
Outcome of Partial Adrenalectomy in MEN2 Syndrome: Personal Experience and Systematic Review of Literature
 , ,
, , 
Abstract
:1. Introduction
2. Material and Methods
2.1. Our Experience
2.1.1. Study Population
2.1.2. Definitions
2.2. Systematic Review
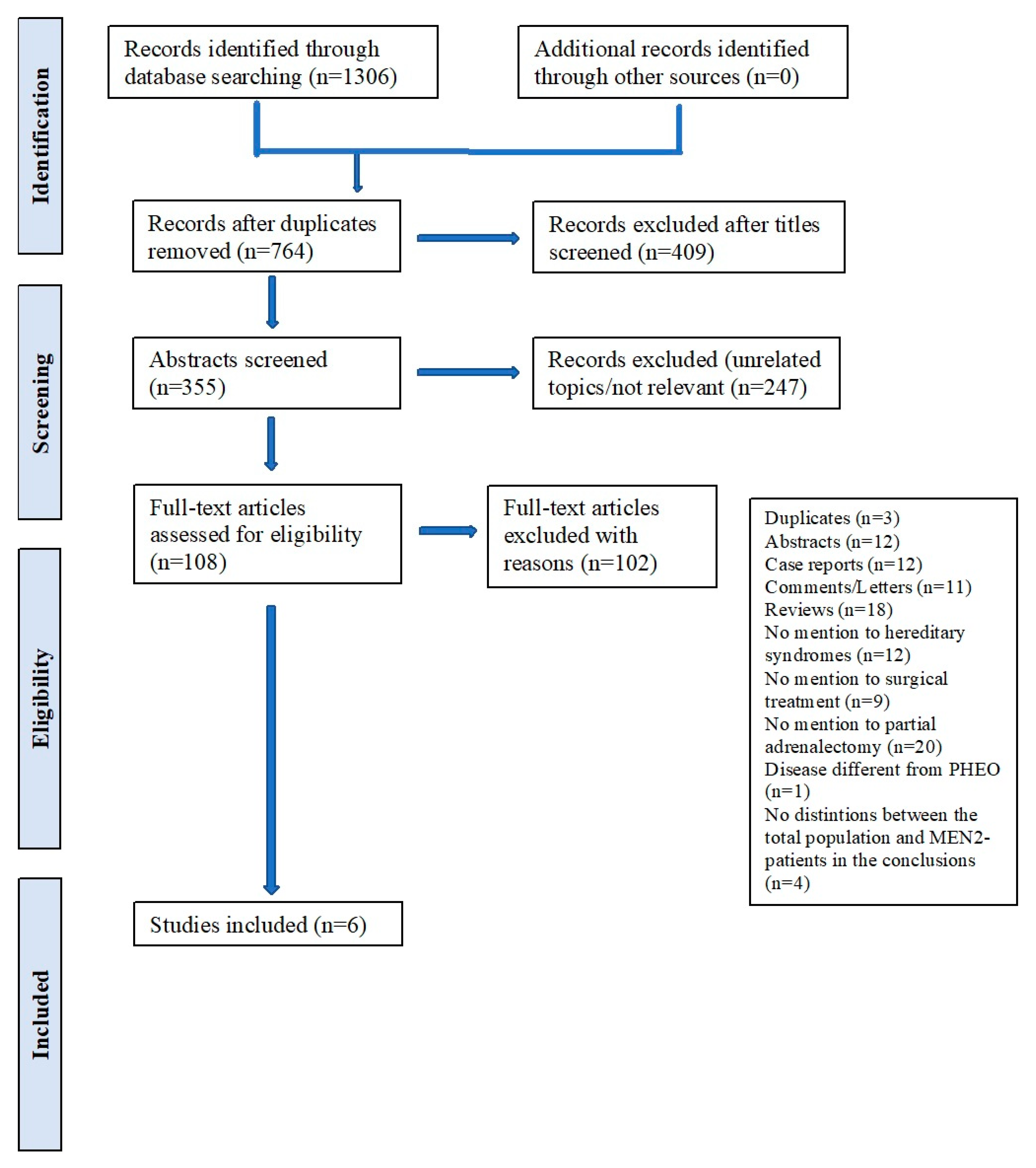
2.2.1. Search Strategy
2.2.2. Eligibility Criteria
2.2.3. Study Selection and Quality Assessment
3. Results-Comparison with Our Experience
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Machens, A.; Brauckhoff, M.; Gimm, O.; Dralle, H. Risk-Oriented Approach to Hereditary Adrenal Pheochromocytoma. In Proceedings of the Annals of the New York Academy of Sciences; Blackwell Publishing Inc.: Hoboken, NJ, USA, 2006; Volume 1073, pp. 417–428. [Google Scholar]
- Gomella, P.T.; Sanford, T.H.; Pinto, P.A.; Bratslavsky, G.; Metwalli, A.R.; Linehan, W.M.; Ball, M.W. Long-Term Functional and Oncologic Outcomes of Partial Adrenalectomy for Pheochromocytoma. Urology 2020, 140, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Kaye, D.R.; Storey, B.B.; Pacak, K.; Pinto, P.A.; Linehan, W.M.; Bratslavsky, G. Partial Adrenalectomy: Underused First Line Therapy for Small Adrenal Tumors. J. Urol. 2010, 184, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Kaman, L.; Behera, A.; Singh, R.; Katariya, R.N. Surgical Management of Phaeochromocytoma. Asian J. Surg. 2002, 25, 139–144. [Google Scholar] [CrossRef]
- Hallin Thompson, L.; Makay, Ö.; Brunaud, L.; Raffaelli, M.; Bergenfelz, A. Adrenalectomy for Incidental and Symptomatic Phaeochromocytoma: Retrospective Multicentre Study Based on the Eurocrine® Database. Br. J. Surg. 2021, 108, 1199–1206. [Google Scholar] [CrossRef] [PubMed]
- Därr, R.; Lenders, J.W.M.; Hofbauer, L.C.; Bornstein, S.R.; Naumann, B.; Eisenhofer, G. Pheochromocytoma-Update on Disease Management. Ther. Adv. Endocrinol. Metab. 2012, 3, 11–26. [Google Scholar] [CrossRef]
- Colleselli, D.; Janetschek, G. Current Trends in Partial Adrenalectomy. Curr. Opin. Urol. 2015, 25, 89–94. [Google Scholar] [CrossRef]
- Cheng, S.P.; Saunders, B.D.; Gauger, P.G.; Doherty, G.M. Laparoscopic Partial Adrenalectomy for Bilateral Pheochromocytomas. Ann. Surg. Oncol. 2008, 15, 2506–2508. [Google Scholar] [CrossRef]
- Gupta, A.; Agarwala, S.; Tandon, N.; Srinivas, M.; Bajpai, M.; Gupta, D.K.; Gupta, A.K.; Bal, C.; Kumar, R.; Bhatnagar, V. Pheochromocytoma Management, Outcomes and the Role of Cortical Preservation. Indian J. Pediatr. 2014, 81, 780–784. [Google Scholar] [CrossRef]
