
Central Centrifugal Cicatricial Alopecia in the Adolescent Population: An Overview of Available Literature
Abstract
:1. Introduction
2. Epidemiology
3. Aetiology
4. Clinical Associations
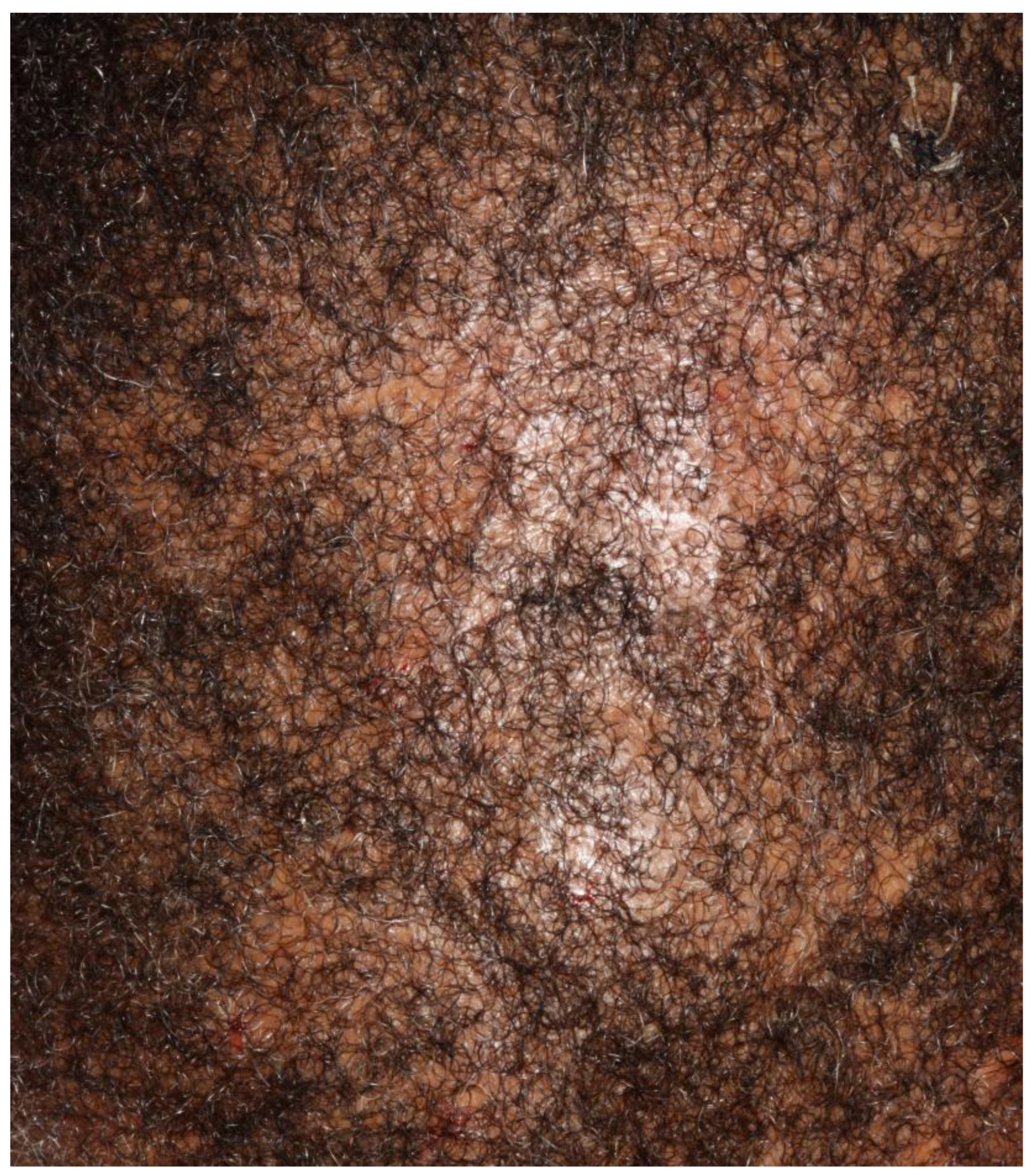
5. Presentation
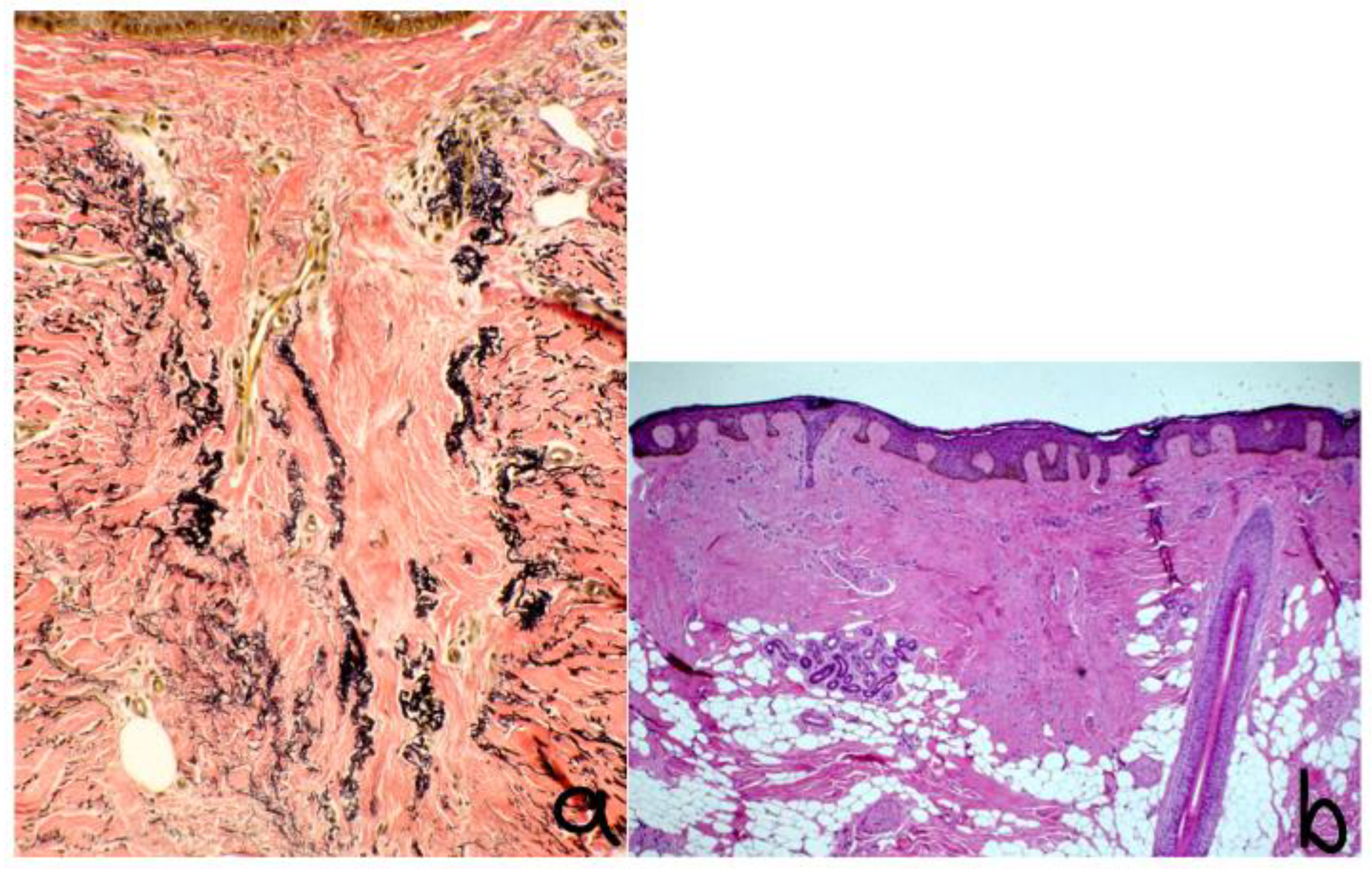
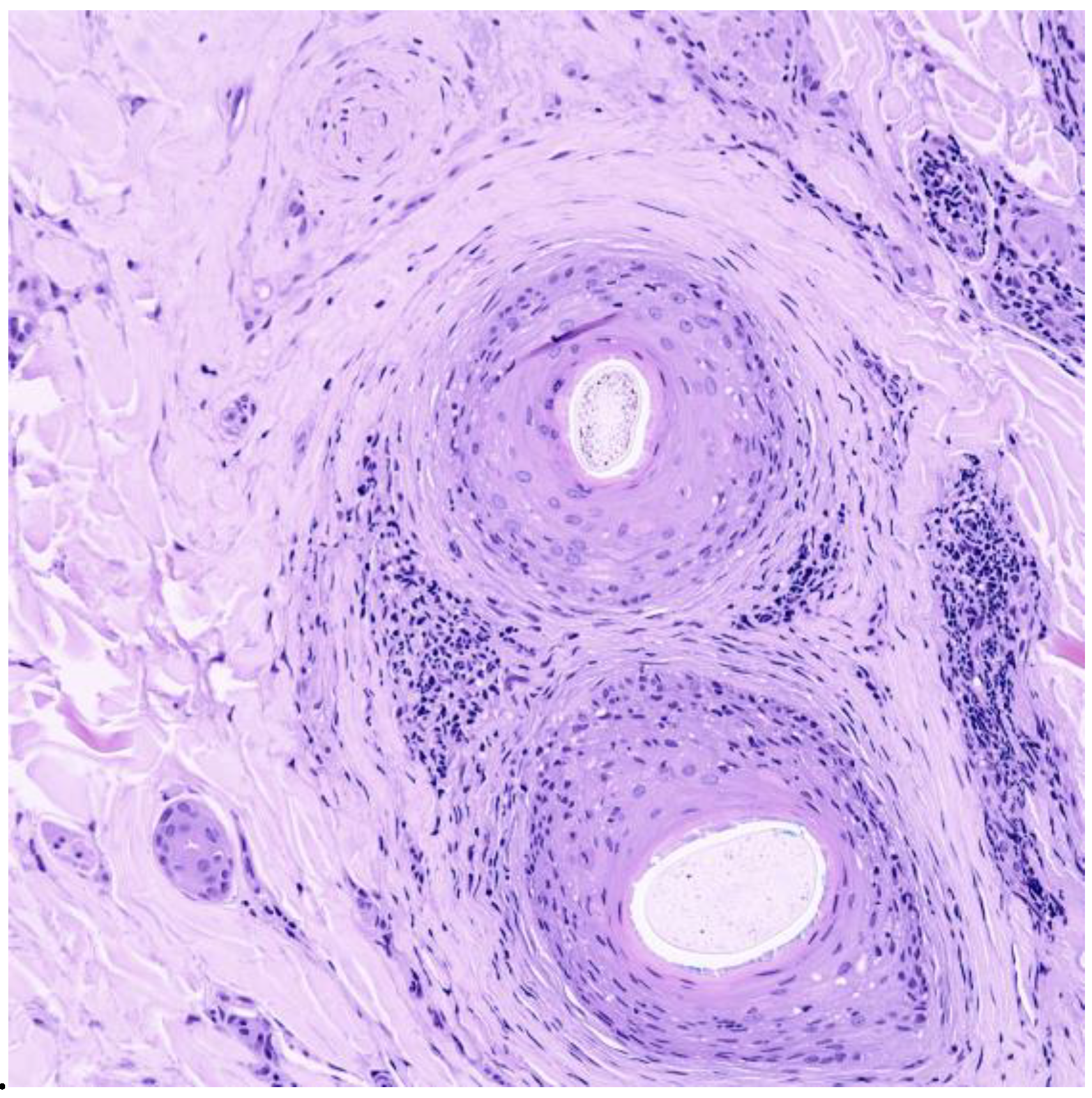
6. Histopathology and Dermoscopy
- Reduced follicular density with altered architecture because of absent or reduced and miniaturised sebaceous glands [16];
- Premature desquamation of the inner root sheath (very sensitive for CCCA, even in the absence of other findings) [16];
- Lamellar hyperkeratosis or parakeratosis [16];
- Naked hair shafts in the dermis [16];
- Follicular miniaturisation [16];
- Increased distance between affected follicles and small blood vessel clusters (BVCs; i.e., the perifollicular mucinous fibroplasia from chronic inflammation results in diminished blood supply [9].
