
Assessing the Suitability of a Virtual ‘Pink Warrior’ for Older Breast Cancer Survivors during COVID-19: A Pilot Study
 , ,
, ,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
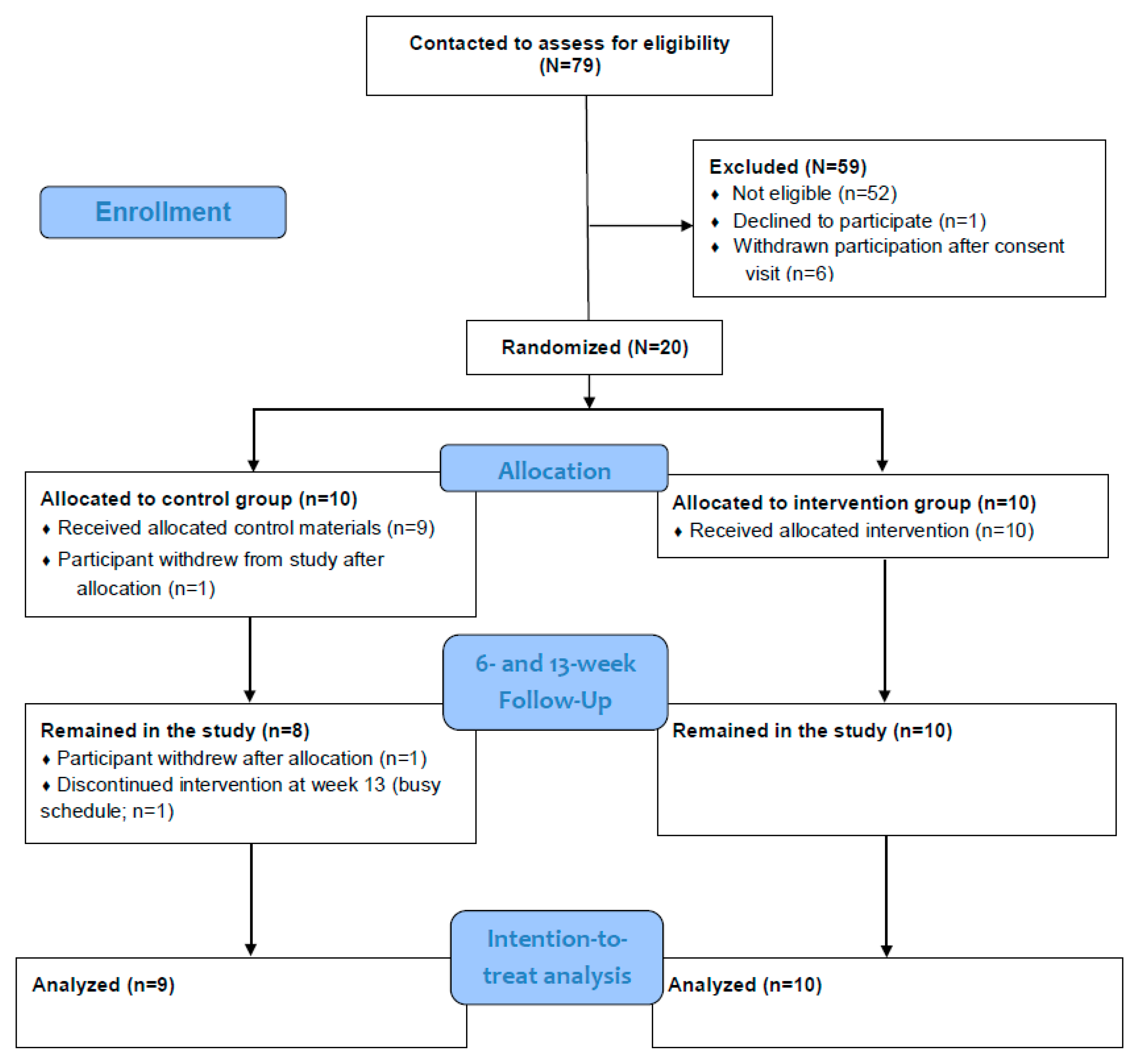
2.1. Participants
2.2. Randomization
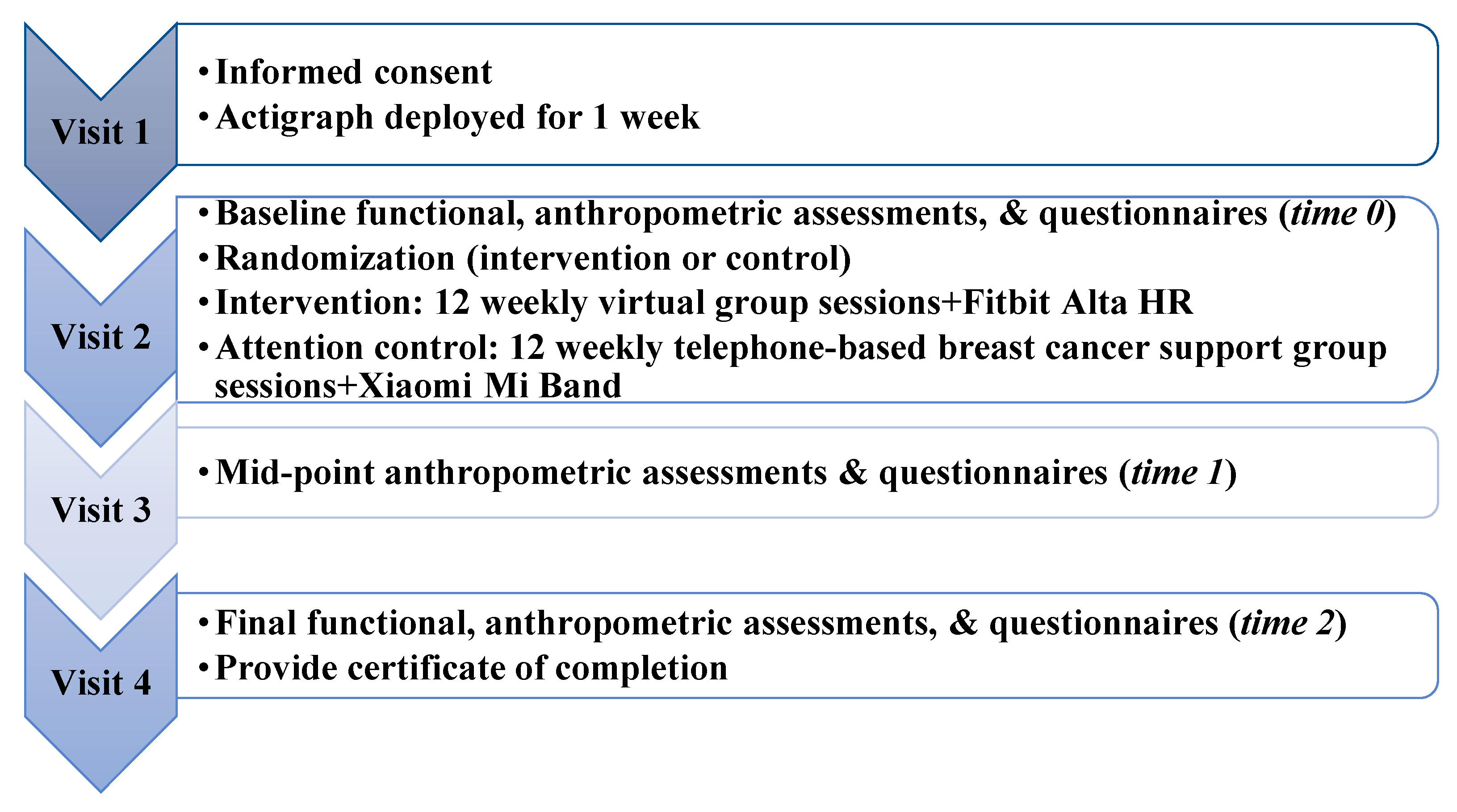
2.3. Procedures
2.4. Ethics Approval
2.5. Intervention
2.6. Attention Control Group
2.7. Primary Outcome Measures
2.7.1. Feasibility
2.7.2. Acceptability
2.8. Secondary Outcome Measures
2.8.1. Objective Physical Function Measures
2.8.2. Physical Activity Measures
2.8.3. Other Patient Reported Measures
2.9. Statistical Analysis
3. Results
3.1. Participants’ Characteristics
3.2. Feasibility and Acceptability
3.2.1. Feasibility
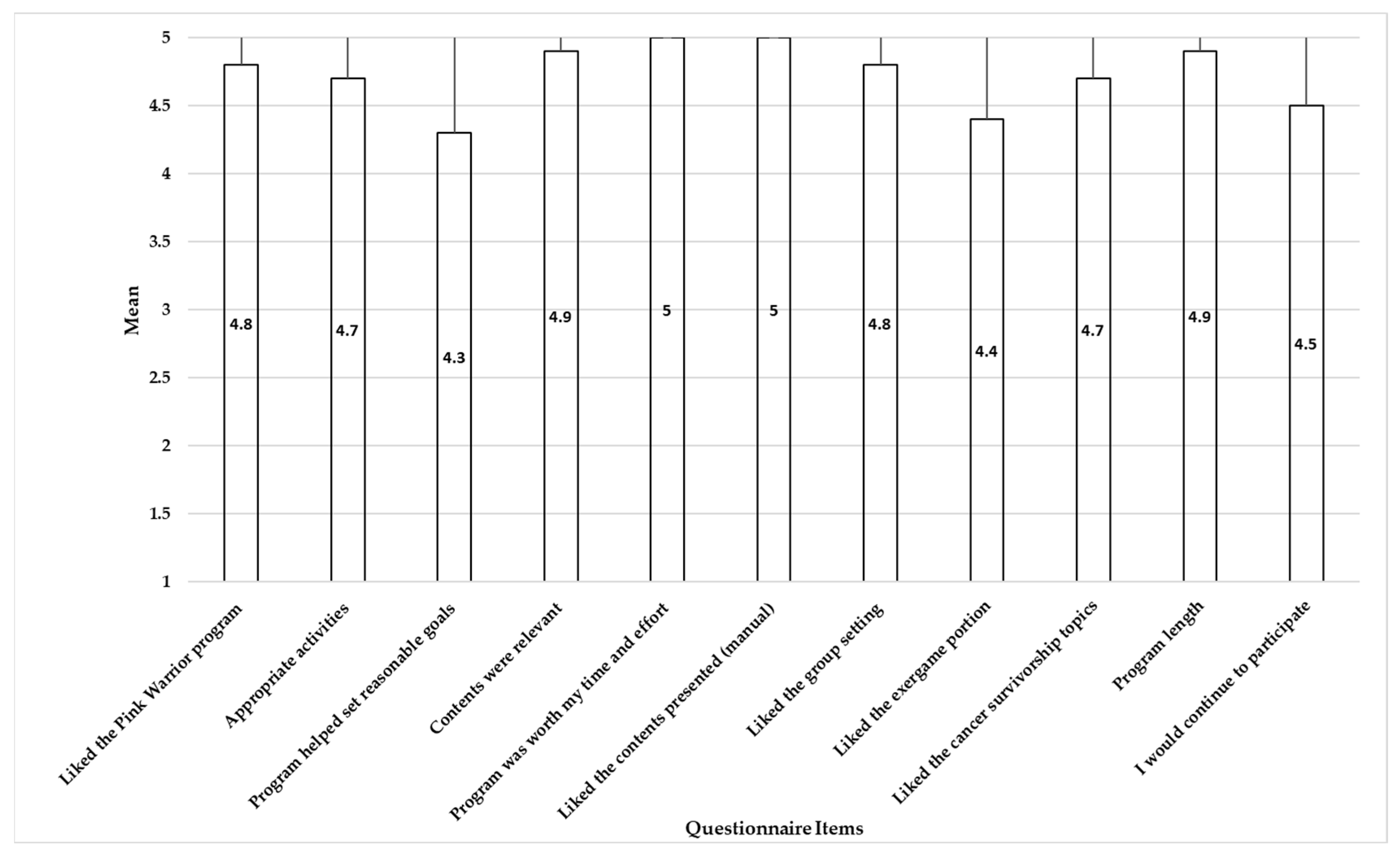
3.2.2. Acceptability
3.3. Physical Function and PA (Exploratory Results)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sulik, G. What cancer survivorship means. AMA J. Ethics 2013, 15, 697–703. [Google Scholar]
- American Cancer Society. Cancer Treatment & Survivorship Facts & Figures 2022–2024. Available online: https://www.cancer.org/content/dam/cancer-org/research/cancer-facts-and-statistics/cancer-treatment-and-survivorship-facts-and-figures/2022-cancer-treatment-and-survivorship-fandf-acs.pdf (accessed on 24 August 2022).
- Schmitz, K.H.; Cappola, A.R.; Stricker, C.T.; Sweeney, C.; Norman, S.A. The Intersection of Cancer and Aging: Establishing the Need for Breast Cancer Rehabilitation. Cancer Epidemiol. Biomark. Prev. 2007, 16, 866–872. [Google Scholar] [CrossRef] [Green Version]
- Cespedes Feliciano, E.M.; Vasan, S.; Luo, J.; Binder, A.M.; Chlebowski, R.T.; Quesenberry, C.; Banack, H.R.; Caan, B.J.; Paskett, E.D.; Williams, G.R.; et al. Long-term Trajectories of Physical Function Decline in Women with and without Cancer. JAMA Oncol. 2023. [Google Scholar] [CrossRef]
- Braithwaite, D.; Satariano, W.A.; Sternfeld, B.; Hiatt, R.A.; Ganz, P.A.; Kerlikowske, K.; Moore, D.H.; Slattery, M.L.; Tammemagi, M.; Castillo, A.; et al. Long-term Prognostic Role of Functional Limitations Among Women With Breast Cancer. JNCI J. Natl. Cancer Inst. 2010, 102, 1468–1477. [Google Scholar] [CrossRef]
- BLAIR, C.K.; MOREY, M.C.; DESMOND, R.A.; COHEN, H.J.; SLOANE, R.; SNYDER, D.C.; DEMARK-WAHNEFRIED, W. Light-Intensity Activity Attenuates Functional Decline in Older Cancer Survivors. Med. Sci. Sport. Exerc. 2014, 46, 1375–1383. [Google Scholar] [CrossRef] [Green Version]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar]
- Jung, A.Y.; Behrens, S.; Schmidt, M.; Thoene, K.; Obi, N.; Hüsing, A.; Benner, A.; Steindorf, K.; Chang-Claude, J. Pre- to postdiagnosis leisure-time physical activity and prognosis in postmenopausal breast cancer survivors. Breast Cancer Res. 2019, 21, 117. [Google Scholar] [CrossRef] [Green Version]
- Cannioto, R.A.; Hutson, A.; Dighe, S.; McCann, W.; McCann, S.E.; Zirpoli, G.R.; Barlow, W.; Kelly, K.M.; DeNysschen, C.A.; Hershman, D.L.; et al. Physical Activity Before, During, and After Chemotherapy for High-Risk Breast Cancer: Relationships With Survival. JNCI J. Natl. Cancer Inst. 2020, 113, 54–63. [Google Scholar] [CrossRef]
