
Monitoring Methodology for an AI Tool for Breast Cancer Screening Deployed in Clinical Centers


Abstract
:1. Introduction
2. Materials and Methods
2.1. AI System
2.2. Data
2.3. Statistical Analysis
3. Results
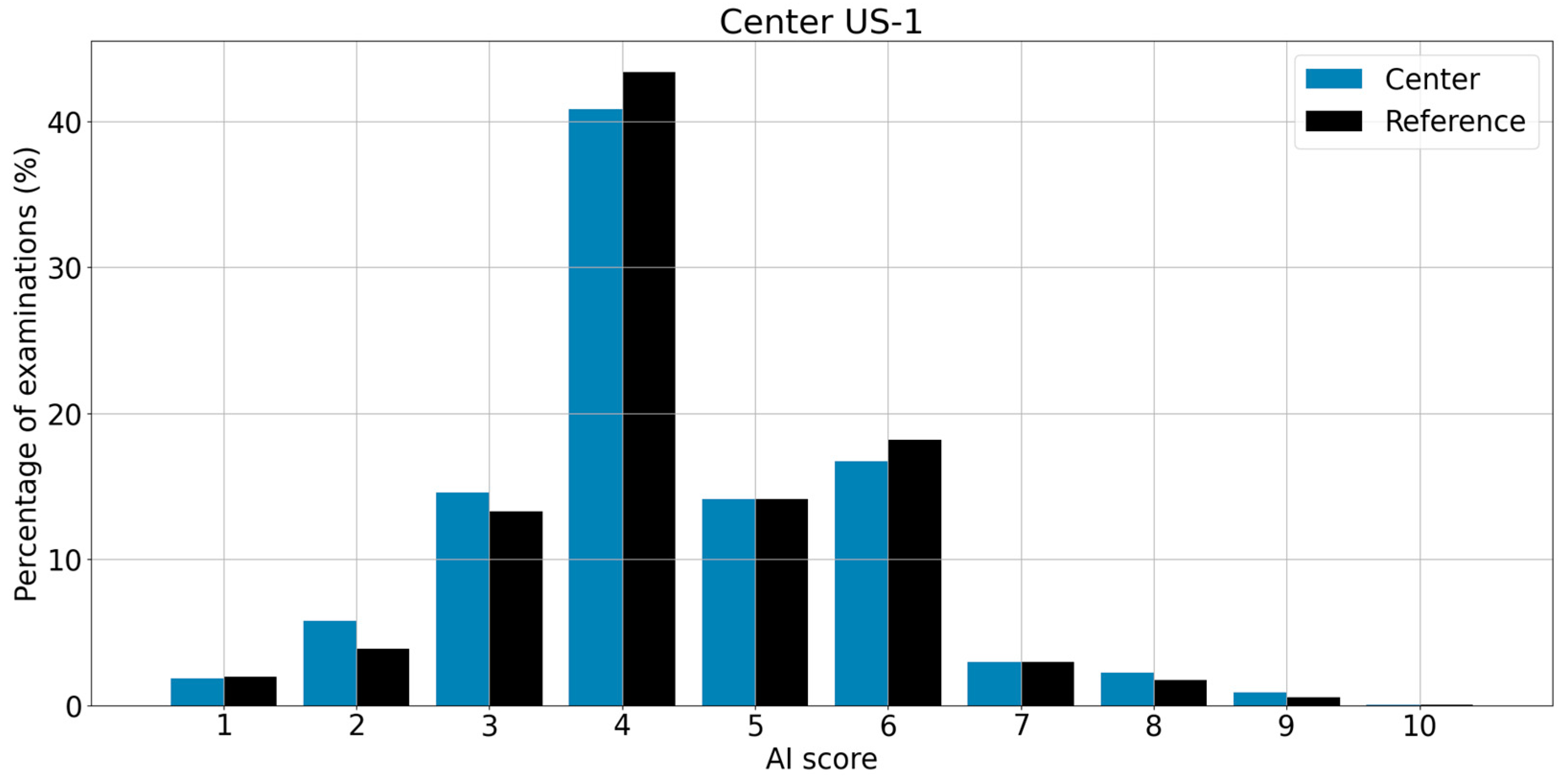
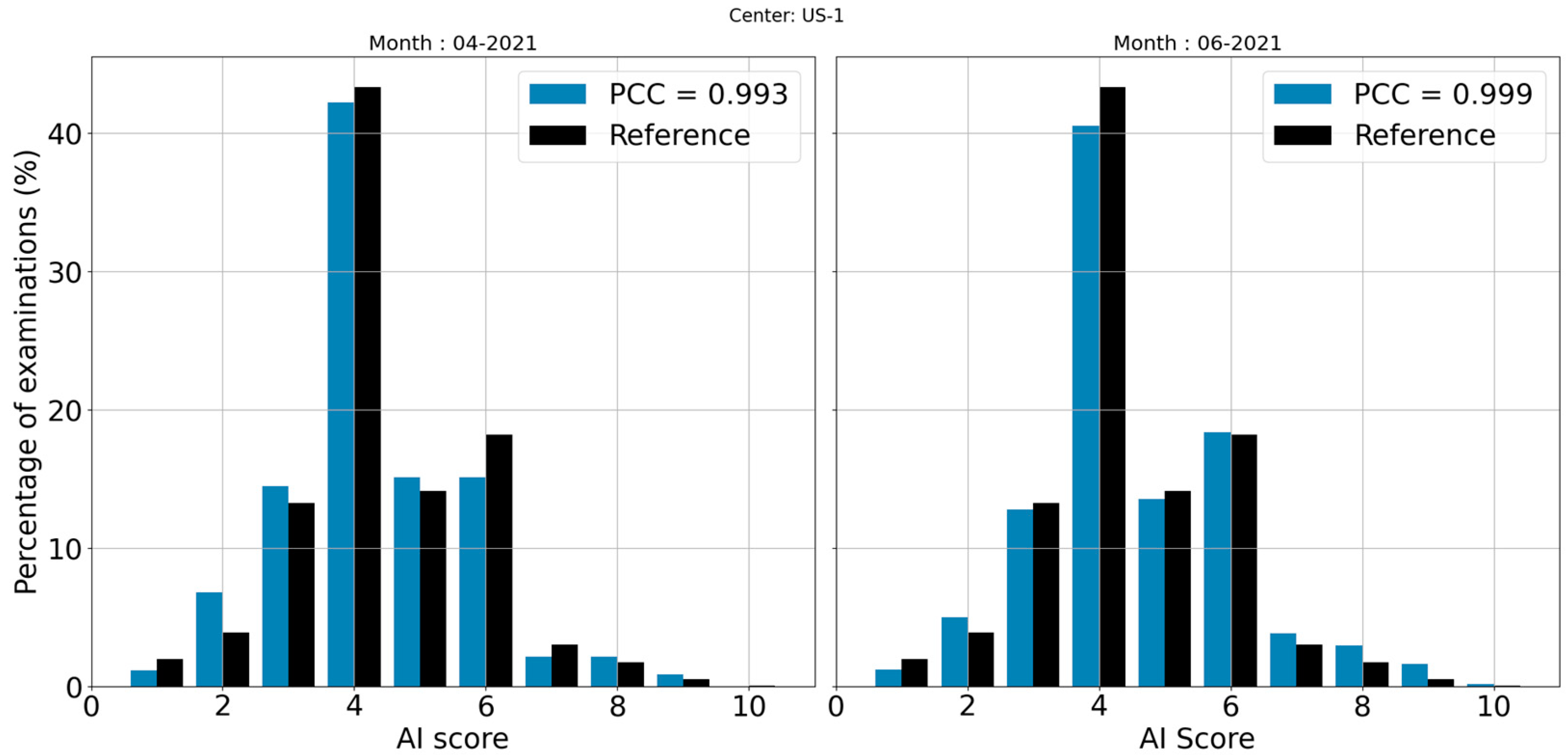
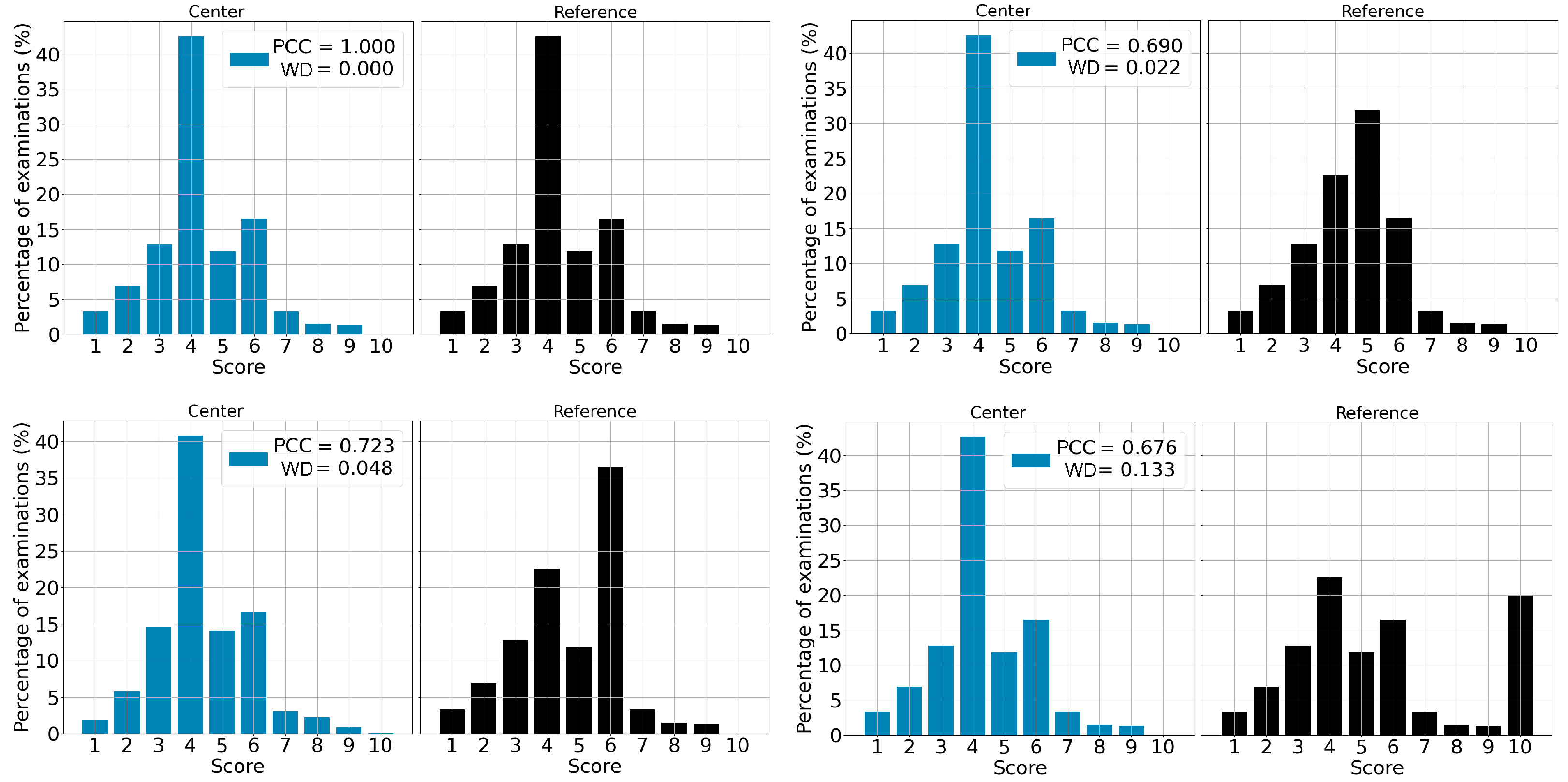
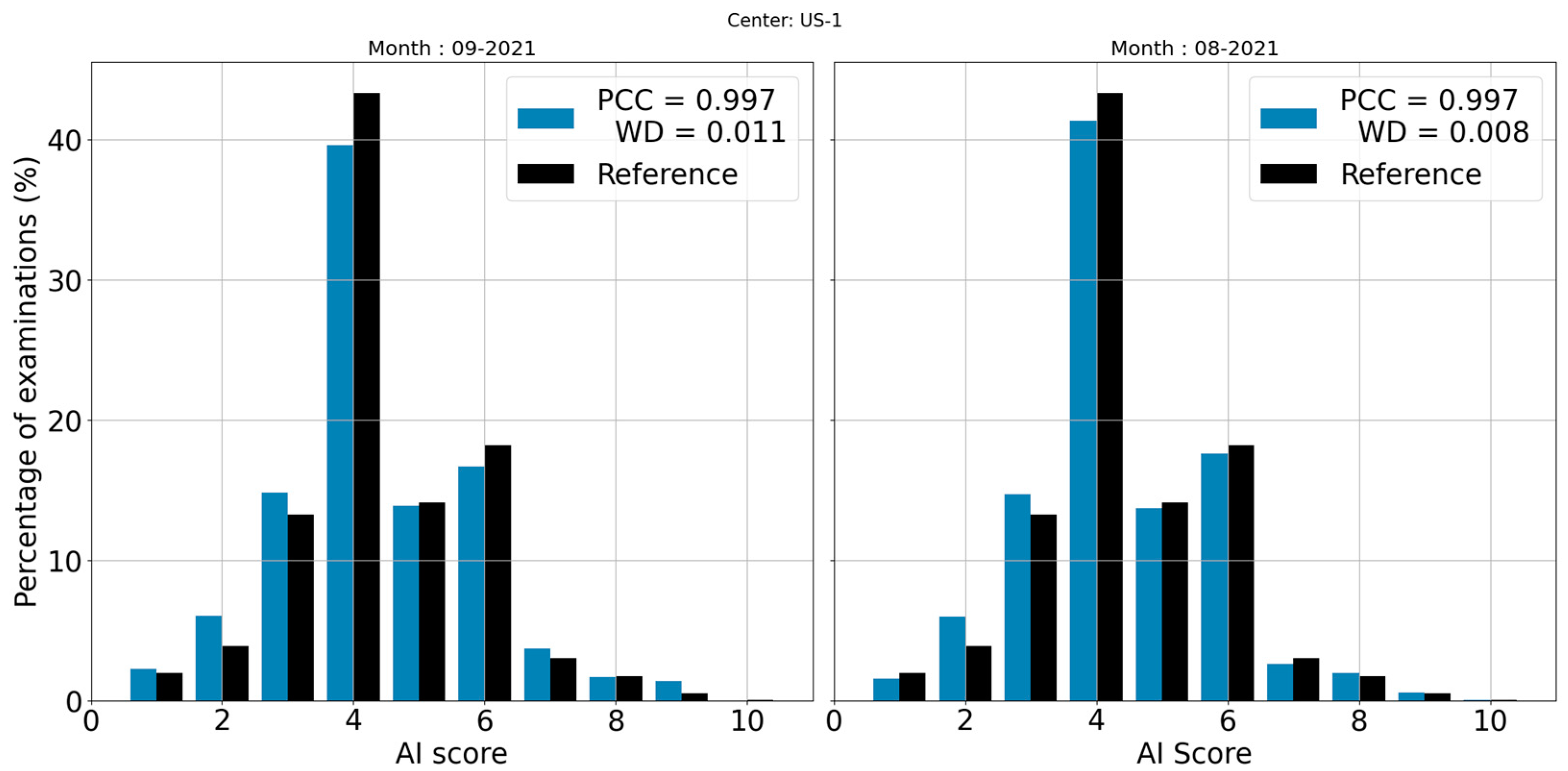
3.1. Correlation between Reference and Center
3.2. χ2 Test
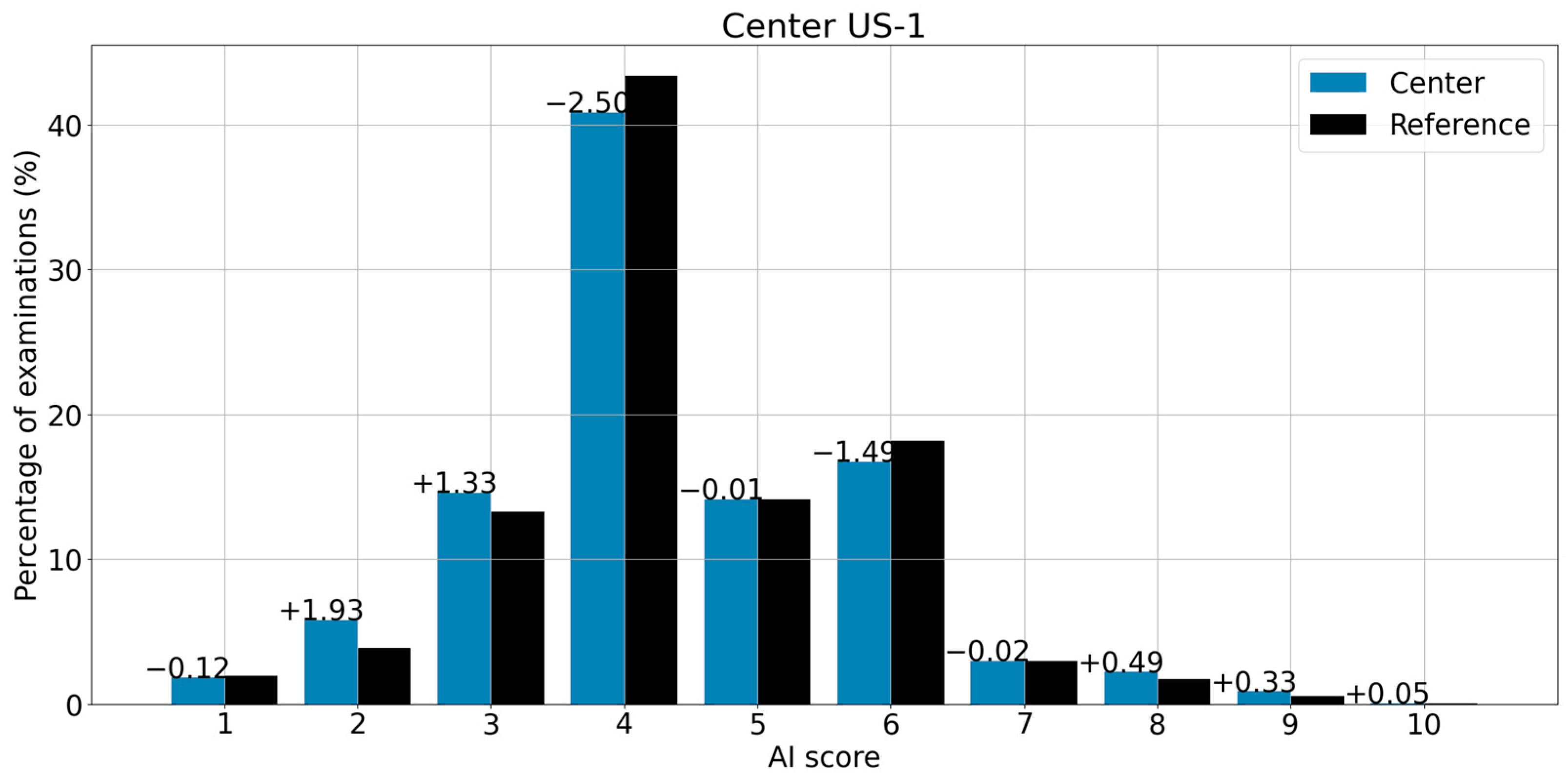
3.3. Score-by-Score Difference
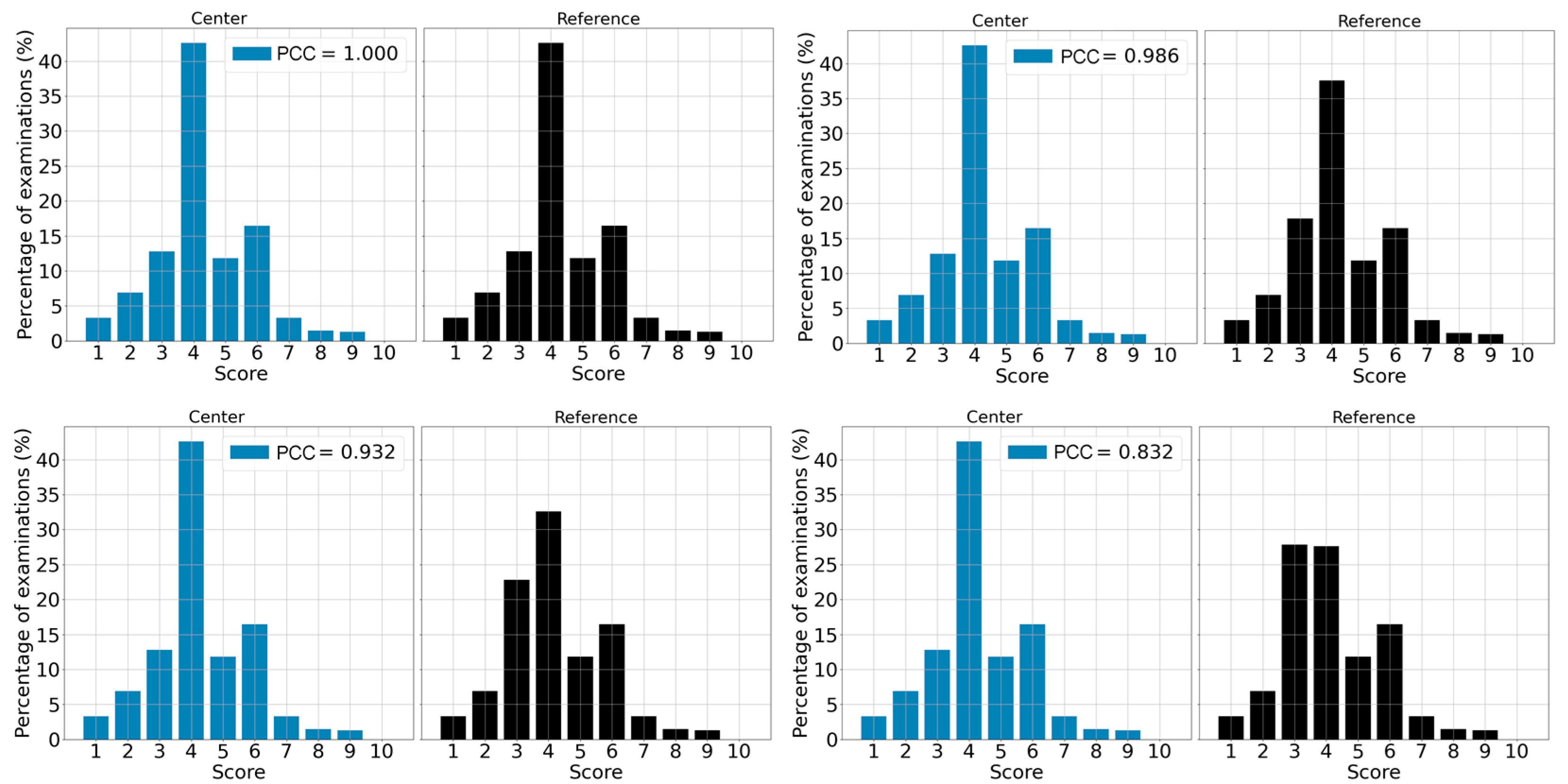
3.4. Deviation Detection
3.5. Severity of a Shift
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yu, K.H.; Beam, A.L.; Kohane, I.S. Artificial intelligence in healthcare. Nat. Biomed. Eng. 2018, 2, 719–731. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very Deep Convolutional Networks for Large-Scale Image Recognition. arXiv 2015, arXiv:1409.1556. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer Statistics, 2021. CA Cancer J. Clin. 2021, 71, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Hosny, A.; Parmar, C.; Quackenbush, J.; Schwartz, L.H.; Aerts, H.J.W.L. Artificial intelligence in radiology. Nat. Rev. Cancer 2018, 18, 500–510. [Google Scholar] [CrossRef] [PubMed]
