef]
- Choi, G.S.; Min, H.S.; Cha, J.J.; Lee, J.E.; Ghee, J.Y.; Yoo, J.A.; Kim, K.T.; Kang, Y.S.; Han, S.Y.; Bae, Y.S.; et al. SH3YL1 protein as a novel biomarker for diabetic nephropathy in type 2 diabetes mellitus. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 498–505. [Google Scholar] [CrossRef]
- Jha, J.C.; Thallas-Bonke, V.; Banal, C.; Gray, S.P.; Chow, B.S.; Ramm, G.; Quaggin, S.E.; Cooper, M.E.; Schmidt, H.H.; Jandeleit-Dahm, K.A. Podocyte-specific Nox4 deletion affords renoprotection in a mouse model of diabetic nephropathy. Diabetologia 2016, 59, 379–389. [Google Scholar] [CrossRef] [Green Version]
- Meng, X.M.; Ren, G.L.; Gao, L.; Yang, Q.; Li, H.D.; Wu, W.F.; Huang, C.; Zhang, L.; Lv, X.W.; Li, J. NADPH oxidase 4 promotes cispla-tin-induced acute kidney injury via ROS-mediated programmed cell death and inflammation. Lab. Investig. 2018, 98, 63–78. [Google Scholar] [CrossRef] [Green Version]
- Babelova, A.; Avaniadi, D.; Jung, O.; Fork, C.; Beckmann, J.; Kosowski, J.; Weissmann, N.; Anilkumar, N.; Shah, A.M.; Schaefer, L.; et al. Role of Nox4 in murine models of kidney disease. Free. Radic. Biol. Med. 2012, 53, 842–853. [Google Scholar] [CrossRef]
- Li, X.-Q.; Tian, W.; Liu, X.-X.; Zhang, K.; Huo, J.-C.; Liu, W.-J.; Li, P.; Xiao, X.; Zhao, M.-G.; Cao, W. Corosolic acid inhibits the proliferation of glomerular mesangial cells and protects against diabetic renal damage. Sci. Rep. 2016, 6, 26854. [Google Scholar] [CrossRef] [Green Version]
- Mason, R.M.; Wahab, N.A. Extracellular matrix metabolism in diabetic nephropathy. J. Am. Soc. Nephrol. 2003, 14, 1358–1373. [Google Scholar] [CrossRef] [Green Version]
- Forbes, J.M.; Coughlan, M.T.; Cooper, M.E. Oxidative stress as a major culprit in kidney disease in diabetes. Diabetes 2008, 57, 1446–1454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Singh, D.K.; Winocour, P.; Farrington, K. Oxidative stress in early diabetic nephropathy: Fueling the fire. Nat. Rev. Endocrinol. 2011, 7, 176–184. [Google Scholar] [CrossRef] [PubMed]
- Bae, Y.S.; Oh, H.; Rhee, S.G.; Yoo, Y.D. Regulation of Reactive Oxygen Species: Generation in Cell Signaling. Mol. Cells 2011, 32, 491–509. [Google Scholar] [CrossRef] [Green Version]
- Gill, P.S.; Wilcoxm, C.S. Forum Review NADPH Oxidases in the Kidney. Antioxid. Redox. Signal. 2006, 8, 1597–1607. [Google Scholar] [CrossRef] [PubMed]
- Gorin, Y.; Block, K. Nox as a target for diabetic complications. Clin. Sci. 2013, 125, 361–382. [Google Scholar] [CrossRef] [Green Version]
