
Thrombolysis Outcomes in Acute Ischaemic Stroke Patients with Pre-Existing Cognitive Impairment
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
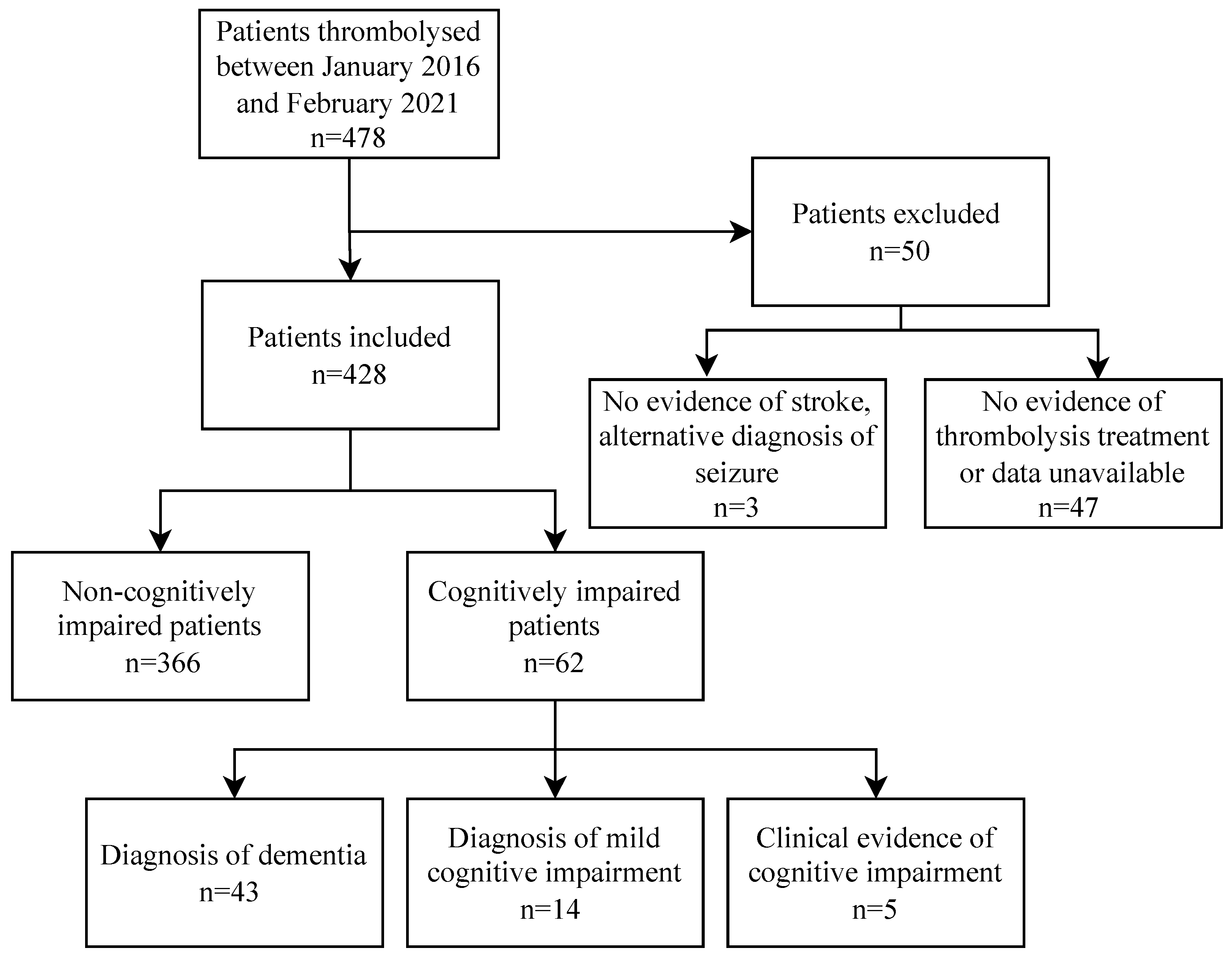
2.1. Data Collection and Study Population Characterisation
2.2. Outcome Measures
2.3. Statistical Analysis
3. Results
3.1. Demographic Data
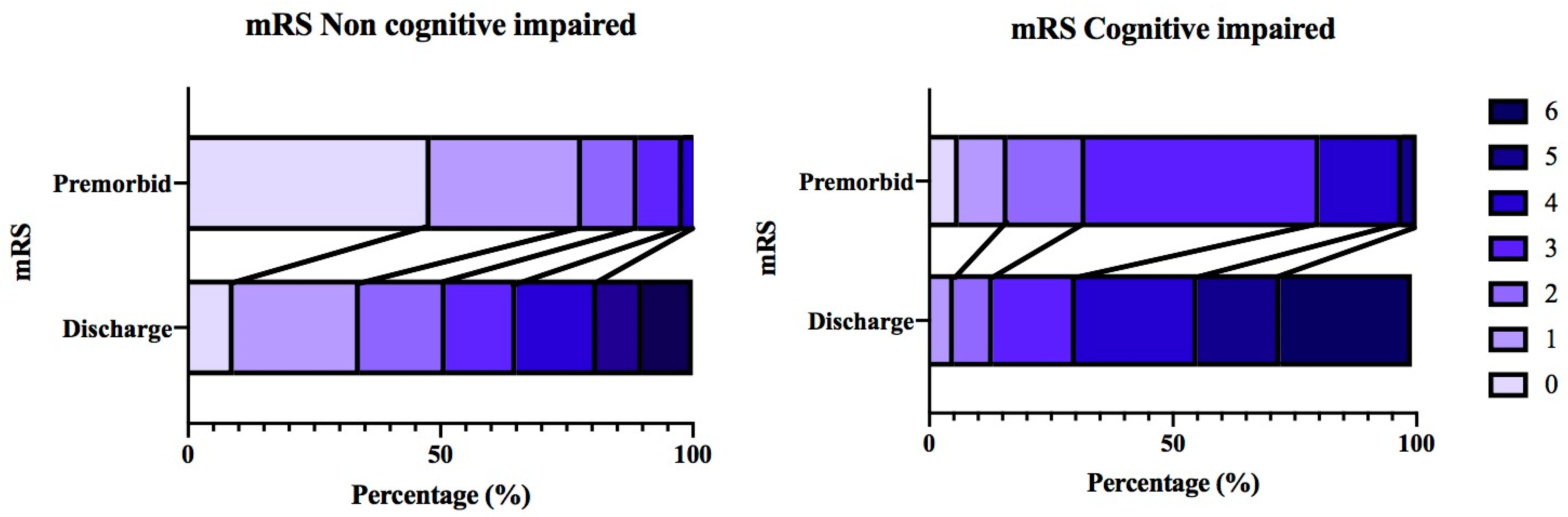
3.2. Morbidity
3.3. Mortality
3.4. Haemorrhagic Complication
3.5. Logistic Regression Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wardlaw, J.M.; Murray, V.; Berge, E.; del Zoppo, G.J. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst. Rev. 2014, 2014, CD000213. [Google Scholar] [CrossRef] [PubMed]
- Hacke, W.; Kaste, M.; Bluhmki, E.; Brozman, M.; Dávalos, A.; Guidetti, D.; Larrue, V.; Lees, K.R.; Medeghri, Z.; Machnig, T. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N. Engl. J. Med. 2008, 359, 1317–1329. [Google Scholar] [CrossRef] [PubMed]
- Merlino, G.; Corazza, E.; Lorenzut, S.; Gigli, G.L.; Cargnelutti, D.; Valente, M. Efficacy and safety of intravenous thrombolysis in patients with acute ischemic stroke and pre-existing disability. J. Clin. Med. 2019, 8, 400. [Google Scholar] [CrossRef]
- Thomson, R.G.; De Brún, A.; Flynn, D.; Ternent, L.; Price, C.I.; Rodgers, H.; Ford, G.A.; Rudd, M.; Lancsar, E.; Simpson, S.; et al. Factors that influence variation in clinical decision-making about thrombolysis in the treatment of acute ischaemic stroke: Results of a discrete choice experiment. Health Serv. Deliv. Res. 2017, 5, 1–116. [Google Scholar] [CrossRef]
- Karlinski, M.; Kobayashi, A.; Czlonkowska, A.; Mikulík, R.; Vaclavik, D.; Brozman, M.; Švigelj, V.; Csiba, L.; Fekete, K.; Kõrv, J.; et al. Role of preexisting disability in patients treated with intravenous thrombolysis for ischemic stroke. Stroke 2014, 45, 770–775. [Google Scholar] [CrossRef] [PubMed]
- Paciaroni, M.; Pantoni, L. Thrombolysis in dementia patients with acute stroke: Is it justified? Neurol Sci. 2017, 38, 27–31. [Google Scholar] [CrossRef] [PubMed]
- Zupanic, E.; von Euler, M.; Kåreholt, I.; Escamez, B.C.; Fastbom, J.; Norrving, B.; Religa, D.; Kramberger, M.G.; Winblad, B.; Johnell, K. Thrombolysis in acute ischemic stroke in patients with dementia: A Swedish registry study. Neurology 2017, 89, 1860–1868. [Google Scholar] [CrossRef]
