
New Insights into Non-Alcoholic Fatty Liver Disease and Coronary Artery Disease: The Liver-Heart Axis

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Epidemiology of the Relationship between NAFLD and CAD
3. Screening and Diagnosis
3.1. CAD in Patients Assessed for NAFLD
3.2. NAFLD in Patients Assessed for CAD
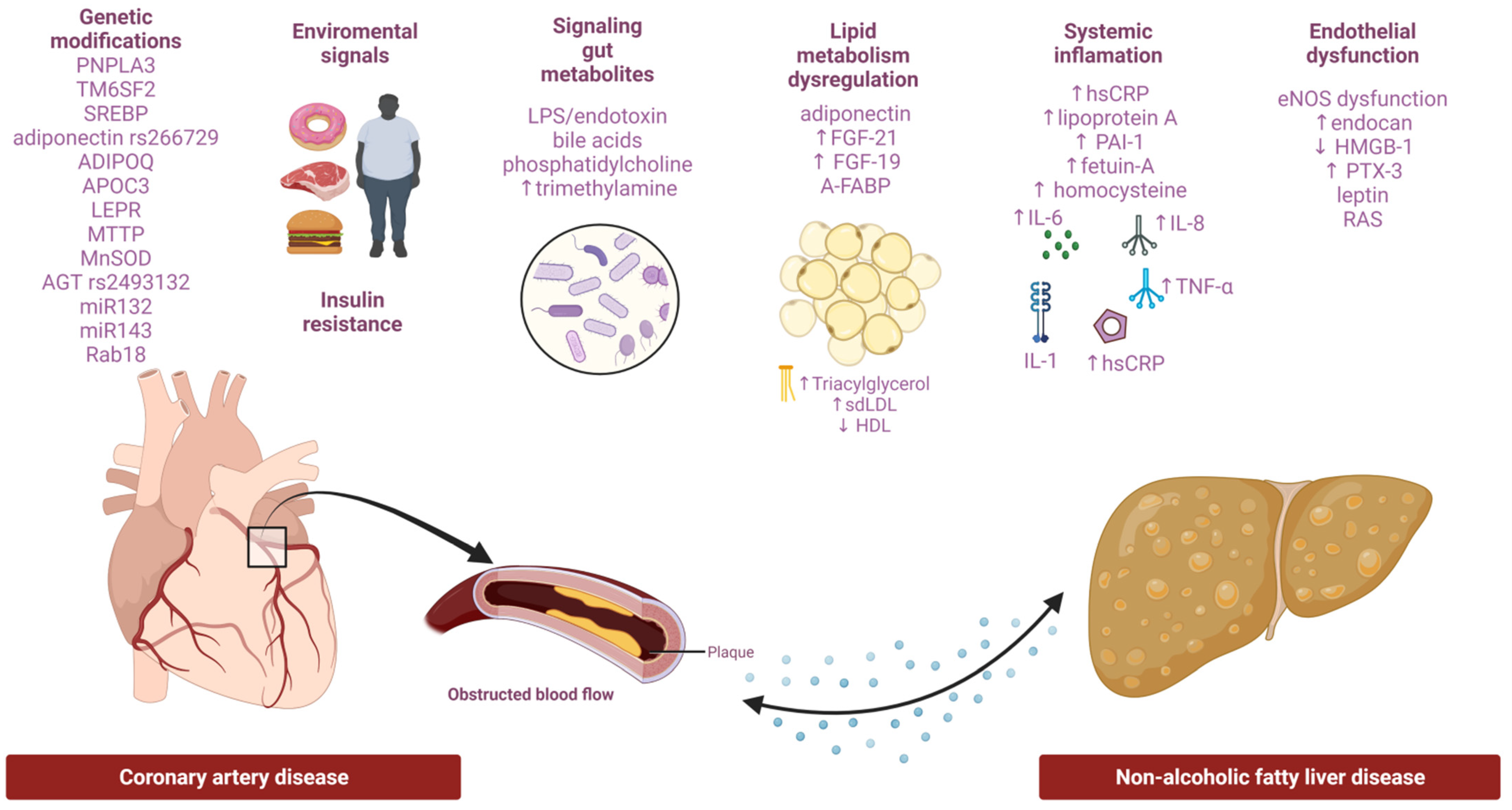
4. Potential Pathogenic Links between NAFLD and CAD
4.1. Common Risk Factors
4.2. Genetics, Epigenetics Modifications
4.3. Lipid and Cholesterol Metabolism
4.4. Systemic Inflammation and Cytokines
4.5. Endothelial Dysfunction and Oxidative Stress
4.6. Gut Microbiota
5. The Challenge of Lean NAFLD and Cardiovascular Risk
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Younossi, Z.; Anstee, Q.M.; Marietti, M.; Hardy, T.; Henry, L.; Eslam, M.; George, J.; Bugianesi, E. Global burden of NAFLD and NASH: Trends, predictions, risk factors and prevention. Nat. Rev. Gastroenterol. Hepatol. 2017, 15, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Koenig, A.B.; Abdelatif, D.; Fazel, Y.; Henry, L.; Wymer, M. Global Epidemiology of Nonalcoholic Fatty Liver Disease—Meta-analytic Assessment of Prevalence, Incidence, and Outcomes. Hepatology 2016, 64, 73–84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Younossi, Z.M.; Henry, L. Epidemiology of non-alcoholic fatty liver disease and hepatocellular carcinoma. JHEP Rep. 2021, 3, 100305. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Golabi, P.; de Avila, L.; Paik, J.M.; Srishord, M.; Fukui, N.; Qiu, Y.; Burns, L.; Afendy, A.; Nader, F. The global epidemiology of NAFLD and NASH in patients with type 2 diabetes: A systematic review and meta-analysis. J. Hepatol. 2019, 71, 793–801. [Google Scholar] [CrossRef]
- European Association for the Study of the Liver (EASL); European Association for the Study of Diabetes (EASD); European Association for the Study of Obesity (EASO). EASL-EASD-EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [Google Scholar] [CrossRef]
- Chalasani, N.; Younossi, Z.; LaVine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef]
- Eslam, M.; Newsome, P.N.; Sarin, S.K.; Anstee, Q.M.; Targher, G.; Romero-Gomez, M.; Zelber-Sagi, S.; Wong, V.W.-S.; Dufour, J.-F.; Schattenberg, J.M.; et al. A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J. Hepatol. 2020, 73, 202–209. [Google Scholar] [CrossRef]
- Kotronen, A.; Yki-Järvinen, H. Fatty Liver. Arter. Thromb. Vasc. Biol. 2008, 28, 27–38. [Google Scholar] [CrossRef]
- Targher, G.; Tilg, H.; Byrne, C.D. Non-alcoholic fatty liver disease: A multisystem disease requiring a multidisciplinary and holistic approach. Lancet Gastroenterol. Hepatol. 2021, 6, 578–588. [Google Scholar] [CrossRef]
- Wijarnpreecha, K.; Aby, E.S.; Ahmed, A.; Kim, D. Evaluation and management of extrahepatic manifestations of nonalcoholic fatty liver disease. Clin. Mol. Hepatol. 2021, 27, 221–235. [Google Scholar] [CrossRef] [PubMed]
- Duell, P.B.; Welty, F.K.; Miller, M.; Chait, A.; Hammond, G.; Ahmad, Z.; Cohen, D.E.; Horton, J.D.; Pressman, G.S.; Toth, P.P. Nonalcoholic Fatty Liver Disease and Cardiovascular Risk: A Scientific Statement from the American Heart Association. Arter. Thromb. Vasc. Biol. 2022, 42. [Google Scholar] [CrossRef]
- Luo, J.; Xu, L.; Li, J.; Zhao, S. Nonalcoholic fatty liver disease as a potential risk factor of cardiovascular disease. Eur. J. Gastroenterol. Hepatol. 2015, 27, 193–199. [Google Scholar] [CrossRef]
- Alexander, M.; Loomis, A.K.; Van Der Lei, J.; Duarte-Salles, T.; Prieto-Alhambra, D.; Ansell, D.; Pasqua, A.; Lapi, F.; Rijnbeek, P.; Mosseveld, M.; et al. Non-alcoholic fatty liver disease and risk of incident acute myocardial infarction and stroke: Findings from matched cohort study of 18 million European adults. BMJ 2019, 367, l5367. [Google Scholar] [CrossRef] [Green Version]
- Olubamwo, O.O.; Virtanen, J.K.; Voutilainen, A.; Kauhanen, J.; Pihlajamäki, J.; Tuomainen, T.-P. Association of fatty liver index with the risk of incident cardiovascular disease and acute myocardial infarction. Eur. J. Gastroenterol. Hepatol. 2018, 30, 1047–1054. [Google Scholar] [CrossRef]
- Shah, R.V.; Anderson, A.; Ding, J.; Budoff, M.; Rider, O.; Petersen, S.; Jensen, M.K.; Koch, M.; Allison, M.; Kawel-Boehm, N.; et al. Pericardial, But Not Hepatic, Fat by CT Is Associated with CV Outcomes and Structure. JACC Cardiovasc. Imaging 2017, 10, 1016–1027. [Google Scholar] [CrossRef]
- Liu, C.-J. Prevalence and risk factors for non-alcoholic fatty liver disease in Asian people who are not obese. J. Gastroenterol. Hepatol. 2012, 27, 1555–1560. [Google Scholar] [CrossRef]
- Oni, E.T.; Agatston, A.S.; Blaha, M.J.; Fialkow, J.; Cury, R.; Sposito, A.; Erbel, R.; Blankstein, R.; Feldman, T.; Al-Mallah, M.H.; et al. A systematic review: Burden and severity of subclinical cardiovascular disease among those with nonalcoholic fatty liver; Should we care? Atherosclerosis 2013, 230, 258–267. [Google Scholar] [CrossRef]
- Al Rifai, M.; Silverman, M.G.; Nasir, K.; Budoff, M.J.; Blankstein, R.; Szklo, M.; Katz, R.; Blumenthal, R.S.; Blaha, M.J. The association of nonalcoholic fatty liver disease, obesity, and metabolic syndrome, with systemic inflammation and subclinical atherosclerosis: The Multi-Ethnic Study of Atherosclerosis (MESA). Atherosclerosis 2015, 239, 629–633. [Google Scholar] [CrossRef] [Green Version]
- Ismael, H.; Tag-Adeen, M.; Abdel-Rady, A.; Shazly, M.; Hussein, A. Non-Alcoholic Fatty Liver Disease as a Coronary Heart Disease Severity Predictor. Int. J. Clin. Med. 2020, 11, 182–192. [Google Scholar] [CrossRef] [Green Version]
- Gaudio, E.; Nobili, V.; Franchitto, A.; Onori, P.; Carpino, G. Nonalcoholic fatty liver disease and atherosclerosis. Intern. Emerg. Med. 2012, 7, 297–305. [Google Scholar] [CrossRef]
- Baharvand-Ahmadi, B.; Sharifi, K.; Namdari, M. Prevalence of non-alcoholic fatty liver disease in patients with coronary artery disease. ARYA Atheroscler. 2016, 12, 201–205. [Google Scholar]
- Ismaiel, A.; Dumitraşcu, D.L. Cardiovascular Risk in Fatty Liver Disease: The Liver-Heart Axis—Literature Review. Front. Med. 2019, 6, 202. [Google Scholar] [CrossRef] [Green Version]
- Przybyszewski, E.M.; Targher, G.; Roden, M.; Corey, K.E. Nonalcoholic Fatty Liver Disease and Cardiovascular Disease. Clin. Liver Dis. 2021, 17, 19–22. [Google Scholar] [CrossRef]
- Akabame, S.; Hamaguchi, M.; Tomiyasu, K.-I.; Tanaka, M.; Kobayashi-Takenaka, Y.; Nakano, K.; Oda, Y.; Yoshikawa, T. Evaluation of Vulnerable Coronary Plaques and Non-Alcoholic Fatty Liver Disease (NAFLD) by 64-Detector Multislice Computed Tomography (MSCT). Circ. J. 2007, 72, 618–625. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.-C.; Hsu, W.-C.; Wu, H.-M.; Wang, J.-Y.; Yang, P.-Y.; Lin, I.-C. Association between the Severity of Nonalcoholic Fatty Liver Disease and the Risk of Coronary Artery Calcification. Medicina 2021, 57, 807. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Choi, S.-Y.; Park, E.H.; Lee, W.; Kang, J.H.; Kim, W.R.; Kim, Y.J.; Yoon, J.-H.; Jeong, S.H.; Lee, D.H.; et al. Nonalcoholic fatty liver disease is associated with coronary artery calcification. Hepatology 2012, 56, 605–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Xia, M.; Ma, H.; Hofman, A.; Hu, Y.; Yan, H.; He, W.; Lin, H.; Jeekel, J.; Zhao, N.; et al. Liver fat content is associated with increased carotid atherosclerosis in a Chinese middle-aged and elderly population: The Shanghai Changfeng study. Atherosclerosis 2012, 224, 480–485. [Google Scholar] [CrossRef]