- Thallas-Bonke, V.; Jha, J.C.; Gray, S.P.; Barit, D.; Haller, H.; Schmidt, H.H.; Coughlan, M.T.; Cooper, M.E.; Forbes, J.M.; Jandeleit-Dahm, K.A. Nox-4 deletion reduces oxidative stress and injury by PKCalpha-associated mechanisms in diabetic nephropathy. Physiol. Rep. 2014, 2, e12192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gorin, Y.; Block, K.; Hernandez, J.; Bhandari, B.; Wagner, B.; Barnes, J.L.; Abboud, H.E. Nox4 NAD(P)H oxidase mediates hypertrophy and fibronectin expression in the diabetic kidney. J. Biol. Chem. 2005, 280, 39616–39626. [Google Scholar] [CrossRef] [Green Version]
- Hong, C.Y.; Chia, K.S. Markers of diabetic nephropathy. J. Diabet. Complicat. 1998, 12, 43–60. [Google Scholar] [CrossRef]
- Yamanouchi, M.; Furuichi, K.; Hoshino, J.; Ubara, Y.; Wada, T. Nonproteinuric diabetic kidney disease. Clin. Exp. Nephrol. 2020, 24, 573–581. [Google Scholar] [CrossRef] [Green Version]
- Lin, Y.C.; Chang, Y.H.; Yang, S.Y.; Wu, K.D.; Chu, T.S. Update of pathophysiology and management of diabetic kidney disease. J. Formos. Med. Assoc. 2018, 117, 662–675. [Google Scholar] [CrossRef]
- Colhoun, H.M.; Marcovecchio, M.L. Biomarkers of diabetic kidney disease. Diabetologia 2018, 61, 996–1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanchez, M.; Roussel, R.; Hadjadj, S.; Moutairou, A.; Marre, M.; Velho, G.; Mohammedi, K. Plasma concentrations of 8-hydroxy-2′-deoxyguanosine and risk of kidney disease and death in individuals with type 1 diabetes. Diabetologia 2018, 61, 977–984. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serdar, M.; Sertoglu, E.; Uyanik, M.; Tapan, S.; Akin, K.; Bilgi, C.; Kurt, I. Comparison of 8-hydroxy-2′-deoxyguanosine (8-OHdG) levels using mass spectrometer and urine albumin creatinine ratio as a predictor of development of diabetic nephropathy. Free. Radic. Res. 2012, 46, 1291–1295. [Google Scholar] [CrossRef]
- Blessing, A.M.; Ganesan, S.; Rajapakshe, K.; Ying, S.Y.; Reddy, B.L.; Shi, Y.; Cheung, E.; Coarfa, C.; Chang, J.T.; McDonnell, D.P.; et al. Identification of a Novel Coregulator, SH3YL1, That Interacts with the Androgen Receptor N-Terminus. Mol. Endocrinol. 2015, 29, 1426–1439. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bai, R.; Li, Z.; Hou, Y.; Lv, S.; Wang, R.; Hua, W.; Wu, H.; Dai, L. Identification of Diagnostic Markers Correlated With HIV+ Immune Non-response Based on Bioinformatics Analysis. Front. Mol. Biosci. 2021, 8, 809085. [Google Scholar] [CrossRef]
- Fernandes, S.J.; Morikawa, H.; Ewing, E.; Ruhrmann, S.; Joshi, R.N.; Lagani, V.; Karathanasis, N.; Khademi, M.; Planell, N.; Schmidt, A.; et al. Non-parametric combination analysis of multiple data types enables detection of novel regulatory mechanisms in T cells of multiple sclerosis patients. Sci. Rep. 2019, 9, 11996. [Google Scholar] [CrossRef] [Green Version]
