
Understanding COVID: Collaborative Government Campaign for Citizen Digital Health Literacy in the COVID-19 Pandemic

 , , , ,
, , , ,
Abstract
:1. Introduction
1.1. COVID-19 Pandemic and Vulnerable Populations
1.2. Decision-Making in the COVID-19 Crisis and Public Health Strategies
1.3. The “Understanding COVID” Strategy
- Listen to citizens’ voices to redesign training actions, keeping in mind the suggestions from the community and acknowledging the difficulties and successes in carrying out the recommended protection measures against COVID-19.
- Search, simplify, and adapt in a more comprehensive way to the community all the information and evidence available to increase people’s protection against COVID-19.
- Promote accessible information on protection measures for citizens in general and for people with hearing or visual disabilities.
- Adapt digital health literacy (or (d)HL) to the particular needs of the population groups to which it is directed (adult population, young people, fathers and mothers, etc.).
- Design specific campaigns for sectors of activity that are particularly exposed, such as workers in poorly ventilated places and/or environments with a large influx of people.
- Work with children and adolescents to increase safety in the school environment.
1.4. Purpose of this Article
2. Design Phases and Preliminary Evaluation of the Implementation Process of the “Understanding COVID” Strategy
2.1. Hearing Citizen’s Voice
2.2. Informative Content
- Self-protection and collective protection measures against COVID-19: including frequent hand washing, interpersonal distance and coughing into the cubital fossa, use of masks, cleaning of domestic environments, collective protection measures and specific environments, and the disinfection of physical spaces.
- Identification and containment of the sources of contagion: early diagnosis of people with symptoms, isolation of cases and tracing and quarantine of close contacts. Therefore, it was important to publicize the symptoms and the protocols for reporting them (e.g., health personnel in the area).
- Content related to emotional management: assertiveness, managing emotions in difficult times, such as facing fear, leaving home after confinement, love, learning to trust, positive thinking, guided visualization, etc.
- Contents related to maintaining healthy habits: healthy diet, physical exercise, maintenance of routines, communication and sleep.
2.3. Digital Health Literacy
2.4. Communicative Materials and Accessibility of Information
2.4.1. Logo and Graphic Identity
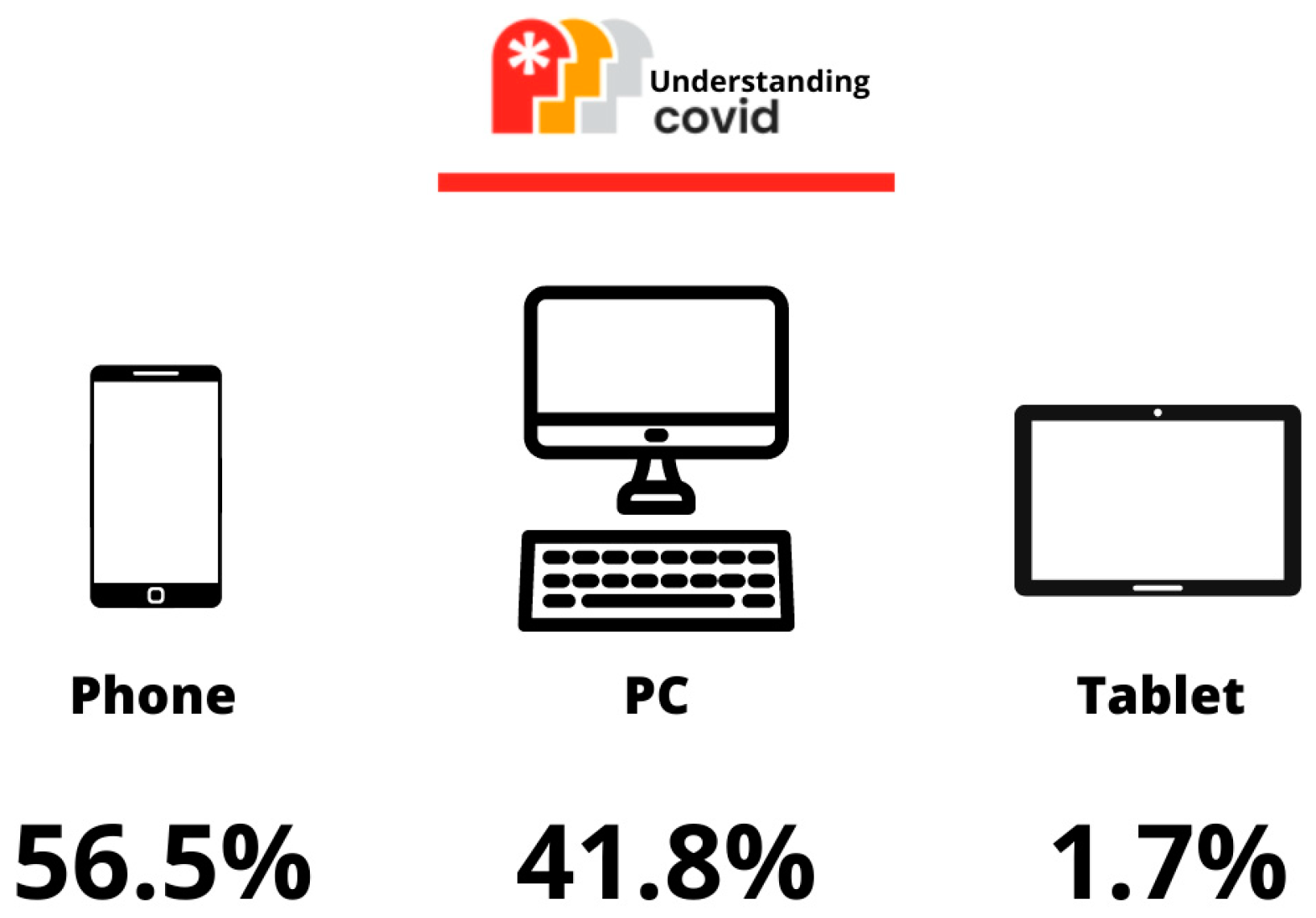
2.4.2. Web Page
- Didactic vocation: Present the information in an orderly, clear and attractive way. Carry out positive communication avoiding contributing to general pandemic fatigue.
- Usability: Simple and intuitive navigation. Increase click efficiency (relevant information in the minimum number of clicks). Prioritize information in plain text.
- Accessibility: Information intended for the whole of society. Visual codes are understandable by all. Its simple structure and adaptation for people with visual disabilities aim to increase the friendliness of its reading, as well as its possible use from mobile phones. Respect for the Accessibility Guidelines for WEB Content (WCAG).