- Arab, J.P.; Dirchwolf, M.; Álvares-Da-Silva, M.R.; Barrera, F.; Benítez, C.; Castellanos-Fernandez, M.; Castro-Narro, G.; Chavez-Tapia, N.; Chiodi, D.; Cotrim, H.; et al. Latin American Association for the study of the liver (ALEH) practice guidance for the diagnosis and treatment of non-alcoholic fatty liver disease. Ann. Hepatol. 2020, 19, 674–690. [Google Scholar] [CrossRef]
- Mahfood Haddad, T.; Hamdeh, S.; Kanmanthareddy, A.; Alla, V.M. Nonalcoholic fatty liver disease and the risk of clinical cardiovascular events: A systematic review and meta-analysis. Diabetes Metab. Syndr. 2017, 11 (Suppl. S1), S209–S216. [Google Scholar] [CrossRef]
- Park, G.-M.; Yun, S.-C.; Cho, Y.-R.; Gil, E.H.; Her, S.H.; Kim, S.H.; Joon-Won, K.; Lee, M.S.; Lee, S.-W.; Kim, Y.-H.; et al. Prevalence of coronary atherosclerosis in an Asian population: Findings from coronary computed tomographic angiography. Int. J. Cardiovasc. Imaging 2015, 31, 659–668. [Google Scholar] [CrossRef]
- Virmani, R.; Burke, A.P.; Farb, A.; Kolodgie, F.D. Pathology of the Vulnerable Plaque. J. Am. Coll. Cardiol. 2006, 47, C13–C18. [Google Scholar] [CrossRef] [Green Version]
- Lim, S.; Shin, H.; Lee, Y.; Yoon, J.W.; Kang, S.M.; Choi, S.H.; Park, K.S.; Jang, H.C.; Choi, S.I.; Chun, E.J. Effect of Metabolic Syndrome on Coronary Artery Stenosis and Plaque Characteristics as Assessed with 64–Detector Row Cardiac CT. Radiology 2011, 261, 437–445. [Google Scholar] [CrossRef]
- Meyersohn, N.M.; Mayrhofer, T.; Corey, K.E.; Bittner, D.O.; Staziaki, P.V.; Szilveszter, B.; Hallett, T.; Lu, M.T.; Puchner, S.B.; Simon, T.G.; et al. Association of Hepatic Steatosis with Major Adverse Cardiovascular Events, Independent of Coronary Artery Disease. Clin. Gastroenterol. Hepatol. 2020, 19, 1480–1488.e14. [Google Scholar] [CrossRef]
- Choi, D.H.; Lee, S.J.; Kang, C.D.; Park, M.O.; Choi, N.W.; Kim, T.S.; Lee, W.; Cho, B.R.; Kim, Y.H.; Lee, B.-K.; et al. Nonalcoholic fatty liver disease is associated with coronary artery disease in Koreans. World J. Gastroenterol. 2013, 19, 6453–6457. [Google Scholar] [CrossRef]
- Toh, J.Z.K.; Pan, X.-H.; Tay, P.W.L.; Ng, C.H.; Yong, J.N.; Xiao, J.; Koh, J.H.; Tan, E.Y.; Tan, E.X.X.; Dan, Y.Y.; et al. A Meta-Analysis on the Global Prevalence, Risk factors and Screening of Coronary Heart Disease in Nonalcoholic Fatty Liver Disease. Clin. Gastroenterol. Hepatol. 2021; in press. [Google Scholar] [CrossRef]
- Lee, S.B.; Park, G.-M.; Lee, J.-Y.; Lee, B.U.; Park, J.H.; Kim, B.G.; Jung, S.W.; Du Jeong, I.; Bang, S.-J.; Shin, J.W.; et al. Association between non-alcoholic fatty liver disease and subclinical coronary atherosclerosis: An observational cohort study. J. Hepatol. 2018, 68, 1018–1024. [Google Scholar] [CrossRef]
- Thomsen, C.; Abdulla, J. Characteristics of high-risk coronary plaques identified by computed tomographic angiography and associated prognosis: A systematic review and meta-analysis. Eur. Hear. J. Cardiovasc. Imaging 2015, 17, 120–129. [Google Scholar] [CrossRef]
- Niikura, T.; Imajo, K.; Ozaki, A.; Kobayashi, T.; Iwaki, M.; Honda, Y.; Kessoku, T.; Ogawa, Y.; Yoneda, M.; Kirikoshi, H.; et al. Coronary Artery Disease is More Severe in Patients with Non-Alcoholic Steatohepatitis than Fatty Liver. Diagnostics 2020, 10, 129. [Google Scholar] [CrossRef] [Green Version]
- Baratta, F.; Pastori, D.; Angelico, F.; Balla, A.; Paganini, A.M.; Cocomello, N.; Ferro, D.; Violi, F.; Sanyal, A.J.; Del Ben, M. Nonalcoholic Fatty Liver Disease and Fibrosis Associated with Increased Risk of Cardiovascular Events in a Prospective Study. Clin. Gastroenterol. Hepatol. 2020, 18, 2324–2331.e4. [Google Scholar] [CrossRef]
- Hsu, P.; Wang, Y.; Lin, C.; Wang, Y.; Ding, Y.; Liou, T.; Huang, S.; Lu, T.; Chan, W.; Lin, S.; et al. The association of the steatosis severity in fatty liver disease with coronary plaque pattern in general population. Liver Int. 2020, 41, 81–90. [Google Scholar] [CrossRef]
- Puchner, S.B.; Lu, M.T.; Mayrhofer, T.; Liu, T.; Pursnani, A.; Ghoshhajra, B.; Truong, Q.A.; Wiviott, S.D.; Fleg, J.L.; Hoffmann, U.; et al. High-Risk Coronary Plaque at Coronary CT Angiography Is Associated with Nonalcoholic Fatty Liver Disease, Independent of Coronary Plaque and Stenosis Burden: Results from the ROMICAT II Trial. Radiology 2015, 274, 693–701. [Google Scholar] [CrossRef] [Green Version]
- Targher, G.; Corey, K.E.; Byrne, C.D. NAFLD, and cardiovascular and cardiac diseases: Factors influencing risk, prediction and treatment. Diabetes Metab. 2020, 47, 101215. [Google Scholar] [CrossRef]
- Wong, V.W.-S.; Wong, G.L.-H.; Yeung, J.C.-L.; Fung, C.Y.-K.; Chan, J.K.-L.; Chang, Z.H.-Y.; Kwan, C.T.-Y.; Lam, H.-W.; Limquiaco, J.; Chim, A.M.-L.; et al. Long-term clinical outcomes after fatty liver screening in patients undergoing coronary angiogram: A prospective cohort study. Hepatology 2015, 63, 754–763. [Google Scholar] [CrossRef] [Green Version]
- Wang, L.; Li, Y.; Gong, X. Changes in inflammatory factors and prognosis of patients complicated with non-alcoholic fatty liver disease undergoing coronary artery bypass grafting. Exp. Ther. Med. 2017, 15, 949–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thévenot, T.; Vendeville, S.; Weil, D.; Akkouche, L.; Calame, P.; Canivet, C.M.; Vanlemmens, C.; Richou, C.; Cervoni, J.-P.; Seronde, M.-F.; et al. Systematic screening for advanced liver fibrosis in patients with coronary artery disease: The CORONASH study. PLoS ONE 2022, 17, e0266965. [Google Scholar] [CrossRef]
- Fiorentino, T.V.; Succurro, E.; Sciacqua, A.; Andreozzi, F.; Perticone, F.; Sesti, G. Non-alcoholic fatty liver disease is associated with cardiovascular disease in subjects with different glucose tolerance. Diabetes/Metabolism Res. Rev. 2020, 36, e3333. [Google Scholar] [CrossRef] [PubMed]
- Jana, S.B.; Paul, K.; Roy, B.; Mandal, S.C. A Correlation Study between Non-Alcoholic Fatty Liver Disease and Severity of Coronary Artery Disease. J. Med Sci. Clin. Res. 2020, 8, 4688–4699. [Google Scholar] [CrossRef]
- Liu, H.-H.; Cao, Y.-X.; Sun, D.; Jin, J.-L.; Guo, Y.-L.; Wu, N.-Q.; Zhu, C.-G.; Gao, Y.; Dong, Q.-T.; Zhao, X.; et al. Impact of Non-Alcoholic Fatty Liver Disease on Cardiovascular Outcomes in Patients with Stable Coronary Artery Disease: A Matched Case–Control Study. Clin. Transl. Gastroenterol. 2019, 10, e00011. [Google Scholar] [CrossRef]
- Langroudi, T.F.; Haybar, H.; Parsa, S.A.; Mahjoorian, M.; Khaheshi, I.; Naderian, M. The severity of coronary artery disease was not associated with non-alcoholic fatty liver disease in a series of 264 non-diabetic patients who underwent coronary angiography. Romanian J. Intern. Med. 2018, 56, 167–172. [Google Scholar] [CrossRef] [Green Version]
- Pulimaddi, R.; Parveda, A.R.; Dasari, D. Prevalence of Non-Alcoholic Fatty Liver Disease (NAFLD) in Type 2 Diabetic Patients in Correlation with Coronary Artery Disease. Int. Arch. Integr. Med. 2016, 3, 118–128. [Google Scholar]
- Sinn, D.H.; Kang, D.; Chang, Y.; Ryu, S.; Gu, S.; Kim, H.; Seong, D.; Cho, S.J.; Yi, B.-K.; Park, H.-D.; et al. Non-alcoholic fatty liver disease and progression of coronary artery calcium score: A retrospective cohort study. Gut 2016, 66, 323–329. [Google Scholar] [CrossRef]
- Idilman, I.S.; Akata, D.; Hazirolan, T.; Erdogan, B.D.; Aytemir, K.; Karcaaltincaba, M. Nonalcoholic fatty liver disease is associated with significant coronary artery disease in type 2 diabetic patients: A computed tomography angiography study. J. Diabetes 2014, 7, 279–286. [Google Scholar] [CrossRef]