- Kwak, J.H.; Lee, K.E. Minimally Invasive Adrenal Surgery. Endocrinol. Metab. 2021, 35, 774–783. [Google Scholar] [CrossRef]
- Castinetti, F.; Taieb, D.; Henry, J.F.; Walz, M.; Guerin, C.; Brue, T.; Conte-Devolx, B.; Neumann, H.P.H.; Sebag, F. Outcome of Adrenal Sparing Surgery in Heritable Pheochromocytoma. Eur. J. Endocrinol. 2016, 174, R9–R18. [Google Scholar] [CrossRef] [Green Version]
- Scholten, A.; Valk, G.D.; Ulfman, D.; Borel, R.I.H.M.; Vriens, M.R. Unilateral Subtotal Adrenalectomy for Pheochromocytoma in Multiple Endocrine Neoplasia Type 2 Patients: A Feasible Surgical Strategy. Ann. Surg. 2011, 254, 1022–1027. [Google Scholar] [CrossRef] [PubMed]
- Alesina, P.F.; Knyazeva, P.; Hinrichs, J.; Walz, M.K. Tailored Approach in Adrenal Surgery: Retroperitoneoscopic Partial Adrenalectomy. Front. Endocrinol. 2022, 13, 855326. [Google Scholar] [CrossRef] [PubMed]
- Rossitti, H.M.; Söderkvist, P.; Gimm, O. Extent of Surgery for Phaeochromocytomas in the Genomic Era. Br. J. Surg. 2018, 105, e84–e98. [Google Scholar] [CrossRef] [PubMed]
- Sanford, T.H.; Storey, B.B.; Linehan, W.M.; Rogers, C.A.; Pinto, P.A.; Bratslavsky, G. Outcomes and Timing for Intervention of Partial Adrenalectomy in Patients with a Solitary Adrenal Remnant and History of Bilateral Phaeochromocytomas. BJU Int. 2011, 107, 571–575. [Google Scholar] [CrossRef] [PubMed]
- Edström, E.; Gröndal, S.; Norström, F.; Palmér, M.; Svensson, K.-A.; Widell, H.; Hamberger, B. Long Term Experience after Subtotal Adrenalectomy for Multiple Endocrine Neoplasia Type IIa. Eur. J. Surg. 1999, 165, 431–435. [Google Scholar]
- Gupta, G.N.; Benson, J.S.; Ross, M.J.; Sundaram, V.S.; Lin, K.Y.; Pinto, P.A.; Linehan, W.M.; Bratslavsky, G. Perioperative, Functional, and Oncologic Outcomes of Partial Adrenalectomy for Multiple Ipsilateral Pheochromocytomas. J. Endourol. 2014, 28, 112–116. [Google Scholar] [CrossRef]
- Kaouk, J.H.; Matin, S.; Bravo, E.L.; Gill, I.S. Laparoscopic Bilateral Partial Adrenalectomy for Pheochromocytoma. Urology 2002, 60, 1100–1103. [Google Scholar] [CrossRef]
- Nagaraja, V.; Eslick, G.D.; Edirimanne, S. Recurrence and Functional Outcomes of Partial Adrenalectomy: A Systematic Review and Meta-Analysis. Int. J. Surg. 2015, 16, 7–13. [Google Scholar] [CrossRef]
- Cavallaro, G.; Letizia, C.; Polistena, A.; de Toma, G. Laparoscopic Adrenal-Sparing Surgery: Personal Experience, Review on Technical Aspects. Updates Surg. 2011, 63, 35–38. [Google Scholar] [CrossRef]