- Vyborny, C.J.; Giger, M.L. Computer vision and artificial intelligence in mammography. Am. J. Roentgenol. 1994, 162, 699–708. [Google Scholar] [CrossRef]
- LeCun, Y.; Bengio, Y.; Hinton, G. Deep learning. Nature 2015, 521, 436–444. [Google Scholar] [CrossRef]
- Kopans, D.B. An open letter to panels that are deciding guidelines for breast cancer screening. Breast Cancer Res. Treat. 2015, 151, 19–25. [Google Scholar] [CrossRef]
- Park, S.H.; Han, K. Methodologic Guide for Evaluating Clinical Performance and Effect of Artificial Intelligence Technology for Medical Diagnosis and Prediction. Radiology 2018, 286, 800–809. [Google Scholar] [CrossRef] [PubMed]
- Yampolskiy, R.V.; Spellchecker, M.S. Artificial Intelligence Safety and Cybersecurity: A Timeline of AI Failures. arXiv 2016, arXiv:1610.07997. [Google Scholar] [CrossRef]
- Ryan, M. In AI We Trust: Ethics, Artificial Intelligence, and Reliability. Sci. Eng. Ethic 2020, 26, 2749–2767. [Google Scholar] [CrossRef]
- Feng, J.; Phillips, R.V.; Malenica, I.; Bishara, A.; Hubbard, A.E.; Celi, L.A.; Pirracchio, R. Clinical artificial intelligence quality improvement: Towards continual monitoring and updating of AI algorithms in healthcare. NPJ Digit. Med. 2022, 5, 66. [Google Scholar] [CrossRef] [PubMed]
- SPacilè, S.; Lopez, J.; Chone, P.; Bertinotti, T.; Grouin, J.M.; Fillard, P. Improving Breast Cancer Detection Accuracy of Mammography with the Concurrent Use of an Artificial Intelligence Tool. Radiol. Artif. Intell. 2020, 2, e190208. [Google Scholar] [CrossRef] [PubMed]
- Al Ridhawi, I.; Otoum, S.; Aloqaily, M.; Boukerche, A. Generalizing AI: Challenges and Opportunities for Plug and Play AI Solutions. IEEE Netw. 2021, 35, 372–379. [Google Scholar] [CrossRef]
- Bar, O.; Neimark, D.; Zohar, M.; Hager, G.D.; Girshick, R.; Fried, G.M.; Wolf, T.; Asselmann, D. Impact of data on generalization of AI for surgical intelligence applications. Sci. Rep. 2020, 10, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Benesty, J.; Chen, J.; Huang, Y.; Cohen, I. Pearson Correlation Coefficient. In Noise Reduction in Speech Processing; Cohen, I., Huang, Y., Chen, J., Benesty, J., Eds.; Springer: Berlin, Heidelberg, Germany, 2009; pp. 1–4. [Google Scholar] [CrossRef]