- Alshekhlee, A.; Li, C.C.; Chuang, S.Y.; Vora, N.; Edgell, R.C.; Kitchener, J.M.; Kale, S.P.; Feen, E.; Piriyawat, P.; Callison, R.C.; et al. Does dementia increase risk of thrombolysis?: A case-control study. Neurology 2011, 76, 1575–1580. [Google Scholar] [CrossRef]
- Henon, H.; Pasquier, F.; Durieu, M.; Godefroy, O.; Lucas, C. Preexisting dementia in stroke patients: Baseline frequency, associated factors, and outcome. Stroke 1997, 28, 2429–2436. [Google Scholar] [CrossRef]
- Sandercock, P.; Lindley, R.; Wardlaw, J.; Dennis, M.; Lewis, S.; Venables, G.; Kobayashi, A.; Czlonkowska, A.; Berge, E.; Slot, K.B.; et al. The third international stroke trial (IST-3) of thrombolysis for acute ischaemic stroke. Trials 2008, 9, 37. [Google Scholar] [CrossRef]
- Boyle, P.A.; Yu, L.; Nag, S.; Leurgans, S.; Wilson, R.S.; Bennett, D.A.; Schneider, J.A. Cerebral amyloid angiopathy and cognitive outcomes in community-based older persons. Neurology 2015, 85, 1930–1936. [Google Scholar] [CrossRef] [PubMed]
- McCarron, M.O.; Nicoll, J.A. Cerebral amyloid angiopathy and thrombolysis-related intracerebral haemorrhage. Lancet Neurol. 2004, 3, 484–492. [Google Scholar] [CrossRef] [PubMed]
- Nasr, D.; Rabinstein, A.; McDonald, J. In-hospital outcomes of thrombolysis in dementia patients with ischemic strokes. Stroke 2015, 46 (Suppl. S1), A59. [Google Scholar] [CrossRef]
- Dos Santos Kawata, K.H.; Hashimoto, R.; Nishio, Y.; Hayashi, A.; Ogawa, N.; Kanno, S.; Hiraoka, K.; Yokoi, K.; Iizuka, O.; Mori, E. A validation study of the Japanese version of the addenbrooke’s cognitive examination-revised. Dement Geriatr. Cogn. Dis. Extra 2012, 2, 29–37. [Google Scholar] [CrossRef] [PubMed]
- Smith, T.; Gildeh, N.; Holmes, C. The Montreal cognitive assessment: Validity and utility in a memory clinic setting. Can J. Psychiatry 2007, 52, 329–332. [Google Scholar] [CrossRef]
- Bejot, Y.; Duloquin, G.; Crespy, V.; Durier, J.; Garnier, L.; Graber, M.; Giroud, M. Influence of preexisting cognitive impairment on clinical severity of ischemic stroke: The Dijon stroke registry. Stroke 2020, 51, 1667–1673. [Google Scholar] [CrossRef]