- Amodru, V.; Taieb, D.; Guerin, C.; Romanet, P.; Paladino, N.; Brue, T.; Cuny, T.; Barlier, A.; Sebag, F.; Castinetti, F. MEN2-Related Pheochromocytoma: Current State of Knowledge, Specific Characteristics in MEN2B, and Perspectives. Endocrine 2020, 69, 496–503. [Google Scholar] [CrossRef]
- Lenders, J.W.M.; Duh, Q.Y.; Eisenhofer, G.; Gimenez-Roqueplo, A.P.; Grebe, S.K.G.; Murad, M.H.; Naruse, M.; Pacak, K.; Young, W.F. Pheochromocytoma and Paraganglioma: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2014, 99, 1915–1942. [Google Scholar] [CrossRef] [Green Version]
- Mete, O.; Asa, S.L.; Gill, A.J.; Kimura, N.; de Krijger, R.R.; Tischler, A. Overview of the 2022 WHO Classification of Paragangliomas and Pheochromocytomas. Endocr. Pathol. 2022, 33, 90–114. [Google Scholar] [CrossRef]
- Raue, F.; Frank-Raue, K. Genotype-Phenotype Relationship in Multiple Endocrine Neoplasia Type 2. Implications for Clinical Management. Hormones 2009, 8, 23–28. [Google Scholar] [CrossRef]
- Bhambhvani, H.P.; Daneshvar, M.A.; Peterson, D.J.; Ball, M.W. Partial versus Total Adrenalectomy for Pheochromocytoma: A Population-Based Comparison of Outcomes. Int. Urol. Nephrol. 2021, 53, 2485–2492. [Google Scholar] [CrossRef]
- Karagiannis, A.; Mikhailidis, D.P.; Athyros, V.G.; Harsoulis, F. Pheochromocytoma: An Update on Genetics and Management. Endocr. Relat. Cancer 2007, 14, 935–956. [Google Scholar] [CrossRef]
- Inabnet, W.B.; Caragliano, P.; Pertsemlidis, D. Pheochromocytoma: Inherited Associations, Bilaterality, and Cortex Preservation. Surgery 2000, 128, 1007–1012. [Google Scholar] [CrossRef]
- Machens, A.; Dralle, H. Advances in Risk-Oriented Surgery for Multiple Endocrine Neoplasia Type 2. Endocr. Relat. Cancer 2018, 25, T41–T52. [Google Scholar] [CrossRef]
- Raffaelli, M.; de Crea, C.; Bellantone, R. Laparoscopic Adrenalectomy. Gland Surg. 2019, 8, S41–S52. [Google Scholar] [CrossRef]
- Miccoli, P.; Raffaelli, M.; Berti, P.; Materazzi, G.; Massi, M.; Bernini, G. Adrenal Surgery before and after the Introduction of Laparoscopic Adrenalectomy. Br. J. Surg. 2002, 89, 779–782. [Google Scholar] [CrossRef]
- de Crea, C.; Raffaelli, M.; D’Amato, G.; Princi, P.; Gallucci, P.; Bellantone, R.; Lombardi, C.P. Retroperitoneoscopic Adrenalectomy: Tips and Tricks. Updates Surg. 2017, 69, 267–270. [Google Scholar] [CrossRef]