2.4.3. Actions for the Child and Adolescent Population
2.4.4. Complementary Actions to Highly Exposed Workers/People
2.4.5. Other Dissemination Actions
3. Discussion
3.1. The “Understanding COVID” Strategy
3.2. Other Strategies and Campaigns
3.3. Lessons Learned and Limitations
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boletín Oficial del Principado de Asturias (BOPA) Acuerdo de 12 de marzo de 2020, del Consejo de Gobierno, sobre medidas preventivas y recomendaciones relacionadas con la infección del SARS CoV-2 (COVID-19). Available online: https://sede.asturias.es/bopa/2020/03/13/2020-02687.pdf (accessed on 18 February 2023).
- Khose, S.; Moore, J.X.; Wang, H.E. Epidemiology of the 2020 Pandemic of COVID-19 in the State of Texas: The First Month of Community Spread. J. Community Health 2020, 45, 696–701. [Google Scholar] [CrossRef] [PubMed]
- Lakhani, H.V.; Pillai, S.S.; Zehra, M.; Sharma, I.; Sodhi, K. Systematic Review of Clinical Insights into Novel Coronavirus (COVID-19) Pandemic: Persisting Challenges in U.S. Rural Population. Int. J. Environ. Res. Public Health 2020, 17, 4279. [Google Scholar] [CrossRef] [PubMed]
- Probst, J.C.; Crouch, E.L.; Eberth, J.M. COVID-19 risk mitigation behaviors among rural and urban community-dwelling older adults in summer, 2020. J. Rural. Health 2021, 37, 473–478. [Google Scholar] [CrossRef]
- Greer, M.L.; Sample, S.; Jensen, H.K.; McBain, S.; Lipschitz, R.; Sexton, K.W. COVID-19 Is Connected with Lower Health Literacy in Rural Areas. Stud. Health Technol. Inform. 2021, 281, 804–808. [Google Scholar] [CrossRef] [PubMed]
- Schippers, M.C.; Rus, D.C. Optimizing Decision-Making Processes in Times of COVID-19: Using Reflexivity to Counteract Information-Processing Failures. Front. Psychol. 2021, 12, 650525. [Google Scholar] [CrossRef]
- Groot, G.; Witham, S.; Badea, A.; Baer, S.; Dalidowicz, M.; Reeder, B.; Froh, J.; Carr, T. Evaluating a learning health system initiative: Lessons learned during COVID-19 in Saskatchewan, Canada. Learn. Health Syst. 2022, e10350. [Google Scholar] [CrossRef]
- Ghoushchi, S.J.; Bonab, S.R.; Ghiaci, A.M. A decision-making framework for COVID-19 infodemic management strategies evaluation in spherical fuzzy environment. Stoch. Environ. Res. Risk Assess. 2023. online early publication. [Google Scholar] [CrossRef]
- Mistry, S.K.; Shaw, M.; Raffan, F.; Johnson, G.; Perren, K.; Shoko, S.; Harris-Roxas, B.; Haigh, F. Inequity in Access and Delivery of Virtual Care Interventions: A Scoping Review. Int. J. Environ. Res. Public Health 2022, 19, 9411. [Google Scholar] [CrossRef]
- World Health Organization. Regional Office for Europe Pandemic Fatigue: Reinvigorating the Public to Prevent COVID-19: Policy Framework for Supporting Pandemic Prevention and Management: Revised Version November 2020; World Health Organization. Regional Office for Europe: Copenhagen, Denmark, 2020. [Google Scholar]
- Consejería de Presidencia y Participación Ciudadana Plan demográfico del Principado de Asturias 2017–2027. Available online: https://www.age-geografia.es/site/wp-content/uploads/2017/10/Plan-Demogr%C3%A1fico-Asturias-2017-2027.pdf (accessed on 10 December 2022).
