
Cutaneous Manifestations of Lyme Borreliosis in Children—A Case Series and Review
 , , and
, , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Series
2.1. Case 1
2.2. Case 2
2.3. Case 3
3. Discussion
3.1. Cutaneous Manifestations of Lyme Disease
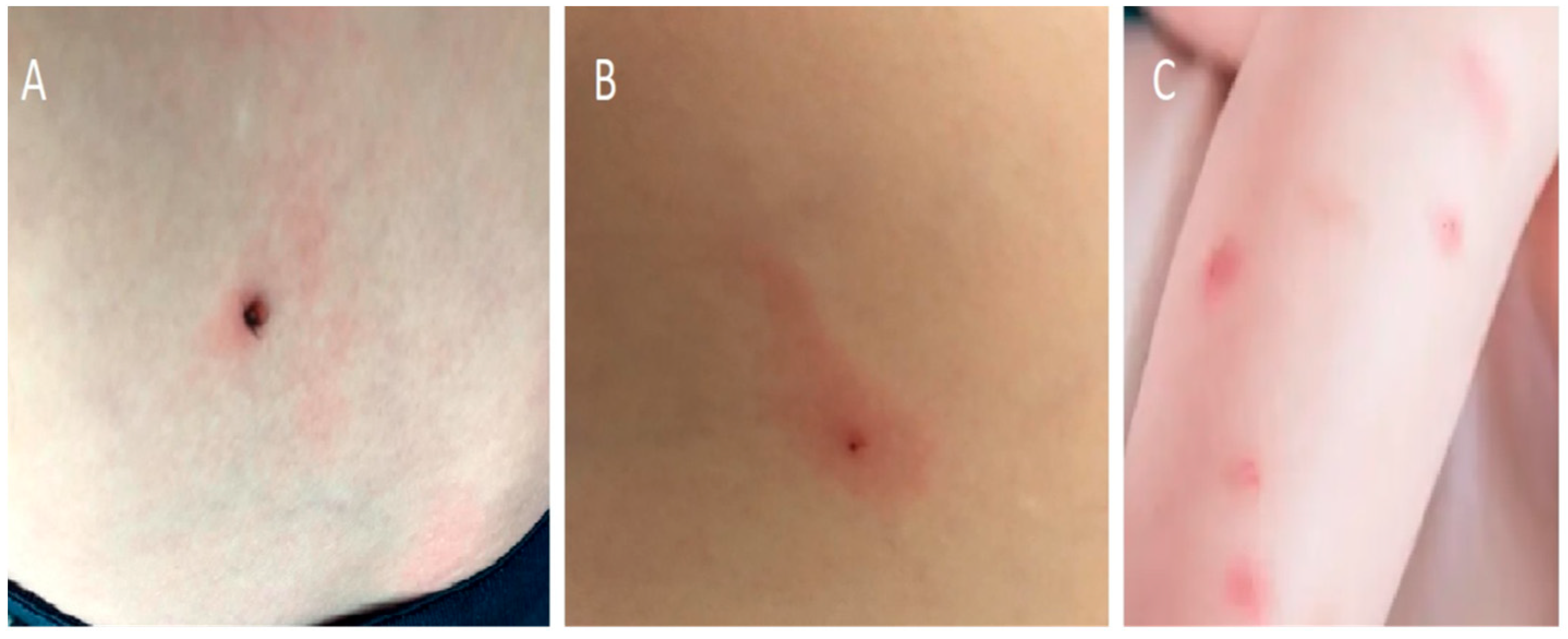
3.2. Tick-Bite without Erythema Migrans
3.3. Erythema Migrans
3.4. Multiple Erythema Migrans (MEM)
3.5. Acrodermatitis Chronica Atrophicans
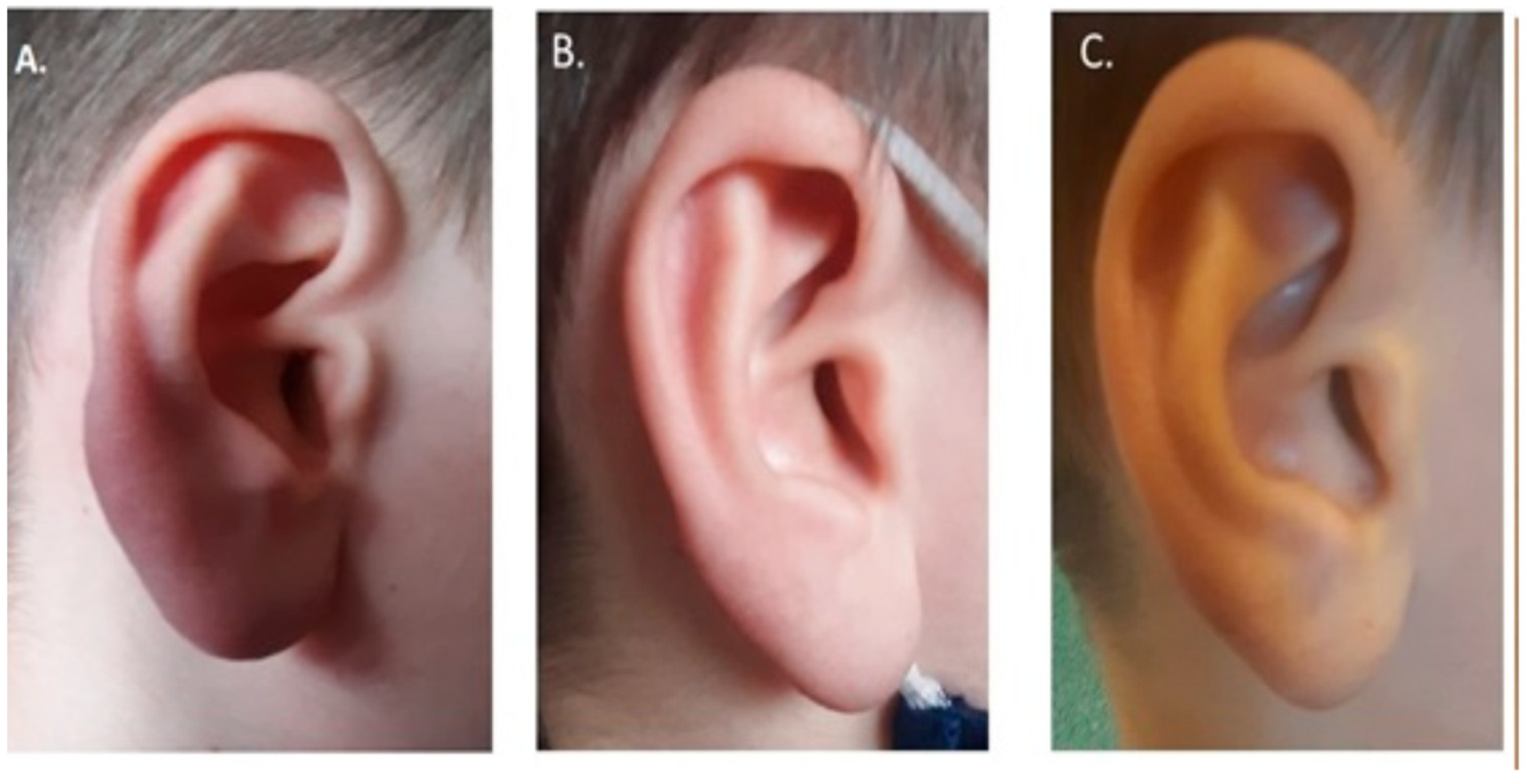
3.6. Borrelial Lymphocytoma
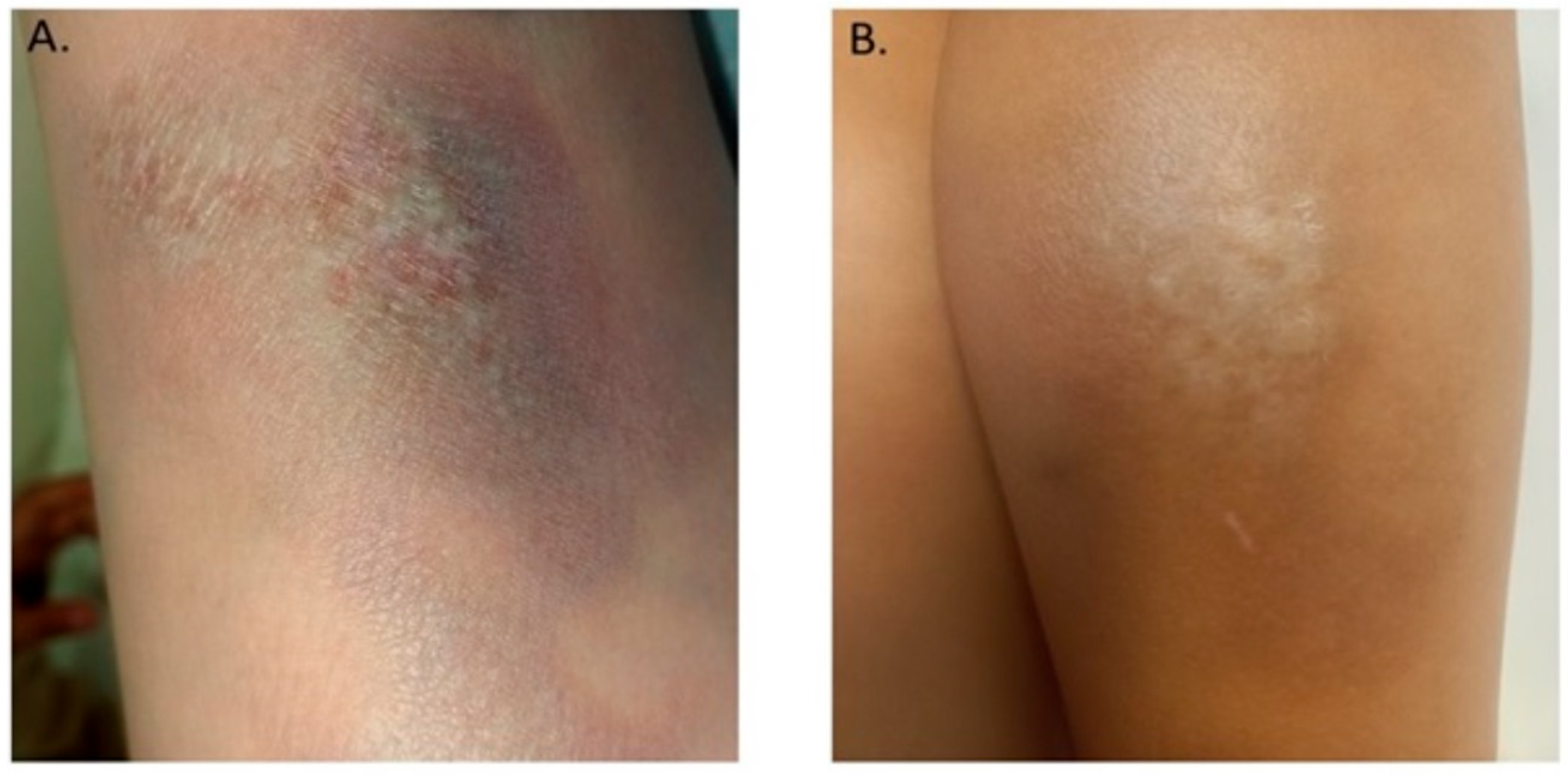
3.7. Localized Scleroderma (Morphea)
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Kmieciak, W.; Ciszewski, M.; Szewczyk, E.M. Choroby odkleszczowe w Polsce—Występowanie i trudności diagnostyczne [Tick-borne diseases in Poland: Prevalence and difficulties in diagnostics]. Med. Pract. 2016, 67, 73–87. [Google Scholar]
- Rizzoli, A.; Hauffe, H.C.; Carpi, G.; Vourch’h, G.I.; Neteler, M.; Rosà, R. Lyme borreliosis in Europe. Euro. Surveill. 2011, 16, 9906. [Google Scholar] [CrossRef]
- Vandekerckhove, O.; De Buck, E.; Van Wijngaerden, E. Lyme disease in Western Europe: An emerging problem? A systematic review. Acta Clin. Belg. 2021, 76, 244–252. [Google Scholar] [CrossRef] [PubMed]
- Myszkowska-Torz, A.; Mazur-Melewska; Tomaszewski, M.; Mania, A.; Figlerowicz, M. Lyme borreliosis in children-trends in epidemiology. A single center study. Ped. Pol. 2022; accepted. [Google Scholar]
- Pancewicz, S.A.; Garlicki, A.M.; Moniuszko-Malinowska, A.; Zajkowska, J.; Kondrusik, M.; Grygorczuk, S.; Czupryna, P.; Dunaj, J.; Polish Society of Epidemiology and Infectious Diseases. Diagnosis and treatment of tick-borne diseases: Recommendations of the Polish Society of Epidemiology and Infectious Diseases. Przegl. Epidemiol. 2015, 69, 421–428. [Google Scholar]