- Raffaelli, M.; Gallucci, P.; Voloudakis, N.; Pennestrì, F.; de Cicco, R.; Arcuri, G.; de Crea, C.; Bellantone, R. The New Robotic Platform HugoTM RAS for Lateral Transabdominal Adrenalectomy: A First World Report of a Series of Five Cases. Updates Surg. 2022, 75, 217–225. [Google Scholar] [CrossRef]
- de Crea, C.; Arcuri, G.; Pennestrì, F.; Paolantonio, C.; Bellantone, R.; Raffaelli, M. Robotic Adrenalectomy: Evaluation of Cost-Effectiveness. Gland Surg. 2020, 9, 831–839. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; Moher, D.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. PRISMA 2020 Explanation and Elaboration: Updated Guidance and Exemplars for Reporting Systematic Reviews. BMJ 2021, 372, n160. [Google Scholar] [CrossRef] [PubMed]
- Nambirajan, T.; Leeb, K.; Neumann, H.P.H.; Graubner, U.B.; Janetschek, G. Laparoscopic Adrenal Surgery for Recurrent Tumours in Patients with Hereditary Phaeochromocytoma. Eur. Urol. 2005, 47, 622–626. [Google Scholar] [CrossRef]
- Walz, M.K.; Alesina, P.F.; Wenger, F.A.; Koch, J.A.; Neumann, H.P.H.; Petersenn, S.; Schmid, K.W.; Mann, K. Laparoscopic and Retroperitoneoscopic Treatment of Pheochromocytomas and Retroperitoneal Paragangliomas: Results of 161 Tumors in 126 Patients. World J. Surg. 2006, 30, 899–908. [Google Scholar] [CrossRef] [PubMed]
- Perysinakis, I.; Aggeli, C.; Kaltsas, G.; Zografos, G.N. Adrenal-Sparing Surgery: Current Concepts on a Theme from the Past. Hormones 2000, 19, 317–327. [Google Scholar] [CrossRef]
- Germain, A.; Klein, M.; Brunaud, L. Surgical Management of Adrenal Tumors. J. Visc. Surg. 2011, 148, e250–e261. [Google Scholar] [CrossRef]
- Decourcy, J.L. Subtotal Bilateral Adrenalectomy for Hyper-Adrenalism (Essential Hypertension). Ann. Surg. 1934, 100, 310. [Google Scholar] [CrossRef]
- Asher, K.P.; Gupta, G.N.; Boris, R.S.; Pinto, P.A.; Linehan, W.M.; Bratslavsky, G. Robot-Assisted Laparoscopic Partial Adrenalectomy for Pheochromocytoma: The National Cancer Institute Technique. Eur. Urol. 2011, 60, 118–124. [Google Scholar] [CrossRef]
- Sasagawa, I.; Suzuki, Y.; Itoh, K.; Izumi, T.; Miura, M.; Suzuki, H.; Tomita, Y. Posterior Retroperitoneoscopic Partial Adrenalectomy: Clinical Experience in 47 Procedures. Eur. Urol. 2003, 43, 381–385. [Google Scholar] [CrossRef]
- Boris, R.S.; Gupta, G.; Linehan, W.M.; Pinto, P.A.; Bratslavsky, G. Robot-Assisted Laparoscopic Partial Adrenalectomy: Initial Experience. Urology 2011, 77, 775–780. [Google Scholar] [CrossRef] [Green Version]
- Kawasaki, Y.; Ishidoya, S.; Kaiho, Y.; Ito, A.; Satoh, F.; Morimoto, R.; Nakagawa, H.; Arai, Y. Laparoscopic Simultaneous Bilateral Adrenalectomy: Assessment of Feasibility and Potential Indications. Int. J. Urol. 2011, 18, 762–767. [Google Scholar] [CrossRef] [PubMed]