- Sudhira, H.; Ramachandra, T.; Jagadish, K. Urban sprawl: Metrics, dynamics and modelling using GIS. Int. J. Appl. Earth Obs. Geoinf. 2004, 5, 29–39. [Google Scholar] [CrossRef]
- Brubacher, L.J.; Hasan, Z.; Sriram, V.; Keidar, S.; Wu, A.; Cheng, M.; Lovato, C.Y.; Berman, P.; U. B. C. Working Group on Health Systems. Response to COVID-19 Investigating the influence of institutions, politics, organizations, and governance on the COVID-19 response in British Columbia, Canada: A jurisdictional case study protocol. Health Res. Policy Syst. 2022, 20, 74. [Google Scholar] [CrossRef]
- Jefatura del Estado Ley Orgánica 3/2018, de 5 de diciembre, de Protección de Datos Personales y garantía de los derechos digitales. Available online: https://www.boe.es/eli/es/lo/2018/12/05/3 (accessed on 11 December 2022).
- Woodrow, N.; Fairbrother, H.; D’Apice, K.; Breheny, K.; Albers, P.; Mills, C.; Tebbett, S.; Campbell, R.; De Vocht, F. Exploring the Potential of a School-Based Online Health and Wellbeing Screening Tool: Young People’s Perspectives. Int. J. Environ. Res. Public Health 2022, 19, 4062. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, M. Open schools! Weighing the effects of viruses and lockdowns on children. Trends Neurosci. Educ. 2021, 22, 100151. [Google Scholar] [CrossRef] [PubMed]
- Odone, A.; Bricchi, L.; Signorelli, C. COVID-19 Control School-Based Interventions: Characteristics and Impact of a Nation-al-Level Educational Programme in Italy. Acta Biomed. 2022, 92, e2021495. [Google Scholar] [CrossRef] [PubMed]
- Barcenilla-Guitard, M.; Espart, A. Influence of Gender, Age and Field of Study on Hand Hygiene in Young Adults: A Cross-Sectional Study in the COVID-19 Pandemic Context. Int. J. Environ. Res. Public Health 2021, 18, 13016. [Google Scholar] [CrossRef] [PubMed]
- Hefferon, C.; Taylor, C.; Bennett, D.; Falconer, C.; Campbell, M.; Williams, J.G.; Schwartz, D.; Kipping, R.; Taylor-Robinson, D. Priorities for the child public health response to the COVID-19 pandemic recovery in England. Arch. Dis. Child. 2020, 106, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Amran, M.S.; Jamaludin, K.A. The Impact of Unplanned School Closures on Adolescent Behavioral Health During the COVID-19 Pandemic in Malaysia. Front. Public Health 2021, 9, 639041. [Google Scholar] [CrossRef]
- Almoslem, M.M.; Alshehri, T.A.; Althumairi, A.A.; Aljassim, M.T.; Hassan, M.E.; Berekaa, M.M. Handwashing Knowledge, Attitudes, and Practices among Students in Eastern Province Schools, Saudi Arabia. J. Environ. Public Health 2021, 2021, 6638443. [Google Scholar] [CrossRef]
- Sugita, E.W. Water, Sanitation and Hygiene (WASH) in Japanese elementary schools: Current conditions and practices. Pediatr. Int. 2021, 64, e15062. [Google Scholar] [CrossRef]
- Rohwer, E.; Mojtahedzadeh, N.; Neumann, F.A.; Nienhaus, A.; Augustin, M.; Harth, V.; Zyriax, B.-C.; Mache, S. The Role of Health Literacy among Outpatient Caregivers during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 11743. [Google Scholar] [CrossRef]
