
The Value of Troponin as a Biomarker of Chemotherapy-Induced Cardiotoxicity

 , , ,
, , ,  ,
,
Abstract
:1. Introduction
2. Cardiotoxicity
- -
- Mild asymptomatic cardiac dysfunction consists of an LVEF > 50% with a rise in troponin (cTn) or natriuretic peptides and a reduction of >15% in the GLS from baseline;
- -
- Moderate asymptomatic cardiac dysfunction is defined by a reduction in the LVEF of ≥10%, which would thus be in the 40–49% range, or a smaller change in the LVEF associated with a significant fall in the GLS and/or a rise in cardiac biomarkers;
- -
- Severe asymptomatic cardiac dysfunction is defined by a reduction in the LVEF to <40% and is associated with a poor prognosis [8].
- -
- Direct or endogenous (e.g., AC)—also called primary cardiomyopathy—which is a consequence of the direct toxic effects of chemotherapy on the myocardium and is caused by myocardial cell loss, necrosis, and apoptosis mediated by oxidative stress [10].
- -
- Indirect (e.g., trastuzumab, VEGF inhibitors), which is caused by factors that do not have a direct toxic effect on cardiomyocytes, but that contribute to a decline in cardiac function. Indirect cardiomyopathy is determined by alterations in the perfusion, innervation, or hormonal background (vasoconstriction, vasospasm). Trastuzumab causes functional abnormalities, though in patients with previous AC treatment, it may exacerbate injury and myocyte death by inhibiting anti-apoptotic pathways [11].
- -
- Caused by inflammatory cell infiltration in the myocardium, which can lead to myocarditis (immune checkpoint inhibitors—ICS) [11].
- Early biochemical cardiotoxicity, which is represented by an increase in cardiac biomarkers (troponin or brain natriuretic peptide—BNP) with normal cardiac imaging.
- Early functional cardiotoxicity, which is characterized by grade III–IV diastolic dysfunction or a reduction in the GLS and normal biomarkers.
- Early mixed cardiotoxicity, which involves the presence of a normal LVEF with increased levels of biomarkers and a reduction in the GLS, or diastolic dysfunction.
- Symptomatic heart failure with preserved EF.
- Asymptomatic LV systolic dysfunction, which is indicated by a reduction in the LVEF to less than 50%, or a reduction of more than 10% resulting in a total LVEF < 55%.
- Symptomatic LV systolic dysfunction, which is represented by a symptomatic reduction in the LVEF to <50%, or a reduction of >10% resulting in a total LVEF < 55% [14].
2.1. Biomarkers for Cardiotoxicity
2.2. Troponins
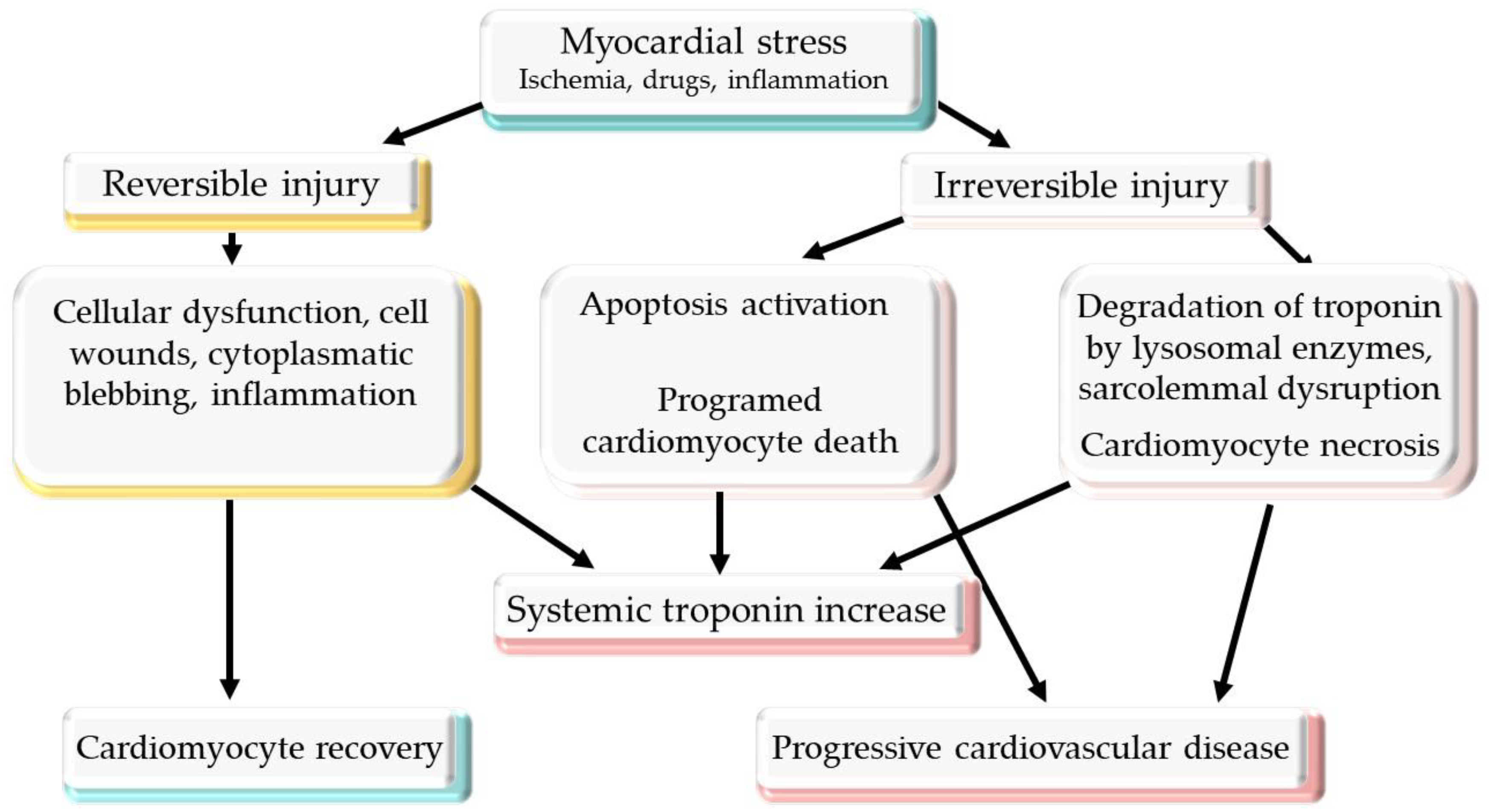
2.3. Mechanism of Troponin Release
2.4. Anthracycline
- -
- Acute toxicity in less than 1% of patients, which may occur after the first cycle of treatment or the first dose and is more common in the elderly, probably owing to underlying cardiac diseases. The forms of manifestation are represented by arrythmias, pericarditis, myocarditis, and acute LV dysfunction and are usually transient [35].