- Calì, B.; Nomine-Criqui, C.; Bihain, F.; Brunaud, L. Robotic Approach for Partial Adrenalectomy. Updates Surg. 2021, 73, 1147–1154. [Google Scholar] [CrossRef]
- Liao, C.H.; Chung, S.D.; Lai, M.K.; Yu, H.J.; Chueh, S.C. Laparoscopic Simultaneous Bilateral Partial and Total Adrenalectomy: A Longer Follow-Up. BJU Int. 2009, 104, 1269–1273. [Google Scholar] [CrossRef] [PubMed]
- Moore, E.C.; Berber, E. Fluorescence Techniques in Adrenal Surgery. Gland Surg. 2019, 8, S22–S27. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Age | Gender | Year | MEN2 Syndrome | Laterality | Procedure | Operative Time (Minutes) | POS (Days) | Follow-Up |
|---|---|---|---|---|---|---|---|---|
| 28 | Female | 2017 | 2B (no further informations available) | Right Metachronous (Left TLA TA, 2010) | Right PA (TLA) | 70 | 7. No post-operative complications | 60 months: Right recurrence that required right CA. Hydrocortison 30 mg/day |
| 36 | Female | 2020 | 2A, C634R | Bilateral Synchronous | Left TA + Right PA (PRA) | 118 | 4. No post-operative complications | 23 months. No recurrence. Hydrocortison 10 mg/day |
| 36 | Male | 2021 | 2A, C634R | Left Metachronous (Right TLA TA, 2014) | Left PA (TLA) | 53 | 3. No post-operative complications | 20 months. No recurrence. Hydrocortison 20 mg/day |
| 26 | Male | 2021 | 2A, C634R | Right | Right PA (TLA) | 77 | 2. No post-operative complications | 11 months. No recurrence. No SI |
| 51 | Female | 2022 | 2A, C618R | Left Metachronous (Right TLA TA, 2011) | Left PA (TLA) | 67 | 3. No post-operative complications | 3 months. No recurrence. Hydrocortison 20 mg/day |
| 39 | Female | 2022 | 2A, C634R | Bilateral Synchronous | Right TA + Left PA (PRA) | 75 | 5. No post-operative complications | 1 month. No recurrence. Hydrocortison 30 mg/day |
| Article | Study Type | PHEO | MEN2 (%) | Median Age | Laterality | First Surgery | R (Months after the Primary Tumor) | S-PHEO | M-PHEO (Months after the Primary Tumor) | Redo Surgery | FU | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| TA | PA | TA | PA | |||||||||||||||
| UL | BL | UL | BL | UL | BL | IL | CL | IL | CL | |||||||||
| Gupta et al., 2014 [17] | Retrosp. Study | 10 | 1 (10) | 30.6 | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 12 |
| Cavallaro et al., 2011 [20] | Retrosp. Study | 3 | 3 (100) | 37 | 0 | 3 | 3 | 0 | 3 | 0 | 0 | 3 | 0 | 0 | 0 | 0 | 0 | 12 |