- Pham, Q.; El-Dassouki, N.; Lohani, R.; Jebanesan, A.; Young, K. The Future of Virtual Care for Older Ethnic Adults Beyond the COVID-19 Pandemic. J. Med. Internet Res. 2022, 24, e29876. [Google Scholar] [CrossRef]
- Zenone, M.A.; Cianfrone, M.; Sharma, R.; Majid, S.; Rakhra, J.; Cruz, K.; Costales, S.; Sekhon, M.; Mathias, S.; Tugwell, A.; et al. Supporting youth 12–24 during the COVID-19 pandemic: How Foundry is mobilizing to provide information, resources and hope across the province of British Columbia. Glob. Health Promot. 2021, 28, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Leader, A.E.; Capparella, L.M.; Waldman, L.B.; Cammy, R.B.; Petok, A.R.; Dean, R.; Shimada, A.; Yocavitch, L.; Rising, K.L.; Garber, G.D.; et al. Digital Literacy at an Urban Cancer Center: Implications for Technology Use and Vulnerable Patients. Kimmel Cancer Center Faculty Papers JCO Clin. Cancer Inform. 2021, 5, 872–880. [Google Scholar] [CrossRef]
- Alford-Teaster, J.; Wang, F.; Tosteson, A.N.A.; Onega, T. Incorporating broadband durability in measuring geographic access to health care in the era of telehealth: A case example of the 2-step virtual catchment area (2SVCA) Method. J. Am. Med. Inform. Assoc. 2021, 28, 2526–2530. [Google Scholar] [CrossRef] [PubMed]
- Malkin, M.; Mickler, A.K.; Ajibade, T.O.; Coppola, A.; Demise, E.; Derera, E.; Ede, J.O.; Gallagher, M.; Gumbo, L.; Jakopo, Z.; et al. Adapting High Impact Practices in Family Planning During the COVID-19 Pandemic: Experiences From Kenya, Nigeria, and Zimbabwe. Glob. Health Sci. Pract. 2022, 10, e2200064. [Google Scholar] [CrossRef]
- Gray, D.J.; Kurscheid, J.; Mationg, M.L.; Williams, G.M.; Gordon, C.; Kelly, M.; Wangdi, K.; McManus, D.P. Health-education to prevent COVID-19 in schoolchildren: A call to action. Infect. Dis. Poverty 2020, 9, 142–144. [Google Scholar] [CrossRef]
- Fetzer, T. Subsidising the spread of COVID-19: Evidence from the UK’S Eat-Out-to-Help-Out Scheme*. Econ. J. 2021, 132, 1200–1217. [Google Scholar] [CrossRef]
- Tamura, M.; Suzuki, S.; Yamaguchi, Y. Effects of tourism promotion on COVID-19 spread: The case of the “Go To Travel” campaign in Japan. J. Transp. Health 2022, 26, 101407. [Google Scholar] [CrossRef]
- Argyris, Y.A.; Nelson, V.R.; Wiseley, K.; Shen, R.; Roscizewski, A. Do social media campaigns foster vaccination adherence? A systematic review of prior intervention-based campaigns on social media. Telemat. Inform. 2023, 76, 101918. [Google Scholar] [CrossRef]
- Puzio, D.; Makowska, I.; Rymarczyk, K. Raising the Child—Do Screen Media Help or Hinder? The Quality over Quantity Hypothesis. Int. J. Environ. Res. Public Health 2022, 19, 9880. [Google Scholar] [CrossRef] [PubMed]
- Bhyat, R.; Hagens, S.; Bryski, K.; Kohlmaier, J.F. Digital Health Value Realization through Active Change Efforts. Front. Public Health 2021, 9, 741424. [Google Scholar] [CrossRef] [PubMed]
- Linardon, J.; Westrupp, E.M.; Macdonald, J.A.; Mikocka-Walus, A.; Stokes, M.A.; Greenwood, C.J.; Youssef, G.J.; Teague, S.; Hutchinson, D.; Sciberras, E.; et al. Monitoring Australian parents’ shifting receptiveness to digital mental health interventions during the COVID-19 pandemic. Aust. N. Z. J. Psychiatry 2021, 56, 1503–1514. [Google Scholar] [CrossRef] [PubMed]