- Rauter, C.; Hartung, T. Prevalence of Borrelia burgdorferi sensu lato genospecies in Ixodes ricinus ticks in Europe: A metaanalysis. Appl. Environ. Microbiol. 2005, 71, 7203–7216. [Google Scholar] [CrossRef] [Green Version]
- Arnez, M.; Pleterski-Rigler, D.; Luznik-Bufon, T.; Ruzic-Sabljić, E.; Strle, F. Solitary and multiple erythema migrans in children: Comparison of demographic, clinical and laboratory findings. Infection 2003, 31, 404–409. [Google Scholar] [CrossRef]
- Müllegger, R.R.; Glatz, M. Skin manifestations of Lyme borreliosis: Diagnosis and management. Am. J. Clin. Dermatol. 2008, 9, 355–368. [Google Scholar] [CrossRef]
- Hu, L.; Shapiro, E.D. Treatment of Lyme disease. In UpToDate; Post, T.W., Ed.; UpToDate: Waltham, MA, USA, 2022. [Google Scholar]
- Hofman, H. The variable spectrum of cutaneous Lyme borreliosis. Diagnosis and therapy. Hautarzt 2012, 63, 381–389. [Google Scholar] [CrossRef]
- Patey, O. Borréliose de Lyme: Mesures préventives secondaires après piqûre de tiques. Med. Mal. Infect. 2007, 37, 446–455. [Google Scholar] [CrossRef]
- Lantos, P.M.; Rumbaugh, J.; Bockenstedt, L.K.; Falck-Ytter, Y.; Aguero-Rosenfeld, M.; Auwaerter, P.G.; Baldwin, K.; Bannuru, R.R.; Belani, K.K.; Bowie, W.R.; et al. Clinical Practice Guidelines by the Infectious Diseases Society of America (IDSA), American Academy of Neurology (AAN), and American College of Rheumatology (ACR): 2020 Guidelines for the Prevention, Diagnosis and Treatment of Lyme Disease. Clin. Infect. Dis. 2021, 72, e1–e48. [Google Scholar] [CrossRef] [PubMed]
