
Mediterranean Diet, Ketogenic Diet or MIND Diet for Aging Populations with Cognitive Decline: A Systematic Review
 , , ,
, , ,  and
and
Abstract
:1. Introduction
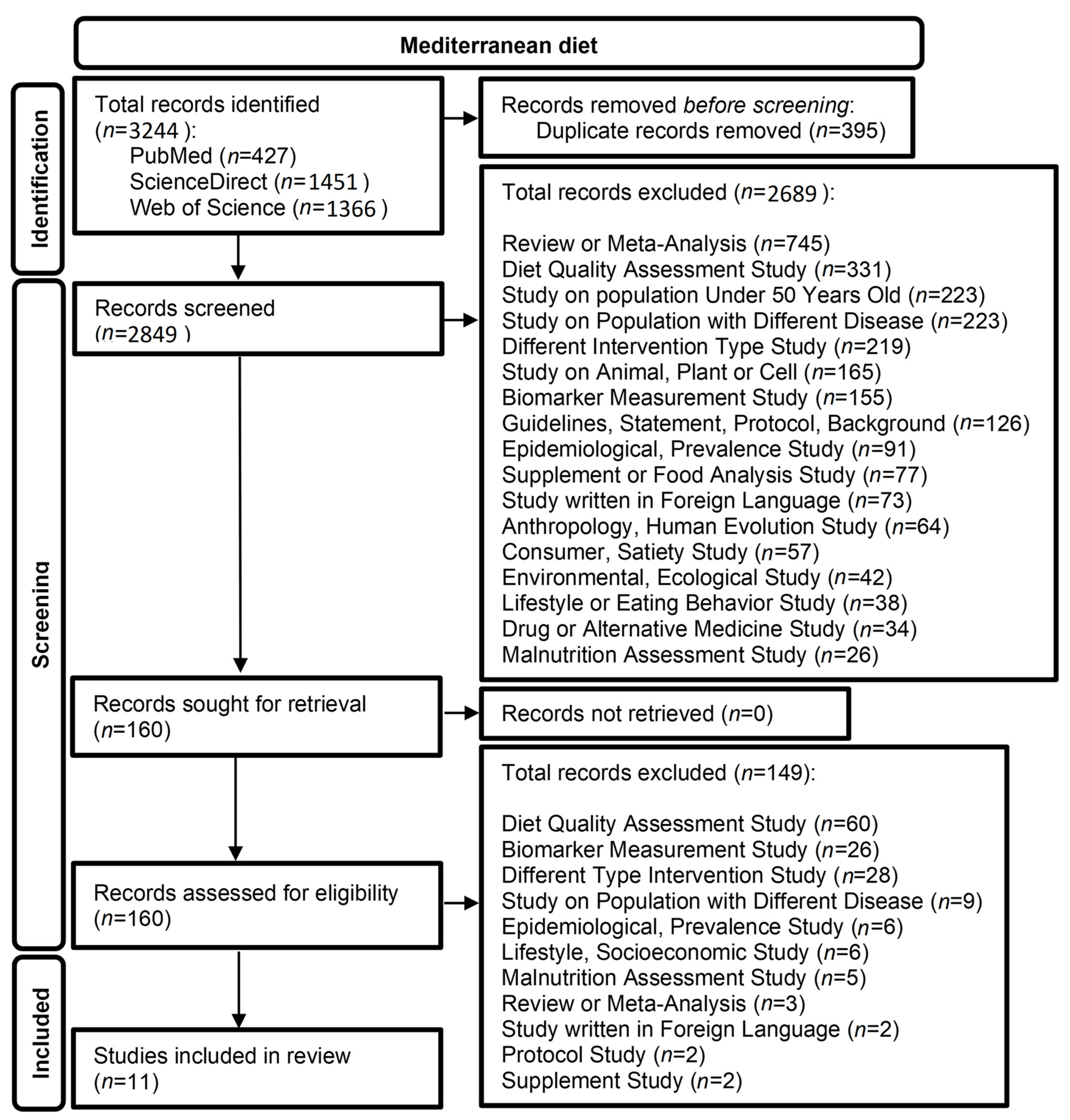
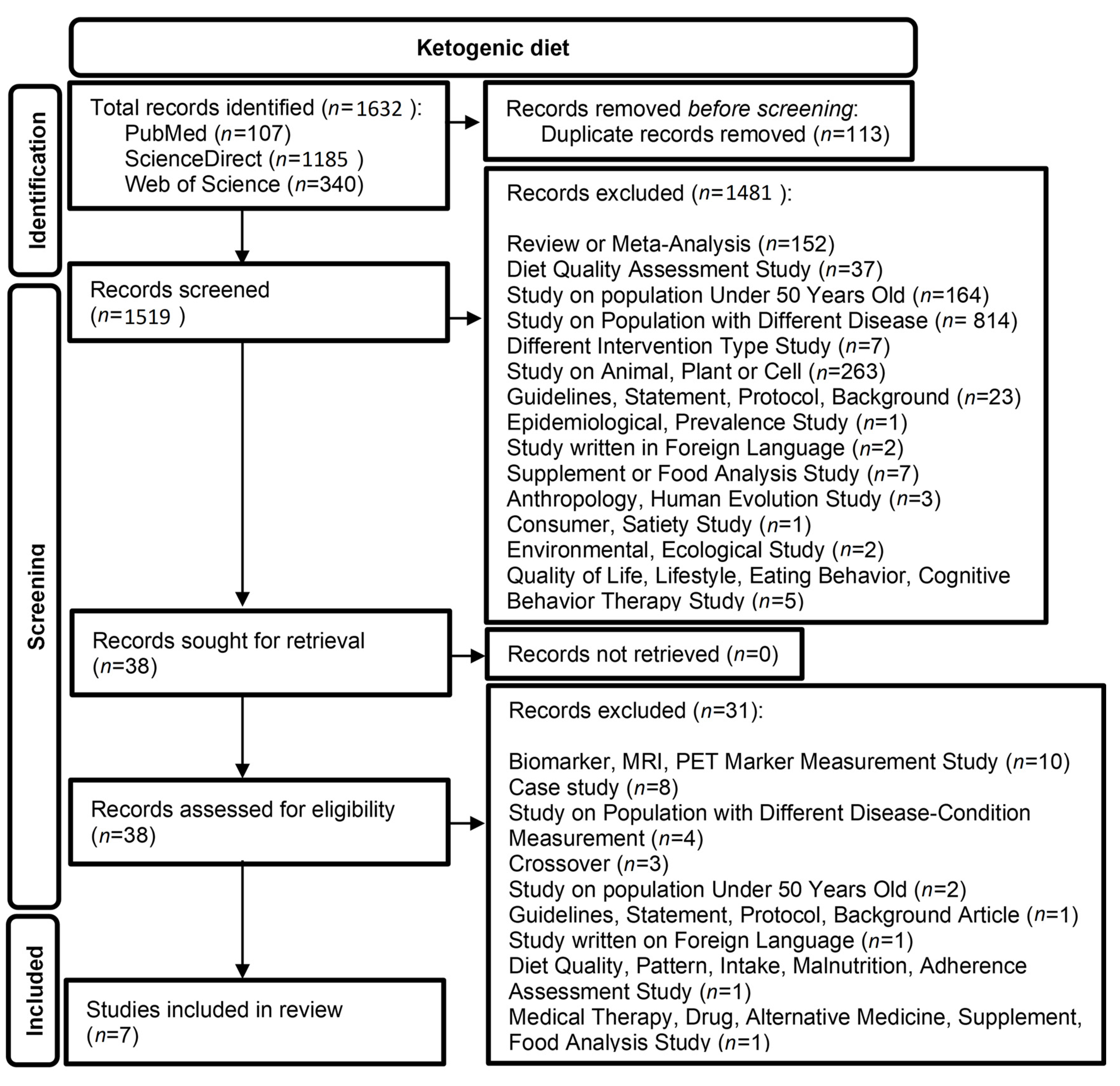
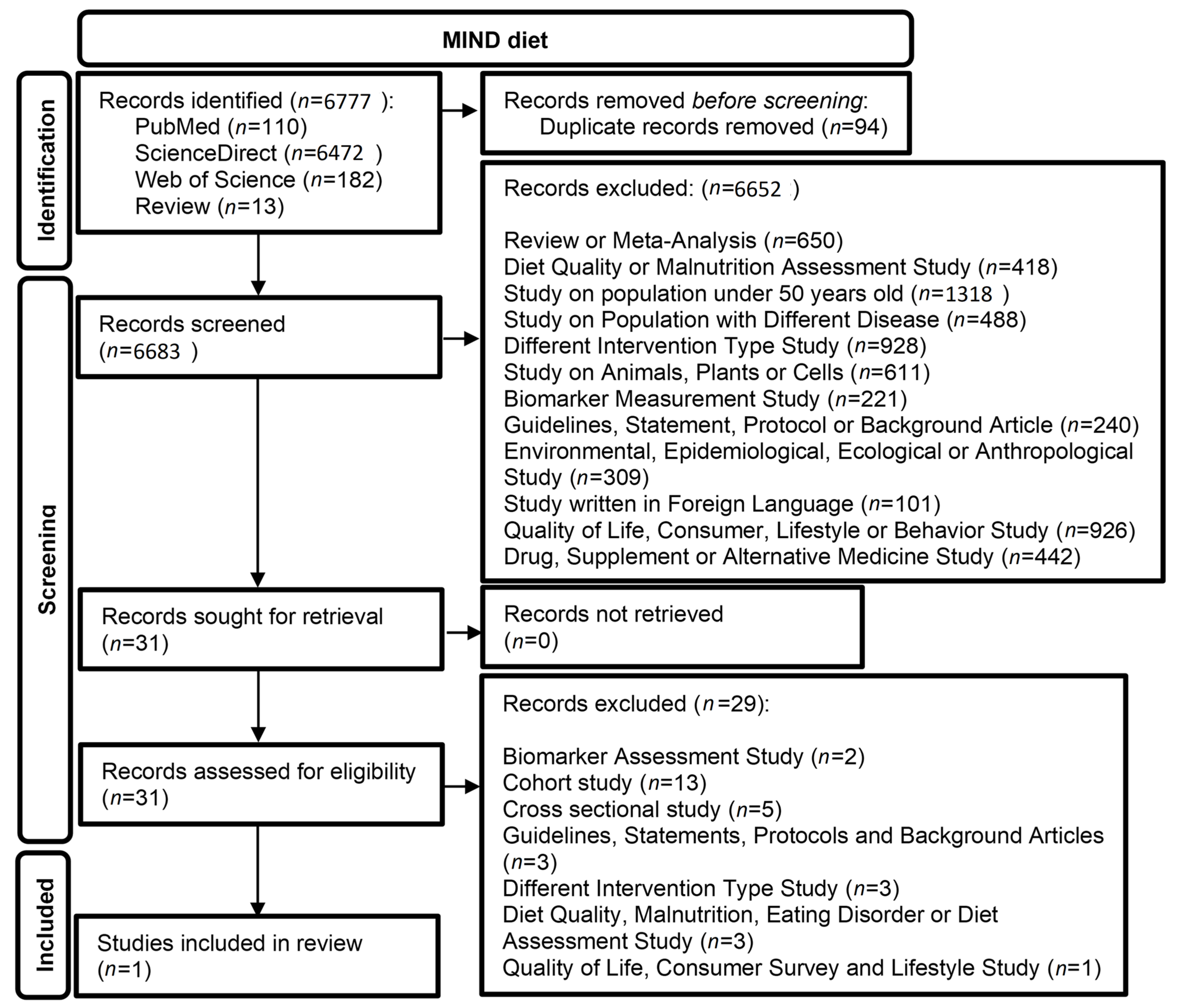
2. Materials and Methods
2.1. Literature Selection Criteria
2.2. Eligibility Criteria
2.3. Study Selection
2.3.1. Outcomes
2.3.2. Data Extraction
2.3.3. Quality Assessment
2.3.4. Data Synthesis
3. Results
3.1. Ketogenic Diet (KD)
3.2. MIND Diet
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Global Status Report on the Public Health Response to Dementia; World Health Organization: Geneva, Switzerland, 2021; ISBN 9789240033245. [Google Scholar]
- Gharbi-Meliani, A.; Dugravot, A.; Sabia, S.; Regy, M.; Fayosse, A.; Schnitzler, A.; Kivimäki, M.; Singh-Manoux, A.; Dumurgier, J. The Association of APOE Ε4 with Cognitive Function over the Adult Life Course and Incidence of Dementia: 20 Years Follow-up of the Whitehall II Study. Alzheimers. Res. Ther. 2021, 13, 5. [Google Scholar] [CrossRef]
- Sardone, R.; Battista, P.; Donghia, R.; Lozupone, M.; Tortelli, R.; Guerra, V.; Grasso, A.; Griseta, C.; Castellana, F.; Zupo, R.; et al. Age-Related Central Auditory Processing Disorder, MCI, and Dementia in an Older Population of Southern Italy. Otolaryngol. Neck Surg. 2020, 163, 348–355. [Google Scholar] [CrossRef] [PubMed]
- Tisher, A.; Salardini, A. A Comprehensive Update on Treatment of Dementia. Semin. Neurol. 2019, 39, 167–178. [Google Scholar] [CrossRef]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia Prevention, Intervention, and Care: 2020 Report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef] [PubMed]
- Gertz, H.-J.; Kurz, A. Diagnose Ohne Therapie. Nervenarzt 2011, 82, 1151–1159. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C. Mild Cognitive Impairment as a Diagnostic Entity. J. Intern. Med. 2004, 256, 183–194. [Google Scholar] [CrossRef]
- Wang, Y.; Jia, R.; Liang, J.; Li, J.; Qian, S.; Li, J.; Xu, Y. Effects of Non-pharmacological Therapies for People with Mild Cognitive Impairment. A Bayesian Network Meta-analysis. Int. J. Geriatr. Psychiatry 2020, 35, 591–600. [Google Scholar] [CrossRef]
- Yao, S.; Liu, Y.; Zheng, X.; Zhang, Y.; Cui, S.; Tang, C.; Lu, L.; Xu, N. Do Nonpharmacological Interventions Prevent Cognitive Decline? A Systematic Review and Meta-Analysis. Transl. Psychiatry 2020, 10, 19. [Google Scholar] [CrossRef] [Green Version]
- Lai, X.; Wen, H.; Li, Y.; Lu, L.; Tang, C. The Comparative Efficacy of Multiple Interventions for Mild Cognitive Impairment in Alzheimer’s Disease: A Bayesian Network Meta-Analysis. Front. Aging Neurosci. 2020, 12, 121. [Google Scholar] [CrossRef] [PubMed]
- Tsolaki, M.; Kounti, F.; Agogiatou, C.; Poptsi, E.; Bakoglidou, E.; Zafeiropoulou, M.; Soumbourou, A.; Nikolaidou, E.; Batsila, G.; Siambani, A.; et al. Effectiveness of Nonpharmacological Approaches in Patients with Mild Cognitive Impairment. Neurodegener. Dis. 2011, 8, 138–145. [Google Scholar] [CrossRef]
- Van Den Brink, A.C.; Brouwer-Brolsma, E.M.; Berendsen, A.A.M.; Van De Rest, O. The Mediterranean, Dietary Approaches to Stop Hypertension (DASH), and Mediterranean-DASH Intervention for Neurodegenerative Delay (MIND) Diets Are Associated with Less Cognitive Decline and a Lower Risk of Alzheimer’s Disease—A Review. Adv. Nutr. 2019, 10, 1040–1065. [Google Scholar] [CrossRef] [Green Version]
- Zupo, R.; Griseta, C.; Battista, P.; Donghia, R.; Guerra, V.; Castellana, F.; Lampignano, L.; Bortone, I.; Lozupone, M.; Giannelli, G.; et al. Role of Plant-Based Diet in Late-Life Cognitive Decline: Results from the Salus in Apulia Study. Nutr. Neurosci. 2022, 25, 1300–1309. [Google Scholar] [CrossRef] [PubMed]
- Skourlis, N.; Patsis, I.; Martimianaki, G.; Peppa, E.; Trichopoulou, A.; Katsouyanni, K. Changes in the Dietary Habits of the Greek EPIC Cohort Participants during a 14-Year Follow-Up Period (1997–2011). Nutrients 2020, 12, 2148. [Google Scholar] [CrossRef] [PubMed]
- Hardman, R.J.; Meyer, D.; Kennedy, G.; Macpherson, H.; Scholey, A.B.; Pipingas, A. Findings of A Pilot Study Investigating the Effects of Mediterranean Diet and Aerobic Exercise on Cognition in Cognitively Healthy Older People Living Independently within Aged Care Facilities: The Lifestyle Intervention in Independent Living Aged Care. Curr. Dev. Nutr. 2020, 4, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ince, N.; Gelener, P.; Besler, H.T. Does Mediterranean Diet Correlate with Cognitive Performance among Elderly? A Cross-Sectional Study from Cyprus. Prog. Nutr. 2020, 22, 75–83. [Google Scholar] [CrossRef]