- -
- Early-onset chronic cardiotoxicity, which is more common (20–30% with asymptomatic decreases in the LVEF, or symptomatic HF in 1.6–2.1%) and can lead to irreversible cardiac dysfunction [35].
- -
- Late or chronic cardiomyopathy related to cumulative doses of AC, with an onset after more than 1 year and which is expressed as an arrythmia or LV dysfunction [10].

{kind=link}
| Study | Patients | Design | Type of Cancer | Chemotherapy | Type of cTn | Determination of cTn | Outcomes |
|---|---|---|---|---|---|---|---|
| Cardinale et al., 2000 [36] | 204 | PR | Breast cancer Ovarian carcinoma Small cell lung cancer Non-Hodgkin’s lymphoma Hodgkin’s disease | AC, radiotherapy | cTnI | Before, immediately after, and then at 12, 24, 36, and 72 h after every single cycle of high-dosage chemotherapy | LVEF decreased in cTnI group (cTnI > 0.5 ng/mL) |
| Auner et al., 2003 [40] | 78 | PR | Acute lymphoblastic leukemia Acute myeloid leukemia Non-Hodgkin’s lymphoma | AC | cTnT | Baseline and after every cycle | Elevated cTnT (>0.03 ng/mL) was associated with a significantly greater decrease in LVEF |
| Cardinale et al., 2004 [37] | 703 | PR | Breast cancer Ewing’s sarcoma Hodgkin’s disease Myeloma Non-Hodgkin’s lymphoma Ovarian carcinoma Small-cell lung cancer | AC, radiotherapy | cTnI | Baseline, after chemotherapy, at 12, 24, 36, and 72 h after every single cycle, and at 1 month after the last cycle | Patients with high levels of cTnI (>0.08 ng/mL) had a higher risk of cardiac events |
| Kilickap et al., 2005 [41] | 41 | PR | Lymphoma Breast cancer Malignant mesenchymal tumor Leukemia Nasopharyngeal carcinoma Thymic carcinoma Neuroectodermal tumor Hepatocellular carcinoma Metastasis of unknown origin Multiple myeloma | AC | cTnT | Baseline, on the 3rd and 5th days following the first dose of anthracycline, and after the last cycle of chemotherapy | High levels of cTn were associated with diastolic dysfunction (decreased E/A ratio, IRT prolongation) |
| Nistico et al., 2007 [42] | 20 | PR | Breast cancer | AC, taxanes | cTnT | Baseline, pre- and post-chemotherapy, and 12 months after the end of treatment | No cTnT serum elevations were found |
| Horacek et al., 2008 [43] | 23 | PR | Leukemia | AC | cTnT cTnI | Baseline, after the first cycle, after the last cycle, and at 6 months after completion of treatment | cTnI seemed to be superior to cTnT for the early detection of cardiac injury |
| Feola et al., 2011 [44] | 53 | PR | Breast cancer | AC | cTnI | Baseline, at 1 month, at 1 year, and at 2 years after the end of the chemotherapy | cTnI elevations were not correlated with changes in LVEF |
| Morris et al., 2011 [45] | 95 | PR | Breast cancer | AC, taxanes, trastuzumab | cTnI | Baseline, every 2 weeks during chemotherapy, and at 6, 9, and 18 months | cTnI levels did not correlate with decreased LVEF |
| Sawaya et al., 2012 [46] | 81 | PR | Breast cancer | AC, taxanes, trastuzumab | usTnI | Baseline, after AC treatment, and every 3 months until 12 months | Elevated usTnI (≥30 pg/mL) at the completion of the AC treatment was predictive of cardiotoxicity |
| Onitilo et al., 2012 [47] | 54 | PR | Breast cancer | AC, trastuzumab | cTnI | Baseline and every 3 weeks until 1 year | A decrease in LVEF was not associated with the levels of cTnI |
| Blaes et al., 2015 [48] | 18 | PR | Breast cancer Non-Hodgkin’s lymphoma | AC | cTnT, cTnI, hs-cTnT | Baseline and at 4 weeks after completion of treatment | A decline in LVEF was associated with baseline high hscTnT levels |
| Malik et al., 2016 [49] | 33 | PR | Breast cancer | AC | cTnT | Baseline, after every cycle, and at 6 months after the end of the treatment | A decrease in the left ventricular diastolic diameter was associated with high cTnT levels |
| Jones et al., 2017 [19] | 84 | PR | Breast cancer Lymphoma Leukemia Leiomyosarcoma | AC | hs-cTnI | Baseline and after every cycle | Smaller AC doses per cycle resulted in less acute cardiomyocyte injury as indicated by hs-cTnI release |
| Ferreira de Souza et al., 2018 [50] | 27 | PR | Breast cancer | AC | cTnT | Baseline, after every cycle, and at 3 and 6 months after treatment | A reduction in LVEF and LV mass was more pronounced in patients with cTnT > 10 pg/mL |