- Ratner, B. The correlation coefficient: Its values range between +1/−1, or do they? J. Targeting, Meas. Anal. Mark. 2009, 17, 139–142. [Google Scholar] [CrossRef]
- Balakrishnan, N.; Voinov, V.; Nikulin, M. Chi-Squared Goodness of Fit Tests with Applications. Academic Press: Cambridge, MA, USA, 2013. [Google Scholar]
- Panaretos, V.M.; Zemel, Y. Statistical Aspects of Wasserstein Distances. Annu. Rev. Stat. Its Appl. 2019, 6, 405–431. [Google Scholar] [CrossRef]
- Welcome to Python.org, Python.org. Available online: https://www.python.org/ (accessed on 17 January 2023).
- Home, OpenCV. Available online: https://opencv.org/ (accessed on 17 January 2023).
- Scipy. Stats. Wasserstein_Distance—SciPy v1.10.0 Manual. Available online: https://docs.scipy.org/doc/scipy/reference/generated/scipy.stats.wasserstein_distance.html (accessed on 17 January 2023).
- Boracchi, G.; Carrera, D.; Cervellera, C.; Macciò, D. QuantTree: Histograms for Change Detection in Multivariate Data Streams. In Proceedings of the 35th International Conference on Machine Learning, Stockholm, Sweden, 10–15 July 2018; pp. 639–648. Available online: https://proceedings.mlr.press/v80/boracchi18a.html (accessed on 6 July 2022).
