
A Rare Gastric Subepithelial Lesion Removed through Submucosal Tunneling Endoscopic Resection: Case Report and Literature Review


Abstract
:1. Introduction
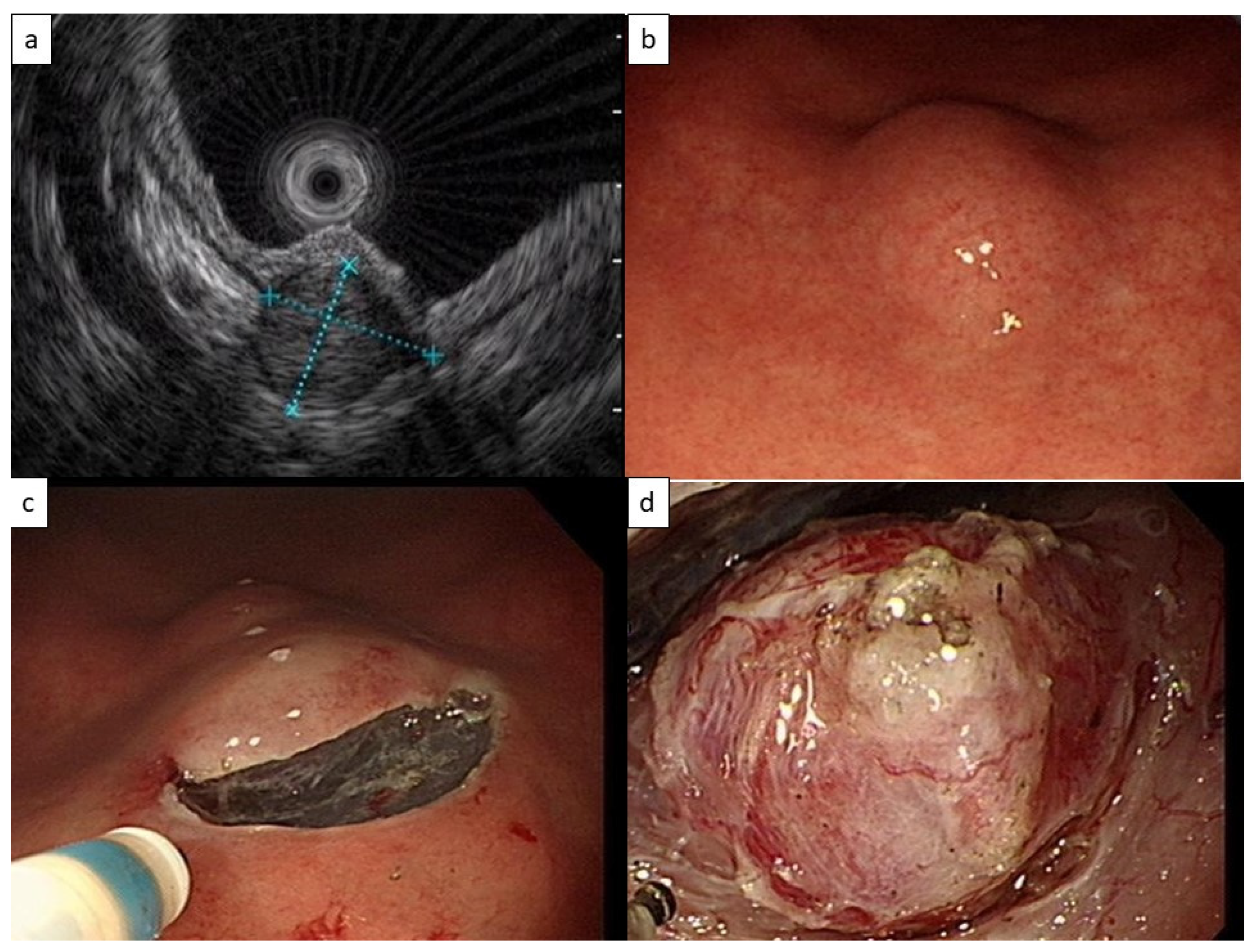
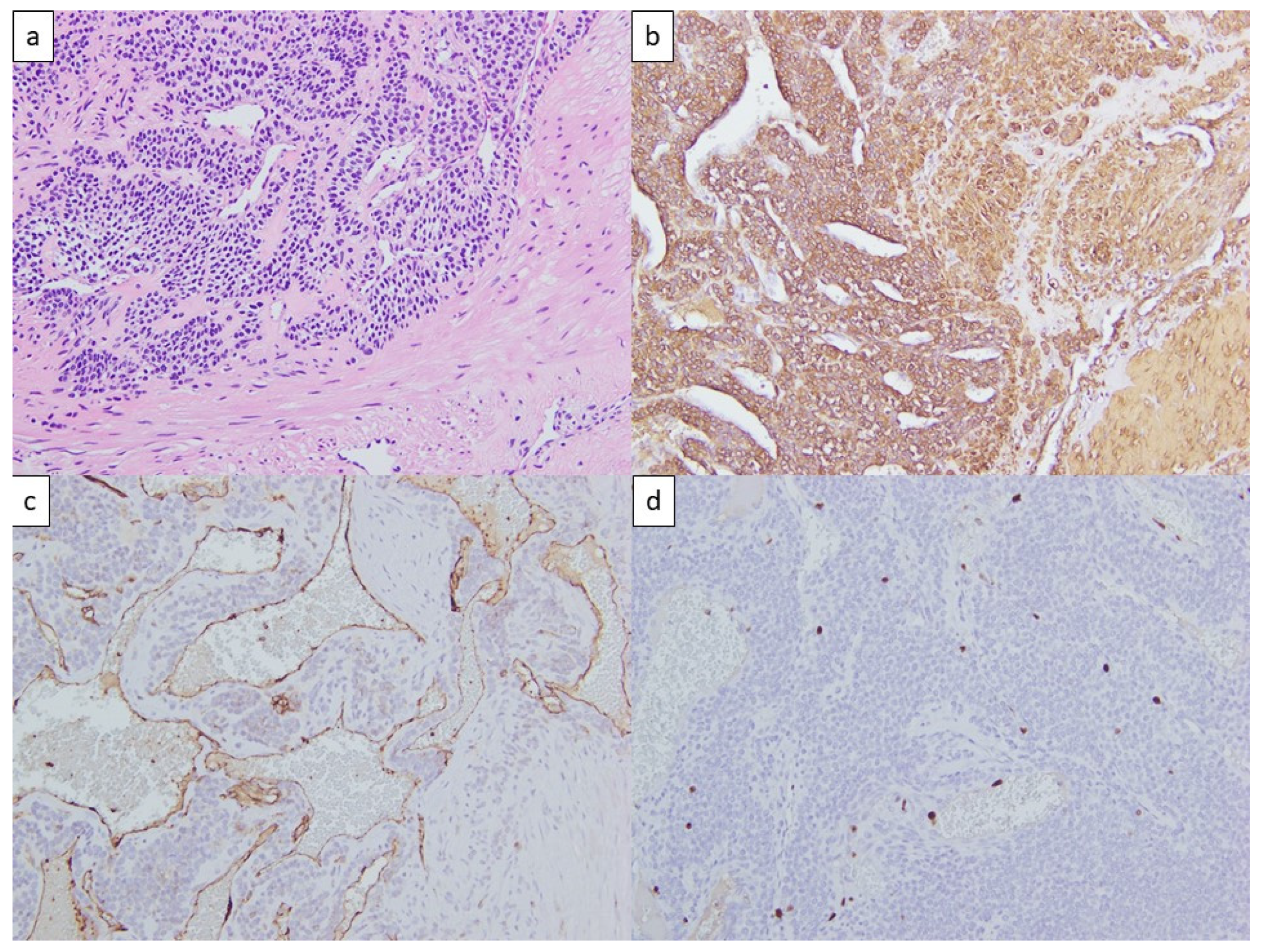
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lee, J.H.; Lee, H.L.; Ahn, Y.W.; Lee, K.N.; Jun, D.W.; Lee, O.Y.; Han, D.S.; Yoon, B.C.; Choi, H.S. Prevalence of Gastric Subepithelial Tumors in Korea: A Single Center Experience. Korean J. Gastroenterol. 2015, 66, 274–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, Y.J.; Son, H.J.; Lee, J.S.; Byun, Y.H.; Suh, H.J.; Rhee, P.L.; Kim, J.J.; Rhee, J.C. Clinical course of subepithelial lesions detected on upper gastrointestinal endoscopy. World J. Gastroenterol. 2010, 16, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Polkowski, M. Endoscopic ultrasound and endoscopic ultrasound-guided fine-needle biopsy for the diagnosis of malignant submucosal tumors. Endoscopy 2005, 37, 635–645. [Google Scholar] [CrossRef] [PubMed]
- Deprez, P.H.; Moons, L.M.G.; O’Toole, D.; Gincul, R.; Seicean, A.; Pimentel-Nunes, P.; Fernandez-Esparrach, G.; Polkowski, M.; Vieth, M.; Borbath, I.; et al. Endoscopic management of subepithelial lesions including neuroendocrine neoplasms: European Society of Gastrointestinal Endoscopy (ESGE) Guideline. Endoscopy 2022, 54, 412–429. [Google Scholar] [CrossRef] [PubMed]
- Standards of Practice Committee; Faulx, A.L.; Kothari, S.; Acosta, R.D.; Agrawal, D.; Bruining, D.H.; Chandrasekhara, V.; Eloubeidi, M.A.; Fanelli, R.D.; Gurudu, S.R.; et al. The role of endoscopy in subepithelial lesions of the GI tract. Gastrointest. Endosc. 2017, 85, 1117–1132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsagkataki, E.S.; Flamourakis, M.E.; Gkionis, I.G.; Giakoumakis, M.I.; Delimpaltadakis, G.N.; Kazamias, G.M.; Giannikaki, E.S.; Christodoulakis, M.S. Gastric glomus tumor: A case report and review of the literature. J. Med. Case Rep. 2021, 15, 415. [Google Scholar] [CrossRef] [PubMed]