- Osawa, K.; Miyoshi, T.; Yamauchi, K.; Koyama, Y.; Nakamura, K.; Sato, S.; Kanazawa, S.; Ito, H. Nonalcoholic Hepatic Steatosis Is a Strong Predictor of High-Risk Coronary-Artery Plaques as Determined by Multidetector CT. PLoS ONE 2015, 10, e0131138. [Google Scholar] [CrossRef]
- Ağaç, M.T.; Korkmaz, L.; Çavuşoğlu, G.; Karadeniz, A.G.; Ağaç, S.; Bektas, H.; Erkan, H.; Varol, M.O.; Vatan, M.B.; Acar, Z.; et al. Association Between Nonalcoholic Fatty Liver Disease and Coronary Artery Disease Complexity in Patients with Acute Coronary Syndrome. Angiology 2013, 64, 604–608. [Google Scholar] [CrossRef]
- Ballestri, S.; Meschiari, E.; Baldelli, E.; Musumeci, F.E.; Romagnoli, D.; Trenti, T.; Zennaro, R.G.; Lonardo, A.; Loria, P. Relationship of Serum Fetuin-A Levels with Coronary Atherosclerotic Burden and NAFLD in Patients Undergoing Elective Coronary Angiography. Metab. Syndr. Relat. Disord. 2013, 11, 289–295. [Google Scholar] [CrossRef]
- Josef, P.; Ali, I.; Ariel, P.; Alon, M.; Nimer, A. Relationship between Retinal Vascular Caliber and Coronary Artery Disease in Patients with Non-Alcoholic Fatty Liver Disease (NAFLD). Int. J. Environ. Res. Public Health 2013, 10, 3409–3423. [Google Scholar] [CrossRef]
- Wong, V.W.-S.; Wong, G.L.-H.; Yip, G.W.K.; Lo, A.O.S.; Limquiaco, J.; Chu, W.C.W.; Chim, A.M.-L.; Yu, C.-M.; Yu, J.; Chan, H.L.Y.; et al. Coronary artery disease and cardiovascular outcomes in patients with non-alcoholic fatty liver disease. Gut 2011, 60, 1721–1727. [Google Scholar] [CrossRef]
- Assy, N.; Djibre, A.; Farah, R.; Grosovski, M.; Marmor, A. Presence of Coronary Plaques in Patients with Nonalcoholic Fatty Liver Disease. Radiology 2010, 254, 393–400. [Google Scholar] [CrossRef] [Green Version]
- Açikel, M.; Sunay, S.; Koplay, M.; Gündoğdu, F.; Karakelleoğlu, S. Evaluation of ultrasonographic fatty liver and severity of coronary atherosclerosis, and obesity in patients undergoing coronary angiography. Anadolu Kardiyol. Derg. AKD Anatol. J. Cardiol. 2009, 9, 273–279. [Google Scholar]
- Arslan, U.; Türkoğlu, S.; Balcioğlu, S.; Tavil, Y.; Karakan, T.; Çengel, A. Association between nonalcoholic fatty liver disease and coronary artery disease. Coron. Artery Dis. 2007, 18, 433–436. [Google Scholar] [CrossRef]
- Carter, J.; Heseltine, T.D.; Meah, M.N.; Tzolos, E.; Kwiecinski, J.; Doris, M.; McElhinney, P.; Moss, A.J.; Adamson, P.D.; Hunter, A.; et al. Hepatosteatosis and Atherosclerotic Plaque at Coronary CT Angiography. Radiol. Cardiothorac. Imaging 2022, 4, e210260. [Google Scholar] [CrossRef]
- Ichikawa, K.; Miyoshi, T.; Osawa, K.; Miki, T.; Toda, H.; Ejiri, K.; Yoshida, M.; Nakamura, K.; Morita, H.; Ito, H. Incremental prognostic value of non-alcoholic fatty liver disease over coronary computed tomography angiography findings in patients with suspected coronary artery disease. Eur. J. Prev. Cardiol. 2021, 28, 2059–2066. [Google Scholar] [CrossRef]
- Wang, X.; Shen, L.; Shen, Y.; Han, F.; Ji, Z. Association between Non-alcoholic Fatty Liver Disease and the Severity of Coronary Artery Stenosis in Eastern Chinese Population. Zahedan J. Res. Med Sci. 2022, 21, 1–7. [Google Scholar] [CrossRef]
- Ichikawa, K.; Miyoshi, T.; Osawa, K.; Miki, T.; Toda, H.; Ejiri, K.; Yoshida, M.; Nanba, Y.; Yoshida, M.; Nakamura, K.; et al. Prognostic value of non-alcoholic fatty liver disease for predicting cardiovascular events in patients with diabetes mellitus with suspected coronary artery disease: A prospective cohort study. Cardiovasc. Diabetol. 2021, 20, 8. [Google Scholar] [CrossRef]
- Saraya, S.; Saraya, M.; Mahmoud, M.; Galal, M.; Soliman, H.H.; Raafat, M. The associations between coronary artery disease, and non-alcoholic fatty liver disease by computed tomography. Egypt. Hear. J. 2021, 73, 96. [Google Scholar] [CrossRef]
- Bae, Y.S.; Ko, Y.S.; Yun, J.M.; Eo, A.Y.; Kim, H. Association and Prediction of Subclinical Atherosclerosis by Nonalcoholic Fatty Liver Disease in Asymptomatic Patients. Can. J. Gastroenterol. Hepatol. 2020, 2020, 8820445. [Google Scholar] [CrossRef]
- Koo, B.K.; Allison, M.A.; Criqui, M.H.; Denenberg, J.O.; Wright, C.M. The association between liver fat and systemic calcified atherosclerosis. J. Vasc. Surg. 2019, 71, 204–211.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, Y.; Cho, Y.K.; Cho, J.; Jung, H.-S.; Yun, K.E.; Ahn, J.; Sohn, C.I.; Shin, H.; Ryu, S. Alcoholic and Nonalcoholic Fatty Liver Disease and Liver-Related Mortality: A Cohort Study. Am. J. Gastroenterol. 2019, 114, 620–629. [Google Scholar] [CrossRef] [PubMed]
- Oni, E.; Budoff, M.J.; Zeb, I.; Li, D.; Veledar, E.; Polak, J.F.; Blankstein, R.; Wong, N.D.; Blaha, M.J.; Agatston, A.; et al. Nonalcoholic Fatty Liver Disease Is Associated with Arterial Distensibility and Carotid Intima-Media Thickness: (from the Multi-Ethnic Study of Atherosclerosis). Am. J. Cardiol. 2019, 124, 534–538. [Google Scholar] [CrossRef]
- Pais, R.; Redheuil, A.; Cluzel, P.; Ratziu, V.; Giral, P. Relationship Among Fatty Liver, Specific and Multiple-Site Atherosclerosis, and 10-Year Framingham Score. Hepatology 2019, 69, 1453–1463. [Google Scholar] [CrossRef] [PubMed]
- Park, H.E.; Lee, H.; Choi, S.-Y.; Kwak, M.-S.; Yang, J.I.; Yim, J.Y.; Chung, G.E. Clinical significance of hepatic steatosis according to coronary plaque morphology: Assessment using controlled attenuation parameter. J. Gastroenterol. 2018, 54, 271–280. [Google Scholar] [CrossRef]
- Gummesson, A.; Strömberg, U.; Schmidt, C.; Kullberg, J.; Angerås, O.; Lindgren, S.; Hjelmgren, O.; Torén, K.; Rosengren, A.; Fagerberg, B.; et al. Non-alcoholic fatty liver disease is a strong predictor of coronary artery calcification in metabolically healthy subjects: A cross-sectional, population-based study in middle-aged subjects. PLoS ONE 2018, 13, e0202666. [Google Scholar] [CrossRef]
- Wu, R.; Hou, F.; Wang, X.; Zhou, Y.; Sun, K.; Wang, Y.; Liu, H.; Wu, J.; Zhao, R.; Hu, J. Nonalcoholic Fatty Liver Disease and Coronary Artery Calcification in a Northern Chinese Population: A Cross Sectional Study. Sci. Rep. 2017, 7, 9933. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, K.; Brouha, S.; Bettencourt, R.; Barrett-Connor, E.; Sirlin, C.; Loomba, R. Association of Nonalcoholic Fatty Liver Disease With Visceral Adiposity but Not Coronary Artery Calcification in the Elderly. Clin. Gastroenterol. Hepatol. 2016, 14, 1337–1344.e3. [Google Scholar] [CrossRef] [Green Version]
- Kim, B.J.; Kim, H.S.; Kang, J.G.; Kim, B.S.; Kang, J.H. Association of epicardial fat volume and nonalcoholic fatty liver disease with metabolic syndrome: From the CAESAR study. J. Clin. Lipidol. 2016, 10, 1423–1430.e1. [Google Scholar] [CrossRef]
- Park, H.E.; Kwak, M.-S.; Kim, D.; Kim, M.-K.; Cha, M.-J.; Choi, S.-Y. Nonalcoholic Fatty Liver Disease is Associated with Coronary Artery Calcification Development: A longitudinal study. J. Clin. Endocrinol. Metab. 2016, 101, 3134–3143. [Google Scholar] [CrossRef] [Green Version]
- Kim, M.K.; Ahn, C.W.; Nam, J.S.; Kang, S.; Park, J.S.; Kim, K.R. Association between nonalcoholic fatty liver disease and coronary artery calcification in postmenopausal women. Menopause 2015, 22, 1323–1327. [Google Scholar] [CrossRef] [Green Version]
- Kang, M.K.; Kang, B.H.; Kim, J.H. Nonalcoholic Fatty Liver Disease Is Associated with the Presence and Morphology of Subclinical Coronary Atherosclerosis. Yonsei Med. J. 2015, 56, 1288–1295. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.-K.; Park, H.-J.; Jeon, W.S.; Park, S.E.; Park, C.-Y.; Lee, W.-Y.; Oh, K.-W.; Park, S.-W.; Rhee, E.-J. Higher association of coronary artery calcification with non-alcoholic fatty liver disease than with abdominal obesity in middle-aged Korean men: The Kangbuk Samsung Health Study. Cardiovasc. Diabetol. 2015, 14, 88. [Google Scholar] [CrossRef] [Green Version]