| Demisei et al., 2020 [51] | 323 | PR | Breast cancer | AC ± trastuzumab | hs-cTnT | Baseline, at 1 month, and after the end of AC treatment at 2 and 4 months | Elevated hs-cTnT (>14 ng/L) was associated with a double risk of cardiotoxicity |
| Michel et al., 2020 [39] | 61 research articles and 5691 patients | Meta-analysis | Various | AC, various high doses of chemotherapy | cTnI, cTnT | Various | In patients with elevated levels of cTn, the likelihood of LVEF dysfunction was higher than in patients with normal cTn |
| Diaz-Anton et al., 2022 [38] | 72 | PR | Breast cancer | AC ± trastuzumab | hs-cTnT | Before and after each cycle and at 1, 3, 6, and 12 months after completion of treatment | hs-cTnT increased gradually, reaching a maximum peak at 1 month after the completion of anthracycline treatment |
2.5. Trastuzumab
2.6. Immunotherapy
2.7. Anti-Vascular Endothelial Growth Factor-Targeted Therapy
3. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Michel, L.; Rassaf, T.; Totzeck, M. Biomarkers for the detection of apparent and subclinical cancer therapy-related cardiotoxicity. J. Thorac. Dis. 2018, 10 (Suppl. 35), S4282–S4295. [Google Scholar] [CrossRef] [PubMed]
- Gong, F.F.; Cascino, G.J.; Murtagh, G.; Akhter, N. Circulating Biomarkers for Cardiotoxicity Risk Prediction. Curr. Treat. Options Oncol. 2021, 22, 46. [Google Scholar] [CrossRef] [PubMed]
- Berliner, D.; Beutel, G.; Bauersachs, J. Echocardiography and biomarkers for the diagnosis of cardiotoxicity. Herz 2020, 45, 637–644. [Google Scholar] [CrossRef] [PubMed]
- Vohra, A.; Asnani, A. Biomarker Discovery in Cardio-Oncology. Curr. Cardiol. Rep. 2018, 20, 52. [Google Scholar] [CrossRef] [PubMed]
- Semeraro, G.C.; Cipolla, C.M.; Cardinale, D.M. Role of Cardiac Biomarkers in Cancer Patients. Cancers 2021, 13, 5426. [Google Scholar] [CrossRef]
- Rao, V.U.; Reeves, D.J.; Chugh, A.R.; O’Quinn, R.; Fradley, M.G.; Raghavendra, M.; Dent, S.; Barac, A.; Lenihan, D. Clinical Approach to Cardiovascular Toxicity of Oral Antineoplastic Agents: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2021, 77, 2693–2716. [Google Scholar] [CrossRef]
- Zamorano, J.L.; Lancellotti, P.; Rodriguez Muñoz, D.; Aboyans, V.; Asteggiano, R.; Galderisi, M.; Habib, G.; Lenihan, D.J.; Lip, G.Y.H.; Lyon, A.R.; et al. 2016 ESC Position Paper on cancer treatments and cardiovascular toxicity developed under the auspices of the ESC Committee for Practice Guidelines: The Task Force for cancer treatments and cardiovascular toxicity of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 2768–2801. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, J.; Lenihan, D.; Armenian, S.; Barac, A.; Blaes, A.; Cardinale, D.; Carver, J.; Dent, S.; Ky, B.; Lyon, A.R.; et al. Defining cardiovascular toxicities of cancer therapies: An International Cardio-Oncology Society (IC-OS) consensus statement. Eur. Heart J. 2022, 43, 280–299. [Google Scholar] [CrossRef]
- Xiao, H.; Wang, X.; Li, S.; Liu, Y.; Cui, Y.; Deng, X. Advances in Biomarkers for Detecting Early Cancer Treatment-Related Cardiac Dysfunction. Front. Cardiovasc. Med. 2021, 8, 753313. [Google Scholar] [CrossRef]
- Bojan, A.; Torok-Vistai, T.; Parvu, A. Assessment and Management of Cardiotoxicity in Hematologic Malignancies. Dis. Markers. 2021, 2021, 6616265. [Google Scholar] [CrossRef] [PubMed]
- Ananthan, K.; Lyon, A.R. The Role of Biomarkers in Cardio-Oncology. J. Cardiovasc. Transl. Res. 2020, 13, 431–450. [Google Scholar] [CrossRef] [PubMed]
- Herrmann, J. Adverse cardiac effects of cancer therapies: Cardiotoxicity and arrhythmia. Nat. Rev. Cardiol. 2020, 17, 474–502. [Google Scholar] [CrossRef] [PubMed]
- Čelutkienė, J.; Pudil, R.; López-Fernández, T.; Grapsa, J.; Nihoyannopoulos, P.; Bergler-Klein, J.; Cohen-Solal, A.; Farmakis, D.; Tocchetti, C.G.; von Haehling, S.; et al. Role of cardiovascular imaging in cancer patients receiving cardiotoxic therapies: A position statement on behalf of the Heart Failure Association (HFA), the European Association of Cardiovascular Imaging (EACVI) and the Cardio-Oncology Council of the European Society of Cardiology (ESC). Eur. J. Heart Fail. 2020, 22, 1504–1524. [Google Scholar] [PubMed]