- Hefferon, K.; Murphy, H.; McLeod, J.; Mutrie, N.; Campbell, A. Understanding barriers to exercise implementation 5-year post-breast cancer diagnosis: A large-scale qualitative study. Health Educ. Res. 2013, 28, 843–856. [Google Scholar] [CrossRef] [Green Version]
- Gomes, M.L.B.; Pinto, S.S.; Domingues, M.R. Barriers to physical activity in women with and without breast cancer. ABCS Health Sci. 2020, 45, e020022. [Google Scholar] [CrossRef]
- Rogers, L.Q.; Courneya, K.S.; Shah, P.; Dunnington, G.; Hopkins-Price, P. Exercise stage of change, barriers, expectations, values and preferences among breast cancer patients during treatment: A pilot study. Eur. J. Cancer Care 2007, 16, 55–66. [Google Scholar] [CrossRef]
- Wurz, A.; St-Aubin, A.; Brunet, J. Breast cancer survivors’ barriers and motives for participating in a group-based physical activity program offered in the community. Support. Care Cancer 2015, 23, 2407–2416. [Google Scholar] [CrossRef] [Green Version]
- Spiteri, K.; Broom, D.; Hassan Bekhet, A.; Xerri de Caro, J.; Laventure, B.; Grafton, K. Barriers and Motivators of Physical Activity Participation in Middle-Aged and Older Adults—A Systematic Review. J. Aging Phys. Act. 2019, 27, 929–944. [Google Scholar] [CrossRef] [Green Version]
- Bandura, A. Social cognitive theory of self-regulation. Organ. Behav. Hum. Decis. Process. 1991, 50, 248–287. [Google Scholar] [CrossRef]
- Whitehead, S.; Lavelle, K. Older Breast Cancer Survivors’ Views and Preferences for Physical Activity. Qual. Health Res. 2009, 19, 894–906. [Google Scholar] [CrossRef]
- Silva, A.P.; Oliveira, E.M.d.; Okubo, R.; Benetti, M. Utilização de exergames e seus efeitos sobre a saúde física de pacientes com diagnóstico de câncer: Uma revisão integrativa. Fisioterapia e Pesquisa 2020, 27, 443–452. [Google Scholar] [CrossRef]
- Tough, D.; Robinson, J.; Gowling, S.; Raby, P.; Dixon, J.; Harrison, S.L. The feasibility, acceptability and outcomes of exergaming among individuals with cancer: A systematic review. BMC Cancer 2018, 18, 1151. [Google Scholar] [CrossRef] [Green Version]
- Swartz, M.C.; Lewis, Z.H.; Deer, R.R.; Stahl, A.L.; Swartz, M.D.; Christopherson, U.; Basen-Engquist, K.; Wells, S.J.; Silva, H.C.; Lyons, E.J. Feasibility and Acceptability of an Active Video Game-Based Physical Activity Support Group (Pink Warrior) for Survivors of Breast Cancer: Randomized Controlled Pilot Trial. JMIR Cancer 2022, 8, e36889. [Google Scholar] [CrossRef]
- Lieberman Debra, A.; Chamberlin, B.; Medina, E.; Franklin Barry, A.; Sanner Brigid, M.; Vafiadis Dorothea, K. The Power of Play: Innovations in Getting Active Summit 2011. Circulation 2011, 123, 2507–2516. [Google Scholar] [CrossRef] [Green Version]
- Costa, M.T.S.; Vieira, L.P.; Barbosa, E.O.; Mendes Oliveira, L.; Maillot, P.; Ottero Vaghetti, C.A.; Giovani Carta, M.; Machado, S.; Gatica-Rojas, V.; Monteiro-Junior, R.S. Virtual Reality-Based Exercise with Exergames as Medicine in Different Contexts: A Short Review. Clin. Pract. Epidemiol. Ment Health 2019, 15, 15–20. [Google Scholar] [CrossRef] [Green Version]