- Efe, D.; Aygün, F. Assessment of the Relationship between Non-Alcoholic Fatty Liver Disease and CAD using MSCT. Arq. Bras. Cardiol. 2013, 102, 10–18. [Google Scholar] [CrossRef]
- Van Wagner, L.B.; Ning, H.; Lewis, C.E.; Shay, C.M.; Wilkins, J.; Carr, J.J.; Terry, J.G.; Lloyd-Jones, D.M.; Jacobs, D.R.; Carnethon, M.R. Associations between nonalcoholic fatty liver disease and subclinical atherosclerosis in middle-aged adults: The Coronary Artery Risk Development in Young Adults Study. Atherosclerosis 2014, 235, 599–605. [Google Scholar] [CrossRef] [Green Version]
- Chhabra, R.; O’Keefe, J.H.; Patil, H.; O’Keefe, E.; Thompson, R.C.; Ansari, S.; Kennedy, K.F.; Lee, L.W.; Helzberg, J.H. Association of Coronary Artery Calcification with Hepatic Steatosis in Asymptomatic Individuals. Mayo Clin. Proc. 2013, 88, 1259–1265. [Google Scholar] [CrossRef] [Green Version]
- Juárez-Rojas, J.G.; Medina-Urrutia, A.X.; Jorge-Galarza, E.; González-Salazar, C.; Kimura-Hayama, E.; Cardoso-Saldaña, G.; Posadas-Sánchez, R.; Martínez-Alvarado, R.; Posadas-Romero, C. Fatty Liver Increases the Association of Metabolic Syndrome with Diabetes and Atherosclerosis. Diabetes Care 2013, 36, 1726–1728. [Google Scholar] [CrossRef] [Green Version]
- Khashper, A.; Gaspar, T.; Azencot, M.; Dobrecky-Mery, I.; Peled, N.; Lewis, B.S.; Halon, D.A. Visceral abdominal adipose tissue and coronary atherosclerosis in asymptomatic diabetics. Int. J. Cardiol. 2013, 162, 184–188. [Google Scholar] [CrossRef]
- Sung, K.-C.; Lim, Y.-H.; Park, S.; Kang, S.-M.; Park, J.B.; Kim, B.-J.; Shin, J.-H. Arterial stiffness, fatty liver and the presence of coronary artery calcium in a large population cohort. Cardiovasc. Diabetol. 2013, 12, 162. [Google Scholar] [CrossRef] [Green Version]
- Arslan, U.; Kocaoğlu, I.; Balcı, M.; Duyuler, S.; Korkmaz, A. The association between impaired collateral circulation and non-alcoholic fatty liver in patients with severe coronary artery disease. J. Cardiol. 2012, 60, 210–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sung, K.-C.; Wild, S.H.; Kwag, H.J.; Byrne, C.D. Fatty Liver, Insulin Resistance, and Features of Metabolic Syndrome. Diabetes Care 2012, 35, 2359–2364. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, A.K.; Jain, V.; Singla, S.; Baruah, B.P.; Arya, V.; Yadav, R.; Singh, V.P. Prevalence of non-alcoholic fatty liver disease and its correlation with coronary risk factors in patients with type 2 diabetes. J. Assoc. Physicians India 2011, 59, 351–354. [Google Scholar] [PubMed]
- Cotter, T.G.; Rinella, M. Nonalcoholic Fatty Liver Disease 2020: The State of the Disease. Gastroenterology 2020, 158, 1851–1864. [Google Scholar] [CrossRef] [PubMed]
- Schindhelm, R.K.; Dekker, J.M.; Nijpels, G.; Bouter, L.M.; Stehouwer, C.D.; Heine, R.J.; Diamant, M. Alanine aminotransferase predicts coronary heart disease events: A 10-year follow-up of the Hoorn Study. Atherosclerosis 2007, 191, 391–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kunutsor, S.; Apekey, T.A.; Cheung, B.M. Gamma-glutamyltransferase and risk of hypertension. J. Hypertens. 2015, 33, 2373–2381. [Google Scholar] [CrossRef] [Green Version]
- Webber, M.; Krishnan, A.; Thomas, N.G.; Cheung, B.M. Association between serum alkaline phosphatase and C-reactive protein in the United States National Health and Nutrition Examination Survey 2005–2006. Clin. Chem. Lab. Med. (CCLM) 2009, 48, 167–173. [Google Scholar] [CrossRef]
- Cheung, B.M.; Ong, K.L.; Wong, L.Y. Elevated serum alkaline phosphatase and peripheral arterial disease in the United States National Health and Nutrition Examination Survey 1999–2004. Int. J. Cardiol. 2009, 135, 156–161. [Google Scholar] [CrossRef]
- Song, D.S.; Chang, U.I.; Kang, S.-G.; Song, S.-W.; Yang, J.M. Noninvasive Serum Fibrosis Markers are Associated with Coronary Artery Calcification in Patients with Nonalcoholic Fatty Liver Disease. Gut Liver 2019, 13, 658–668. [Google Scholar] [CrossRef]
- Lee, C.-O.; Li, H.-L.; Tsoi, M.-F.; Cheung, C.-L.; Cheung, B.M.Y. Association between the liver fat score (LFS) and cardiovascular diseases in the national health and nutrition examination survey 1999–2016. Ann. Med. 2021, 53, 1067–1075. [Google Scholar] [CrossRef]
- Lee, Y.-H.; Cho, Y.; Lee, B.-W.; Park, C.-Y.; Lee, D.H.; Cha, B.-S.; Rhee, E.-J. Nonalcoholic Fatty Liver Disease in Diabetes. Part I: Epidemiology and Diagnosis. Diabetes Metab. J. 2019, 43, 31–45. [Google Scholar] [CrossRef]
- Berzigotti, A.; Tsochatzis, E.; Boursier, J.; Castera, L.; Cazzagon, N.; Friedrich-Rust, M.; Petta, S.; Thiele, M. EASL Clinical Practice Guidelines on non-invasive tests for evaluation of liver disease severity and prognosis—2021 update. J. Hepatol. 2021, 75, 659–689. [Google Scholar] [CrossRef]
- European Association for Study of Liver. EASL-ALEH Clinical Practice Guidelines: Non-invasive tests for evaluation of liver disease severity and prognosis. J. Hepatol. 2015, 63, 237–264. [Google Scholar] [CrossRef] [Green Version]
- Long, M.T.; Zhang, X.; Xu, H.; Liu, C.; Corey, K.E.; Chung, R.T.; Loomba, R.; Benjamin, E.J. Hepatic Fibrosis Associates with Multiple Cardiometabolic Disease Risk Factors: The Framingham Heart Study. Hepatology 2020, 73, 548–559. [Google Scholar] [CrossRef]
- You, S.C.; Kim, K.J.; Kim, S.U.; Kim, B.K.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; Lee, W.J.; Han, K.-H. Factors associated with significant liver fibrosis assessed using transient elastography in general population. World J. Gastroenterol. 2015, 21, 1158–1166. [Google Scholar] [CrossRef]
- Magalhães, R.D.S.; Xavier, S.; Magalhães, J.; Rosa, B.; Marinho, C.; Cotter, J. Transient elastography through controlled attenuated parameter assisting the stratification of cardiovascular disease risk in NAFLD patients. Clin. Res. Hepatol. Gastroenterol. 2020, 45, 101580. [Google Scholar] [CrossRef]
- Kerut, S.E.; Balart, J.T.; Kerut, E.K.; McMullan, M.R. Diagnosis of fatty liver by computed tomography coronary artery calcium score. Echocardiography 2017, 34, 937–938. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.-M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: Developed by the Task Force for cardio-vascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies with the special contribution of the European Association of Preventive Cardiology (EAPC). Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef]
- Targher, G.; Byrne, C.D.; Tilg, H. NAFLD and increased risk of cardiovascular disease: Clinical associations, pathophysiological mechanisms and pharmacological implications. Gut 2020, 69, 1691–1705. [Google Scholar] [CrossRef]
- Niederseer, D.; Wernly, S.; Bachmayer, S.; Wernly, B.; Bakula, A.; Huber-Schönauer, U.; Semmler, G.; Schmied, C.; Aigner, E.; Datz, C. Diagnosis of Non-Alcoholic Fatty Liver Disease (NAFLD) Is Independently Associated with Cardiovascular Risk in a Large Austrian Screening Cohort. J. Clin. Med. 2020, 9, 1065. [Google Scholar] [CrossRef] [Green Version]
- Van Veelen, A.; van der Sangen, N.M.R.; Delewi, R.; Beijk, M.A.M.; Henriques, J.P.S.; Claessen, B.E.P.M. Detection of Vulnerable Coronary Plaques Using Invasive and Non-Invasive Imaging Modalities. J. Clin. Med. 2022, 11, 1361. [Google Scholar] [CrossRef]
- Xu, X.; Lu, L.; Dong, Q.; Li, X.; Zhang, N.; Xin, Y.; Xuan, S. Research advances in the relationship between nonalcoholic fatty liver disease and atherosclerosis. Lipids Heal. Dis. 2015, 14, 158. [Google Scholar] [CrossRef] [Green Version]