- de Amicis, R.; Leone, A.; Foppiani, A.; Osio, D.; Lewandowski, L.; Giustizieri, V.; Cornelio, P.; Cornelio, F.; Fusari Imperatori, S.; Cappa, S.F.; et al. Mediterranean Diet and Cognitive Status in Free-Living Elderly: A Cross-Sectional Study in Northern Italy. J. Am. Coll. Nutr. 2018, 37, 494–500. [Google Scholar] [CrossRef]
- Martínez-Huélamo, M.; Rodríguez-Morató, J.; Boronat, A.; de la Torre, R. Modulation of Nrf2 by Olive Oil and Wine Polyphenols and Neuroprotection. Antioxidants 2017, 6, 73. [Google Scholar] [CrossRef] [Green Version]
- Lourida, I.; Soni, M.; Thompson-Coon, J.; Purandare, N.; Lang, I.A.; Ukoumunne, O.C.; Llewellyn, D.J. Mediterranean Diet, Cognitive Function, and Dementia. Epidemiology 2013, 24, 479–489. [Google Scholar] [CrossRef]
- Davis, C.; Bryan, J.; Hodgson, J.; Murphy, K. Definition of the Mediterranean Diet; A Literature Review. Nutrients 2015, 7, 9139–9153. [Google Scholar] [CrossRef] [Green Version]
- Trichopoulou, A.; Kouris-Blazos, A.; Wahlqvist, M.L.; Gnardellis, C.; Lagiou, P.; Polychronopoulos, E.; Vassilakou, T.; Lipworth, L.; Trichopoulos, D. Diet and Overall Survival in Elderly People. Br. Med. J. 1995, 311, 1457. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Costacou, T.; Bamia, C.; Trichopoulos, D. Adherence to a Mediterranean Diet and Survival in a Greek Population. N. Engl. J. Med. 2003, 348, 2599–2608. [Google Scholar] [CrossRef] [Green Version]
- Martínez-González, M.A.; Fernández-Jarne, E.; Serrano-Martínez, M.; Wright, M.; Gomez-Gracia, E. Development of a Short Dietary Intake Questionnaire for the Quantitative Estimation of Adherence to a Cardioprotective Mediterranean Diet. Eur. J. Clin. Nutr. 2004, 58, 1550–1552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Ruiz-Gutiérrez, V.; Covas, M.I.; Fiol, M.; Gómez-Gracia, E.; López-Sabater, M.C.; Vinyoles, E.; et al. Effects of a Mediterranean-Style Diet on Cardiovascular Risk Factors: A Randomized Trial. Ann. Intern. Med. 2006, 145, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Panagiotakos, D.B.; Pitsavos, C.; Stefanadis, C. Dietary Patterns: A Mediterranean Diet Score and Its Relation to Clinical and Biological Markers of Cardiovascular Disease Risk. Nutr. Metab. Cardiovasc. Dis. 2006, 16, 559–568. [Google Scholar] [CrossRef]
- Alberti-Fidanza, A.; Fidanza, F. Mediterranean Adequacy Index of Italian Diets. Public Health Nutr. 2004, 7, 937–941. [Google Scholar] [CrossRef] [PubMed]
- Gutierrez, L.; Folch, A.; Rojas, M.; Cantero, J.L.; Atienza, M.; Folch, J.; Camins, A.; Ruiz, A.; Papandreou, C.; Bulló, M. Effects of Nutrition on Cognitive Function in Adults with or without Cognitive Impairment: A Systematic Review of Randomized Controlled Clinical Trials. Nutrients 2021, 13, 3728. [Google Scholar] [CrossRef]
- Sofi, F.; Abbate, R.; Gensini, G.F.; Casini, A. Accruing Evidence on Benefits of Adherence to the Mediterranean Diet on Health: An Updated Systematic Review and Meta-Analysis. Am. J. Clin. Nutr. 2010, 92, 1189–1196. [Google Scholar] [CrossRef] [Green Version]
- Petersson, S.D.; Philippou, E. Mediterranean Diet, Cognitive Function, and Dementia: A Systematic Review of the Evidence. Adv. Nutr. 2016, 7, 889–904. [Google Scholar] [CrossRef] [Green Version]
- Buckinx, F.; Aubertin-Leheudre, M. Nutrition to Prevent or Treat Cognitive Impairment in Older Adults: A GRADE Recommendation. J. Prev. Alzheimer’s Dis. 2020, 8, 1–7. [Google Scholar] [CrossRef]
- Grammatikopoulou, M.G.; Goulis, D.G.; Gkiouras, K.; Theodoridis, X.; Gkouskou, K.K.; Evangeliou, A.; Dardiotis, E.; Bogdanos, D.P. To Keto or Not to Keto? A Systematic Review of Randomized Controlled Trials Assessing the Effects of Ketogenic Therapy on Alzheimer Disease. Adv. Nutr. 2020, 11, 1583–1602. [Google Scholar] [CrossRef]
- Pavón, S.; Lázaro, E.; Martínez, O.; Amayra, I.; López-Paz, J.F.; Caballero, P.; Al-Rashaida, M.; Luna, P.M.; García, M.; Pérez, M.; et al. Ketogenic Diet and Cognition in Neurological Diseases: A Systematic Review. Nutr. Rev. 2021, 79, 802–813. [Google Scholar] [CrossRef]
- Kullmann, S.; Heni, M.; Hallschmid, M.; Fritsche, A.; Preissl, H.; Häring, H.-U. Brain Insulin Resistance at the Crossroads of Metabolic and Cognitive Disorders in Humans. Physiol. Rev. 2016, 96, 1169–1209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Steen, E.; Terry, B.M.; Rivera, E.J.; Cannon, J.L.; Neely, T.R.; Tavares, R.; Xu, X.J.; Wands, J.R.; de la Monte, S.M. Impaired Insulin and Insulin-like Growth Factor Expression and Signaling Mechanisms in Alzheimer’s Disease—Is This Type 3 Diabetes? J. Alzheimer’s Dis. 2005, 7, 63–80. [Google Scholar] [CrossRef] [Green Version]
- Kossoff, E.H.; Rowley, H.; Sinha, S.R.; Vining, E.P.G. A Prospective Study of the Modified Atkins Diet for Intractable Epilepsy in Adults. Epilepsia 2008, 49, 316–319. [Google Scholar] [CrossRef] [PubMed]
- Caraballo, R.H.; Vining, E. Ketogenic Diet. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2012; Volume 108, pp. 783–793. [Google Scholar]