- Busl, K.M.; Nogueira, R.G.; Yoo, A.J.; Hirsch, J.A.; Schwamm, L.H.; Rost, N.S. Prestroke dementia is associated with poor outcomes after reperfusion therapy among elderly stroke patients. J. Stroke Cerebrovasc. Dis. 2013, 22, 718–724. [Google Scholar] [CrossRef] [PubMed]
- Wouters, A.; Nysten, C.; Thijs, V.; Lemmens, R. Prediction of outcome in patients with acute ischemic stroke based on initial severity and improvement in the first 24 h. Front. Neurol. 2018, 9, 308. [Google Scholar] [CrossRef]
- Muruet, W.; Rudd, A.; Wolfe, C.D.A.; Douiri, A. Long-term survival after intravenous thrombolysis for ischemic stroke: A propensity score-matched cohort with up to 10-year follow-up. Stroke 2018, 49, 607–613. [Google Scholar] [CrossRef]
- Kwiatkowski, T.G.; Libman, R.B.; Frankel, M.; Tilley, B.C.; Morgenstern, L.B.; Lu, M.; Broderick, J.P.; Lewandowski, C.A.; Marler, J.R.; Levine, S.R.; et al. Effects of tissue plasminogen activator for acute ischemic stroke at one year. National institute of neurological disorders and stroke recombinant tissue plasminogen activator stroke study group. N. Engl. J. Med. 1999, 340, 1781–1787. [Google Scholar] [CrossRef]
- Multicentre Acute Stroke Trial—Italy (MAST-I) Group. Randomised controlled trial of streptokinase, aspirin, and combination of both in treatment of acute ischaemic stroke. Lancet 1995, 346, 1509–1514. [Google Scholar] [CrossRef]
- Muth, C.C. Long-term outcomes after thrombolytic therapy for acute ischemic stroke. JAMA 2020, 323, 2184–2185. [Google Scholar] [CrossRef] [PubMed]
- Gumbinger, C.; Ringleb, P.; Ippen, F.; Ungerer, M.; Reuter, B.; Bruder, I.; Daffertshofer, M.; Stock, C.; Stroke Working Group of B-W. Outcomes of patients with stroke treated with thrombolysis according to prestroke Rankin Scale scores. Neurology 2019, 93, e1834–e1843. [Google Scholar] [CrossRef] [PubMed]
- Caruso, P.; Ajcevic, M.; Furlanis, G.; Ridolfi, M.; Lugnan, C.; Cillotto, T.; Naccarato, M.; Manganotti, P. Thrombolysis safety and effectiveness in acute ischemic stroke patients with pre-morbid disability. J. Clin. Neurosci. 2020, 72, 180–184. [Google Scholar] [CrossRef] [PubMed]