- ASGE Technology Committee; Aslanian, H.R.; Sethi, A.; Bhutani, M.S.; Goodman, A.J.; Krishnan, K.; Lichtenstein, D.R.; Melson, J.; Navaneethan, U.; Pannala, R.; et al. ASGE guideline for endoscopic full-thickness resection and submucosal tunnel endoscopic resection. VideoGIE 2019, 4, 343–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharzehi, K.; Sethi, A.; Savides, T. AGA Clinical Practice Update on Management of Subepithelial Lesions Encountered During Routine Endoscopy: Expert Review. Clin. Gastroenterol. Hepatol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Casali, P.G.; Blay, J.Y.; Abecassis, N.; Bajpai, J.; Bauer, S.; Biagini, R.; Bielack, S.; Bonvalot, S.; Boukovinas, I.; Bovee, J.; et al. Gastrointestinal stromal tumours: ESMO-EURACAN-GENTURIS Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2022, 33, 20–33. [Google Scholar] [CrossRef] [PubMed]
- National Comprehensive Cancer Network. Gastrointestinal Stromal Tumors (GISTs) (Version 2.2022). Available online: https://www.nccn.org/professionals/physician_gls/pdf/gist.pdf (accessed on 2 December 2022).
- Koo, D.H.; Ryu, M.H.; Kim, K.M.; Yang, H.K.; Sawaki, A.; Hirota, S.; Zheng, J.; Zhang, B.; Tzen, C.Y.; Yeh, C.N.; et al. Asian Consensus Guidelines for the Diagnosis and Management of Gastrointestinal Stromal Tumor. Cancer Res. Treat. 2016, 48, 1155–1166. [Google Scholar] [CrossRef] [PubMed]
- Nishida, T.; Hirota, S.; Yanagisawa, A.; Sugino, Y.; Minami, M.; Yamamura, Y.; Otani, Y.; Shimada, Y.; Takahashi, F.; Kubota, T.; et al. Clinical practice guidelines for gastrointestinal stromal tumor (GIST) in Japan: English version. Int. J. Clin. Oncol. 2008, 13, 416–430. [Google Scholar] [CrossRef] [PubMed]
- Hasuda, H.; Hu, Q.; Miyashita, Y.; Zaitsu, Y.; Tsuda, Y.; Hisamatsu, Y.; Nakashima, Y.; Ando, K.; Kimura, Y.; Yamada, Y.; et al. Gastric glomus tumor with a preoperative diagnosis by endoscopic ultrasonography-guided fine needle aspiration: A case report. Int. Cancer Conf. J. 2021, 10, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Pansa, A.; Sama, L.; Ruspi, L.; Sicoli, F.; Cananzi, F.C.M.; Quagliuolo, V. Glomus tumor of the stomach: A systematic review and illustrative case report. Dig. Dis. 2022, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Folpe, A.L.; Fanburg-Smith, J.C.; Miettinen, M.; Weiss, S.W. Atypical and malignant glomus tumors: Analysis of 52 cases, with a proposal for the reclassification of glomus tumors. Am. J. Surg. Pathol. 