- Paoli, A.; Bianco, A.; Damiani, E.; Bosco, G. Ketogenic Diet in Neuromuscular and Neurodegenerative Diseases. Biomed Res. Int. 2014, 2014, 1–10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gershuni, V.M.; Yan, S.L.; Medici, V. Nutritional Ketosis for Weight Management and Reversal of Metabolic Syndrome. Curr. Nutr. Rep. 2018, 7, 97–106. [Google Scholar] [CrossRef]
- Biessels, G.J.; Staekenborg, S.; Brunner, E.; Brayne, C.; Scheltens, P. Risk of Dementia in Diabetes Mellitus: A Systematic Review. Lancet Neurol. 2006, 5, 64–74. [Google Scholar] [CrossRef] [PubMed]
- Goldenberg, J.Z.; Day, A.; Brinkworth, G.D.; Sato, J.; Yamada, S.; Jönsson, T.; Beardsley, J.; Johnson, J.A.; Thabane, L.; Johnston, B.C. Efficacy and Safety of Low and Very Low Carbohydrate Diets for Type 2 Diabetes Remission: Systematic Review and Meta-Analysis of Published and Unpublished Randomized Trial Data. Br. Med. J. 2021, 372, m4743. [Google Scholar] [CrossRef]
- Avgerinos, K.I.; Egan, J.M.; Mattson, M.P.; Kapogiannis, D. Medium Chain Triglycerides Induce Mild Ketosis and May Improve Cognition in Alzheimer’s Disease. A Systematic Review and Meta-Analysis of Human Studies. Ageing Res. Rev. 2020, 58, 101001. [Google Scholar] [CrossRef]
- Xu, Q.; Zhang, Y.; Zhang, X.; Liu, L.; Zhou, B.; Mo, R.; Li, Y.; Li, H.; Li, F.; Tao, Y.; et al. Medium-Chain Triglycerides Improved Cognition and Lipid Metabolomics in Mild to Moderate Alzheimer’s Disease Patients with APOE4−/−: A Double-Blind, Randomized, Placebo-Controlled Crossover Trial. Clin. Nutr. 2020, 39, 2092–2105. [Google Scholar] [CrossRef]
- Prins, P.J.; D’Agostino, D.P.; Rogers, C.Q.; Ault, D.L.; Welton, G.L.; Jones, D.W.; Henson, S.R.; Rothfuss, T.J.; Aiken, K.G.; Hose, J.L.; et al. Dose Response of a Novel Exogenous Ketone Supplement on Physiological, Perceptual and Performance Parameters. Nutr. Metab. 2020, 17, 81. [Google Scholar] [CrossRef]
- Sacks, F.M.; Katan, M. Randomized Clinical Trials on the Effects of Dietary Fat and Carbohydrate on Plasma Lipoproteins and Cardiovascular Disease. Am. J. Med. 2002, 113, 13–24. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.C.; Tangney, C.C.; Wang, Y.; Sacks, F.M.; Barnes, L.L.; Bennett, D.A.; Aggarwal, N.T. MIND Diet Slows Cognitive Decline with Aging. Alzheimer’s Dement. 2015, 11, 1015–1022. [Google Scholar] [CrossRef] [Green Version]
- Morris, M.C.; Tangney, C.C.; Wang, Y.; Sacks, F.M.; Bennett, D.A.; Aggarwal, N.T. MIND Diet Associated with Reduced Incidence of Alzheimer’s Disease. Alzheimer’s Dement. 2015, 11, 1007–1014. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karanja, N.M.; Obarzanek, E.; Lin, P.-H.; Mccullough, M.L.; Phillips, K.M.; Swain, J.F.; Champagne, C.M.; Hoben, K.P. Descriptive Characteristics of the Dietary Patterns Used in the Dietary Approaches to Stop Hypertension Trial. J. Am. Diet. Assoc. 1999, 99, S19–S27. [Google Scholar] [CrossRef] [PubMed]
- Kheirouri, S.; Alizadeh, M. MIND Diet and Cognitive Performance in Older Adults: A Systematic Review. Crit. Rev. Food Sci. Nutr. 2021, 62, 1–19. [Google Scholar] [CrossRef]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gotzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Healthcare Interventions: Explanation and Elaboration. Br. Med. J. 2009, 339, b2700. [Google Scholar] [CrossRef] [Green Version]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. ‘Mini-Mental State’. A Practical Method for Grading the Cognitive State of Patients for the Clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C. The Cochrane Collaboration’s Tool for Assessing Risk of Bias in Randomised Trials. Br. Med. J. 2011, 343, d5928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Risk of Bias 2 (RoB 2) Tool Cochrane Methods. Available online: https://methods.cochrane.org/risk-bias-2 (accessed on 18 January 2022).
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.M.; Gavaghan, D.J.; McQuay, H.J. Assessing the Quality of Reports of Randomized Clinical Trials: Is Blinding Necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Hoscheidt, S.; Sanderlin, A.H.; Baker, L.D.; Jung, Y.; Lockhart, S.; Kellar, D.; Whitlow, C.; Hanson, A.J.; Friedman, S.; Register, T.; et al. Mediterranean and Western Diet Effects on Alzheimer’s Disease Biomarkers, Cerebral Perfusion, and Cognition in Mid-life: A Randomized Trial. Alzheimer’s Dement. 2021, 18, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Knight, A.; Bryan, J.; Wilson, C.; Hodgson, J.; Davis, C.; Murphy, K. The Mediterranean Diet and Cognitive Function among Healthy Older Adults in a 6-Month Randomised Controlled Trial: The MedLey Study. Nutrients 2016, 8, 579. [Google Scholar] [CrossRef] [Green Version]