- Quinn, T.J.; Dawson, J.; Walters, M.R.; Lees, K.R. Reliability of the modified Rankin Scale: A systematic review. Stroke 2009, 40, 3393–3395. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, G.; Chan, E.; Ambler, G.; Wilson, D.; Cipolotti, L.; Shakeshaft, C.; Cohen, H.; Yousry, T.; Salman, R.A.; Lip, G.Y.H.; et al. Cognitive impairment before atrial fibrillation-related ischemic events: Neuroimaging and prognostic associations. J. Am. Heart Assoc. 2020, 9, e014537. [Google Scholar] [CrossRef]
- De Reuck, J.L. The significance of small cerebral bleeds in neurodegenerative dementia syndromes. Aging Dis. 2012, 3, 307. [Google Scholar]
- Karaszewski, B.; Houlden, H.; Smith, E.E.; Markus, H.S.; Charidimou, A.; Levi, C.; Werring, D.J. What causes intracerebral bleeding after thrombolysis for acute ischaemic stroke? Recent insights into mechanisms and potential biomarkers. J. Neurol. Neurosurg. Psychiatry 2015, 86, 1127–1136. [Google Scholar] [CrossRef]
- Yang, W.S.; Li, Q.; Li, R.; Liu, Q.J.; Wang, X.C.; Zhao, L.B.; Xie, P. Defining the optimal midline shift threshold to predict poor outcome in patients with supratentorial spontaneous intracerebral hemorrhage. Neurocrit. Care 2018, 28, 314–321. [Google Scholar] [CrossRef]
- Zhang, J.; Yang, Y.; Sun, H.; Xing, Y. Hemorrhagic transformation after cerebral infarction: Current concepts and challenges. Ann. Transl. Med. 2014, 2, 81. [Google Scholar] [CrossRef]
- Saposnik, G.; Kapral, M.K.; Cote, R.; Rochon, P.A.; Wang, J.; Raptis, S.; Mamdani, M.; Black, S.E. Is pre-existing dementia an independent predictor of outcome after stroke? A propensity score-matched analysis. J. Neurol. 2012, 259, 2366–2375. [Google Scholar] [CrossRef] [PubMed]
- Murao, K.; Bodenant, M.; Cordonnier, C.; Bombois, S.; Henon, H.; Pasquier, F.; Bordet, R.; Leys, D. Does pre-existing cognitive impairment no-dementia influence the outcome of patients treated by intravenous thrombolysis for cerebral ischaemia? J. Neurol. Neurosurg Psychiatry 2013, 84, 1412–1414. [Google Scholar] [CrossRef] [PubMed]
- Murao, K.; Leys, D.; Jacquin, A.; Kitazono, T.; Bordet, R.; Béjot, Y.; Kimura, K.; Godefroy, O.; Wakisaka, Y.; Moulin, S.; et al. Thrombolytic therapy for stroke in patients with preexisting cognitive impairment. Neurology 2014, 82, 2048–2054. [Google Scholar] [CrossRef]