- Fortier, M.S.; Williams, G.C.; Sweet, S.N.; Patrick, H. Self-Determination theory: Process models for health behavior change. In Emerging Theories in Health Promotion Practice and Research, 2nd ed.; Jossey-Bass/Wiley: Hoboken, NJ, USA, 2009; pp. 157–183. [Google Scholar]
- Milne, H.M.; Wallman, K.E.; Guilfoyle, A.; Gordon, S.; Corneya, K.S. Self-determination theory and physical activity among breast cancer survivors. J. Sport Exerc. Psychol. 2008, 30, 23–38. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am. Psychol. 2000, 55, 68–78. [Google Scholar] [CrossRef]
- Teixeira, P.J.; Carraca, E.V.; Markland, D.; Silva, M.N.; Ryan, R.M. Exercise, physical activity, and self-determination theory: A systematic review. Int. J. Behav. Nutr. Phys. Act 2012, 9, 78. [Google Scholar] [CrossRef] [Green Version]
- Teixeira, P.J.; Marques, M.M.; Silva, M.N.; Brunet, J.; Duda, J.L.; Haerens, L.; La Guardia, J.; Lindwall, M.; Lonsdale, C.; Markland, D.; et al. A classification of motivation and behavior change techniques used in self-determination theory-based interventions in health contexts. Motiv. Sci. 2020, 6, 438–455. [Google Scholar] [CrossRef]
- Stevens, C.J.; Baldwin, A.S.; Bryan, A.D.; Conner, M.; Rhodes, R.E.; Williams, D.M. Affective Determinants of Physical Activity: A Conceptual Framework and Narrative Review. Front. Psychol. 2020, 11, 568331. [Google Scholar] [CrossRef]
- Zimmerling, A.; Chen, X. Innovation and possible long-term impact driven by COVID-19: Manufacturing, personal protective equipment and digital technologies. Technol. Soc. 2021, 65, 101541. [Google Scholar] [CrossRef]
- Ross, K.M.; Carpenter, C.A.; Arroyo, K.M.; Shankar, M.N.; Yi, F.; Qiu, P.; Anthony, L.; Ruiz, J.; Perri, M.G. Impact of transition from face-to-face to telehealth on behavioral obesity treatment during the COVID-19 pandemic. Obesity 2022, 30, 858–863. [Google Scholar] [CrossRef]
- Guidarelli, C.; Lipps, C.; Stoyles, S.; Dieckmann, N.F.; Winters-Stone, K.M. Remote administration of physical performance tests among persons with and without a cancer history: Establishing reliability and agreement with in-person assessment. J. Geriatr. Oncol. 2022, 13, 691–697. [Google Scholar] [CrossRef]
- Blair, C.K.; Harding, E.; Herman, C.; Boyce, T.; Demark-Wahnefried, W.; Davis, S.; Kinney, A.Y.; Pankratz, V.S. Remote Assessment of Functional Mobility and Strength in Older Cancer Survivors: Protocol for a Validity and Reliability Study. JMIR Res. Protoc. 2020, 9, e20834. [Google Scholar] [CrossRef]
- Eldridge, S.M.; Chan, C.L.; Campbell, M.J.; Bond, C.M.; Hopewell, S.; Thabane, L.; Lancaster, G.A. CONSORT 2010 statement: Extension to randomised pilot and feasibility trials. BMJ 2016, 355, i5239. [Google Scholar] [CrossRef] [Green Version]
- Czajkowski, S.M.; Powell, L.H.; Adler, N.; Naar-King, S.; Reynolds, K.D.; Hunter, C.M.; Laraia, B.; Olster, D.H.; Perna, F.M.; Peterson, J.C.; et al. From ideas to efficacy: The ORBIT model for developing behavioral treatments for chronic diseases. Health Psychol. 2015, 34, 971–982. [Google Scholar] [CrossRef]