- Marseglia, A.; Xu, W.; Fratiglioni, L.; Fabbri, C.; Berendsen, A.A.M.; Bialecka-Debek, A.; Jennings, A.; Gillings, R.; Meunier, N.; Caumon, E.; et al. Effect of the NU-AGE Diet on Cognitive Functioning in Older Adults: A Randomized Controlled Trial. Front. Physiol. 2018, 9, 1–12. [Google Scholar] [CrossRef]
- Martínez-Lapiscina, E.H.; Clavero, P.; Toledo, E.; Estruch, R.; Salas-Salvadó, J.; San Julián, B.; Sanchez-Tainta, A.; Ros, E.; Valls-Pedret, C.; Martinez-Gonzalez, M.Á. Mediterranean Diet Improves Cognition: The PREDIMED-NAVARRA Randomised Trial. J. Neurol. Neurosurg. Psychiatry 2013, 84, 1318–1325. [Google Scholar] [CrossRef] [Green Version]
- Martínez-Lapiscina, E.H.; Galbete, C.; Corella, D.; Toledo, E.; Buil-Cosiales, P.; Salas-Salvado, J.; Ros, E.; Martinez-Gonzalez, M.Á. Genotype Patterns at CLU, CR1, PICALM and APOE, Cognition and Mediterranean Diet: The PREDIMED-NAVARRA Trial. Genes Nutr. 2014, 9, 393. [Google Scholar] [CrossRef] [Green Version]
- Martinez-Lapiscina, E.H.; Clavero, P.; Toledo, E.; San Julian, B.; Sanchez-Tainta, A.; Corella, D.; Lamuela-Raventos, R.M.; Martinez, J.A.; Martinez-Gonzalez, M.Á. Virgin Olive Oil Supplementation and Long-Term Cognition: The Predimed-Navarra Randomized, Trial. J. Nutr. Health Aging 2013, 17, 544–552. [Google Scholar] [CrossRef]
- Valls-Pedret, C.; Sala-Vila, A.; Serra-Mir, M.; Corella, D.; de la Torre, R.; Martínez-González, M.Á.; Martínez-Lapiscina, E.H.; Fitó, M.; Pérez-Heras, A.; Salas-Salvadó, J.; et al. Mediterranean Diet and Age-Related Cognitive Decline. J. Am. Med. Assoc. Intern. Med. 2015, 175, 1094. [Google Scholar] [CrossRef] [Green Version]
- Mazza, E.; Fava, A.; Ferro, Y.; Rotundo, S.; Romeo, S.; Bosco, D.; Pujia, A.; Montalcini, T. Effect of the Replacement of Dietary Vegetable Oils with a Low Dose of Extravirgin Olive Oil in the Mediterranean Diet on Cognitive Functions in the Elderly. J. Transl. Med. 2018, 16, 10. [Google Scholar] [CrossRef]
- Paknahad, Z.; Sheklabadi, E.; Derakhshan, Y.; Bagherniya, M.; Chitsaz, A. The Effect of the Mediterranean Diet on Cognitive Function in Patients with Parkinson’s Disease: A Randomized Clinical Controlled Trial. Complement. Ther. Med. 2020, 50, 102366. [Google Scholar] [CrossRef] [PubMed]
- Tsolaki, M.; Lazarou, E.; Kozori, M.; Petridou, N.; Tabakis, I.; Lazarou, I.; Karakota, M.; Saoulidis, I.; Melliou, E.; Magiatis, P. A Randomized Clinical Trial of Greek High Phenolic Early Harvest Extra Virgin Olive Oil in Mild Cognitive Impairment: The MICOIL Pilot Study. J. Alzheimer’s Dis. 2020, 78, 801–817. [Google Scholar] [CrossRef]
- Wardle, J.; Rogers, P.; Judd, P.; Taylor, M.A.; Rapoport, L.; Green, M.; Nicholson Perry, K. Randomized Trial of the Effects of Cholesterol-Lowering Dietary Treatment on Psychological Function. Am. J. Med. 2000, 108, 547–553. [Google Scholar] [CrossRef]
- Brandt, J.; Buchholz, A.; Henry-Barron, B.; Vizthum, D.; Avramopoulos, D.; Cervenka, M.C. Preliminary Report on the Feasibility and Efficacy of the Modified Atkins Diet for Treatment of Mild Cognitive Impairment and Early Alzheimer’s Disease. J. Alzheimer’s Dis. 2019, 68, 969–981. [Google Scholar] [CrossRef]
- Fortier, M.; Castellano, C.; Croteau, E.; Langlois, F.; Bocti, C.; St-Pierre, V.; Vandenberghe, C.; Bernier, M.; Roy, M.; Descoteaux, M.; et al. A Ketogenic Drink Improves Brain Energy and Some Measures of Cognition in Mild Cognitive Impairment. Alzheimer’s Dement. 2019, 15, 625–634. [Google Scholar] [CrossRef] [PubMed]
- Fortier, M.; Castellano, C.-A.; St-Pierre, V.; Myette-Côté, É.; Langlois, F.; Roy, M.; Morin, M.-C.; Bocti, C.; Fulop, T.; Godin, J.; et al. A Ketogenic Drink Improves Cognition in Mild Cognitive Impairment: Results of a 6-month RCT. Alzheimer’s Dement. 2021, 17, 543–552. [Google Scholar] [CrossRef] [PubMed]
- Henderson, S.T.; Vogel, J.L.; Barr, L.J.; Garvin, F.; Jones, J.J.; Costantini, L.C. Study of the Ketogenic Agent AC-1202 in Mild to Moderate Alzheimer’s Disease: A Randomized, Double-Blind, Placebo-Controlled, Multicenter Trial. Nutr. Metab. 2009, 6, 31. [Google Scholar] [CrossRef] [Green Version]
- Krikorian, R.; Shidler, M.D.; Dangelo, K.; Couch, S.C.; Benoit, S.C.; Clegg, D.J. Dietary Ketosis Enhances Memory in Mild Cognitive Impairment. Neurobiol. Aging 2012, 33, 425.e19–425.e27. [Google Scholar] [CrossRef] [Green Version]
- Krikorian, R.; Shidler, M.D.; Summer, S.S.; Sullivan, P.G.; Duker, A.P.; Isaacson, R.S.; Espay, A.J. Nutritional Ketosis for Mild Cognitive Impairment in Parkinson’s Disease: A Controlled Pilot Trial. Clin. Park. Relat. Disord. 2019, 1, 41–47. [Google Scholar] [CrossRef]
- De la Rubia Ortí, J.E.; García-Pardo, M.P.; Drehmer, E.; Sancho Cantus, D.; Julián Rochina, M.; Aguilar, M.A.; Hu Yang, I. Improvement of Main Cognitive Functions in Patients with Alzheimer’s Disease after Treatment with Coconut Oil Enriched Mediterranean Diet: A Pilot Study. J. Alzheimer’s Dis. 2018, 65, 577–587. [Google Scholar] [CrossRef]