- Cruickshank, M.; O’Flynn, N.; Faust, S.N. Guideline Committee. Lyme disease: Summary of NICE guidance. BMJ 2018, 361, k1261. [Google Scholar]
- Figoni, J.; Chirouze, C.; Hansmann, Y.; Lemogne, C.; Hentgen, V.; Saunier, A.; Bouiller, K.; Gehanno, J.F.; Rabaud, C.; Perrot, S.; et al. Lyme borreliosis and other tick-borne diseases. Guidelines from the French Scientific Societies (I): Prevention, epidemiology, diagnosis. Med. Mal. Infect. 2019, 49, 318–324. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatrics. Lyme disease. In Red Book: 2018 Report of the Committee on Infectious Diseases, 31st ed.; Kimberlin, D.W., Brady, M.T., Jackson, M.A., Long, S.S., Eds.; American Academy of Pediatrics: Itasca, IL, USA, 2018; pp. 515–523. [Google Scholar]
- Smith, R.P.; Schoen, R.T.; Rahn, D.W.; Sikand, V.K.; Nowakowski, J.; Parenti, D.L.; Holman, M.S.; Persing, D.H.; Steere, A.C. Clinical characteristics and treatment outcome of early Lyme disease in patients with microbiologically confirmed erythema migrans. Ann. Intern. Med. 2002, 136, 421–428. [Google Scholar] [CrossRef]
- Trevisan, G.; Bonin, S.; Ruscio, M. A practical approach to the diagnosis of Lyme borreliosis: From clinical heterogeneity to laboratory methods. Front. Med. 2020, 7, 265. [Google Scholar] [CrossRef]
- Volovitz, B.; Shkap, R.; Amir, J.; Calderon, S.; Varsano, I.; Nussinovitch, M. Absence of tooth staining with doxycycline treatment in young children. Clin. Pediatr. 2007, 46, 121–126. [Google Scholar] [CrossRef]