- Caturano, A.; Acierno, C.; Nevola, R.; Pafundi, P.C.; Galiero, R.; Rinaldi, L.; Salvatore, T.; Adinolfi, L.E.; Sasso, F.C. Non-Alcoholic Fatty Liver Disease: From Pathogenesis to Clinical Impact. Processes 2021, 9, 135. [Google Scholar] [CrossRef]
- Kang, S.H.; Cho, Y.; Jeong, S.W.; Kim, S.U.; Lee, J.-W.; Korean NAFLD Study Group. From nonalcoholic fatty liver disease to metabolic-associated fatty liver disease: Big wave or ripple? Clin. Mol. Hepatol. 2021, 27, 257–269. [Google Scholar] [CrossRef]
- Eslam, M.; Sanyal, A.J.; George, J.; on behalf of the International Consensus Panel. MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020, 158, 1999–2014.e1991. [Google Scholar] [CrossRef]
- Fernandez-Friera, L.; Fuster, V.; López-Melgar, B.; Oliva, B.; García-Ruiz, J.M.; Mendiguren, J.; Bueno, H.; Pocock, S.; Ibanez, B.; Fernández-Ortiz, A.; et al. Normal LDL-Cholesterol Levels Are Associated with Subclinical Atherosclerosis in the Absence of Risk Factors. J. Am. Coll. Cardiol. 2017, 70, 2979–2991. [Google Scholar] [CrossRef] [PubMed]
- Gariani, K.; Jornayvaz, F.R. Pathophysiology of NASH in endocrine diseases. Endocr. Connect. 2021, 10, R52–R65. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Lu, H.-Y. Nonalcoholic fatty liver disease and cardiovascular disease. World J. Gastroenterol. 2014, 20, 8407–8415. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.S.; Zhang, H.; Cheung, C.Y.Y.; Xu, M.; Ho, J.C.Y.; Zhou, W.; Cherny, S.S.; Zhang, Y.; Holmen, O.; Au, K.-W.; et al. Exome-wide association analysis reveals novel coding sequence variants associated with lipid traits in Chinese. Nat. Commun. 2015, 6, 10206. [Google Scholar] [CrossRef] [Green Version]
- Francque, S.M.; van der Graaff, D.; Kwanten, W.J. Non-alcoholic fatty liver disease and cardiovascular risk: Pathophysiological mechanisms and implications. J. Hepatol. 2016, 65, 425–443. [Google Scholar] [CrossRef] [Green Version]
- Brouwers, M.C.G.J.; Simons, N.; Stehouwer, C.D.A.; Isaacs, A. Non-alcoholic fatty liver disease and cardiovascular disease: Assessing the evidence for causality. Diabetologia 2019, 63, 253–260. [Google Scholar] [CrossRef] [Green Version]
- Simons, N.; Isaacs, A.; Koek, G.H.; Kuč, S.; Schaper, N.C.; Brouwers, M.C. PNPLA3, TM6SF2, and MBOAT7 Genotypes and Coronary Artery Disease. Gastroenterology 2017, 152, 912–913. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, C.-J.; Wang, P.W.; Hu, T.H. Association of Adiponectin Gene Polymorphism with Nonalcoholic Fatty Liver Disease in Taiwanese Patients with Type 2 Diabetes. PLoS ONE 2015, 10, e0127521. [Google Scholar] [CrossRef] [Green Version]
- Li, X.-L.; Sui, J.-Q.; Lu, L.-L.; Zhang, N.-N.; Xu, X.; Dong, Q.-Y.; Xin, Y.-N.; Xuan, S.-Y. Gene polymorphisms associated with non-alcoholic fatty liver disease and coronary artery disease: A concise review. Lipids Heal. Dis. 2016, 15, 53. [Google Scholar] [CrossRef] [Green Version]
- Dong, M.; Liu, S.; Wang, M.; Wang, Y.; Xin, Y.; Xuan, S. Relationship between AGT rs2493132 polymorphism and the risk of coronary artery disease in patients with NAFLD in the Chinese Han population. J. Int. Med Res. 2021, 49. [Google Scholar] [CrossRef]
- Pulido, M.R.; Diaz-Ruiz, A.; Jiménez-Gómez, Y.; Garcia-Navarro, S.; Gracia-Navarro, F.; Tinahones, F.; López-Miranda, J.; Frühbeck, G.; Vázquez-Martínez, R.; Malagón, M.M. Rab18 Dynamics in Adipocytes in Relation to Lipogenesis, Lipolysis and Obesity. PLoS ONE 2011, 6, e22931. [Google Scholar] [CrossRef] [Green Version]
- Mehta, R.; Otgonsuren, M.; Younoszai, Z.; Allawi, H.; Raybuck, B.; Younossi, Z. Circulating miRNA in patients with non-alcoholic fatty liver disease and coronary artery disease. BMJ Open Gastroenterol. 2016, 3, e000096. [Google Scholar] [CrossRef]
- Cao, Y.-X.; Zhang, H.-W.; Jin, J.-L.; Liu, H.-H.; Zhang, Y.; Xue, R.-X.; Gao, Y.; Guo, Y.-L.; Zhu, C.-G.; Hua, Q.; et al. Prognostic utility of triglyceride-rich lipoprotein-related markers in patients with coronary artery disease. J. Lipid Res. 2020, 61, 1254–1262. [Google Scholar] [CrossRef]
- Dongiovanni, P.; Paolini, E.; Corsini, A.; Sirtori, C.R.; Ruscica, M. Nonalcoholic fatty liver disease or metabolic dysfunction-associated fatty liver disease diagnoses and cardiovascular diseases: From epidemiology to drug approaches. Eur. J. Clin. Investig. 2021, 51, e13519. [Google Scholar] [CrossRef]
- Athyros, V.G.; Tziomalos, K.; Gossios, T.D.; Griva, T.; Anagnostis, P.; Kargiotis, K.; Pagourelias, E.D.; Theocharidou, E.; Karagiannis, A.; Mikhailidis, D.P. Safety and efficacy of long-term statin treatment for cardiovascular events in patients with coronary heart disease and abnormal liver tests in the Greek Atorvastatin and Coronary Heart Disease Evaluation (GREACE) Study: A post-hoc analysis. Lancet 2010, 376, 1916–1922. [Google Scholar] [CrossRef]
- Virtue, S.; Vidal-Puig, A. Adipose tissue expandability, lipotoxicity and the Metabolic Syndrome—An allostatic perspective. Biochim. Biophys. Acta 2010, 1801, 338–349. [Google Scholar] [CrossRef]
- Jeon, W.S.; Park, S.E.; Rhee, E.-J.; Park, C.-Y.; Oh, K.-W.; Park, S.-W.; Lee, W.-Y. Association of Serum Adipocyte-Specific Fatty Acid Binding Protein with Fatty Liver Index as a Predictive Indicator of Nonalcoholic Fatty Liver Disease. Endocrinol. Metab. 2013, 28, 283–287. [Google Scholar] [CrossRef] [Green Version]
- Lee, C.H.; Woo, Y.C.; Chow, W.S.; Cheung, C.Y.Y.; Fong, C.H.Y.; Yuen, M.M.A.; Xu, A.; Tse, H.F.; Lam, K.S.L. Role of Circulating Fibroblast Growth Factor 21 Measurement in Primary Prevention of Coronary Heart Disease Among Chinese Patients with Type 2 Diabetes Mellitus. J. Am. Hear. Assoc. 2017, 6, e005344. [Google Scholar] [CrossRef] [Green Version]
- Gómez-Ambrosi, J.; Gallego-Escuredo, J.M.; Catalán, V.; Rodríguez, A.; Domingo, P.; Moncada, R.; Valentí, V.; Salvador, J.; Giralt, M.; Villarroya, F.; et al. FGF19 and FGF21 serum concentrations in human obesity and type 2 diabetes behave differently after diet- or surgically-induced weight loss. Clin. Nutr. 2016, 36, 861–868. [Google Scholar] [CrossRef]
- Deprince, A.; Haas, J.T.; Staels, B. Dysregulated lipid metabolism links NAFLD to cardiovascular disease. Mol. Metab. 2020, 42, 101092. [Google Scholar] [CrossRef]
- Hao, Y.; Zhou, J.; Zhou, M.; Ma, X.; Lu, Z.; Gao, M.; Pan, X.; Tang, J.; Bao, Y.; Jia, W. Serum Levels of Fibroblast Growth Factor 19 Are Inversely Associated with Coronary Artery Disease in Chinese Individuals. PLoS ONE 2013, 8, e72345. [Google Scholar] [CrossRef]
- Zhou, M.; Learned, R.M.; Rossi, S.J.; DePaoli, A.M.; Tian, H.; Ling, L. Engineered FGF19 eliminates bile acid toxicity and lipotoxicity leading to resolution of steatohepatitis and fibrosis in mice. Hepatol. Commun. 2017, 1, 1024–1042. [Google Scholar] [CrossRef]
- Kasper, P.; Martin, A.; Lang, S.; Kütting, F.; Goeser, T.; Demir, M.; Steffen, H.-M. NAFLD and cardiovascular diseases: A clinical review. Clin. Res. Cardiol. 2020, 110, 921–937. [Google Scholar] [CrossRef]
- Baars, T.; Gieseler, R.K.; Patsalis, P.C.; Canbay, A. Towards harnessing the value of organokine crosstalk to predict the risk for cardiovascular disease in non-alcoholic fatty liver disease. Metabolism 2022, 130, 155179. [Google Scholar] [CrossRef]
- Cheng, Y.; An, B.; Jiang, M.; Xin, Y.; Xuan, S. Association of Tumor Necrosis Factor-alpha Polymorphisms and Risk of Coronary Artery Disease in Patients with Non-alcoholic Fatty Liver Disease. Zahedan J. Res. Med Sci. 2015, 15, e26818. [Google Scholar] [CrossRef] [Green Version]