- Arjmand, G.; Abbas-Zadeh, M.; Eftekhari, M.H. Effect of MIND Diet Intervention on Cognitive Performance and Brain Structure in Healthy Obese Women: A Randomized Controlled Trial. Sci. Rep. 2022, 12, 2871. [Google Scholar] [CrossRef] [PubMed]
- Foscolou, A.; D’Cunha, N.M.; Naumovski, N.; Tyrovolas, S.; Rallidis, L.; Matalas, A.-L.; Polychronopoulos, E.; Sidossis, L.S.; Panagiotakos, D. Midday Napping and Successful Aging in Older People Living in the Mediterranean Region: The Epidemiological Mediterranean Islands Study (MEDIS). Brain Sci. 2019, 10, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mamalaki, E.; Anastasiou, C.A.; Kosmidis, M.H.; Dardiotis, E.; Hadjigeorgiou, G.M.; Sakka, P.; Scarmeas, N.; Yannakoulia, M. Social Life Characteristics in Relation to Adherence to the Mediterranean Diet in Older Adults: Findings from the Hellenic Longitudinal Investigation of Aging and Diet (HELIAD) Study. Public Health Nutr. 2020, 23, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Cherian, L.; Wang, Y.; Holland, T.; Agarwal, P.; Aggarwal, N.; Morris, M.C. DASH and Mediterranean-Dash Intervention for Neurodegenerative Delay (MIND) Diets Are Associated with Fewer Depressive Symptoms Over Time. J. Gerontol. Ser. A 2021, 76, 151–156. [Google Scholar] [CrossRef]
- Vassilaki, M.; Aakre, J.A.; Syrjanen, J.A.; Mielke, M.M.; Geda, Y.E.; Kremers, W.K.; Machulda, M.M.; Alhurani, R.E.; Staubo, S.C.; Knopman, D.S.; et al. Mediterranean Diet, Its Components, and Amyloid Imaging Biomarkers. J. Alzheimer’s Dis. 2018, 64, 281–290. [Google Scholar] [CrossRef] [PubMed]
- Rainey-Smith, S.R.; Gu, Y.; Gardener, S.L.; Doecke, J.D.; Villemagne, V.L.; Brown, B.M.; Taddei, K.; Laws, S.M.; Sohrabi, H.R.; Weinborn, M.; et al. Mediterranean Diet Adherence and Rate of Cerebral Aβ-Amyloid Accumulation: Data from the Australian Imaging, Biomarkers and Lifestyle Study of Ageing. Transl. Psychiatry 2018, 8, 238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghosh, T.S.; Rampelli, S.; Jeffery, I.B.; Santoro, A.; Neto, M.; Capri, M.; Giampieri, E.; Jennings, A.; Candela, M.; Turroni, S.; et al. Mediterranean Diet Intervention Alters the Gut Microbiome in Older People Reducing Frailty and Improving Health Status: The NU-AGE 1-Year Dietary Intervention across Five European Countries. Gut 2020, 69, 1218–1228. [Google Scholar] [CrossRef] [Green Version]
- Mattei, J.; Bigornia, S.J.; Sotos-Prieto, M.; Scott, T.; Gao, X.; Tucker, K.L. The Mediterranean Diet and 2-Year Change in Cognitive Function by Status of Type 2 Diabetes and Glycemic Control. Diabetes Care 2019, 42, 1372–1379. [Google Scholar] [CrossRef] [Green Version]
- Matthews, D.C.; Davies, M.; Murray, J.; Williams, S.; Tsui, W.H.; Li, Y.; Andrews, R.D.; Lukic, A.; McHugh, P.; Vallabhajosula, S.; et al. Physical Activity, Mediterranean Diet and Biomarkers-Assessed Risk of Alzheimer’s: A Multi-Modality Brain Imaging Study. Adv. Mol. Imaging 2014, 4, 43–57. [Google Scholar] [CrossRef] [Green Version]
- Wade, A.T.; Elias, M.F.; Murphy, K.J. Adherence to a Mediterranean Diet Is Associated with Cognitive Function in an Older Non-Mediterranean Sample: Findings from the Maine-Syracuse Longitudinal Study. Nutr. Neurosci. 2021, 24, 542–553. [Google Scholar] [CrossRef]
- Mungas, D.; Cooper, J.K.; Weiler, P.G.; Gietzen, D.; Franzi, C.; Bernick, C. Dietary Preference for Sweet Foods in Patients with Dementia. J. Am. Geriatr. Soc. 1990, 38, 999–1007. [Google Scholar] [CrossRef] [PubMed]
- Neth, B.J.; Mintz, A.; Whitlow, C.; Jung, Y.; Solingapuram Sai, K.; Register, T.C.; Kellar, D.; Lockhart, S.N.; Hoscheidt, S.; Maldjian, J.; et al. Modified Ketogenic Diet Is Associated with Improved Cerebrospinal Fluid Biomarker Profile, Cerebral Perfusion, and Cerebral Ketone Body Uptake in Older Adults at Risk for Alzheimer’s Disease: A Pilot Study. Neurobiol. Aging 2020, 86, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Pérez-Guisado, J.; Muñoz-Serrano, A.; Alonso-Moraga, Á. Spanish Ketogenic Mediterranean Diet: A Healthy Cardiovascular Diet for Weight Loss. Nutr. J. 2008, 7, 30. [Google Scholar] [CrossRef] [Green Version]
- Filippini, T.; Adani, G.; Malavolti, M.; Garuti, C.; Cilloni, S.; Vinceti, G.; Zamboni, G.; Tondelli, M.; Galli, C.; Costa, M.; et al. Dietary Habits and Risk of Early-Onset Dementia in an Italian Case-Control Study. Nutrients 2020, 12, 3682. [Google Scholar] [CrossRef]
- Agarwal, P.; Wang, Y.; Buchman, A.S.; Bennett, D.A.; Morris, M.C. Dietary Patterns and Self-Reported Incident Disability in Older Adults. J. Gerontol. Ser. A 2019, 74, 1331–1337. [Google Scholar] [CrossRef] [PubMed]