- Galluccio, F.; Walker, U.A.; Nihtyanova, S.; Moinzadeh, P.; Hunzelmann, N.; Krieg, T.; Steen, V.; Baron, M.; Sampaio-Barros, P.; Kayser, C.; et al. Registries in systemic sclerosis: A worldwide experience. Rheumatology 2010, 50, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Cestari, D.M.; Weine, D.M.; Panageas, K.S.; Segal, A.Z.; DeAngelis, L.M. Stroke in patients with cancer: Incidence and etiology. Neurology 2004, 62, 2025–2030. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Type of Cognitive Impairment | |
|---|---|
| Definite diagnosis of dementia | Recorded pre-stroke diagnosis of dementia |
| Definite diagnosis of mild cognitive impairment | Recorded pre-stroke diagnosis of mild cognitive impairment |
| Clinical evidence of cognitive impairment | Recorded pre-stroke cognitive scores: <80 in the Addenbrooke’s Cognitive Examination-Revised <25 in the Montreal Cognitive Assessment <25 in the Mini-Mental State Examination |
| Non-Cognitively Impaired (n = 366) | Cognitively Impaired (n = 62) | p-Value | |
|---|---|---|---|
| Age 1 | 76.0 (65.8–82.0) | 81.0 (76.0–90.0) | <0.001 * |
| Time taken to thrombolysis (min) 1 | 164.0 (128.5–210.0) | 181.5 (129.5–245.5) | 0.074 |
| Sex 2 | |||
| Male | 208 (56.8%) | 25 (40.3%) | 0.016 * |
| Female | 158 (43.2%) | 37 (59.7%) | 0.016 * |
| Thrombectomy 2 | 44 (12.0%) | 2 (3.2%) | 0.039 * |
| Stroke location 2 | |||
| Left MCA | 134 (36.6%) | 20 (32.3%) | 0.509 |
| Right MCA | 126 (34.4%) | 23 (37.1%) | 0.683 |
| Basilar | 3 (0.8%) | 1 (1.6%) | 0.548 |
| Other | 99 (27.0%) | 18 (29.0%) | 0.746 |
| Unknown | 4 (1.1%) | 0 | 0.408 |
| Cardiovascular comorbidity (any) 2 | 324 (88.5%) | 59 (95.2%) | 0.104 |
| New AF diagnosis | 46 (12.6%) | 7 (11.3%) | 0.778 |
| Pre-existing AF diagnosis | 51(13.9%) | 21 (33.9%) | <0.001 * |
| Hypertension | 195 (53.3%) | 32 (51.6%) | 0.808 |
| Previous MI | 69 (18.9%) | 16 (35.8%) | 0.204 |
| Previous stroke | 56 (15.3%) | 25 (40.3%) | <0.001 * |
| Previous TIA | 30 (8.2%) | 3 (4.8%) | 0.359 |
| Hyperlipidaemia | 73 (19.9%) | 10 (16.1%) | 0.482 |
| Non-smoker | 274 (74.9%) | 58 (93.5%) | 0.001 * |
| Ex-smoker | 42 (11.5%) | 3 (4.8%) | 0.115 |
| Current smoker | 50 (13.7%) | 1 (1.6%) | 0.007 * |
| Type 1 diabetes | 3 (0.8%) | 2 (3.2%) | 0.103 |