- Kendall, J.M. Designing a research project: Randomised controlled trials and their principles. Emerg. Med. J. 2003, 20, 164–168. [Google Scholar] [CrossRef] [Green Version]
- Lyons, E.J.; Swartz, M.C.; Lewis, Z.H.; Martinez, E.; Jennings, K. Feasibility and Acceptability of a Wearable Technology Physical Activity Intervention With Telephone Counseling for Mid-Aged and Older Adults: A Randomized Controlled Pilot Trial. JMIR Mhealth Uhealth 2017, 5, e28. [Google Scholar] [CrossRef]
- Haahr, M. Random. org: True Random Number Service. Available online: Random.org (accessed on 1 October 2022).
- Adams, M.M.; Davis, P.G.; Gill, D.L. A Hybrid Online Intervention for Reducing Sedentary Behavior in Obese Women. Front. Public Health 2013, 1, 45. [Google Scholar] [CrossRef] [Green Version]
- Setera, K. FBI Warns of Teleconferencing and Online Classroom Hijacking During COVID-19 Pandemic. Available online: https://www.fbi.gov/contact-us/field-offices/boston/news/press-releases/fbi-warns-of-teleconferencing-and-online-classroom-hijacking-during-covid-19-pandemic (accessed on 26 December 2022).
- Basen-Engquist, K.; Taylor, C.L.C.; Rosenblum, C.; Smith, M.A.; Shinn, E.H.; Greisinger, A.; Gregg, X.; Massey, P.; Valero, V.; Rivera, E. Randomized pilot test of a lifestyle physical activity intervention for breast cancer survivors. Patient Educ. Couns. 2006, 64, 225–234. [Google Scholar] [CrossRef]
- Tami-Maury, I.M.; Liao, Y.; Rangel, M.L.; Gatus, L.A.; Shinn, E.H.; Alexander, A.; Basen-Engquist, K. Active Living After Cancer: Adaptation and evaluation of a community-based physical activity program for minority and medically underserved breast cancer survivors. Cancer 2022, 128, 353–363. [Google Scholar] [CrossRef]
- Michie, S.; West, R.; Campbell, R.; Brown, J.; Gainforth, H. ABC of Behaviour Change Theories; Silverback Publishing: Great Britain, UK, 2014. [Google Scholar]
- Michie, S.; Ashford, S.; Sniehotta, F.F.; Dombrowski, S.U.; Bishop, A.; French, D.P. A refined taxonomy of behaviour change techniques to help people change their physical activity and healthy eating behaviours: The CALO-RE taxonomy. Psychol. Health 2011, 26, 1479–1498. [Google Scholar] [CrossRef]
- Maillot, P.; Perrot, A.; Hartley, A. Effects of interactive physical-activity video-game training on physical and cognitive function in older adults. Psychol. Aging 2012, 27, 589–600. [Google Scholar] [CrossRef] [Green Version]
- Lin, J.H. “Just Dance”: The Effects of Exergame Feedback and Controller Use on Physical Activity and Psychological Outcomes. Games Health J. 2015, 4, 183–189. [Google Scholar] [CrossRef]
- Tate, D.F.; Lyons, E.J.; Valle, C.G. High-Tech Tools for Exercise Motivation: Use and Role of Technologies Such as the Internet, Mobile Applications, Social Media, and Video Games. Diabetes Spectr. 2015, 28, 45–54. [Google Scholar] [CrossRef] [Green Version]