- Dhana, K.; James, B.D.; Agarwal, P.; Aggarwal, N.T.; Cherian, L.J.; Leurgans, S.E.; Barnes, L.L.; Bennett, D.A.; Schneider, J.A. MIND Diet, Common Brain Pathologies, and Cognition in Community-Dwelling Older Adults. J. Alzheimer’s Dis. 2021, 83, 683–692. [Google Scholar] [CrossRef]
- Liu, X.; Dhana, K.; Furtado, J.D.; Agarwal, P.; Aggarwal, N.T.; Tangney, C.; Laranjo, N.; Carey, V.; Barnes, L.L.; Sacks, F.M. Higher Circulating α-Carotene Was Associated with Better Cognitive Function: An Evaluation among the MIND Trial Participants. J. Nutr. Sci. 2021, 10, e64. [Google Scholar] [CrossRef]
- Nishi, S.K.; Babio, N.; Gómez-Martínez, C.; Martínez-González, M.Á.; Ros, E.; Corella, D.; Castañer, O.; Martínez, J.A.; Alonso-Gómez, Á.M.; Wärnberg, J.; et al. Mediterranean, DASH, and MIND Dietary Patterns and Cognitive Function: The 2-Year Longitudinal Changes in an Older Spanish Cohort. Front. Aging Neurosci. 2021, 13, 782067. [Google Scholar] [CrossRef]
- Ferreira, N.V.; Lotufo, P.A.; Marchioni, D.M.L.; Barreto, S.M.; Viana, M.C.; Caramelli, P.; Bensenor, I.J.M.; Suemoto, C.K. Association Between Adherence to the MIND Diet and Cognitive Performance Is Affected by Income. Alzheimer Dis. Assoc. Disord. 2022, 32, 1–7. [Google Scholar] [CrossRef]
- Männikkö, R.; Komulainen, P.; Schwab, U.; Heikkilä, H.M.; Savonen, K.; Hassinen, M.; Hänninen, T.; Kivipelto, M.; Rauramaa, R. The Nordic Diet and Cognition—The DR’s EXTRA Study. Br. J. Nutr. 2015, 114, 231–239. [Google Scholar] [CrossRef]
- Willcox, D.C.; Scapagnini, G.; Willcox, B.J. Healthy Aging Diets Other than the Mediterranean: A Focus on the Okinawan Diet. Mech. Ageing Dev. 2014, 136–137, 148–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ayati, Z.; Yang, G.; Ayati, M.H.; Emami, S.A.; Chang, D. Saffron for Mild Cognitive Impairment and Dementia: A Systematic Review and Meta-Analysis of Randomised Clinical Trials. BMC Complement. Med. Ther. 2020, 20, 333. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.-N.; Mei, X.; Zhang, Z.-G.; Xie, Y.; Lang, F. Curcumin Intervention for Cognitive Function in Different Types of People: A Systematic Review and Meta-Analysis. Phyther. Res. 2019, 33, 524–533. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bredesen, D.; Perlmutter, D. The End of Alzheimer’s Program: The First Protocol to Enhance Cognition and Reverse Decline at Any Age; Penguin Publishing Group: London, UK, 2020; ISBN 9780525538509. [Google Scholar]
- Rosenberg, A.; Mangialasche, F.; Ngandu, T.; Solomon, A.; Kivipelto, M. Multidomain Interventions to Prevent Cognitive Impairment, Alzheimer’s Disease, and Dementia: From FINGER to World-Wide FINGERS. J. Prev. Alzheimer’s Dis. 2020, 7, 29–36. [Google Scholar] [CrossRef]
- Park, H.K.; Jeong, J.H.; Moon, S.Y.; Park, Y.K.; Hong, C.H.; Na, H.R.; Song, H.-S.; Lee, S.M.; Choi, M.; Park, K.W.; et al. South Korean Study to Prevent Cognitive Impairment and Protect Brain Health Through Lifestyle Intervention in At-Risk Elderly People: Protocol of a Multicenter, Randomized Controlled Feasibility Trial. J. Clin. Neurol. 2020, 16, 292. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, Y.K.; Song, J.E.; Hong, C.H.; Moon, S.Y.; Jeong, J.H.; Park, H.K.; Na, H.R.; Choi, S.H. South Korean Study to Prevent Cognitive Impairment and Protect BRAIN (SUPERBRAIN) Showed Improvement in Cognitive Function Mostly in Individuals with Nutritional Improvement: Sub-analysis of SUPERBRAIN Results. Alzheimer’s Dement. 2021, 17, e054727. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 10, 89. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Bias Arising from the Randomization Process | Bias Due to Deviations from Intended Intervention | Bias Due to Missing Outcome Data | Bias in Measurement of the Outcome | Bias in Selection of the Reported Results | Overall | |
|---|---|---|---|---|---|---|
| Hoscheidt, 2021 [56] |  | | | |  | |
| Knight, 2016 [57] | | | | | | |
| Marseglia, 2018 [58] | | | | | | |
| Martinez-Lapiscina, 2013a [59] | | | | | | |
| Martínez-Lapiscina, 2014 [60] | | | | | | |
| Martinez-Lapiscina, 2013b [61] | | | | | | |
| Valls-Pedret, 2015 [62] | | | |  | | |
| Mazza, 2018 [63] | | | | | | |
| Paknahad, 2020 [64] | | | | | | |
| Tsolaki, 2020 [65] | | | | | | |
| Wardle, 2000 [66] | | | | | | |
low bias; some concerns; high bias.| If Randomization Is Mentioned | If Randomization Method Is Appropriate | If Blinding Is Mentioned | If Blinding Method Is Appropriate | If (n Account) the Fate of All Patients Is Known | Overall Score | Overall Score Evaluation | |
|---|---|---|---|---|---|---|---|
| Hoscheidt, 2021 [56] | 1 | 0 | 1 | 1 | 0 | 3 | |
| Knight, 2016 [57] | 1 | 1 | 1 | 1 | 0 | 4 | |
| Marseglia, 2018 [58] | 1 | 1 | 1 | 1 | 0 | 4 | |
| Martinez-Lapiscina, 2013a [59] | 1 | 1 | 1 | 1 | 0 | 4 | |
| Martínez-Lapiscina, 2014 [60] | 1 | 1 | 1 | 1 | 0 | 4 | |
| Martinez-Lapiscina, 2013b [61] | 1 | 1 | 1 | 1 | 0 | 4 | |
| Valls-Pedret, 2015 [62] | 1 | 1 | 0 | 0 | 0 | 2 | |