| Type 2 diabetes | 59 (16.1%) | 13 (21.0%) | 0.345 |
| Prediabetes | 3 (0.8%) | 0 | 0.474 |
| COPD | 37 (10.1%) | 7 (11.3%) | 0.777 |
| CKD | 39 (10.7%) | 12 (19.4%) | 0.054 |
| Non-Cognitively Impaired (n = 366) | Cognitively Impaired (n = 62) | p-Value | |
|---|---|---|---|
| Morbidity | |||
| NIHSS on admission 1 | 11.0 (6.0–17.8) | 15.0 (8.0–20.0) | 0.015 * |
| NIHSS post-treatment 1 | 6.0 (3.0–12.0) | 11.0 (6.0–19.0) | <0.001 * |
| NIHSS 24 h post-treatment 1 | 4.0.(1.0–10.0) | 8.0 (4.0–17.0) | <0.001 * |
| Pre-morbid mRS 1 | 1.00 (0.0–1.0) | 3.0 (2.0–3.0) | <0.001 * |
| Discharge mRS 1 | 2.5 (1.0–4.0) | 4.0 (3.0–6.0) | <0.001 * |
| Discharge location | |||
| Home 2 | 202 (55.2%) | 14 (22.6%) | <0.001 * |
| Secondary care facility 2 | 103 (28.1%) | 17 (27.4%) | 0.907 |
| Return to nursing home 2 | 8 (2.2%) | 11 (17.7%) | <0.001 * |
| New admission to nursing home 2 | 12 (3.3%) | 3 (4.8%) | 0.539 |
| Missing data 2 | 5 (1.4%) | 0 (0%) | 0.355 |
| Odds ratio | 95% CI | p-value | |
| Discharge mRS > 2 3 | 7.86 | 3.48–17.72 | <0.001 * |
| Discharge mRS ≥ 4 3 | 4.41 | 2.44–7.95 | <0.001 * |
| New discharge mRS ≥ 4 3 | 2.01 | 1.12–3.60 | 0.008 * |
| Post-treatment NIHSS improvement 3 | 0.57 | 0.31–1.06 | 0.074 |
| 24-h NIHSS improvement 3 | 0.48 | 0.24–0.95 | 0.035 * |
| Mortality | |||
| Time to death from thrombolysis (days) 2 | 70.0 (19.0–466.0) | 38.0 (10.5–277.5) | 0.214 |
| Death within admission 2 | 36 (9.8%) | 17 (27.4%) | <0.001 * |
| Odds ratio | 95% CI | p-value | |
| Death during admission 3 | 3.46 | 1.80–6.67 | <0.001 * |
| Death within 90 days 3 | 3.34 | 1.85–6.01 | <0.001 * |
| Haemorrhagic complication | |||
| Any haemorrhagic complication 2 | 57 (15.6%) | 14 (22.6%) | 0.176 |
| Asymptomatic 2 | 17 (4.6%) | 3 (4.8%) | 0.947 |
| Mild 2 | 17 (4.6%) | 3 (4.8%) | 0.947 |
| Severe 2 | 23 (6.3%) | 8 (12.9%) | 0.069 |
| Fatal 2 | 6 (1.6%) | 5 (8.1%) | 0.003 * |
| Haemorrhagic transformation contributing to death | 19 (5.2%) | 7 (11.3%) | 0.063 |
| Odds ratio | 95% CI | p-value | |
| Any haemorrhagic complication 3 | 1.58 | 0.82–3.05 | 0.176 |
| Severe 3 | 2.21 | 0.94–5.19 | 0.069 |
| Fatal 3 | 5.26 | 1.56–17.82 | 0.003 * |
| Haemorrhage contributing to death | 2.32 | 0.93–5.78 | 0.063 |
| R2 Nagelkerke | Odds Ratio § | 95% CI § | p-Value § | |