- Richards, M.; Westcombe, A.; Love, S.; Littlejohns, P.; Ramirez, A. Influence of delay on survival in patients with breast cancer: A systematic review. Lancet 1999, 353, 1119–1126. [Google Scholar] [CrossRef]
- Caplan, L. Delay in Breast Cancer: Implications for Stage at Diagnosis and Survival. Front. Public Health 2014, 2. Available online: https://www.frontiersin.org/articles/10.3389/fpubh.2014.00087 (accessed on 19 January 2023). [CrossRef]
- Cha, S.-H.; Srihari, S.N. On measuring the distance between histograms. Pattern Recognit. 2002, 35, 1355–1370. [Google Scholar] [CrossRef] [Green Version]
- Swain, M.J.; Ballard, D.H. Color indexing. Int. J. Comput. Vis. 1991, 7, 11–32. [Google Scholar] [CrossRef]
- Aherne, F.J.; Thacker, N.A.; Rockett, P.I. The Bhattacharyya metric as an absolute similarity measure for frequency coded data. Kybernetika 1998, 34, 363–368. [Google Scholar]
- Zeng, J.; Kruger, U.; Geluk, J.; Wang, X.; Xie, L. Detecting abnormal situations using the Kullback–Leibler divergence. Automatica 2014, 50, 2777–2786. [Google Scholar] [CrossRef]