- Simon, T.G.; Trejo, M.E.P.; McClelland, R.; Bradley, R.; Blaha, M.J.; Zeb, I.; Corey, K.E.; Budoff, M.J.; Chung, R.T. Circulating Interleukin-6 is a biomarker for coronary atherosclerosis in nonalcoholic fatty liver disease: Results from the Multi-Ethnic Study of Atherosclerosis. Int. J. Cardiol. 2018, 259, 198–204. [Google Scholar] [CrossRef]
- Otsuka, F.; Sugiyama, S.; Kojima, S.; Maruyoshi, H.; Funahashi, T.; Sakamoto, T.; Yoshimura, M.; Kimura, K.; Umemura, S.; Ogawa, H. Hypoadiponectinemia is Associated with Impaired Glucose Tolerance and Coronary Artery Disease in Non-Diabetic Men. Circ. J. 2007, 71, 1703–1709. [Google Scholar] [CrossRef] [Green Version]
- Treeprasertsuk, S.; Lopez-Jimenez, F.; Lindor, K.D. Nonalcoholic Fatty Liver Disease and the Coronary Artery Disease. Am. J. Dig. Dis. 2010, 56, 35–45. [Google Scholar] [CrossRef]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef]
- Jose, N.; Vasant, P.K.; Kulirankal, K.G. Study of Endothelial Dysfunction in Patients with Non-alcoholic Fatty Liver Disease. Cureus 2021, 13, e20515. [Google Scholar] [CrossRef]
- Yilmaz, Y.; Kurt, R.; Yonal, O.; Polat, N.; Celikel, C.A.; Gurdal, A.; Oflaz, H.; Ozdogan, O.; Imeryuz, N.; Kalayci, C.; et al. Coronary flow reserve is impaired in patients with nonalcoholic fatty liver disease: Association with liver fibrosis. Atherosclerosis 2010, 211, 182–186. [Google Scholar] [CrossRef] [PubMed]
- Keskin, M.; Hayıroğlu, M.; Uzun, A.O.; Güvenç, T.S.; Şahin, S.; Kozan, Ö. Effect of Nonalcoholic Fatty Liver Disease on In-Hospital and Long-Term Outcomes in Patients With ST–Segment Elevation Myocardial Infarction. Am. J. Cardiol. 2017, 120, 1720–1726. [Google Scholar] [CrossRef] [PubMed]
- Persico, M.; Masarone, M.; Damato, A.; Ambrosio, M.; Federico, A.; Rosato, V.; Bucci, T.; Carrizzo, A.; Vecchione, C. Non alcoholic fatty liver disease and eNOS dysfunction in humans. BMC Gastroenterol. 2017, 17, 35. [Google Scholar] [CrossRef] [Green Version]
- Frühbeck, G.; Gómez-Ambrosi, J. Control of body weight: A physiologic and transgenic perspective. Diabetologia 2003, 46, 143–172. [Google Scholar] [CrossRef] [Green Version]
- Fortuño, A.; Rodríguez, A.; Gómez-Ambrosi, J.; Muñiz, P.; Salvador, J.; Díez, J.; Frühbeck, G. Leptin Inhibits Angiotensin II-Induced Intracellular Calcium Increase and Vasoconstriction in the Rat Aorta. Endocrinology 2002, 143, 3555–3560. [Google Scholar] [CrossRef] [Green Version]
- Cernea, S.; Roiban, A.L.; Both, E.; Huţanu, A. Serum leptin and leptin resistance correlations with NAFLD in patients with type 2 diabetes. Diabetes/Metabolism Res. Rev. 2018, 34, e3050. [Google Scholar] [CrossRef]
- Silva, A.C.S.; Miranda, A.S.; Rocha, N.P.; Teixeira, A.L. Renin angiotensin system in liver diseases: Friend or foe? World J. Gastroenterol. 2017, 23, 3396–3406. [Google Scholar] [CrossRef]
- Elsheikh, E.; Younoszai, Z.; Otgonsuren, M.; Hunt, S.; Raybuck, B.; Younossi, Z.M. Markers of endothelial dysfunction in patients with non-alcoholic fatty liver disease and coronary artery disease. J. Gastroenterol. Hepatol. 2014, 29, 1528–1534. [Google Scholar] [CrossRef]
- Dallio, M.; Masarone, M.; Caprio, G.G.; Di Sarno, R.; Tuccillo, C.; Sasso, F.C.; Persico, M.; Loguercio, C.; Federico, A. Endocan Serum Levels in Patients with Non-Alcoholic Fatty Liver Disease with or without Type 2 Diabetes Mellitus: A Pilot Study. J. Gastrointest. Liver Dis. 2017, 26, 261–268. [Google Scholar] [CrossRef]
- Gurel, H.; Genç, H.; Celebi, G.; Sertoglu, E.; Cicek, A.F.; Kayadibi, H.; Ercin, C.N.; Dogru, T. Plasma pentraxin-3 is associated with endothelial dysfunction in non-alcoholic fatty liver disease. Eur. Rev. Med Pharmacol. Sci. 2016, 20, 4305–4312. [Google Scholar]
- Marušić, M.; Paić, M.; Knobloch, M.; Pršo, A.-M.L. NAFLD, Insulin Resistance, and Diabetes Mellitus Type 2. Can. J. Gastroenterol. Hepatol. 2021, 2021, 6613827. [Google Scholar] [CrossRef]
- Sanduzzi Zamparelli, M.; Compare, D.; Coccoli, P.; Rocco, A.; Nardone, O.M.; Marrone, G.; Gasbarrini, A.; Grieco, A.; Nardone, G.; Miele, L. The Metabolic Role of Gut Microbiota in the Development of Nonalcoholic Fatty Liver Disease and Cardiovascular Disease. Int. J. Mol. Sci. 2016, 17, 1225. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Xu, J.; Wang, X.; Ren, X.; Liu, Y. Changes of intestinal bacterial microbiota in coronary heart disease complicated with nonalcoholic fatty liver disease. BMC Genom. 2019, 20, 862. [Google Scholar] [CrossRef]
- Karlsson, F.H.; Fåk, F.; Nookaew, I.; Tremaroli, V.; Fagerberg, B.; Petranovic, D.; Bäckhed, F.; Nielsen, J. Symptomatic atherosclerosis is associated with an altered gut metagenome. Nat. Commun. 2012, 3, 1245. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, C.C.; Duboc, D.; Rainteau, D.; Sokol, H.; Humbert, L.; Seksik, P.; Bellino, A.; Abdoul, H.; Bouazza, N.; Treluyer, J.-M.; et al. Circulating bile acids concentration is predictive of coronary artery disease in human. Sci. Rep. 2021, 11, 22661. [Google Scholar] [CrossRef]
- Wang, Z.; Tang, W.H.W.; Buffa, J.A.; Fu, X.; Britt, E.B.; Koeth, R.A.; Levison, B.; Fan, Y.; Wu, Y.; Hazen, S.L. Prognostic value of choline and betaine depends on intestinal microbiota-generated metabolite trimethylamine-N-oxide. Eur. Hear. J. 2014, 35, 904–910. [Google Scholar] [CrossRef]
- Roberts, A.B.; Gu, X.; Buffa, J.A.; Hurd, A.G.; Wang, Z.; Zhu, W.; Gupta, N.; Skye, S.M.; Cody, D.B.; Levison, B.S.; et al. Development of a gut microbe–targeted nonlethal therapeutic to inhibit thrombosis potential. Nat. Med. 2018, 24, 1407–1417. [Google Scholar] [CrossRef]
- Lu, F.; Zheng, K.I.; Rios, R.S.; Targher, G.; Byrne, C.D.; Zheng, M. Global epidemiology of lean non-alcoholic fatty liver disease: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2020, 35, 2041–2050. [Google Scholar] [CrossRef]
- Zou, B.; Yeo, Y.H.; Nguyen, V.H.; Cheung, R.; Ingelsson, E. Prevalence, characteristics and mortality outcomes of obese, nonobese and lean NAFLD in the United States, 1999–2016. J. Intern. Med. 2020, 288, 139–151. [Google Scholar] [CrossRef]
- Aneni, E.C.; Bittencourt, M.S.; Teng, C.; Cainzos-Achirica, M.; Osondu, C.U.; Soliman, A.; Al-Mallah, M.; Buddoff, M.; Parise, E.R.; Santos, R.D.; et al. The risk of cardiometabolic disorders in lean non-alcoholic fatty liver disease: A longitudinal study. Am. J. Prev. Cardiol. 2020, 4, 100097. [Google Scholar] [CrossRef]
- Semmler, G.; Wernly, S.; Bachmayer, S.; Wernly, B.; Schwenoha, L.; Huber-Schönauer, U.; Stickel, F.; Niederseer, D.; Aigner, E.; Datz, C. Nonalcoholic Fatty Liver Disease in Lean Subjects: Associations with Metabolic Dysregulation and Cardiovascular Risk—A Single-Center Cross-Sectional Study. Clin. Transl. Gastroenterol. 2021, 12, e00326. [Google Scholar] [CrossRef]
- Golabi, P.; Paik, J.; Fukui, N.; Locklear, C.T.; de Avilla, L.; Younossi, Z.M. Patients with Lean Nonalcoholic Fatty Liver Disease Are Metabolically Abnormal and Have a Higher Risk for Mortality. Clin. Diabetes 2019, 37, 65–72. [Google Scholar] [CrossRef] [Green Version]
- Bisaccia, G.; Ricci, F.; Mantini, C.; Tana, C.; Romani, G.L.; Schiavone, C.; Gallina, S. Nonalcoholic fatty liver disease and cardiovascular disease phenotypes. SAGE Open Med. 2020, 8. [Google Scholar] [CrossRef]
- Kumar, R.; Mohan, S. Non-alcoholic Fatty Liver Disease in Lean Subjects: Characteristics and Implications. J. Clin. Transl. Hepatol. 2017, 5, 216–223. [Google Scholar] [CrossRef]