- Walsh-Burke, K.; Marcusen, C. Self-Advocacy Training for Cancer Survivors. Cancer Pract. 1999, 7, 297–301. [Google Scholar] [CrossRef]
- LaFave, S.E.; Granbom, M.; Cudjoe, T.K.M.; Gottsch, A.; Shorb, G.; Szanton, S.L. Attention control group activities and perceived benefit in a trial of a behavioral intervention for older adults. Res. Nurs. Health 2019, 42, 476–482. [Google Scholar] [CrossRef]
- Lewis, Z.H.; Cannon, M.; Rubio, G.; Swartz, M.C.; Lyons, E.J. Analysis of the Behavioral Change and Utility Features of Electronic Activity Monitors. Technologies 2020, 8, 75. [Google Scholar] [CrossRef]
- Walters, S.J.; Bonacho Dos Anjos Henriques-Cadby, I.; Bortolami, O.; Flight, L.; Hind, D.; Jacques, R.M.; Knox, C.; Nadin, B.; Rothwell, J.; Surtees, M.; et al. Recruitment and retention of participants in randomised controlled trials: A review of trials funded and published by the United Kingdom Health Technology Assessment Programme. BMJ Open 2017, 7, e015276. [Google Scholar] [CrossRef]
- Singh, B.; Spence, R.R.; Steele, M.L.; Sandler, C.X.; Peake, J.M.; Hayes, S.C. A Systematic Review and Meta-Analysis of the Safety, Feasibility, and Effect of Exercise in Women With Stage II+ Breast Cancer. Arch. Phys. Med. Rehabil. 2018, 99, 2621–2636. [Google Scholar] [CrossRef] [Green Version]
- Ormel, H.L.; van der Schoot, G.G.F.; Sluiter, W.J.; Jalving, M.; Gietema, J.A.; Walenkamp, A.M.E. Predictors of adherence to exercise interventions during and after cancer treatment: A systematic review. Psycho-Oncology 2018, 27, 713–724. [Google Scholar] [CrossRef] [Green Version]
- Vandelanotte, C.; De Bourdeaudhuij, I. Acceptability and feasibility of a computer-tailored physical activity intervention using stages of change: Project FAITH. Health Educ. Res. 2003, 18, 304–317. [Google Scholar] [CrossRef] [Green Version]
- Vandelanotte, C.; De Bourdeaudhuij, I.; Brug, J. Acceptability and feasibility of an interactive computer-tailored fat intake intervention in Belgium. Health Promot. Int. 2004, 19, 463–470. [Google Scholar] [CrossRef] [Green Version]
- Puthoff, M.L. Outcome measures in cardiopulmonary physical therapy: Short physical performance battery. Cardiopulm. Phys. Ther. J. 2008, 19, 17–22. [Google Scholar] [CrossRef]
- Bohannon, R.W. Reference Values for the Timed Up and Go Test: A Descriptive Meta-Analysis. J. Geriatr. Phys. Ther. 2006, 29, 64–68. [Google Scholar] [CrossRef] [Green Version]
- Shumway-Cook, A.; Brauer, S.; Woollacott, M. Predicting the Probability for Falls in Community-Dwelling Older Adults Using the Timed Up & Go Test. Physical. Ther. 2000, 80, 896–903. [Google Scholar] [CrossRef] [Green Version]
- Podsiadlo, D.; Richardson, S. The timed “Up & Go”: A test of basic functional mobility for frail elderly persons. J. Am. Geriatr. Soc. 1991, 39, 142–148. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Development and Validation of a Functional Fitness Test for Community-Residing Older Adults. J. Aging Phys. Act. 1999, 7, 129–161. [Google Scholar] [CrossRef]