- Pöyhönen, H.; Nurmi, M.; Peltola, V.; Alaluusua, S.; Ruuskanen, O.; Lähdesmäki, T. Dental staining after doxycycline use in children. J. Antimicrob. Chemother. 2017, 72, 2887–2890. [Google Scholar] [CrossRef] [Green Version]
- Wormser, G.P.; Strle, F.; Shapiro, E.D. Is Doxycycline Appropriate for Routine Treatment of Young Children with Erythema Migrans? Pediatr. Infect. Dis. J. 2019, 38, 1113–1114. [Google Scholar] [CrossRef]
- Bennet, L.; Danell, S.; Berglund, J. Clinical outcome of erythema migrans after treatment with phenoxymethyl penicillin. Scand. J. Infect. Dis. 2003, 35, 129–131. [Google Scholar] [CrossRef]
- Arnez, M.; Ruzic-Sabljic, E. Borrelia burgdorferi sensu lato bacteremia in Slovenian children with solitary and multiple erythema migrans. Pediatr. Infect. Dis. J. 2011, 30, 988–990. [Google Scholar] [CrossRef]
- Sharma, A.; Guleria, S.; Sharma, R.; Sharma, A. Lyme disease: A case report with typical and atypical lesions. Indian Dermatol. Online J. 2017, 8, 124–127. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.S.; Varatharaj Palraj, B.R. Multiple erythema migrans rashes characteristic of early disseminated Lyme disease, before and after therapy. Mayo Clin. Proc. 2019, 94, 172–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glatz, M.; Resinger, A.; Semmelweis, K.; Ambros-Rudolph, C.M.; Müllegger, R.R. Clinical spectrum of skin manifestations of Lyme borreliosis in 204 children in Austria. Acta Derm. Venereol. 2015, 95, 565–571. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moniuszko-Malinowska, A.; Czupryna, P.; Dunaj, J.; Pancewicz, S.; Garkowski, A.; Kondrusik, M.; Grygorczuk, S.; Zajkowska, J. Acrodermatitis chronica atrophicans: Various faces of the late form of Lyme borreliosis. Post Derm. Alerg. 2018, 35, 490–494. [Google Scholar] [CrossRef]