- Lee, C.-H.; Han, K.-D.; Kim, D.H.; Kwak, M.-S. The Repeatedly Elevated Fatty Liver Index Is Associated with Increased Mortality: A Population-Based Cohort Study. Front. Endocrinol. 2021, 12, 638615. [Google Scholar] [CrossRef]
- Yoshitaka, H.; Hamaguchi, M.; Kojima, T.; Fukuda, T.; Ohbora, A.; Fukui, M. Nonoverweight nonalcoholic fatty liver disease and incident cardiovascular disease. Medicine 2017, 96, e6712. [Google Scholar] [CrossRef]
- Honda, Y.; Yoneda, M.; Kessoku, T.; Ogawa, Y.; Tomeno, W.; Imajo, K.; Mawatari, H.; Fujita, K.; Hyogo, H.; Ueno, T.; et al. Characteristics of non-obese non-alcoholic fatty liver disease: Effect of genetic and environmental factors. Hepatol. Res. 2016, 46, 1011–1018. [Google Scholar] [CrossRef]
- Kuchay, M.S.; Martínez-Montoro, J.I.; Choudhary, N.S.; Fernández-García, J.C.; Ramos-Molina, B. Non-Alcoholic Fatty Liver Disease in Lean and Non-Obese Individuals: Current and Future Challenges. Biomedicines 2021, 9, 1346. [Google Scholar] [CrossRef]
- Tang, A.; Ng, C.H.; Phang, P.H.; Chan, K.E.; Chin, Y.H.; Fu, C.E.; Zeng, R.W.; Xiao, J.; Tan, D.J.H.; Quek, J.; et al. Comparative Burden of Metabolic Dysfunction in Lean NAFLD vs. Non-Lean NAFLD—A Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2022. [Google Scholar] [CrossRef]
- Kim, Y.; Han, E.; Lee, J.S.; Lee, H.W.; Kim, B.K.; Kim, M.K.; Kim, H.S.; Park, J.Y.; Kim, D.Y.; Ahn, S.H.; et al. Cardiovascular Risk Is Elevated in Lean Subjects with Nonalcoholic Fatty Liver Disease. Gut Liver 2022, 16, 290–299. [Google Scholar] [CrossRef]
- Van Wagner, L.B.; Khan, S.S.; Ning, H.; Siddique, J.; Lewis, C.E.; Carr, J.J.; Vos, M.B.; Speliotes, E.; Terrault, N.A.; Rinella, M.E.; et al. Body mass index trajectories in young adulthood predict non-alcoholic fatty liver disease in middle age: The CARDIA cohort study. Liver Int. 2017, 38, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Sung, K.C.; Ryan, M.C.; Wilson, A.M. The severity of nonalcoholic fatty liver disease is associated with increased cardiovascular risk in a large cohort of non-obese Asian subjects. Atherosclerosis 2009, 203, 581–586. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author, Year, Ref. | Country | Study Type | NAFLD Diagnosis | CAD Diagnosis | Patients Characteristics | Impact of NAFLD on CAD/ Results |
|---|---|---|---|---|---|---|
| Thévenot et al., 2022 [45] | France | Prospective (CORONASH) | NIT FibroScan | Coronary angiography | 189 | 5.3% advanced liver fibrosis (LSM ≥ 8 kPa) eLIFT, NFS—good sensitivity and specificity as first-line screening test for liver fibrosis |
| Hsu et al., 2021 [40] | Taiwan | Retrospective | US APRI | CCTA | 1502 893 NAFLD 581 CAD | Steatosis severity associated with mixed plaque pattern (p = 0.043) |
| Fiorentino et al., 2020 [46] | Italy | Retrospective | US | Coronary angiography | 1254 601 NAFLD 130 CAD | prediabetes and NAFLD—increased risk of CVD or CAD by 2.3 and 2 fold T2DM with NAFLD—2.3 and 2 fold higher risk of CVD or CAD |
| Niikura et al., 2020 [38] | Japan | Prospective | Liver biopsy | CCTA CACS (CT) | 101 NAFLD 51 CACS | NASH and fibrosis—independent RF for CAS NASH—not significantly associated with presence of CACS NASH independent RF for high-risk plaque |
| Seba et al., 2020 [47] | India | Prospective | US FibroScan | Coronary angiography SINTAX Score | 300 CAD 165 NAFLD | NAFLD associated with CAD No correlation between NAFLD grades and CAD |
| Liu HH et al., 2019 [48] | China | Prospective | US | Coronary angiography | 162 CAD 40 NAFLD | NAFLD—independent predictor of CVD outcomes in patients with stable, new-onset CAD (OR: 2.72, 95% CI: 1.16–6.39, p = 0.022) |
| Langroudi TF et al., 2018 [49] | Iran | Retrospective | US | Coronary angiography | 264 191 NAFLD 127 CHD | NAFLD presence and grade not correlated with coronary arteries ATS and its severity in non-diabetic patients |
| Pulimaddi et al., 2016 [50] | India | Cross-sectional | US | ECG/coronary angiogram/angioplasty | 150 T2DM >30 years | 59.3% prevalence of CAD in the NAFLD group (significant statistically) |
| Sinn et al., 2017 [51] | South Korea | Retrospective | US | CACS | 4731 2088 NAFLD | NAFLD significantly associated with the development of CAC independent of CV and metabolic RF |
| Idilman et al., 2015 [52] | Turkey | Retrospective | CT | CCTA | 273 T2DM 59 NAFLD 44 CAD | NAFLD—associated with CAD in T2DM p = 0.04 |
| Osawa K et al., 2015 [53] | Japan | Retrospective | CT | CT | 414 64 NAFLD 22 CHD | NAFLD—independent predictor of high-risk plaques (OR: 4.60; 95% CI: 1.94–9.07, p < 0.01 |
| Puchner SB et al., 2014 [41] | USA | Prospective | CT | CCTA | 445 205 CP 190 NCP | NAFLD—significantly associated with the presence of high-risk plaque (adjusted OR: 2.13; 95%, CI: 1.18, 3.85), adjusted for CV RF and the extent and severity of CAD |
| Agaç et al., 2013 [54] | Turkey | Prospective | US | Coronary angiography | 80, acute coronary syndrome | 81.2% patients with NAFLD and acute coronary syndrome; NAFLD associated with higher SYNTAX score (OR: 13.20; 95% CI: 2.52–69.15) |
| Ballestri S et al., 2014 [55] | Italy | Retrospective | US Fetuin-A | Coronary angiography | 29 NAFLD 20 CAD | High Fetuin-A associated with NAFLD and lower risk of CAD |
| Choi DH et al., 2013 [34] | South Korea | Prospective | US | Coronary angiography | 134 | NAFLD—independent predictor for CAD (p = 0.03, OR: 1.685; 95% CI: 1.051–2.702); Increased proportion of severe fatty liver in higher grade CAD; Adiponectin level decreased once the CAD progressed |
| Josef et al., 2013 [56] | Israel | Retrospective | CT | CCTA | 29 NAFLD 9 CHD | Smaller retinal AVR (<0.7)—increased risk for CAD and carotid atherosclerosis in NAFLD even without hypertension or diabetes |
| Wong VW-S et al., 2011 [57] | Hong Kong | Prospective | US | Coronary angiography | 612 356 NAFLD 301 CAD | Steatosis (adjusted OR: 2.31; 95% CI: 1.46–3.64) and alanine aminotransferase level (adjusted OR: 1.01; 95% CI: 1.00–1.02) independently associated with CAD |
| Assy et al., 2010 [58] | Israel | Prospective | CT | CT | 29 NAFLD 11 CHD | NAFLD—associated with high prevalence of CP and NCP, independently of the MS and CRP |
| Açikel M et al., 2009 [59] | Turkey | Retrospective | US | Coronary angiography | 355 215 NAFLD 153 CHD | NAFLD—independent predictor of CHD (> 50% stenosis of ≥1 major coronary artery) after adjustment for CVD risk factors |
| Arslan U et al., 2007 [60] | Turkey | Retrospective | US | Coronary angiography | 65 NAFLD 39 CHD | NAFLD—independent predictor of CHD (>50% stenosis of ≥1 major coronary artery) after adjustment for CVD risk factors and MS |
| Author, Year, Ref. | Country | Study Type | NAFLD Diagnosis | CAD Diagnosis | Patients Characteristics | Impact of NAFLD on CAD/Results |
|---|---|---|---|---|---|---|
| Carter et al., 2022 [61] | Scotland | Post-hoc analysis of Prospective Scottish Computed Tomography of HEART trial | CT | CT (CACS) | 1726 155 hepatic steatosis | Hepatic steatosis associated with increased prevalence of CAD No difference in MI in those with and without steatosis (1.9% vs. 2.4%, p = 0.92) |
| Ichikawa et al., 2022 [62] | Japan | Prospective | CT | CCTA | 1148 247 hepatic steatosis 977 suspected CAD | High association between hepatic steatosis and increased risk of MACE in suspected stable CAD |
| Wang X et al., 2022 [63] | China | Retrospective | FIB-4 score | Coronary angiography Gensini score | 342 105 NAFLD | NAFLD severity—associated with CAS High FIB-4 score—high CAC |
| Chen et al., 2021 [25] | Taiwan | Prospective | US | CACS (CT) | 545 437 NAFLD 242 CAC | 1.36-fold greater risk of developing CAC in patients with different severity of NAFLD vs. those without NAFLD (OR: 1.36, 95% CI: 1.07–1.77, p = 0.016) |