- Rikli, R.E.; Jones, C.J. Functional Fitness Normative Scores for Community-Residing Older Adults, Ages 60–94. J. Aging Phys. Act. 1999, 7, 162–181. [Google Scholar] [CrossRef]
- Hoenemeyer, T.W.; Cole, W.W.; Oster, R.A.; Pekmezi, D.W.; Pye, A.; Demark-Wahnefried, W. Test/Retest Reliability and Validity of Remote vs. In-Person Anthropometric and Physical Performance Assessments in Cancer Survivors and Supportive Partners. Cancers 2022, 14, 1075. [Google Scholar] [CrossRef]
- Keadle, S.K.; Shiroma, E.J.; Freedson, P.S.; Lee, I.M. Impact of accelerometer data processing decisions on the sample size, wear time and physical activity level of a large cohort study. BMC Public Health 2014, 14, 1210. [Google Scholar] [CrossRef] [Green Version]
- Lipsey, M.W.; Wilson, D.B. Practical Meta-Analysis; Sage Publications, Inc.: Thousand Oaks, CA, USA, 2001; p. ix, 247. [Google Scholar]
- BOHANNON, R.W. Comfortable and maximum walking speed of adults aged 20–79 years: Reference values and determinants. Age Ageing 1997, 26, 15–19. [Google Scholar] [CrossRef] [Green Version]
- Perera, S.; Mody, S.H.; Woodman, R.C.; Studenski, S.A. Meaningful change and responsiveness in common physical performance measures in older adults. J. Am. Geriatr. Soc. 2006, 54, 743–749. [Google Scholar] [CrossRef]
- Makizako, H.; Shimada, H.; Doi, T.; Tsutsumimoto, K.; Nakakubo, S.; Hotta, R.; Suzuki, T. Predictive Cutoff Values of the Five-Times Sit-to-Stand Test and the Timed “Up & Go” Test for Disability Incidence in Older People Dwelling in the Community. Phys. Ther. 2017, 97, 417–424. [Google Scholar] [CrossRef]
- Mirza, M.; Siebert, S.; Pratt, A.; Insch, E.; McIntosh, F.; Paton, J.; Wright, C.; Buckley, C.D.; Isaacs, J.; McInnes, I.B.; et al. Impact of the COVID-19 pandemic on recruitment to clinical research studies in rheumatology. Musculoskelet. Care 2022, 20, 209–213. [Google Scholar] [CrossRef]
- de Koning, R.; Egiz, A.; Kotecha, J.; Ciuculete, A.C.; Ooi, S.Z.Y.; Bankole, N.D.A.; Erhabor, J.; Higginbotham, G.; Khan, M.; Dalle, D.U.; et al. Survey Fatigue During the COVID-19 Pandemic: An Analysis of Neurosurgery Survey Response Rates. Front. Surg. 2021, 8, 690680. [Google Scholar] [CrossRef]
- Cardel, M.I.; Manasse, S.; Krukowski, R.A.; Ross, K.; Shakour, R.; Miller, D.R.; Lemas, D.J.; Hong, Y.-R. COVID-19 Impacts Mental Health Outcomes and Ability/Desire to Participate in Research Among Current Research Participants. Obesity 2020, 28, 2272–2281. [Google Scholar] [CrossRef]
- Taylor, L.M.; Maddison, R.; Pfaeffli, L.A.; Rawstorn, J.C.; Gant, N.; Kerse, N.M. Activity and Energy Expenditure in Older People Playing Active Video Games. Arch. Phys. Med. Rehabil. 2012, 93, 2281–2286. [Google Scholar] [CrossRef]
- Bohannon, R.W.; Glenney, S.S. Minimal clinically important difference for change in comfortable gait speed of adults with pathology: A systematic review. J. Eval. Clin. Pract. 2014, 20, 295–300. [Google Scholar] [CrossRef]
- Brown, J.C.; Harhay, M.O.; Harhay, M.N. Physical function as a prognostic biomarker among cancer survivors. Br. J. Cancer 2015, 112, 194–198. [Google Scholar] [CrossRef] [Green Version]