- Joyce, J.M. Kullback-Leibler Divergence. In International Encyclopedia of Statistical Science; Lovric, M., Ed.; Springer: Berlin/Heidelberg, Germany, 2011; pp. 720–722. [Google Scholar] [CrossRef]
- Belov, D.I.; Armstrong, R.D. Distributions of the Kullback-Leibler divergence with applications. Br. J. Math. Stat. Psychol. 2011, 64, 291–309. [Google Scholar] [CrossRef] [PubMed]
- Rogerson, P.A. The Detection of Clusters Using a Spatial Version of the Chi-Square Goodness-of-Fit Statistic. Geogr. Anal. 1999, 31, 130–147. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Center | Manufacturer | Reports | AI-Version | Modality | Dates (Months) |
|---|---|---|---|---|---|
| US-1 | Hologic® | 18,470 (51 %) | 1.2 | FFDM | April 2021–February 2022 (11) |
| US-2 | Hologic® | 6227 (17 %) | 1.3 | FFDM | October 2021–March 2022 (6) |
| US-3 | Hologic® | 11,100 (30 %) | 2.0.1 | DBT | October 2021–October 2022 (13) |
| US-4 | Hologic® | 784 (2 %) | 1.2 | FFDM | July 2021–March 2022 (9) |
| Number of Exams | AI Version Assessed | Manufacturer | Modality | Dates |
|---|---|---|---|---|
| 13,433 (25.4%) | 1.2 | Hologic® | FFDM | December 2006–July 2019 |