|---|---|---|---|---|
| Model 1: Cognitive Impairment | ||||
| Morbidity | ||||
| Post-treatment NIHSS improvement | 0.012 | 0.57 | 0.31–1.06 | 0.074 |
| 24 h NIHSS improvement | 0.019 | 0.48 | 0.24–0.95 | 0.035 * |
| New mRS ≥ 4 on discharge | 0.023 | 2.01 | 1.12–3.60 | 0.008 * |
| Mortality | ||||
| Death within admission | 0.054 | 3.46 | 1.80–6.67 | <0.001 * |
| Death within 90 days | 0.056 | 3.34 | 1.85–6.01 | <0.001 * |
| Haemorrhagic complication (any) | 0.007 | 1.58 | 0.82–3.05 | 0.176 |
| Severe haemorrhage | 0.017 | 2.21 | 0.94–5.19 | 0.069 |
| Fatal haemorrhage | 0.068 | 5.26 | 1.56–17.82 | 0.003 * |
| Haemorrhage contributing to death | 0.018 | 2.32 | 0.93–5.78 | 0.063 |
| Model 2: Factors significantly different between study groups | ||||
| Morbidity | ||||
| Post-treatment NIHSS improvement | 0.033 | 0.70 | 0.36–1.34 | 0.280 |
| 24 h NIHSS improvement | 0.070 | 0.58 | 0.28–1.20 | 0.143 |
| New mRS ≥ 4 on discharge | 0.160 | 1.21 | 0.67–2.20 | 0.531 |
| Mortality | ||||
| Death within admission | 0.184 | 1.91 | 0.93–3.93 | 0.080 |
| Death within 90 days | 0.260 | 1.56 | 0.82–3.09 | 0.171 |
| Haemorrhagic complication (any) | 0.048 | 1.28 | 0.63–2.59 | 0.489 |
| Severe haemorrhage | 0.031 | 1.91 | 0.76–4.81 | 0.168 |
| Fatal haemorrhage | 0.139 | 3.39 | 0.90–12.86 | 0.072 |
| Haemorrhage contributing to death | 0.074 | 1.39 | 0.52–3.70 | 0.509 |
| Model 3: Factors suspected to impact haemorrhagic complication | ||||
| Morbidity | ||||
| Post-treatment NIHSS improvement | 0.059 | 0.59 | 0.31–1.15 | 0.120 |
| 24 h NIHSS improvement | 0.058 | 0.64 | 0.31–1.31 | 0.219 |
| New mRS ≥ 4 on discharge | 0.240 | 1.33 | 0.73–2.43 | 0.357 |
| Mortality | ||||
| Death within admission | 0.260 | 2.21 | 1.07–4.58 | 0.033 * |
| Death within 90 days | 0.351 | 1.73 | 0.86–3.45 | 0.123 |
| Haemorrhagic complication (any) | 0.057 | 1.29 | 0.65–2.59 | 0.469 |
| Severe haemorrhage | 0.058 | 2.17 | 0.86–5.43 | 0.099 |
| Fatal haemorrhage | 0.170 | 4.79 | 1.24–18.45 | 0.023 * |
| Haemorrhage contributing to death | 0.152 | 1.61 | 0.60–4.30 | 0.340 |
| Model 2: Covariates Showing Significant Correlation | Model 3: Factors Suspected to Impact Haemorrhagic Complications | |||
|---|---|---|---|---|