| Ichikawa et al., 2021 [64] | Japan | Prospective | CT | CACS FRS | 529 T2DM | NAFLD, CACS, and FRS-associated with CVE (HR and 95% CI: 5.43, 2.82–10.44, p < 0.001; 1.56, 1.32–1.86, p < 0.001; 1.23, 1.08–1.39, p = 0.001, respectively) |
| Meyersohn NM et al., 2021 [33] | North America | Nested cohort study | CT | CCTA | 3756 | Hepatic steatosis associated with MACE (4.4% vs 2.6% in those without steatosis) indepently of other CV RF/extent of CAD |
| Saraya et al., 2021 [65] | Egypt | Prospective | CT | CCTA | 800 440 CAD | NAFLD and high-risk plaque features: Napkin ring sign, Positive remodeling, Low HU, and Spotty calcium (OR: 7.88, 95% CI (4.39–14.12), p < 0.001, OR: 5.84, 95% (3.85–8.85), p < 0.001, OR: 7.25, 95% CI (3.31–15.90), p < 0.001 and OR: 6.66, 95% CI (3.75–11.82), p < 0.001) |
| Bae YS et al., 2020 [66] | South Korea | Retrospective | US NFS, FIB-4 index | CCTA | 3693 244 CAS 1588 NAFLD | NAFLD associated with CAS (≥50% stenosis) stronger in women, but absolute risk higher in men |
| Ismael H et al., 2020 [19] | Egypt | Prospective | FibroScan | Coronary angiography Gensini score | 100 42 NAFLD | S2-S3 NAFLD and CVD (OR: 24, 95% CI: 17–31) |
| Koo BK et al., 2020 [67] | USA | Retrospective | CT | CCTA | 719 NAFLD 443 CHD | NAFLD significantly associated with coronary calcification (OR: 1.28; 95% CI: 1.07–1.53) |
| Chang Y et al., 2019 [68] | South Korea | Retrospective | US FIB-4 score, APRI | CACS | 105328 34382 NAFLD 5249 CAD | NAFLD, AFLD associated with CAC |
| Oni E et al., 2019 [69] | USA | Retrospective | CT | CACS CIMT | 4123 729 NAFLD 386 CHD | NAFLD—independently associated with CAC> 0 and CIMT > 1 mm |
| Pais et al., 2019 [70] | France | Retrospective | FLI | FRS CACS (CT) | 2617 930 NAFLD | High prevalence of CAC (183 ± 425 vs 117 ± 288, p < 0.001) in those with hepatic steatosis vs without |
| Park HE et al., 2019 [71] | South Korea | Retrospective | CAP | CCTA Coronary plaque >1.5 mm2 | 330 NAFLD 186 CAD 147 NCP | CAP-defined NAFLD significantly associated with NCP, independent with cardiometabolic RF (adjusted OR: 3.528, 95% CI: 1.463–8.511, p = 0.005), no significant correlation with CP (p = 0.171) |
| Sinn DH et al., 2019 [51] | South Korea | Retrospective | US NFS | Hospitalization for MI | 111492 37263 NAFLD 183 MI | NAFLD associated with increased incidence of MI independent of RF |
| Gummesson et al., 2018 [72] | Sweden | Retrospective | CT | CACS (CT) | 106 NAFLD 73 CHD | NAFLD and CACS association in subjects with few other metabolic risk factors (60% subjects of the total cohort) with 0 or 1 of the 7 predefined RF; OR: 5.94, 95% CI: 2.13 ± 16.6 |
| Lee SB et al., 2018 [36] | South Korea | Retrospective | US, FLI, NFS | CCTA | 5121 38.6% NAFLD | NAFLD associated with NCP; significant association of FLI ≥30 with NCP (1.37, 95% CI: 1.14–1.65, p = 0.001) and NFS ≥ −1.455 with NCP (1.20, 95% CI: 1.08–1.42, p = 0.030) |
| Wu R et al., 2017 [73] | China | Retrospective | US | CACS (CT) | 2345 1272 NAFLD 237 CHD | NAFLD—significantly associated with the development of coronary artery calcifications (adjusted OR: 1.348, 95% CI: 1.030–1.765) |
| Jacobs K et al., 2016 [74] | USA | Retrospective | US | CACS (CT) (VAT) | 250 71 NAFLD 52 CHD | NAFLD and CAC—no clear association Increased CAC, VAT with age, but no increased NAFLD |
| Kim JB et al., 2016 [75] | South Korea | Retrospective | US | CT EFV | 1472 677 NAFLD 147 CHD | Higher EFV levels and NAFLD prevalence in individuals with MS than those without MS (81.0 cm3 vs 57.3 cm3, p < 0.001; 75.6% vs 36.5%, p < 0.001) |
| Park HE et al., 2016 [76] | South Korea | Retrospective | US | CCTA (CAC) | 1732 846 NAFLD 413 CAC | NAFLD associated with CAC development independent of other metabolic RF in those without CAC at baseline, but not with CAC progression in those with CAC at baseline DM risk factor for CAC progression |
| Al Rifai M et al., 2015 [18] | USA | Retrospective | CT | CACS (CT) | 3976 670 NAFLD 362 CAC | NAFLD—associated with inflammation and CAC |
| Kim MK et al., 2015 [77] | South Korea | Retrospective | US | CACS (CT) | 919 Postmenopausal women 294 NAFLD 81 CAC | OR for prevalence of CAC: no NAFLD, 1.0; mild NAFLD, 1.34 (95% CI: 0.92–2.16); moderate to severe NAFLD, 1.83 (95% CI: 1.06–3.16) NAFLD—not independent factor for CAD in postmenopausal women |
| Kang MK et al., 2015 [78] | South Korea | Retrospective | US | CT | 346 NAFLD 173 CHD | NAFLD—associated with coronary plaques OR: 1.48; 95% CI: 1.05–2.08, p = 0.025 |
| Lee M-K et al., 2015 [79] | South Korea | Retrospective | US | CACS (CT) | 10063 NAFLD 1843 CAD 340 CACS>100 | NAFLD relatively increased risk for CAC vs non-NAFLD; higher OR than that in subjects with abdominal obesity [1.360; 95% CI: 1.253–1.476) vs (1.220; 95% CI: 1.122–1.326)] |
| Efe D et al., 2014 [80] | Turkey | Retrospective | CT | CT | 372 204 NAFLD 107 CAD | Higher prevalence of CAD in NAFLD than non-NAFLD |
| VanWagner et al., 2014 [81] | USA | Retrospective | CT | CACS (CT) | 2424 232 NAFLD 88 CAD | Increased CAC (37.9% vs 26.0%, p < 0.001) in NAFLD cases Obesity attenuates NAFLD-ATS relation |
| Chhabra et al., 2013 [82] | USA | Retrospective | CT | CACS (CT) | 400 43 NAFLD 15 CAD | Hepatic steatosis—independent predictor of CACS |
| Juarez-Rojas et al., 2013 [83] | Mexico | Retrospective | CT | CACS (CT) | 765 163 NAFLD 64 CHD | Fatty liver associated with T2DM and MS |
| Khashper et al., 2013 [84] | Israel | Retrospective | CT | CACS (CT) | 318 93 NAFLD 70 CAD | Increased VAT in patients with coronary artery plaques, p < 0.001 |
| Sung KC et al., 2013 [85] | South Korea | Retrospective | US | CACS (CT) | 7371 39.5% NAFLD 4.5% CACS > 0 | Steatosis and baPWV are independently associated with the presence of CAC |
| Arslan et al., 2012 [86] | Turkey | Prospective | US | Coronary angiography | 151 98 NAFLD | 64.9% patients with NAFLD NAFLD associated with poor coronary collateral development |
| Kim D et al., 2012 [26] | South Korea | Prospective | US | CACS (CT) | 4023 1617 NAFLD 649 CAD | High CACS significantly associated with the presence of NAFLD (OR: 1.28, 95% CI: 1.04–1.59, p = 0.023) independent of visceral adiposity |
| Sung KC et al., 2012 [87] | South Korea | Retrospective | US | CACS (CT) | 3784 NAFLD 510 CAD | Steatosis (OR: 1.21, 95% CI: 1.01–1.45, p = 0.04) and HOMA-IR (1.10; 1.02–1.18, p = 0.02) associated with CACS > 0 |
| Agarwal et al., 2011 [88] | India | Prospective | US | CIMT | 124 T2DM 71 NAFLD 43 CAD | 60.5% CAD of the patients with NAFLD; 45.2% of the ones without NAFLD NAFLD—risk marker for CAD in T2DM |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cazac, G.-D.; Lăcătușu, C.-M.; Mihai, C.; Grigorescu, E.-D.; Onofriescu, A.; Mihai, B.-M. New Insights into Non-Alcoholic Fatty Liver Disease and Coronary Artery Disease: The Liver-Heart Axis. Life 2022, 12, 1189. https://doi.org/10.3390/life12081189
Cazac G-D, Lăcătușu C-M, Mihai C, Grigorescu E-D, Onofriescu A, Mihai B-M. New Insights into Non-Alcoholic Fatty Liver Disease and Coronary Artery Disease: The Liver-Heart Axis. Life. 2022; 12(8):1189. https://doi.org/10.3390/life12081189
Chicago/Turabian StyleCazac, Georgiana-Diana, Cristina-Mihaela Lăcătușu, Cătălina Mihai, Elena-Daniela Grigorescu, Alina Onofriescu, and Bogdan-Mircea Mihai. 2022. "New Insights into Non-Alcoholic Fatty Liver Disease and Coronary Artery Disease: The Liver-Heart Axis" Life 12, no. 8: 1189. https://doi.org/10.3390/life12081189