- Vamos, S.D.; McDermott, R.J. Rebranding School Health: The Power of Education for Health Literacy. J. Sch. Health 2021, 91, 670–676. [Google Scholar] [CrossRef] [PubMed]
- Mörelius, E.; Robinson, S.; Arabiat, D.; Whitehead, L. Digital Interventions to Improve Health Literacy among Parents of Children Aged 0 to 12 Years with a Health Condition: Systematic Review. J. Med. Internet Res. 2021, 23, e31665. [Google Scholar] [CrossRef] [PubMed]
- Santoveña-Casal, S.; Gil-Quintana, J.; Ramos, L. Digital citizens’ feelings in national #COVID 19 campaigns in Spain. Heliyon 2021, 7, e08112. [Google Scholar] [CrossRef] [PubMed]
- Santoveña-Casal, S.; Pérez, M.D.F. Relevance of E-Participation in the state health campaign in Spain: #EstoNoEsUnJuego/#ThisIsNotAGame. Technol. Soc. 2022, 68, 101877. [Google Scholar] [CrossRef] [PubMed]
- Graffigna, G.; Bosio, C.; Savarese, M.; Barello, M.; Barello, S. “#I-Am-Engaged”: Conceptualization and First Implementation of a Multi-Actor Participatory, Co-designed Social Media Campaign to Raise Italians Citizens’ Engagement in Preventing the Spread of COVID-19 Virus. Front. Psychol. 2020, 11, 567101. [Google Scholar] [CrossRef] [PubMed]
- Silesky, M.D.; Panchal, D.; Fields, M.; Peña, A.S.; Diez, M.; Magdaleno, A.; Frausto-Rodriguez, P.; Bonnevie, E. A Multifaceted Campaign to Combat COVID-19 Misinformation in the Hispanic Community. J. Community Health 2022. Online early publication. [Google Scholar] [CrossRef]
- Miller, A.F.; Yang, C.; Grieb, S.M.; Lipke, M.; Bigelow, B.F.; Phillips, K.H.; Palomino, P.; Page, K.R. A Community-Engaged Social Marketing Campaign to Promote Equitable Access to COVID-19 Services among Latino Immigrants. Am. J. Public Health 2023, 113, e1–e4. [Google Scholar] [CrossRef]
- Marcell, L.; Dokania, E.; Navia, I.; Baxter, C.; Crary, I.; Rutz, S.; Monteverde, M.J.S.; Simlai, S.; Hernandez, C.; Huebner, E.M.; et al. One Vax Two Lives: A social media campaign and research program to address COVID-19 vaccine hesitancy in pregnancy. Am. J. Obstet. Gynecol. 2022, 227, 685–695.e2. [Google Scholar] [CrossRef]
- Ioannides, S.; Hess, I.; Lamberton, C.; Luisi, B. Engaging with culturally and linguistically diverse communities during a COVID-19 outbreak: A NSW Health interagency public health campaign. Public Health Res. Pract. 2022. [Google Scholar] [CrossRef]
- Park, S.; Oh, S. Factors associated with preventive behaviors for COVID-19 among adolescents in South Korea. J. Pediatr. Nurs. 2021, 62, e69–e76. [Google Scholar] [CrossRef] [PubMed]
- Luo, L.; Zeng, X.; Wu, Y.; An, F.; Huang, J.; Yang, H.; Jiang, Q.; Ou, Q.; Du, J.; Song, N. Influencing Factors of Students Aged 10–20 Non-participating in Home Physical Exercise During the COVID-19 Isolation Policy Period: A Cross-Sectional Study From China. Front. Public Health 2022, 10, 787857. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.; Yuan, Y.; Wang, D. Analysis of mental health status and influencing factors of College Students under the epidemic of novel coronavirus pneumonia. J. South. Med. Univ. 2020, 2, 171–176. [Google Scholar] [CrossRef]