- Vasudevan, B.; Chatterjee, M. Lyme borreliosis and skin. Indian J. Dermatol. 2013, 58, 167–174. [Google Scholar] [CrossRef]
- Gade, A.; Matin, T.; Rubenstein, R.; Robinson, C.A. Acrodermatitis chronica atrophicans. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Stanek, G.; Strle, F. Lyme disease: European perspective. Infect. Dis. Clin. N. Am. 2008, 22, 327–339. [Google Scholar] [CrossRef]
- Maraspin, V.; Nahtigal Klevisar, M.; Ruzic-Sabljic, E.; Lusa, L.; Strle, F. Borrelial lymphocytoma in adult patients. Clin. Infect. Dis. 2016, 63, 914–921. [Google Scholar] [CrossRef] [Green Version]
- Arnež, M.; Ružić-Sabljić, E. Borrelial Lymphocytoma in Children. Pediatr. Infect. Dis. J. 2015, 34, 1319–1322. [Google Scholar] [CrossRef]
- Maraspin, V.; Strle, F. Borrelial lymphocytoma. Wien. Klin. Wochenschr. 2022; epub ahead of print. [Google Scholar] [CrossRef]
- Maraspin, V.; Ogrinc, K.; Ružić-Sabljić, E.; Lotrič-Furlan, S.; Strle, F. Isolation of Borrelia burgdorferi sensu lato from blood of adult patients with borrelial lymphocytoma, Lyme neuroborreliosis, Lyme arthritis and acrodermatitis chronica atrophicans. Infection 2011, 39, 35–40. [Google Scholar] [CrossRef]
- Strle, F.; Pleterski-Rigler, D.; Stanek, G.; Pejovnik-Pustinek, A.; Ruzic, E.; Cimperman, J. Solitary borrelial lymphocytoma: Report of 36 cases. Infection 1992, 20, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Cerroni, L.; Zochling, N.; Putz, B.; Kerl, H. Infection by Borrelia burgdorferi and cutaneous B-cell lymphoma. J. Cutan. Pathol. 