| 25,330 (47.8%) | 1.3 | Hologic® | FFDM | October 2006–July 2019 |
| 14,187 (26.8%) | 2.0 | Hologic® | DBT | October 2006–July 2019 |
| Center | PCC Mean | PCC Standard Deviation |
|---|---|---|
| US-1 | 0.996 | 0.002 |
| US-2 | 0.968 | 0.023 |
| US-3 | 0.985 | 0.084 |
| US-4 | 0.971 | 0.083 |
| Center. | Manufacturer and Modality | Version | PCC | χ² p-Value | Reference |
|---|---|---|---|---|---|
| US-1 | Hologic FFDM | 1.2 | 0.998 [min: 0.993, max: 0.999] | 0.853 | Hologic (FFDM), V 1.2 |
| US-2 | Hologic FFDM | 1.3 | 0.975 [min: 0.923, max: 0.986] | 0.616 | Hologic (FFDM), V 1.3 |
| US-3 | Hologic DBT | 2.0 | 0.995 [min: 0.972, max: 0.998] | 0.743 | Hologic (DBT), V 2.0 |
| US-4 | Hologic FFDM | 1.2 | 0.994 [min: 0.962, max: 0.982] | 0.785 | Hologic (FFDM), V 1.2 |
| Center | AI Score | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | |
| US-2 | +0.37 | −4.8 | +5.54 | +5.82 | −3.71 | −5.71 | +0.41 | +1.29 | +0.65 | +0.14 |
| US-3 | +0.94 | −1.64 | −2.21 | −0.95 | −0.11 | +1.22 | +0.76 | +1.18 | +0.7 | +0.11 |
| US-4 | +1.47 | +3.09 | −0.44 | −1.02 | −2.25 | −1.79 | +0.3 | −0.18 | +0.82 | +0 |
| Center | Manufacturer and Modality | Version | PCC | χ² p-Value | Reference | Mismatch Cause |