- Pareek, N.; Cevallos, J.; Moliner, P.; Shah, M.; Tan, L.L.; Chambers, V.; Baksi, A.J.; Khattar, R.S.; Sharma, R.; Rosen, S.D.; et al. Activity and outcomes of a cardio-oncology service in the United Kingdom-a five-year experience. Eur. J. Heart Fail. 2018, 20, 1721–1731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stevens, P.L.; Lenihan, D.J. Cardiotoxicity due to Chemotherapy: The Role of Biomarkers. Curr. Cardiol. Rep. 2015, 17, 603. [Google Scholar] [CrossRef] [PubMed]
- Yu, A.F.; Ky, B. Roadmap for biomarkers of cancer therapy cardiotoxicity. Heart 2016, 102, 425–430. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Horacek, J.M.; Vasatova, M.; Pudil, R.; Tichy, M.; Zak, P.; Jakl, M.; Jebavy, L.; Maly, J. Biomarkers for the early detection of anthracycline-induced cardiotoxicity: Current status. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech Repub. 2014, 158, 511–517. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Semeraro, G.C.; Lamantia, G.; Cipolla, C.M.; Cardinale, D. How to identify anthracycline-induced cardiotoxicity early and reduce its clinical impact in everyday practice. Kardiol. Pol. 2021, 79, 114–122. [Google Scholar] [CrossRef]
- Jones, M.; O’Gorman, P.; Kelly, C.; Mahon, N.; Fitzgibbon, M.C. High-sensitive cardiac troponin-I facilitates timely detection of subclinical anthracycline-mediated cardiac injury. Ann. Clin. Biochem. 2017, 54, 149–157. [Google Scholar] [CrossRef]
- Tan, L.L.; Lyon, A.R. Role of Biomarkers in Prediction of Cardiotoxicity During Cancer Treatment. Curr Treat. Options Cardiovasc. Med. 2018, 20, 55. [Google Scholar] [CrossRef] [Green Version]
- Cardinale, D.; Sandri, M.T. Role of biomarkers in chemotherapy-induced cardiotoxicity. Prog. Cardiovasc. Dis. 2010, 53, 121–129. [Google Scholar] [CrossRef]
- Shah, K.S.; Yang, E.H.; Maisel, A.S.; Fonarow, G.C. The Role of Biomarkers in Detection of Cardio-toxicity. Curr. Oncol. Rep. 2017, 19, 42. [Google Scholar] [CrossRef] [Green Version]
- Muthu, V.; Kozman, H.; Liu, K.; Smulyan, H.; Villarreal, D. Cardiac troponins: Bench to bedside interpretation in cardiac disease. Am. J. Med. Sci. 2014, 347, 331–337. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, P.J. Cardiac troponin is the most effective translational safety biomarker for myocardial injury in cardiotoxicity. Toxicology 2008, 245, 206–218. [Google Scholar] [CrossRef] [PubMed]
- Soetkamp, D.; Raedschelders, K.; Mastali, M.; Sobhani, K.; Bairey Merz, C.N.; Van Eyk, J. The continuing evolution of cardiac troponin I biomarker analysis: From protein to proteoform. Expert. Rev. Proteom. 2017, 14, 973–986. [Google Scholar] [CrossRef] [PubMed]
- Sorodoc, V.; Sorodoc, L.; Ungureanu, D.; Sava, A.; Jaba, I.M. Cardiac troponin T and NT-proBNP as biomarkers of early myocardial damage in amitriptyline-induced cardiovascular toxicity in rats. Int. J. Toxicol. 2013, 32, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Pudil, R.; Mueller, C.; Čelutkienė, J.; Henriksen, P.A.; Lenihan, D.; Dent, S.; Barac, A.; Stanway, S.; Moslehi, J.; Suter, T.M.; et al. Role of serum biomarkers in cancer patients receiving cardiotoxic cancer therapies: A position statement from the Cardio-Oncology Study Group of the Heart Failure Association and the Cardio-Oncology Council of the European Society of Cardiology. Eur. J. Heart Fail. 2020, 22, 1966–1983. [Google Scholar] [CrossRef] [PubMed]
- Agewall, S.; Giannitsis, E. Troponin elevation in coronary ischemia and necrosis. Curr. Atheroscler. Rep. 2014, 16, 396. [Google Scholar] [CrossRef] [PubMed]
- Mair, J.; Lindahl, B.; Hammarsten, O.; Müller, C.; Giannitsis, E.; Huber, K.; Möckel, M.; Plebani, M.; Thygesen, K.; Jaffe, A.S. How is cardiac troponin released from injured myocardium? Eur. Heart J. Acute Cardiovasc. Care 2018, 7, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Hammarsten, O.; Mair, J.; Möckel, M.; Lindahl, B.; Jaffe, A.S. Possible mechanisms behind cardiac troponin elevations. Biomarkers 2018, 23, 725–734. [Google Scholar] [CrossRef] [Green Version]