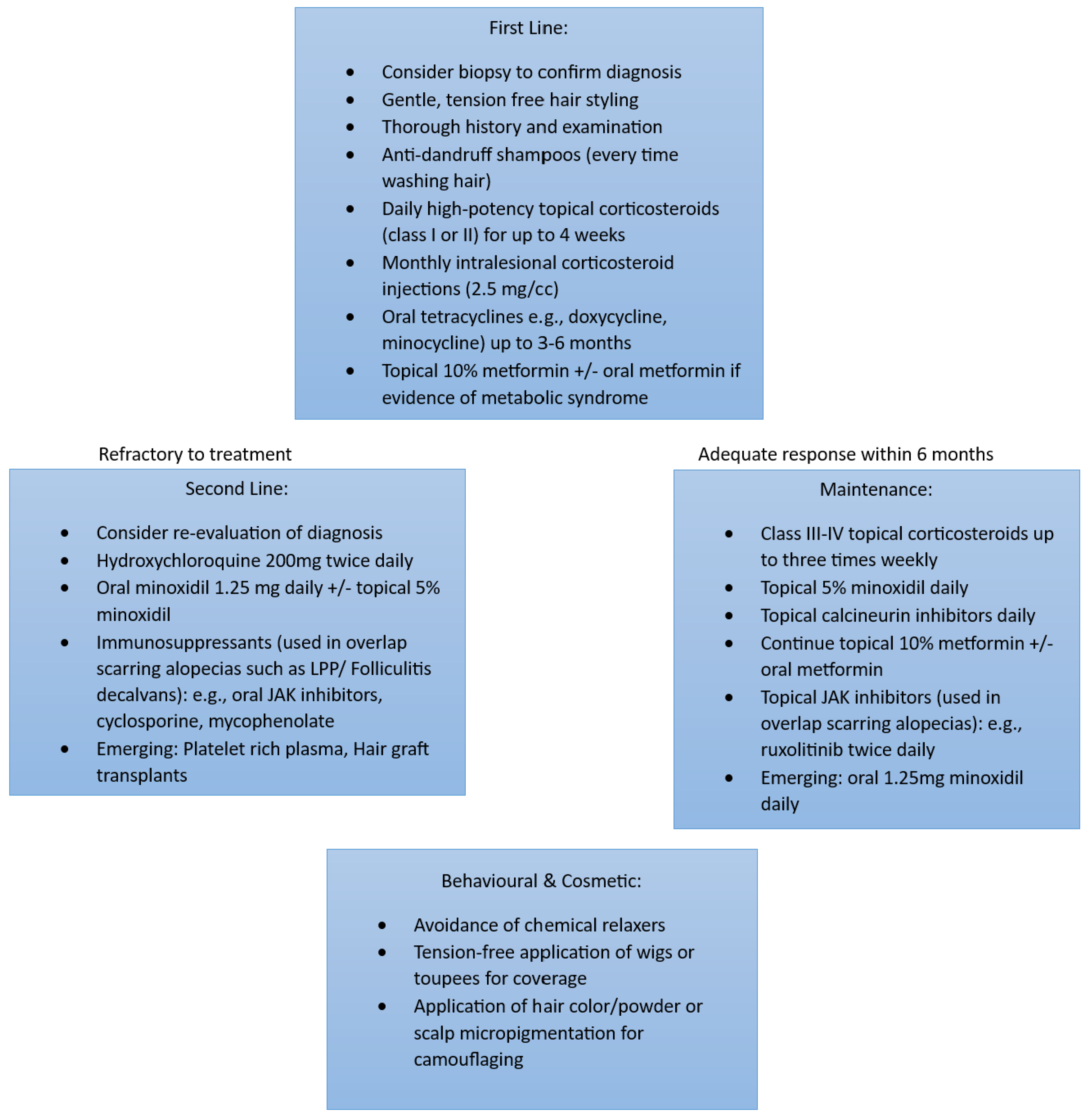
7. Management
8. Recommendations
9. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Taylor, S.C.; Kelly, A.P.; Lim, H.; Serrano, A.M. Taylor and Kelly’s Dermatology for Skin of Color 2/E; McGraw Hill Professional: New York, NY, USA, 2016. [Google Scholar]
- Mitchell, K.N.; Tay, Y.K.; Heath, C.R.; Trachtman, R.; Silverberg, N.B. Emerging issues in pediatric skin of color, part 1. Pediatr. Dermatol. 2021, 38, 20–29. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, L.J.; Castelo-Soccio, L.A. Alopecia: Kids are not just little people. Clin. Dermatol. 2015, 33, 622–630. [Google Scholar] [CrossRef] [PubMed]
- Olsen, E.A.; Callender, V.; McMichael, A.; Sperling, L.; Anstrom, K.J.; Shapiro, J.; Roberts, J.; Durden, F.; Whiting, D.; Bergfeld, W. Central hair loss in African American women: Incidence and potential risk factors. J. Am. Acad. Dermatol. 2011, 64, 245–252. [Google Scholar] [CrossRef] [PubMed]
- Funakoshi, Y.; Wang, Y.; Semba, T.; Masuda, H.; Hout, D.; Ueno, N.T.; Wang, X. Comparison of molecular profile in triple-negative inflammatory and non-inflammatory breast cancer not of mesenchymal stem-like subtype. PLoS ONE 2019, 14, e0222336. [Google Scholar] [CrossRef] [PubMed]
- Cheng, T.; Chen, P.; Chen, J.; Deng, Y.; Huang, C. Landscape analysis of matrix metalloproteinases unveils key prognostic markers for patients with breast cancer. Front. Genet. 2022, 12, 2769. [Google Scholar] [CrossRef]
- Roche, F.C.; Harris, J.; Ogunleye, T.; Taylor, S.C. Association of type 2 diabetes with central centrifugal cicatricial alopecia: A follow-up study. J. Am. Acad. Dermatol. 2022, 86, 661–662. [Google Scholar] [CrossRef] [PubMed]
- Sperling, L.C.; Cowper, S.E. The histopathology of primary cicatricial alopecia. Semin. Cutan. Med. Surg. 2006, 25, 41–50. [Google Scholar] [CrossRef]
- George, E.A.; Matthews, C.; Roche, F.C.; Taylor, S.C. Beyond the Hot Comb: Updates in Epidemiology, Pathogenesis, and Treatment of Central Centrifugal Cicatricial Alopecia from 2011 to 2021. Am. J. Clin. Dermatol. 2023, 24, 81–88. [Google Scholar] [CrossRef]
- Eginli, A.N.; Dlova, N.C.; McMichael, A. Central Centrifugal Cicatricial Alopecia in Children: A Case Series and Review of the Literature. Pediatr. Dermatol. 2017, 34, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Imhof, R.L.; Cantwell, H.M.; Proffer, S.L.; Tolkachjov, S.N.; Torgerson, R.R.; Tollefson, M.M. The spectrum of pediatric scarring alopecia: A retrospective review of 27 patients seen at Mayo Clinic. Pediatr. Dermatol. 2021, 38, 580–584. [Google Scholar] [CrossRef]