- Brown, M.; O’Connor, D.; Murphy, C.; McClean, M.; McMeekin, A.; Prue, G. Impact of COVID-19 on an established physical activity and behaviour change support programme for cancer survivors: An exploratory survey of the Macmillan Move More service for Northern Ireland. Support. Care Cancer 2021, 29, 6135–6143. [Google Scholar] [CrossRef]
- Bu, F.; Bone, J.K.; Mitchell, J.J.; Steptoe, A.; Fancourt, D. Longitudinal changes in physical activity during and after the first national lockdown due to the COVID-19 pandemic in England. Sci. Rep. 2021, 11, 17723. [Google Scholar] [CrossRef]
- Tison, G.H.; Avram, R.; Kuhar, P.; Abreau, S.; Marcus, G.M.; Pletcher, M.J.; Olgin, J.E. Worldwide Effect of COVID-19 on Physical Activity: A Descriptive Study. Ann. Intern. Med. 2020, 173, 767–770. [Google Scholar] [CrossRef]
- Said, C.M.; Batchelor, F.; Duque, G. The Impact of the COVID-19 Pandemic on Physical Activity, Function, and Quality of Life. Clin. Geriatr. Med. 2022, 38, 519–531. [Google Scholar] [CrossRef]
- Hergenroeder, A.L.; Barone Gibbs, B.; Kotlarczyk, M.P.; Kowalsky, R.J.; Perera, S.; Brach, J.S. Accuracy of Objective Physical Activity Monitors in Measuring Steps in Older Adults. Gerontol. Geriatr. Med. 2018, 4, 2333721418781126. [Google Scholar] [CrossRef] [Green Version]
- Park, A.H.; Zhong, S.; Yang, H.; Jeong, J.; Lee, C. Impact of COVID-19 on physical activity: A rapid review. J. Glob. Health 2022, 12, 05003. [Google Scholar] [CrossRef]
- Wittink, H.; Rogers, W.; Sukiennik, A.; Carr, D.B. Physical Functioning: Self-Report and Performance Measures Are Related but Distinct. Spine 2003, 28, 2407–2413. [Google Scholar] [CrossRef]
- Brach, J.S.; VanSwearingen, J.M.; Newman, A.B.; Kriska, A.M. Identifying Early Decline of Physical Function in Community-Dwelling Older Women: Performance-Based and Self-Report Measures. Physical. Ther. 2002, 82, 320–328. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Name of the Assessment | Description | Detailed Descriptions |
|---|---|---|
| The Short Physical Performance Battery (SPPB) | Score range: 0 to 12 Consist of 3 components:
|
|
| Timed Up & Go TUG) | Score range: ≤10 s = normal; ≤20 s = good mobility without gait aid; ≤30 s = problems, requires gait aid; ≥14 s is associated with high fall risk | Participants need to stand up from a chair and move as quickly as participants feel safe until the participant passes a tape that is 10 feet from the chair. Then, they turn around and walk back to the chair and sit back down. |
| Two-minute step test | Norm for 60–64: 75–107 steps march in place for 2 min | Participants need to march in place, but the knee needs to hit the halfway mark between participants’ iliac crest and patella height. |
| Characteristic | Total (N = 20) | Intervention (N = 10) | Control (N = 10) | p-Value a |
|---|---|---|---|---|
| Race/ethnicity (n = 20; n; %) | ||||
| Non-Hispanic White African American Hispanic Other | 16 (80) 2 (10) 1 (5) 1 (5) | 8 (80) 0 (0) 1 (10) 1 (10) | 8 (80) 2 (20) 0 (0) 0 (0) | 0.474 |
| Stage (n = 18; n; %) | ||||