| Mazza, 2018 [63] | 1 | 0 | 1 | 1 | 0 | 3 | |
| Paknahad, 2020 [64] | 1 | 1 | 1 | 1 | 0 | 4 | |
| Tsolaki, 2020 [65] | 1 | 1 | 1 | 1 | 0 | 4 | |
| Wardle, 2000 [66] | 1 | 0 | 1 | 1 | 0 | 3 | |
high quality; low quality.| Study (REF) Year, Country | Type of Study | Intervention Group 1 Included | Intervention Group 2 Included | Control Group Included | Cognitive Status at Baseline | Overall Health Status | Intervention | Duration of Intervention | Measures of Cognitive Outcomes | Outcomes—Significant Benefit of Intervention |
|---|---|---|---|---|---|---|---|---|---|---|
| Hoscheidt [56] 2021 USA | RCT | n= 44 Age 55.7 ± 5.5 y | N/A | n = 43 Age 56.9 ± 4.7 y | NC 3MS 97 ± 2 & MCI 3MS 95 ± 4 | Healthy | IG1: MeDi (<7% SF, GI < 55, Na+ 1.3 g/day) CG: Western diet (25% SF, GI > 70, Na+ 3.2 g/day) | 4 weeks | 3MS, SRT, BSRT, DCT | p > 0.1 |
| Knight [57] 2016 Australia | RCT | n = 70 Age 72.1 ± 4.9 y | N/A | n = 67 Age 72 ± 5 y | NC | Healthy | IG1: MeDi CG: no guidance | 6 months | Stroop, LFT, TOL, RAVLT, F&B-DS, LNS, SS&C, BVRT | BVRT (p = 0.01) RAVLT (p = 0.03) RAVLT/F&B-DS/LNS (p = 0.05) |
| Marseglia [58] 2018 France, Italy, Netherlands, Poland, and UK | RCT | n = 573 Age 70.7 ± 0.2 y | N/A | n = 571 Age 71.1 ± 0.2 | NC MMSE 28 ± 2 | Healthy | IG1: NU-AGE diet CG: national guidelines | 12 months | CERAD-NB, MMSE, CFT, BSR, PCT, DCT, TMT-A&B, BNT, WLM, CPT | MMSE/CERAD-NB (p = 0.05) WLM/BSRT (p = 0.03) |
| Martinez-Lapiscina [59] 2013a Spain | RCT | n = 224 Age 67.4 ± 5.7 y | n = 166 Age 67.3 ± 5.8 y | n = 132 Age 67.6 ± 5.5 y | NC | High Risk of CVD | IG1: MeDi-EVOO (1 L/week) IG2: MeDi-MN (30 g/day) CG: LF | 6.5 years | MMSE, CDT | MMSE (p = 0.015) CDT (p = 0.048) |
| Martínez-Lapiscina [60] 2014 Spain | RCT | n = 381 Age 67 ± 6 y | N/A | n = 129 Age 67 ± 6 y | NC | High Risk of CVD | IG: MeDi CG: LF | 6.5 years | MMSE, CDT | CLU MMSE (p = 0.04) CLU CDT (p = 0.001) CR1 MMSE (p = 0.001) CR1 CDT (p = 0.006) PICALM MMSE (p = 0.02) PICALM CDT (p = 0.005) APOE MMSE (p < 0.001) APOE CDT (p = 0.007) |
| Martinez-Lapiscina [61] 2013b Spain | RCT | n = 91 Age 67.2 ± 5.6 y | n = 88 Age 67.3 ± 6 y | n = 89 Age 67.5 ± 5.7 y | NC | High Risk of CVD | IG1: MeDi-EVOO (1 L/week) IG2: MeDi-MN (30 g/day) CG: LF | 6.5 years | MMSE, CDT, VPA, RAVLT, ROCFT, BNT, AFT, FAST, F&B-DS, TMT-A&B, CDR | MMSE, ROCF, FAST, F-DS (p < 0.05) |
| Valls-Pedret [62] 2015 Spain | RCT | n = 127 Age 67.9 ± 5.4 y | n = 112 Age 66.7 ± 5.3 y | n = 95 Age 65.5 ± 5.8 y | NC MMSE 28 ± 1 | High Risk of CVD | IG1: MeDi-EVOO (1 L/week) IG2: MeDi-MN (30 g/day) CG: LF | 4.1 years | MMSE, RAVLT, VPAT, AFT, F&B-DS, CTT-1&2 | RAVLT/VPAT (p = 0.04) DS/CTT (p = 0.004) all tests composite (p = 0.01) |
| Mazza [63] 2018 Italy | RCT | n = 55 Age 70 ± 4 y | N/A | N = 55 Age 70 ± 4y | MCI MMSE 25 ± 1 | 52% HL 52% HT 48% DM | IG: MeDi-EVOO (20–30 g/day) CG: MeDi | 12 months | MMSE, ADAS-Cog, VF | MMSE (p < 0.001) ADAS-Cog (p < 0.001) |
| Paknahad [64] 2020 Iran | RCT | n = 35 Age 59.3 ± 8.3 y | N/A | n = 35 Age 58.6 ± 9.3 y | PD-MCI MoCA 19 ± 6 | PD | IG: MeDi CG: healthy recommendations | 10 weeks | MoCA | total score (p = 0.001) executive function (p = 0.001) language (p = 0.02) attention, concentration, working memory (p = 0.04) |
| Tsolaki [65] 2020 Greece | RCT | n = 18 Age 68.5 ± 6.8 y | n = 16 Age 70.8 ± 8.1 y | n = 16 Age 70.1 ± 6 y | MCI MMSE 28 ± 2 | Healthy | IG1: MeDi-HP-EVOO (50 mL/day) IG2: MeDi-MP-EVOO (50 mL/day) CG: MeDi | 12 months | MMSE, SRT, ROCF, TMT-A&B, ADAS-Cog, F&B-DS, LFT, CFT, CDT | ADAS-Cog (p = 0.001) MMSE (p = 0.03) F-DS (p = 0.006) LFT (p = 0.003) |
| Wardle [66] 2000 United Kingdom | RCT | n = 52 Age 52 ± 11 y | n = 53 Age 54 ± 11 y | n = 50 Age 53 ± 8 y | NC | HL | IG1: LF IG2: MeDi CG: no guidance | 12 weeks | VIFR, TFT, CRT, SAT | SAT (p < 0.001) |
| Bias Arising from the Randomization Process | Bias Due to Deviations from Intended Intervention | Bias Due to Missing Outcome Data | Bias in Measurement of the Outcome | Bias in Selection of the Reported Results | Overall | |
|---|---|---|---|---|---|---|
| Brandt, 2019 [67] | | | | | | |
| Fortier, 2019 [68] | | | | | | |
| Fortier, 2021 [69] | | | | | | |
| Henderson, 2009 [70] | | | | | | |
| Krikorian, 2012 [71] | | | | | | |
| Krikorian, 2019 [72] | | | | | | |
| de la Rubia Ortí, 2018 [73] | | | | | | |
low bias; some concerns; high bias.| If Randomization Is Mentioned | If Randomization Method Is Appropriate | If Blinding Is Mentioned | If Blinding Method Is Appropriate | If (n Account) the Fate of All Patients Is Known | Overall Score | Overall Score Evaluation | |
|---|---|---|---|---|---|---|---|
| Brandt, 2019 [67] | 1 | 1 | 1 | 1 | 0 | 4 | |
| Fortier, 2019 [68] | 1 | 1 | 1 | 1 | 0 | 4 | |
| Fortier, 2021 [69] | 1 | 1 | 1 | 1 | 0 | 4 | |