2001, 25, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Papke, D.J., Jr.; Sholl, L.M.; Doyle, L.A.; Fletcher, C.D.M.; Hornick, J.L. Gastroesophageal Glomus Tumors: Clinicopathologic and Molecular Genetic Analysis of 26 Cases With a Proposal for Malignancy Criteria. Am. J. Surg. Pathol. 2022, 46, 1436–1446. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Ge, N.; Wang, S.; Liu, X.; Guo, J.; Wang, G.; Sun, S. The Role of Endoscopic Ultrasound and Endoscopic Resection for Gastric Glomus: A Case Series and Literature Review. J. Transl. Int. Med. 2019, 7, 149–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Zhou, P.; Xu, M.; Chen, W.; Li, Q.; Ji, Y.; Yao, L. Endoscopic diagnosis and treatment of gastric glomus tumors. Gastrointest. Endosc. 2011, 73, 371–375. [Google Scholar] [CrossRef] [PubMed]
- Xu, M.; Jiang, X.M.; He, Y.L.; Zhang, Y.L.; Xu, M.D.; Yao, L.Q. Glomus tumor of the stomach: A case treated by endoscopic submucosal dissection. Clin. Res. Hepatol. Gastroenterol. 2011, 35, 325–328. [Google Scholar] [CrossRef] [PubMed]
- Ojima, T.; Takifuji, K.; Nakamura, M.; Nakamori, M.; Hayata, K.; Kitadani, J.; Yamaue, H. Endoscopic submucosal tunnel dissection versus conventional endoscopic submucosal dissection for early gastric cancers: Outcomes of 799 consecutive cases in a single institution. Surg. Endosc. 2020, 34, 5625–5631. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Society, Year | Timing for Tissue Acquisition | Gastric GIST, <20 mm, without High-Risk Features 1 | Gastric SELs with Unclear Diagnosis |
|---|---|---|---|
| ESGE, 2022 [4] |
| Surveillance or resection | <10 mm EGD at 3–6 months, then at 2–3 years interval 10–20 mm EGD at 3–6 months, then at 1–2 years interval. Diagnostic resection is an alternative for SELs <20 mm after failure of attempts to obtain diagnosis >20 mm EGD + EUS at 6 months, then at 6–12 months interval |