- Gresslien, T.; Agewall, S. Troponin and exercise. Int. J. Cardiol. 2016, 221, 609–621. [Google Scholar] [CrossRef] [PubMed]
- Hickman, P.E.; Potter, J.M.; Aroney, C.; Koerbin, G.; Southcott, E.; Wu, A.H.; Roberts, M.S. Cardiac troponin may be released by ischemia alone, without necrosis. Clin. Chim. Acta 2010, 411, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Clerico, A.; Zaninotto, M.; Passino, C.; Aspromonte, N.; Piepoli, M.F.; Migliardi, M.; Perrone, M.; Fortunato, A.; Padoan, A.; Testa, A.; et al. Evidence on clinical relevance of cardiovascular risk evaluation in the general population using cardio-specific biomarkers. Clin. Chem. Lab. Med. 2020, 59, 79–90. [Google Scholar] [CrossRef] [PubMed]
- Swain, S.M.; Whaley, F.S.; Ewer, M.S. Congestive heart failure in patients treated with doxorubicin: A retrospective analysis of three trials. Cancer 2003, 97, 2869–2879. [Google Scholar] [CrossRef] [PubMed]
- Fornaro, A.; Olivotto, I.; Rigacci, L.; Ciaccheri, M.; Tomberli, B.; Ferrantini, C.; Coppini, R.; Girolami, F.; Mazzarotto, F.; Chiostri, M.; et al. Comparison of long-term outcome in anthracycline-related versus idiopathic dilated cardiomyopathy: A single centre experience. Eur. J. Heart Fail. 2018, 20, 898–906. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, D.; Sandri, M.T.; Martinoni, A.; Tricca, A.; Civelli, M.; Lamantia, G.; Cinieri, S.; Martinelli, G.; Cipolla, C.M.; Fiorentini, C. Left ventricular dysfunction predicted by early troponin I release after high-dose chemotherapy. J. Am. Coll. Cardiol. 2000, 36, 517–522. [Google Scholar] [CrossRef]
- Cardinale, D.; Sandri, M.T.; Colombo, A.; Colombo, N.; Boeri, M.; Lamantia, G.; Civelli, M.; Peccatori, F.; Martinelli, G.; Fiorentini, C.; et al. Prognostic value of troponin I in cardiac risk stratification of cancer patients undergoing high-dose chemotherapy. Circulation 2004, 109, 2749–2754. [Google Scholar] [CrossRef] [Green Version]
- Díaz-Antón, B.; Madurga, R.; Zorita, B.; Wasniewski, S.; Moreno-Arciniegas, A.; López-Melgar, B.; Ramírez Merino, N.; Martín-Asenjo, R.; Barrio, P.; Amado Escañuela, M.G.; et al. Early detection of anthracycline- and trastuzumab-induced cardiotoxicity: Value and optimal timing of serum biomarkers and echocardiographic parameters. ESC Heart Fail. 2022, 9, 1127–1137. [Google Scholar] [CrossRef] [PubMed]
- Michel, L.; Mincu, R.I.; Mahabadi, A.A.; Settelmeier, S.; Al-Rashid, F.; Rassaf, T.; Totzeck, M. Troponins and brain natriuretic peptides for the prediction of cardiotoxicity in cancer patients: A meta-analysis. Eur. J. Heart Fail. 2020, 22, 350–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Auner, H.W.; Tinchon, C.; Linkesch, W.; Tiran, A.; Quehenberger, F.; Link, H.; Sill, H. Prolonged monitoring of troponin T for the detection of anthracycline cardiotoxicity in adults with hematological malignancies. Ann. Hematol. 2003, 82, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Kilickap, S.; Barista, I.; Akgul, E.; Aytemir, K.; Aksoyek, S.; Aksoy, S.; Celik, I.; Kes, S.; Tekuzman, G. cTnT can be a useful marker for early detection of anthracycline cardiotoxicity. Ann. Oncol. 2005, 16, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Nisticò, C.; Bria, E.; Cuppone, F.; Carpino, A.; Ferretti, G.; Vitelli, G.; Sperduti, I.; Calabretta, F.; Toglia, G.; Tomao, S.; et al. Troponin-T and myoglobin plus echocardiographic evaluation for monitoring early cardiotoxicity of weekly epirubicin-paclitaxel in metastatic breast cancer patients. Anticancer Drugs. 2007, 18, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Horacek, J.M.; Pudil, R.; Tichy, M.; Jebavy, L.; Strasova, A.; Ulrychova, M.; Zak, P.; Maly, J. Cardiac troponin I seems to be superior to cardiac troponin T in the early detection of cardiac injury associated with anthracycline treatment. Onkologie 2008, 31, 559–560. [Google Scholar] [CrossRef] [PubMed]
- Feola, M.; Garrone, O.; Occelli, M.; Francini, A.; Biggi, A.; Visconti, G.; Albrile, F.; Bobbio, M.; Merlano, M. Cardiotoxicity after anthracycline chemotherapy in breast carcinoma: Effects on left ventricular ejection fraction, troponin I and brain natriuretic peptide. Int. J. Cardiol. 2011, 148, 194–198. [Google Scholar] [CrossRef] [PubMed]