- Shen, X.; Li, Y.; Feng, J.; Lu, Z.; Tian, K.; Gan, Y. Current status and associated factors of psychological resilience among the Chinese residents during the coronavirus disease 2019 pandemic. Int. J. Soc. Psychiatry 2020, 68, 34–43. [Google Scholar] [CrossRef]
- Almansour, A.; Hussein, S.M.; Felemban, S.G.; Mahamid, A.W. Acceptance and hesitancy of parents to vaccinate children against coronavirus disease 2019 in Saudi Arabia. PLoS ONE 2022, 17, e0276183. [Google Scholar] [CrossRef]
- Fedele, F.; Aria, M.; Esposito, V.; Micillo, M.; Cecere, G.; Spano, M.; De Marco, G. COVID-19 vaccine hesitancy: A survey in a population highly compliant to common vaccinations. Hum. Vaccines Immunother. 2021, 17, 3348–3354. [Google Scholar] [CrossRef]
- Zhang, M.-X.; Lin, X.-Q.; Chen, Y.; Tung, T.-H.; Zhu, J.-S. Determinants of parental hesitancy to vaccinate their children against COVID-19 in China. Expert Rev. Vaccines 2021, 20, 1339–1349. [Google Scholar] [CrossRef]
- Lubis, T.A.; Gunardi, H.; Soedjatmiko, S.; Satari, H.I.; Alatas, F.S.; Pulungan, A.B. Educational videos to address vaccine hesitancy in childhood immunization. Vaccine 2022, 40, 5965–5970. [Google Scholar] [CrossRef]
- Ngandjon, J.K.; Ostermann, T.; Kenmoue, V.; Laengler, A. Insights into Predictors of Vaccine Hesitancy and Promoting Factors in Childhood Immunization Programs—A Cross-Sectional Survey in Cameroon. Int. J. Environ. Res. Public Health 2022, 19, 2721. [Google Scholar] [CrossRef]
- Huang, L.-L.; Yang, Y.-P.; Mao, H.-P.; Hu, W.-W.; Jiang, Y.-H.; Jiesisibieke, Z.L.; Tung, T.-H. Parental hesitancy towards vaccinating their children with a booster dose against COVID-19: Real-world evidence from Taizhou, China. J. Infect. Public Health 2022, 15, 1006–1012. [Google Scholar] [CrossRef]
- Xu, Y.; Zhang, R.; Zhou, Z.; Fan, J.; Liang, J.; Cai, L.; Peng, L.; Ren, F.; Lin, W. Parental psychological distress and attitudes towards COVID-19 vaccination: A cross-sectional survey in Shenzhen, China. J. Affect. Disord. 2021, 292, 552–558. [Google Scholar] [CrossRef] [PubMed]
- Altulahi, N.; AlNujaim, S.; Alabdulqader, A.; Alkharashi, A.; AlMalki, A.; AlSiari, F.; Bashawri, Y.; Alsubaie, S.; AlShahrani, D.; AlGoraini, Y. Willingness, beliefs, and barriers regarding the COVID-19 vaccine in Saudi Arabia: A multiregional cross-sectional study. BMC Fam. Pract. 2021, 22, 247. [Google Scholar] [CrossRef] [PubMed]
- Microsoft Power BI. Available online: https://app.powerbi.com/view?r=eyJrIjoiNTdhYzlhYjUtZmFjNi00NjBhLThiNTktMmNjNDY5NzYzNjBlIiwidCI6IjI4ZmI0NmYwLTU0OWYtNDI5Ny1iOTZmLWFjNjJhZTkxY2YwYyIsImMiOjl9&pageName=ReportSectionda82d8ffb60be1590dd8 (accessed on 4 November 2022).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Question | Likert Scale * | |||||
|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | 5 | |
| 0% | 2% | 2% | 2% | 9% | 84% |
| 5% | 3% | 7% | 9% | 11% | 65% |
| 0% | 2% | 2% | 3% | 13% | 80% |
| 0% | 1% | 4% | 4% | 12% | 79% |
| 1% | 2% | 2% | 4% | 11% | 80% |
| 0% | 2% | 1% | 5% | 10% | 82% |
| Questions | Options |
|---|---|
| 6-item Likert scale 0 = not useful 5 = very useful |
| yes/no/don’t know |
| 6-item Likert scale 0 = little accessible 5 = very accessible |
| 11-item Likert scale 0 = no satisfaction 10 = very satisfied |
| Open-ended question |
| Open-ended question |