| AGA, 2022 [8] | Lesion arising from muscularis propria layer | Surveillance with EUS, 1 year interval | Not specifically mentioned |
| ESMO–EURACAN–GENTURIS, 2022 [9] | Size > 20 mm | Resection. Surveillance is an alternative | <20 mm Active surveillance. short interval (e.g., 3 months) then increased interval. Resection as an alternative ≥ 20 mm Biopsy/excision |
| NCCN, 2022 [10] | When surgical resection or oncological treatment is required | Periodic endoscopic or radiographic surveillance. Risk and benefit should be discussed with the patient | Not specifically mentioned |
| ASGE, 2017 [5] | Lesions arising from submucosal or muscularis propria layer | Surveillance with EUS, 6–12 months interval | Removal as an alternative to tissue acquisition |
| Asian consensus guidelines for GIST, 2016 [11] | When surgical resection or oncological treatment is required | Resection. Surveillance is an alternative after informing the risk of malignancy | Not specifically mentioned |
| Japan GIST guideline subcommittee, 2008 [12] | Not specifically mentioned | Resection | <20 mm EGD at 6–12 months interval. When tumor growth or high-risk feature is noted, further examination is suggested, while resection is an alternative 20–50 mm Meticulous examinations with CT, EUS, and EUS-FNAB |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chien, M.-M.; Lin, Y.-H.; Chang, C.-C.; Chien, H.-Y. A Rare Gastric Subepithelial Lesion Removed through Submucosal Tunneling Endoscopic Resection: Case Report and Literature Review. Life 2023, 13, 179. https://doi.org/10.3390/life13010179
Chien M-M, Lin Y-H, Chang C-C, Chien H-Y. A Rare Gastric Subepithelial Lesion Removed through Submucosal Tunneling Endoscopic Resection: Case Report and Literature Review. Life. 2023; 13(1):179. https://doi.org/10.3390/life13010179
Chicago/Turabian StyleChien, Mu-Ming, Yun-Ho Lin, Chun-Chao Chang, and Hsi-Yuan Chien. 2023. "A Rare Gastric Subepithelial Lesion Removed through Submucosal Tunneling Endoscopic Resection: Case Report and Literature Review" Life 13, no. 1: 179. https://doi.org/10.3390/life13010179