- Dlova, N.C.; Forder, M. Central centrifugal cicatricial alopecia: Possible familial aetiology in two African families from South Africa. Int. J. Dermatol. 2012, 51 (Suppl. S1), 17–20. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.K.; Alexis, A.F. Central centrifugal cicatricial alopecia: Retrospective chart review. J. Cutan. Med. Surg. 2010, 14, 212–222. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.C.; Gathers, R.C.; Callender, V.D.; Rodriguez, D.A.; Badreshia-Bansal, S. Treatments for Skin of Color E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2011. [Google Scholar]
- Lawson, C.N.; Bakayoko, A.; Callender, V.D. Central Centrifugal Cicatricial Alopecia: Challenges and Treatments. Dermatol. Clin. 2021, 39, 389–405. [Google Scholar] [CrossRef] [PubMed]
- Herskovitz, I.; Miteva, M. Central centrifugal cicatricial alopecia: Challenges and solutions. Clin. Cosmet. Investig. Dermatol. 2016, 9, 175–181. [Google Scholar] [CrossRef] [Green Version]
- Huang, C.; Wu, Z.; Du, Y.; Ogawa, R. The Epidemiology of Keloids. In Textbook on Scar Management; Téot, L., Mustoe, T.A., Middelkoop, E., Gauglitz, G.G., Eds.; Springer: Cham, Switzerland, 2020. [Google Scholar] [CrossRef]
- Jamerson, T.A.; Conover Talbot, C., Jr.; Dina, Y.; Kwatra, S.G.; Garza, L.A.; Aguh, C. Gene expression profiling suggests severe, extensive central centrifugal cicatricial alopecia may be both clinically and biologically distinct from limited disease subtypes. Exp. Dermatol. 2022, 31, 789–793. [Google Scholar] [CrossRef]
- Gathers, R.C.; Jankowski, M.; Eide, M.; Lim, H.W. Hair grooming practices and central centrifugal cicatricial alopecia. J. Am. Acad. Dermatol. 2009, 60, 574–578. [Google Scholar] [CrossRef] [PubMed]
- Khumalo, N.P.; Gumedze, F. Traction: Risk factor or coincidence in central centrifugal cicatricial alopecia? Br. J. Dermatol. 2012, 167, 1191–1193. [Google Scholar] [CrossRef] [PubMed]
- Whiting, D.A.; Olsen, E.A. Central centrifugal cicatricial alopecia. Dermatol. Ther. 2008, 21, 268–278. [Google Scholar] [CrossRef]
- Suchonwanit, P.; Hector, C.E.; Bin Saif, G.A.; McMichael, A.J. Factors afecting the severity of central centrifugal cicatricial alopecia. Int. J. Dermatol. 2016, 55, e338–e343. [Google Scholar] [CrossRef]
- Kyei, A.; Bergfeld, W.F.; Piliang, M.; Summers, P. Medical and environmental risk factors for the development of central centrifugal cicatricial alopecia: A population study. Arch. Dermatol. 2011, 147, 909–914. [Google Scholar] [CrossRef] [Green Version]
- Dina, Y.; Okoye, G.A.; Aguh, C. Association of Uterine Leiomyomas With Central Centrifugal Cicatricial Alopecia. JAMA Dermatol. 2018, 154, 213–214. [Google Scholar] [CrossRef] [PubMed]
- Brown-Korsah, J.B.; Roche, F.C.; Taylor, S.C. Association of breast and colorectal cancer in patients with central centrifugal cicatricial alopecia: A retrospective, cross-sectional pilot study. J. Am. Acad. Dermatol. 2021, 84, 859–860. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Surveillance, Epidemiology, and End Results Program (SEER) Database; National Cancer Institute: Bethesda, MD, USA, 2018.