| Open-ended question |
| Type of Training | Usefulness (Likert) | Time | Accessibility (Likert) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | 5 | Yes | No | Don’t Know | 0 | 1 | 2 | 3 | 4 | 5 | |
| Families associations | 0% | 0% | 0% | 0% | 22% | 78% | 97% | 0% | 3% | 0% | 0% | 0% | 2% | 15% | 83% |
| Secondary schools | 0% | 0% | 0% | 0% | 14% | 86% | 100% | 0% | 0% | 0% | 0% | 0% | 0% | 14% | 86% |
| Drop by Drop | 0% | 0% | 0% | 4% | 18% | 77% | 95% | 1% | 4% | 0% | 0% | 0% | 2% | 15% | 83% |
| First Quality Air | 0% | 0% | 0% | 3% | 10% | 88% | 95% | 5% | 0% | 0% | 0% | 0% | 0% | 20% | 80% |
| Type of Training | Satisfaction (Likert) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
| Families associations | 0% | 0% | 0% | 0% | 0% | 0% | 2% | 6% | 9% | 34% | 49% |
| Secondary schools | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 4% | 11% | 86% |
| Drop by Drop | 0% | 0% | 0% | 0% | 0% | 0% | 1% | 2% | 2% | 5% | 89% |
| First Quality Air | 0% | 0% | 0% | 0% | 0% | 0% | 0% | 5% | 5% | 5% | 85% |
| Group /Environment | Specific Populations |
|---|---|
| Citizenship | Citizens in rural areas |
| Citizens in urban areas | |
| Municipal technical professionals | |
| Ethnic minorities: Roma, Immigrants | |
| Citizens with impaired vision | |
| Citizens with impaired hearing | |
| Associations of people with mental health problems or addictions | |
| Non-professional caregivers | |
| School environment | School-age students (6–12 years old) |
| Secondary education and vocational training students (12–18 years) | |
| Families with school-age children ages 6–12 years | |
| Families Association of students aged 3 to 16 years according to educational levels of public and private centers and special education | |
| Professional sector | Professionals from shelters |
| Home caregiving professionals | |
| Non-professional caregivers | |
| Risk prevention services | |
| Hostelry | |
| Tourism | |
| Small business | |
| Religious groups |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López-Ventoso, M.; Pisano González, M.; Fernández García, C.; Diez Valcarce, I.; Rey Hidalgo, I.; Rodríguez Nachón, M.J.; Menéndez García, A.M.; Perello, M.; Avagnina, B.; Zanutto, O.; et al. Understanding COVID: Collaborative Government Campaign for Citizen Digital Health Literacy in the COVID-19 Pandemic. Life 2023, 13, 589. https://doi.org/10.3390/life13020589
López-Ventoso M, Pisano González M, Fernández García C, Diez Valcarce I, Rey Hidalgo I, Rodríguez Nachón MJ, Menéndez García AM, Perello M, Avagnina B, Zanutto O, et al. Understanding COVID: Collaborative Government Campaign for Citizen Digital Health Literacy in the COVID-19 Pandemic. Life. 2023; 13(2):589. https://doi.org/10.3390/life13020589
Chicago/Turabian StyleLópez-Ventoso, Mónica, Marta Pisano González, Cristina Fernández García, Isabel Diez Valcarce, Inés Rey Hidalgo, María Jesús Rodríguez Nachón, Ana María Menéndez García, Michelle Perello, Beatrice Avagnina, Oscar Zanutto, and et al. 2023. "Understanding COVID: Collaborative Government Campaign for Citizen Digital Health Literacy in the COVID-19 Pandemic" Life 13, no. 2: 589. https://doi.org/10.3390/life13020589