| Henderson, 2009 [70] | 1 | 1 | 1 | 1 | 0 | 4 | |
| Krikorian, 2012 [71] | 0 | 0 | 0 | 0 | 1 | 1 | |
| Krikorian, 2019 [72] | 1 | 1 | 0 | 0 | 0 | 2 | |
| de la Rubia Ortí, 2018 [73] | 1 | 1 | 1 | 1 | 0 | 4 | |
high quality; low quality.| Study (REF) Year Country | Type of Study | Intervention Group Included | Control Group Included | Cognitive Status at Baseline | Overall Health Status | Intervention (Details of Diet) | Duration of Intervention | Measures of Cognitive Outcomes | Outcomes—Significant Benefit of Intervention |
|---|---|---|---|---|---|---|---|---|---|
| Brandt [67] 2019 USA | RCT | n = 9 Age 73.5 ± 6.4 y | n = 5 Age 69.1 ± 5 y | MCI or early AD MoCA 20.4 ± 3.8 | NR | IG: MAD CG: NIA diet | 12 weeks | CDR, MoCA, MMSE-2:EV, HVLT-R, BVMT-R | p > 0.05 |
| Fortier [68] 2019 Canada | RCT | n = 19 Age 73.8 ± 6.3 y | n = 20 Age 75.4 ± 6.6 y | MCI MoCA 22.9 ± 3 MMSE 27.4 ± 2.2 | NR | IG: 15 g MCT drink (60% caprylic acid, 40% capric acid) twice daily CG: Placebo sunflower oil drink | 6 months | MMSE, MoCA, F&C-WL&RT, BVMT-R, TMT, Stroop, VF, DSST, BNT | BNT p = 0.003 F&C-WL&RT p = 0.013 BVMT-R p = 0.027 Stroop p = 0.046 TMT p = 0.043 |
| Fortier [69] 2021 Canada | RCT | n = 39 Age 71.4 ± 7.2 y | n = 44 Age 72.9 ± 6.9 y | MCI MoCA 24 ± 2.5 MMSE 27.5 ± 2.2 | NR | IG: 15 g MCT drink (60% caprylic acid, 40% capric acid) twice daily CG: Placebo sunflower oil drink | 6 months | MMSE, MoCA, F&C-WL&RT, BVMT-R, TMT, Stroop, VF, DSST, BNT | F&C-WL&RT p = 0.047 VF p = 0.024 TMT p = 0.017 Stroop p = 0.042 BNT p = 0.033 |
| Henderson [70] 2009 USA | RCT | n = 46 Age 76.9 ± 8.9 y | n = 50 Age 76.8 ± 7.4 y | Mild-moderate AD MMSE 19.6 ± 4.4 | NR | IG: 20 g MCT drink (glycerin, caprylic acid) daily CG: Placebo safflower oil drink | 90 days | ADAS-Cog, ADCS-CGIC, MMSE | ADAS-Cog p = 0.02 |
| Krikorian [71] 2012 USA | RCT | n = 12 Age 68 ± 3 y | n = 11 Age 71 ± 8 y | MCI CDR 0.7 ± 0.4 | NR | IG: ≤20 g carbohydrates per day CG: 50% of daily calories from carbohydrates | 6 weeks | CDR, TMT-B, VPAL | VPAL p = 0.01 |
| Krikorian [72] 2019 USA | RCT | n = 7 Age 66 ± 5.5 y | n = 7 Age 65.4 ± 6.5 y | PD-MCI MoCA 24.8 ± 2 | NR | IG: ≤20 g carbohydrates per day CG: 50% of daily calories from carbohydrates | 8 weeks | MoCA, COWA, CVLT, VPAL | COWA p = 0.02 VPAL p < 0.04 CVLT p = 0.06 |
| de la Rubia Ortí [73] 2018 Spain | RCT | n = 22 Age 65-85 y | n = 22 Age 65-85 y | AD (institutionalized) | NR | IG: MeDi + 20 mL coconut oil twice daily CG: MeDi | 21 days | MMSE, BTOT, CDT, VF, F&C-SRT | BTOT p < 0.05 VF p < 0.05 F&C-SRT p < 0.05 |
| Bias Arising from the Randomization Process | Bias Due to Deviations from Intended Intervention | Bias Due to Missing Outcome Data | Bias in Measurement of the Outcome | Bias in Selection of the Reported Results | Overall | |
|---|---|---|---|---|---|---|
| Arjmand, 2020 [74] | | | | | | |
low bias; some concerns.| If Randomization Is Mentioned | If Randomization Method Is Appropriate | If Blinding Is Mentioned | If Blinding Method Is Appropriate | If (n Account) the Fate of All Patients Is Known | Overall Score | Overall Score Evaluation | |
|---|---|---|---|---|---|---|---|
| Arjmand, 2020 [74] | 1 | 1 | 1 | 1 | 0 | 4 | |
high quality.| Study (REF) Year, Country | Type of Study | Intervention Group Included | Control Group Included | Cognitive Status at Baseline | Overall Health Status | Intervention | Duration of Intervention | Measures of Cognitive Outcomes | Outcomes—Significant Benefit of Intervention |
|---|---|---|---|---|---|---|---|---|---|
| Arjmand [74] 2020 Iran | RCT | n = 22 Age 49 ± 1.1 y | n = 15 Age 48.9 ± 1.6 y | CN MMSE 26.4 ± 0.5 | Obesity BMI 32 ± 1 | IG: calorie-restricted MIND diet CG: calorie-restricted diet | 3 months | MMSE, F&BDST, LNST, SDMT, RAVLT, TMT-A&B, Stroop | LNST p ≤ 0.001 RAVLT p ≤ 0.001 F&BDST p ≤ 0.05 SDMT p ≤ 0.001 TMT-A p = 0.002 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Devranis, P.; Vassilopoulou, Ε.; Tsironis, V.; Sotiriadis, P.M.; Chourdakis, M.; Aivaliotis, M.; Tsolaki, M. Mediterranean Diet, Ketogenic Diet or MIND Diet for Aging Populations with Cognitive Decline: A Systematic Review. Life 2023, 13, 173. https://doi.org/10.3390/life13010173
Devranis P, Vassilopoulou Ε, Tsironis V, Sotiriadis PM, Chourdakis M, Aivaliotis M, Tsolaki M. Mediterranean Diet, Ketogenic Diet or MIND Diet for Aging Populations with Cognitive Decline: A Systematic Review. Life. 2023; 13(1):173. https://doi.org/10.3390/life13010173
Chicago/Turabian StyleDevranis, Paschalis, Εmilia Vassilopoulou, Vasileios Tsironis, Panagiotis Marios Sotiriadis, Michail Chourdakis, Michalis Aivaliotis, and Magdalini Tsolaki. 2023. "Mediterranean Diet, Ketogenic Diet or MIND Diet for Aging Populations with Cognitive Decline: A Systematic Review" Life 13, no. 1: 173. https://doi.org/10.3390/life13010173