- Ameen, M. Epidemiology of superficial fungal infections. Clin. Dermatol. 2010, 28, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Afifi, L.; Oparaugo, N.C.; Hogeling, M. Review of traction alopecia in the pediatric patient: Diagnosis, prevention, and management. Pediatr. Dermatol. 2021, 38, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Ayandibu, G.; Bergfeld, W. Retrospective cohort study to assess the prevalence of different factors of metabolic syndrome in central centrifugal cicatricial alopecia patients. J. Am. Acad. Dermatol. 2018, 79, AB246. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Scarring Alopecia | Symptoms | Distribution of Scalp Alopecia |
|---|---|---|
| Central Centrifugal Cicatricial Alopecia | Scalp pruritus, scaling, tender papules or pustules, asymptomatic | Vertex, frontal, parietal or patchy distribution |
| Folliculitis Decalvans | Follicular hyperkeratosis, tufting, pustules, scalp induration and atrophy, mild pain or discomfort | Vertex or patchy distribution |
| Lichen Planopilaris (LPP) | Single or multiple plaques with itching, stinging or burning | Classic LPP: Confluent random plaques FFA: Primarily frontotemporal involvement Lasseur-Graham-Little-Picardi: Patchy distribution |
| Aplasia Cutis Congenita | Asymptomatic; characterised by absence of skin | Primarily vertex involvement |
| Tina Capitis | Scalp pruritus, scaling, tender papules or pustules, asymptomatic | Patchy distribution |
| Morphea (Localised Scleroderma) | Erythematous patches or plaques with itching, tenderness or asymptomatic | Variable |
| Discoid Lupus Erythematosus | Scaling, erythematous annular plaques, asymptomatic | Variable |
| Dissecting Cellulitis | Painful nodules and abscesses, scaling | Variable |
| Keratosis Follicularis Spinulosa Decalvans | Keratotic follicular papules, atrophic depression | Variable |
| Study | Age at Time of Biopsy (Age at Onset of Symptoms) | Histopathologic Findings of Biopsy-Proven-CCCA |
|---|---|---|
| Dlova et al. [12] | 11 (No Data) | Perifollicular and perivascular lymphoid cell infiltrate with eccentric thinning of the follicular epithelium with concentric lamellar fibroplasia |
| Eginli et al. [10] | 14 (11) 15 (13) 16 (12) 17 (15) 19 (16) 19 (17) | Concentric perifollicular fibrosis and lymphocytes at the level of the infundibulum and isthmus |
| Shah et al. [13] | 18 (15–16) | Scarring, perifollicular fibrosis, fibrotic tracts, inflammatory infiltrate, few follicles |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palmer, V.; Valdebran, M. Central Centrifugal Cicatricial Alopecia in the Adolescent Population: An Overview of Available Literature. Life 2023, 13, 1022. https://doi.org/10.3390/life13041022
Palmer V, Valdebran M. Central Centrifugal Cicatricial Alopecia in the Adolescent Population: An Overview of Available Literature. Life. 2023; 13(4):1022. https://doi.org/10.3390/life13041022
Chicago/Turabian StylePalmer, Victoria, and Manuel Valdebran. 2023. "Central Centrifugal Cicatricial Alopecia in the Adolescent Population: An Overview of Available Literature" Life 13, no. 4: 1022. https://doi.org/10.3390/life13041022