| Covariates Showing Significant Correlation | R2 Nagelkerke | Covariates Showing Significant Correlation | R2 Nagelkerke | |
| Morbidity | ||||
| Post-treatment NIHSS improvement | No significant variables | 0.033 | Time to thrombolysis: OR 0.42, p = 0.019 | 0.059 |
| 24 h NIHSS improvement | Age: OR 0.96, p = 0.007 | 0.070 | Age: OR 0.97, p = 0.027 | 0.058 |
| New mRS ≥ 4 on discharge | Age: OR 1.05, p < 0.001 AF: OR 2.26, p = 0.001 | 0.160 | Age: OR 1.04, p < 0.011 Admission NIHSS > 6: OR 7.21, p < 0.001 | 0.240 |
| Mortality | ||||
| Death within admission | Age: OR 1.08, p < 0.001 AF: OR 1.96, p < 0.036 | 0.184 | Cognitive status: OR 2.21, p = 0.033 Age: OR 1.08, p < 0.001 Time to thrombolysis: OR 3.35, p = 0.031 Admission NIHSS > 6: OR 19.0, p = 0.004 | 0.260 |
| Death within 90 days admission | Age: OR 1.11, p < 0.001 Prev stroke/TIA: OR 2.07, p = 0.013 | 0.260 | Age: OR 1.11, p < 0.001 Time to thrombolysis: OR 3.85, p = 0.005 Admission NIHSS > 6: OR 16.9, p < 0.001 | 0.351 |
| Haemorrhagic complication (any) | Smoking: OR 0.43, p = 0.036 | 0.048 | Admission NIHSS > 6: OR 2.98, p = 0.006 | 0.057 |
| Severe haemorrhage | No significant variables | 0.031 | No significant variables | 0.058 |
| Fatal haemorrhage | No significant variables | 0.139 | Cognitive status: OR 4.79, p = 0.023 | 0.170 |
| Haemorrhage contributing to death | No significant variables | 0.074 | Age: OR 1.05, p = 0.046 | 0.152 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ramnarine, I.V.P.; Rasheed, O.W.; Laud, P.J.; Majid, A.; Harkness, K.A.; Bell, S.M. Thrombolysis Outcomes in Acute Ischaemic Stroke Patients with Pre-Existing Cognitive Impairment. Life 2023, 13, 1055. https://doi.org/10.3390/life13041055
Ramnarine IVP, Rasheed OW, Laud PJ, Majid A, Harkness KA, Bell SM. Thrombolysis Outcomes in Acute Ischaemic Stroke Patients with Pre-Existing Cognitive Impairment. Life. 2023; 13(4):1055. https://doi.org/10.3390/life13041055
Chicago/Turabian StyleRamnarine, Isabela V. P., Omar W. Rasheed, Peter J. Laud, Arshad Majid, Kirsty A. Harkness, and Simon M. Bell. 2023. "Thrombolysis Outcomes in Acute Ischaemic Stroke Patients with Pre-Existing Cognitive Impairment" Life 13, no. 4: 1055. https://doi.org/10.3390/life13041055