| 0 I II III | 2 (11.1) 8 (44.4) 4 (22.2) 4 (22.2) | 1 (10) 2 (20) 4 (40) 3 (30) | 1 (12.5) 6 (75) 0 (0) 1 (12.5) | 0.106 |
| Treatment type (n = 18; n; %) | ||||
| Surgery only Surgery and chemotherapy Surgery, chemotherapy, and radiation Surgery and radiation | 1 (5.6) 4 (22.2) 8 (44.4) 5 (27.8) | 1 (10) 2 (20) 5 (50) 2 (20) | 0 (0) 2 (25) 3 (37.5) 3 (37.5) | 0.904 |
| Current treatment status (n = 18; n; %) | ||||
| Off treatment On treatment | 16 (89) 2 (11) | 8 (80) 2 (20) | 8 (100) 0 (36.67) | 0.477 |
| Patient-reported neuropathy (n = 18; n; %) | ||||
| Yes No | 6 (33.3) 12 (66.7) | 4 (40) 6 (60) | 2 (25) 6 (75) | 0.638 |
| Age (n = 20; years, range 55–79; mean; SD) | 63.75 (6.35) | 64.90 (8.03) | 62.60 (4.20) | 0.43 |
| Time since diagnosis (n = 18; months; mean; SD) | 96.11 (82.61) Range: 2–284 months | 113.70 (92.99) | 74.13 (66.81) | 0.33 |
| BMI (n = 19; kg/m2; mean; SD) | 31.89 (6.04) | 33.91 (7.11) | 29.66 (3.80) | 0.13 |
| Variables | Intervention | Control | Effect Size | ||||
|---|---|---|---|---|---|---|---|
| Baseline Mean (SD) | Follow-Up Mean (SD) | Mean of Difference (SD) | Baseline Mean (SD) | Follow-Up Mean (SD) | Mean of Difference (SD) | Cohen’s d | |
| Gait speed (meter/seconds); n = 19 | 0.76 (0.24) | 0.94 (0.17) | 0.18 (0.17) | 0.89 (0.18) | 1.01 (0.15) | 0.11 (0.13) | 0.46 |
| Total SPPB a score; n = 19 | 8.70 (1.57) | 10.30 (1.34) | 1.6 (1.17) | 9.56 (1.59) | 10 (1.12) | 0.44 (1.01) | 1.06 |
| TUG b (seconds); n = 18 | 10.46 (3.52) | 9.78 (3.11) | −0.69 (0.91) | 9.12 (1.73) | 8.93 (0.85) | −0.01 (2.06) | 0.43 |
| Two-minute step test (count); n = 18 | 62.89 (21.69) | 75.0 (24.26) | 12.11 (13.83) | 75.89 (30.98) | 76.11 (28.81) | 0.22 (24.11) | 0.61 |
| Steps (average steps); n = 19 | 4652.60 (2659.88) | 4423.09 (2016.41) | −229.52 (1905.94) | 4268.52 (1721.36) | 5838.69 (2767.52) | 1570.17 (2355.59) | 0.85 |
| MVPA c (average minutes); n = 19 | 9.4689 (9.93) | 10.00 (9.13) | 0.54 (8.78) | 12.07 (13.67) | 17.34 (23.09) | 5.28 (23.66) | 0.27 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Swartz, M.C.; Robertson, M.C.; Christopherson, U.; Wells, S.J.; Lewis, Z.H.; Bai, J.; Swartz, M.D.; Silva, H.C.; Martinez, E.; Lyons, E.J. Assessing the Suitability of a Virtual ‘Pink Warrior’ for Older Breast Cancer Survivors during COVID-19: A Pilot Study. Life 2023, 13, 574. https://doi.org/10.3390/life13020574
Swartz MC, Robertson MC, Christopherson U, Wells SJ, Lewis ZH, Bai J, Swartz MD, Silva HC, Martinez E, Lyons EJ. Assessing the Suitability of a Virtual ‘Pink Warrior’ for Older Breast Cancer Survivors during COVID-19: A Pilot Study. Life. 2023; 13(2):574. https://doi.org/10.3390/life13020574
Chicago/Turabian StyleSwartz, Maria C., Michael C. Robertson, Ursela Christopherson, Stephanie J. Wells, Zakkoyya H. Lewis, Jinbing Bai, Michael D. Swartz, H. Colleen Silva, Eloisa Martinez, and Elizabeth J. Lyons. 2023. "Assessing the Suitability of a Virtual ‘Pink Warrior’ for Older Breast Cancer Survivors during COVID-19: A Pilot Study" Life 13, no. 2: 574. https://doi.org/10.3390/life13020574