- Morris, P.G.; Chen, C.; Steingart, R.; Fleisher, M.; Lin, N.; Moy, B.; Come, S.; Sugarman, S.; Abbruzzi, A.; Lehman, R.; et al. Troponin I and C-reactive protein are commonly detected in patients with breast cancer treated with dose-dense chemotherapy incorporating trastuzumab and lapatinib. Clin. Cancer Res. 2011, 17, 3490–3499. [Google Scholar] [CrossRef] [Green Version]
- Sawaya, H.; Sebag, I.A.; Plana, J.C.; Januzzi, J.L.; Ky, B.; Tan, T.C.; Cohen, V.; Banchs, J.; Carver, J.R.; Wiegers, S.E.; et al. Assessment of echocardiography and biomarkers for the extended prediction of cardiotoxicity in patients treated with anthracyclines, taxanes, and trastuzumab. Circ. Cardiovasc. Imaging 2012, 5, 596–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Onitilo, A.A.; Engel, J.M.; Stankowski, R.V.; Liang, H.; Berg, R.L.; Doi, S.A. High-sensitivity C-reactive protein (hs-CRP) as a biomarker for trastuzumab-induced cardiotoxicity in HER2-positive early-stage breast cancer: A pilot study. Breast Cancer Res. Treat. 2012, 134, 291–298. [Google Scholar] [CrossRef]
- Blaes, A.H.; Rehman, A.; Vock, D.M.; Luo, X.; Menge, M.; Yee, D.; Missov, E.; Duprez, D. Utility of high-sensitivity cardiac troponin T in patients receiving anthracycline chemotherapy. Vasc. Health Risk Manag. 2015, 11, 591–594. [Google Scholar] [CrossRef] [Green Version]
- Malik, A.; Jeyaraj, P.A.; Calton, R.; Uppal, B.; Negi, P.; Shankar, A.; Patil, J.; Mahajan, M.K. Are Biomarkers Predictive of Anthracycline-Induced Cardiac Dysfunction? Asian Pac. J. Cancer Prev. 2016, 17, 2301–2305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferreira de Souza, T.; Quinaglia AC Silva, T.; Osorio Costa, F.; Shah, R.; Neilan, T.G.; Velloso, L.; Nadruz, W.; Brenelli, F.; Sposito, A.C.; Matos-Souza, J.R.; et al. Anthracycline Therapy Is Associated with Cardiomyocyte Atrophy and Preclinical Manifestations of Heart Disease. JACC Cardiovasc. Imaging 2018, 11, 1045–1055. [Google Scholar] [CrossRef]
- Demissei, B.G.; Hubbard, R.A.; Zhang, L.; Smith, A.M.; Sheline, K.; McDonald, C.; Narayan, V.; Domchek, S.M.; DeMichele, A.; Shah, P.; et al. Changes in Cardiovascular Biomarkers with Breast Cancer Therapy and Associations with Cardiac Dysfunction. J. Am. Heart Assoc. 2020, 9, e014708. [Google Scholar] [CrossRef]
- Cardinale, D.; Colombo, A.; Sandri, M.T.; Lamantia, G.; Colombo, N.; Civelli, M.; Martinelli, G.; Veglia, F.; Fiorentini, C.; Cipolla, C.M. Prevention of high-dose chemotherapy-induced cardiotoxicity in high-risk patients by angiotensin-converting enzyme inhibition. Circulation 2006, 114, 2474–2481. [Google Scholar] [CrossRef] [Green Version]
- Cardinale, D.; Ciceri, F.; Latini, R.; Franzosi, M.G.; Sandri, M.T.; Civelli, M.; Cucchi, G.; Menatti, E.; Mangiavacchi, M.; Cavina, R.; et al. ICOS-ONE Study Investigators. Anthracycline-induced cardiotoxicity: A multicenter randomised trial comparing two strategies for guiding prevention with enalapril: The International CardioOncology Society-one trial. Eur. J. Cancer. 2018, 94, 126–137. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, D.; Colombo, A.; Lamantia, G.; Colombo, N.; Civelli, M.; De Giacomi, G.; Rubino, M.; Veglia, F.; Fiorentini, C.; Cipolla, C.M. Anthracycline-induced cardiomyopathy: Clinical relevance and response to pharmacologic therapy. J. Am. Coll. Cardiol. 2010, 55, 213–220. [Google Scholar] [CrossRef] [Green Version]
- Xu, T.; Meng, Q.H.; Gilchrist, S.C.; Lin, S.H.; Lin, R.; Xu, T.; Milgrom, S.A.; Gandhi, S.J.; Wu, H.; Zhao, Y.; et al. Assessment of Prognostic Value of High-Sensitivity Cardiac Troponin T for Early Prediction of Chemoradiation Therapy-Induced Cardiotoxicity in Patients with Non-Small Cell Lung Cancer: A Secondary Analysis of a Prospective Randomized Trial. Int. J. Radiat. Oncol. Biol. Phys. 2021, 111, 907–916. [Google Scholar] [CrossRef]
- Kirkham, A.A.; Pituskin, E.; Thompson, R.B.; Mackey, J.R.; Koshman, S.L.; Jassal, D.; Pitz, M.; Haykowsky, M.J.; Pagano, J.J.; Chow, K.; et al. Cardiac and cardiometabolic phenotyping of trastuzumab-mediated cardiotoxicity: A secondary analysis of the MANTICORE trial. Eur. Heart J. Cardiovasc. Pharmacother. 2022, 8, 130–139. [Google Scholar] [CrossRef]