- Hasegawa, J.; Jebri, I.; Yamamoto, H.; Tsujita, K.; Tokuda, E.; Shibata, H.; Maki, M.; Itoh, T. SH3YL1 cooperates with ESCRT-I in the sorting and degradation of the EGF receptor. J. Cell. Sci. 2019, 132, 229179. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Total | USCR | Plasma SH3YL1 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Tertile 1 | Tertile 2 | Tertile 3 | p-Value | Tertile 1 | Tertile 2 | Tertile 3 | p-Value | ||
| Number (M:F) | 89:42 | 29:7 | 31:5 | 22:15 | 0.021 | 30:8 | 27:11 | 28:10 | 0.723 |
| Age (years) | 62.7 ± 11.4 | 66.3 ± 9.3 | 66.0 ± 10.2 | 57.3 ± 11.8 | <0.001 | 62.2 ± 9.6 | 62.8 ± 12.0 | 64.4 ± 11.6 | 0.685 |
| BMI | 25.4 ± 3.51 | 25.5 ± 2.10 | 25.5 ± 3.50 | 24.7 ± 4.09 | 0.503 | 24.5 ± 3.18 | 25.5 ± 3.68 | 25.7 ± 3.01 | 0.274 |
| Duration (y) | 13.1 ± 8.3 | 12.2 ± 8.1 | 13.6 ± 8.5 | 12.1 ± 7.7 | 0.660 | 11.4 ± 7.8 | 12.9 ± 8.5 | 13.4 ± 8.3 | 0.567 |
| SBP (mmHg) | 135.8 ± 14.8 | 133.5 ± 14.2 | 134.5 ± 11.2 | 136.7 ± 18.5 | 0.633 | 132.1 ± 11.8 | 135.4 ± 14.6 | 137.2 ± 18.1 | 0.345 |
| DBP (mmHg) | 74.1 ± 11.9 | 72.1 ± 12.6 | 72.3 ± 11.6 | 77.0 ± 11.4 | 0.131 | 73.4 ± 10.9 | 75.3 ± 12.8 | 71.4 ± 11.4 | 0.357 |
| FBS (mg/dL) | 131 (105.7–154.5) | 128.5 (114.0–149.3) | 129.0 (105.0–164.0) | 131.0 (109.0–152.0) | 0.967 | 118.0 (92.0–148.0) | 138.5 (120.3–158.5) | 130.0 (114.5–173.3) | 0.054 |
| HbA1c (%) | 6.90 (6.40–8.05) | 6.75 (6.40–7.43) | 6.90 (6.50–8.05) | 7.00 (6.40–8.20) | 0.463 | 6.90 (6.60–7.40) | 6.95 (6.40–7.50) | 7.30 (6.43–9.20) | 0.521 |
| BUN (mg/dL) | 30.0 ± 20.1 | 26.3 ± 12.0 | 26.5 ± 21.1 | 24.9 ± 13.5 | 0.892 | 20.7 ± 19.8 | 26.3 ± 12.6 | 30.5 ± 12.6 | 0.029 |
| Creatinine (mg/dL) | 1.95 ± 1.61 | 1.48 ± 0.60 | 1.38 ± 0.54 | 1.64 ± 0.85 | 0.244 | 1.15 ± 0.38 | 1.59 ± 0.69 | 1.77 ± 0.77 | <0.001 |
| eGFR (ml/min/1.73 m2) | 46.0 (28.8–78.3) | 78.0 (51.0–92.8) | 46.4 (35.1–71.9) | 35.6 (28.0–56.4) | <0.001 | 53.6 (35.9–64.5) | 53.1 (35.7–81.2) | 50.9 (32.5–89.6) | 0.903 |
| Hemoglobin (g/dL) | 12.58 ± 2.26 | 13.1 ± 2.13 | 13.4 ± 1.87 | 12.5 ± 1.89 | 0.163 | 13.9 ± 1.89 | 13.0 ± 2.10 | 12.1 ± 1.66 | 0.001 |
| Total protein (g/L) | 6.94 ± 0.60 | 7.07 ± 0.47 | 6.88 ± 0.45 | 6.85 ± 0.83 | 0.238 | 7.09 ± 0.58 | 7.02 ± 0.52 | 6.72 ± 0.59 | 0.018 |
| Albumin (g/L) | 4.12 ± 0.49 | 4.19 ± 0.44 | 4.18 ± 0.38 | 3.99 ± 0.62 | 0.154 | 4.24 ± 0.50 | 4.21 ± 0.39 | 3.94 ± 0.48 | 0.011 |
| Cholesterol (mg/dL) | 152.0 (132.0–183.5) | 152.9 (136.2–182.3) | 138.0 (129.7–161.0) | 155.5 (138.6–192.8) | 0.096 | 143.3 (131.0–163.1) | 153.7 (135.9–180.9) | 155.2 (132.3–191.3) | 0.380 |