|---|---|---|---|---|---|---|
| US-1 | Hologic FFDM | 1.2 | 0.714 | 0.026 | Hologic (DBT), V 2.0 | Wrong modality, Wrong version |
| US-2 | Hologic FFDM | 1.3 | 0.825 | 0.320 | Fuji (FFDM), V 1.3 | Wrong manufacturer |
| US-3 | Hologic DBT | 2.0 | 0.707 | 0.221 | Fuji (FFDM), V 1.3 | Wrong manufacturer, Wrong version |
| US-4 | Hologic FFDM | 1.2 | 0.364 | 0.026 | Fuji (FFDM), V 1.3 | Wrong manufacturer, Wrong version |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aguilar, C.; Pacilè, S.; Weber, N.; Fillard, P. Monitoring Methodology for an AI Tool for Breast Cancer Screening Deployed in Clinical Centers. Life 2023, 13, 440. https://doi.org/10.3390/life13020440
Aguilar C, Pacilè S, Weber N, Fillard P. Monitoring Methodology for an AI Tool for Breast Cancer Screening Deployed in Clinical Centers. Life. 2023; 13(2):440. https://doi.org/10.3390/life13020440
Chicago/Turabian StyleAguilar, Carlos, Serena Pacilè, Nicolas Weber, and Pierre Fillard. 2023. "Monitoring Methodology for an AI Tool for Breast Cancer Screening Deployed in Clinical Centers" Life 13, no. 2: 440. https://doi.org/10.3390/life13020440