- Dempsey, N.; Rosenthal, A.; Dabas, N.; Kropotova, Y.; Lippman, M.; Bishopric, N.H. Trastuzumab-induced cardiotoxicity: A review of clinical risk factors, pharmacologic prevention, and cardiotoxicity of other HER2-directed therapies. Breast Cancer Res. Treat. 2021, 188, 21–36. [Google Scholar] [CrossRef] [PubMed]
- Bouwer, N.I.; Jager, A.; Liesting, C.; Kofflard, M.J.M.; Brugts, J.J.; Kitzen, J.J.E.M.; Boersma, E.; Levin, M.D. Cardiac monitoring in HER2-positive patients on trastuzumab treatment: A review and implications for clinical practice. Breast 2020, 52, 33–44. [Google Scholar] [CrossRef] [PubMed]
- Cardinale, D.; Colombo, A.; Torrisi, R.; Sandri, M.T.; Civelli, M.; Salvatici, M.; Lamantia, G.; Colombo, N.; Cortinovis, S.; Dessanai, M.A.; et al. Trastuzumab-induced cardiotoxicity: Clinical and prognostic implications of troponin I evaluation. J. Clin. Oncol. 2010, 28, 3910–3916. [Google Scholar] [CrossRef] [PubMed]
- Fallah-Rad, N.; Walker, J.R.; Wassef, A.; Lytwyn, M.; Bohonis, S.; Fang, T.; Tian, G.; Kirkpatrick, I.D.; Singal, P.K.; Krahn, M.; et al. The utility of cardiac biomarkers, tissue velocity and strain imaging, and cardiac magnetic resonance imaging in predicting early left ventricular dysfunction in patients with human epidermal growth factor receptor II-positive breast cancer treated with adjuvant trastuzumab therapy. J. Am. Coll. Cardiol. 2011, 57, 2263–2270. [Google Scholar] [PubMed]
- Ky, B.; Putt, M.; Sawaya, H.; French, B.; Januzzi JLJr Sebag, I.A.; Plana, J.C.; Cohen, V.; Banchs, J.; Carver, J.R.; Wiegers, S.E.; et al. Early increases in multiple biomarkers predict subsequent cardiotoxicity in patients with breast cancer treated with doxorubicin, taxanes, and trastuzumab. J. Am. Coll. Cardiol. 2014, 63, 809–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zardavas, D.; Suter, T.M.; Van Veldhuisen, D.J.; Steinseifer, J.; Noe, J.; Lauer, S.; Al-Sakaff, N.; Piccart-Gebhart, M.J.; de Azambuja, E. Role of Troponins I and T and N-Terminal Prohormone of Brain Natriuretic Peptide in Monitoring Cardiac Safety of Patients with Early-Stage Human Epidermal Growth Factor Receptor 2-Positive Breast Cancer Receiving Trastuzumab: A Herceptin Adjuvant Study Cardiac Marker Substudy. J. Clin. Oncol. 2017, 35, 878–884. [Google Scholar] [PubMed]
- Yu, A.F.; Manrique, C.; Pun, S.; Liu, J.E.; Mara, E.; Fleisher, M.; Patil, S.; Jones, L.W.; Steingart, R.M.; Hudis, C.A.; et al. Cardiac Safety of Paclitaxel Plus Trastuzumab and Pertuzumab in Patients with HER2-Positive Metastatic Breast Cancer. Oncologist 2016, 21, 418–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Vries Schultink, A.H.M.; Boekhout, A.H.; Gietema, J.A.; Burylo, A.M.; Dorlo, T.P.C.; van Hasselt, J.G.C.; Schellens, J.H.M.; Huitema, A.D.R. Pharmacodynamic modeling of cardiac biomarkers in breast cancer patients treated with anthracycline and trastuzumab regimens. J. Pharmacokinet. Pharmacodyn. 2018, 45, 431–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponde, N.; Bradbury, I.; Lambertini, M.; Ewer, M.; Campbell, C.; Ameels, H.; Zardavas, D.; Di Cosimo, S.; Baselga, J.; Huober, J.; et al. Cardiac biomarkers for early detection and prediction of trastuzumab and/or lapatinib-induced cardiotoxicity in patients with HER2-positive early-stage breast cancer: A NeoALTTO sub-study (BIG 1-06). Breast Cancer Res. Treat. 2018, 168, 631–638. [Google Scholar] [CrossRef]
- Ben Kridis, W.; Sghaier, S.; Charfeddine, S.; Toumi, N.; Daoud, J.; Kammoun, S.; Khanfir, A. A Prospective Study About Trastuzumab-induced Cardiotoxicity in HER2-positive Breast Cancer. Am. J. Clin. Oncol. 2020, 43, 510–516. [Google Scholar] [CrossRef] [PubMed]
- Seidman, A.; Hudis, C.; Pierri, M.K.; Shak, S.; Paton, V.; Ashby, M.; Murphy, M.; Stewart, S.J.; Keefe, D. Cardiac dysfunction in the trastuzumab clinical trials experience. J. Clin. Oncol. 2002, 20, 1215–1221. [Google Scholar] [CrossRef]