| HDL (mg/dL) | 46.0 ± 11.7 | 43.1 ± 5.37 | 49.1 ± 14.4 | 45.8 ± 13.2 | 0.569 | 52.4 ± 17.0 | 38.9 ± 7.96 | 46.9 ± 10.0 | 0.082 |
| LDL (mg/dL) | 89.9 ± 30.8 | 83.2 ± 23.7 | 87.5 ± 23.3 | 99.0 ± 41.6 | 0.082 | 90.9 ± 28.0 | 83.4 ± 23.3 | 94.4 ± 38.9 | 0.327 |
| Triglyceride (mg/dL) | 132.0 (97.0–200.0) | 126.0 (90.0–200.0) | 127.0 (97.0–190.0) | 153.0 (105.5–209.5) | 0.704 | 145.0 (100.3–218.8) | 111.0 (90.3–181.5) | 139.5 (104.0–191.0) | 0.287 |
| Uric acid (mg/dL) | 6.62 ± 2.10 | 6.91 ± 2.13 | 6.39 ± 1.98 | 6.56 ± 2.11 | 0.558 | 5.80 ± 1.80 | 6.84 ± 1.94 | 7.23 ± 2.29 | 0.012 |
| UACR (g/gCr) | 0.173 (0.016–1.000) | 0.019 (0.005–0.099) | 0.165 (0.014–0.562) | 0.720 (0.052–1.652) | <0.001 | 0.088 (0.010–0.627) | 0.045 (0.010–0.338) | 0.285 (0.053–1.778) | 0.011 |
| USCR (pg/mgCr) | 7.73 (2.84–25.5) | 1.92 (0.72–2.48) | 6.60 (4.79–8.33) | 34.1 (20.4–104.3) | <0.001 | 8.97 (2.65–34.1) | 4.52 (1.92–11.0) | 7.53 (3.10–21.6) | 0.098 |
| Plasma SH3YL1 (pg/mL) | 301.1 (154.3–1035.8) | 242.9 (163.5–585.1) | 433.1 (172.4–1119.9) | 181.2 (141.5–647.4) | 0.194 | 129.7 (96.5–151.6) | 265.6 (206.2–403.2) | 1133.1 (771.9–1318.5) | <0.001 |
| Markers | Number of Events/Number of Patients | Unadjusted | Model 1 | Model 2 | |||
|---|---|---|---|---|---|---|---|
| HR (95% CI) | p-Value | aHR (95% CI) | p-Value | aHR (95% CI) | p-Value | ||
| Urine SH3YL1-to-Cr ratio | |||||||
| Tertile 1 | 4/33 | Ref. | Ref. | Ref. | |||
| Tertile 2 | 13/32 | 3.778 (1.231–11.597) | 0.020 | 3.772 (1.228–11.584) | 0.020 | 2.633(0.809–8.576) | 0.108 |
| Tertile 3 | 26/35 | 8.326 (2.888–24.003) | <0.001 | 9.616 (3.291–28.099) | <0.001 | 4.636 (1.416–15.181) | 0.011 |
| Serum SH3YL1 | |||||||
| Tertile 1 | 12/35 | Ref. | Ref. | Ref. | |||
| Tertile 2 | 12/36 | 0.995 (0.447–2.215) | 0.991 | 1.065 (0.475–2.390) | 0.879 | 1.075 (0.473–2.441) | 0.863 |
| Tertile 3 | 20/34 | 2.167 (1.053–4.458) | 0.036 | 2.448 (1.124–5.333) | 0.024 | 1.511 (0.643–3.549) | 0.343 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, S.Y.; Han, S.H.; Ghee, J.Y.; Cha, J.J.; Kang, Y.S.; Cha, D.R. SH3YL1 Protein Predicts Renal Outcomes in Patients with Type 2 Diabetes. Life 2023, 13, 963. https://doi.org/10.3390/life13040963
Han SY, Han SH, Ghee JY, Cha JJ, Kang YS, Cha DR. SH3YL1 Protein Predicts Renal Outcomes in Patients with Type 2 Diabetes. Life. 2023; 13(4):963. https://doi.org/10.3390/life13040963
Chicago/Turabian StyleHan, Sang Youb, Seung Hyun Han, Jung Yeon Ghee, Jin Joo Cha, Young Sun Kang, and Dae Ryong Cha. 2023. "SH3YL1 Protein Predicts Renal Outcomes in Patients with Type 2 Diabetes" Life 13, no. 4: 963. https://doi.org/10.3390/life13040963