| Edstrom et al., 1999 [16] | Retrosp. Study | 5 | 5 (100) | 38 | 3 | 2 | 4 | 0 | 3 | 0 | 0 | 2 | 3 (108) | 0 | 0 | 0 | 3 | 132 |
| Scholten et al., 2011 [12] | Retrosp. Study | 61 | 61 (100) | 33 | 37 | 24 | 30 | 22 | 7 | 2 | 3 (4.9) | 24 | 17 (6.3) | 3 | 13 | 0 | 4 | 16.2 |
| Nambirajan et al., 2005 [35] | Retrosp. Study | 5 | 1 (20) | 24 | 1 | 0 | 0 | 0 | 1 | 0 | 1 (NR) | 0 | 0 | 1 | 0 | 0 | 0 | NR |
| Walz et al., 2006 [36] | Prosp. Study | 134 | 12 (9) | 41.7 | 4 | 6 | 5 | 0 | 7 | 3 | 0 | 6 | 2 (120) | 0 | 0 | 0 | 2 | 36 |
| Our experience | 194 | 6 (3) | 36 | 4 | 2 | 5 | 0 | 3 | 0 | 1 (48) | 2 | 3 (84) | 1 | 0 | 0 | 3 | 15.5 | |
| Article | Bilateral Adrenalectomies | First Surgery | Synchronous PHEO | Recurrences | Metachronous PHEO | Second Surgery | Third Surgery | SI |
|---|---|---|---|---|---|---|---|---|
| Cavallaro et al., 2011 [20] | 3 | 3 UL TA+ CL PA | 3 | 0 | 0 | / | 1 (33.3%) | |
| Edstrom et al., 1999 [16] | 5 | 2 UL TA + CL PA | 2 | 0 | 0 | / | 1 (20%) | |
| 2 UL TA | 0 | 0 | 2 | 2 CL PA | ||||
| 1 UL PA | 0 | 0 | 1 | 1 CL TA | ||||
| Scholten et al., 2011 [12] | 42 | 22 BL TA | 22 | 0 | 0 | / | 35 (83%) | |
| 2 BL PA | 2 | 2 | 0 | 2 IL TA | ||||
| 13 UL TA | 0 | 0 | 13 | 11 CL TA 2 CL PA | ||||
| 5 UL PA | 0 | 0 | 4 | 2 CL TA 2 CL PA | / | |||
| 0 | 1 | 0 | 1 BL TA | / | ||||
| Walz, 2006 [36] | 8 | 3 BL PA | 3 | 0 | 0 | / | / | 1 (25%) |
| 3 UL TA + CL PA | 3 | 0 | 0 | / | / | |||
| 2 UL TA | 0 | 0 | 2 | 2 CL PA | / | |||
| Our experience | 5 | 2 UL TA + CL PA | 2 | 0 | 0 | / | / | 5 (100%) |
| 3 UL TA | 0 | 1 | 3 | 3 CL PA | 1 IL TA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Procopio, P.F.; Pennestrì, F.; De Crea, C.; Voloudakis, N.; Bellantone, R.; Raffaelli, M. Outcome of Partial Adrenalectomy in MEN2 Syndrome: Personal Experience and Systematic Review of Literature. Life 2023, 13, 425. https://doi.org/10.3390/life13020425
Procopio PF, Pennestrì F, De Crea C, Voloudakis N, Bellantone R, Raffaelli M. Outcome of Partial Adrenalectomy in MEN2 Syndrome: Personal Experience and Systematic Review of Literature. Life. 2023; 13(2):425. https://doi.org/10.3390/life13020425
Chicago/Turabian StyleProcopio, Priscilla Francesca, Francesco Pennestrì, Carmela De Crea, Nikolaos Voloudakis, Rocco Bellantone, and Marco Raffaelli. 2023. "Outcome of Partial Adrenalectomy in MEN2 Syndrome: Personal Experience and Systematic Review of Literature" Life 13, no. 2: 425. https://doi.org/10.3390/life13020425