1997, 24, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Krasowska, D.; Rudnicka, L.; Dańczak-Pazdrowska, A.; Chodorowska, G.; Woźniacka, A.; Lis-Święty, A.; Czuwara, J.; Maj, J.; Majewski, S.; Sysa-Jędrzejowska, A.; et al. Localized scleroderma (morphea). Diagnostic and therapeutic recommendations of the Polish Dermatological Society. Przegl. Derm. 2019, 106, 333–353. [Google Scholar]
- Bahali, A.G.; Su, O.; Emiroglu, N.; Cengiz, F.P.; Kaya, O.M.; Onsun, N. Evaluation of mean platelet volume in localized scleroderma. An. Bras. Dermatol. 2017, 92, 635–637. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- George, E.; Nielson, C.B.; Vincek, V. Tick Bite-Associated Morphea: A Case Report. Am. J. Dermatopathol. 2019, 41, 747–749. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Myszkowska-Torz, A.; Tomaszewski, M.; Kotowski, M.; Witczak, C.; Figlerowicz, M.; Mazur-Melewska, K. Cutaneous Manifestations of Lyme Borreliosis in Children—A Case Series and Review. Life 2023, 13, 72. https://doi.org/10.3390/life13010072
Myszkowska-Torz A, Tomaszewski M, Kotowski M, Witczak C, Figlerowicz M, Mazur-Melewska K. Cutaneous Manifestations of Lyme Borreliosis in Children—A Case Series and Review. Life. 2023; 13(1):72. https://doi.org/10.3390/life13010072
Chicago/Turabian StyleMyszkowska-Torz, Agnieszka, Mateusz Tomaszewski, Michał Kotowski, Cezary Witczak, Magdalena Figlerowicz, and Katarzyna Mazur-Melewska. 2023. "Cutaneous Manifestations of Lyme Borreliosis in Children—A Case Series and Review" Life 13, no. 1: 72. https://doi.org/10.3390/life13010072