- Rushton, M.; Johnson, C.; Dent, S. Trastuzumab-induced cardiotoxicity: Testing a clinical risk score in a real-world cardio-oncology population. Curr. Oncol. 2017, 24, 176–180. [Google Scholar] [CrossRef] [Green Version]
- Viani, G.A.; Afonso, S.L.; Stefano, E.J.; De Fendi, L.I.; Soares, F.V. Adjuvant trastuzumab in the treatment of her-2-positive early breast cancer: A meta-analysis of published randomized trials. BMC Cancer 2007, 7, 153. [Google Scholar] [CrossRef] [Green Version]
- Witteles, R.M. Biomarkers as Predictors of Cardiac Toxicity from Targeted Cancer Therapies. J. Card Fail. 2016, 22, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Ganatra, S.; Parikh, R.; Neilan, T.G. Cardiotoxicity of Immune Therapy. Cardiol Clin. 2019, 37, 385–397. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, S.S.; Fradley, M.G.; Cohen, J.V.; Nohria, A.; Reynolds, K.L.; Heinzerling, L.M.; Sullivan, R.J.; Damrongwatanasuk, R.; Chen, C.L.; Gupta, D.; et al. Myocarditis in Patients Treated with Immune Checkpoint Inhibitors. J. Am. Coll. Cardiol. 2018, 71, 1755–1764. [Google Scholar] [CrossRef] [PubMed]
- Bonaca, M.P.; Olenchock, B.A.; Salem, J.E.; Wiviott, S.D.; Ederhy, S.; Cohen, A.; Stewart, G.C.; Choueiri, T.K.; Di Carli, M.; Allenbach, Y.; et al. Myocarditis in the Setting of Cancer Therapeutics: Proposed Case Definitions for Emerging Clinical Syndromes in Cardio-Oncology. Circulation 2019, 140, 80–91. [Google Scholar] [CrossRef] [PubMed]
- Spallarossa, P.; Tini, G.; Sarocchi, M.; Arboscello, E.; Grossi, F.; Queirolo, P.; Zoppoli, G.; Ameri, P. Identification and Management of Immune Checkpoint Inhibitor-Related Myocarditis: Use Troponin Wisely. J. Clin. Oncol. 2019, 37, 2201–2205. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chitturi, K.R.; Xu, J.; Araujo-Gutierrez, R.; Bhimaraj, A.; Guha, A.; Hussain, I.; Kassi, M.; Bernicker, E.H.; Trachtenberg, B.H. Immune Checkpoint Inhibitor-Related Adverse Cardiovascular Events in Patients with Lung Cancer. JACC Cardio Oncol. 2019, 1, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Ederhy, S.; Massard, C.; Dufaitre, G.; Balheda, R.; Meuleman, C.; Rocca, C.G.; Izzedine, H.; Cohen, A.; Soria, J.C. Frequency and management of troponin I elevation in patients treated with molecular targeted therapies in phase I trials. Investig. New Drugs 2012, 30, 611–615. [Google Scholar] [CrossRef] [PubMed]

| Study | Patients | Design | Type of Cancer | Chemotherapy | Type of cTn | Determination of cTn | Outcomes |
|---|---|---|---|---|---|---|---|
| Cardinale et al., 2010 [59] | 251 | PR | Breast cancer | TRA | cTnI | Baseline and before and after each trastuzumab cycle | cTnI > 0.08 ng/mL was the strongest independent predictor of cardiotoxicity |
| Fallah-Rad et al., 2011 [60] | 42 | PR | Breast cancer | AC, TRA | cTnT | Before AC, before trastuzumab therapy, and 3, 6, 9, and 12 months after the initiation of trastuzumab | cTnT did not show any significant changes over 1 year of follow-up |
| Ky et al., 2014 [61] | 78 | PR | Breast cancer | AC, taxanes, TRA | us-cTnI | Baseline and every 3 months (maximum 15 months) | cTnI was associated with the risk of cardiotoxicity |
| Zardavas et al., 2016 [62] | 533 | PR | Breast cancer | TRA | us-cTnI hs-cTnT | Baseline; weeks 13, 25, and 52; and months 18, 24, 30, and 36 | High-baseline cTnT and cTnI was associated with a 4-fold increased risk of cardiac dysfunction |
| Yu et al., 2016 [63] | 69 | Phase 2 sub-study | Breast cancer | Paclitaxel, TRA, pertuzumab | cTnI | Baseline and before every cycle | cTnI (>0.06 ng/mL) was not associated with a decline in LVEF |
| de Vries Schultink et al., 2017 [64] | 206 | Secondary analysis of randomized placebo-controlled clinical trial | Breast cancer | AC, TRA | cTnT | Before AC treatment, before starting trastuzumab treatment, and 3, 12, 24, 36, 52, 64, 78, and 92 weeks afterwards | Maximum concentration of cTnT after AC treatment was an important determinant of reduced LVEF |
| Ponde et al., 2018 [65] | 280 | Phase III trial sub-study | Breast cancer | Lapatinib, TRA, paclitaxel | cTnT | Baseline and on weeks 2 and 18 | No correlation between high cTnT levels and cardiac events |
| Ben Kridis et al., 2020 [66] | 50 | PR | Breast cancer | AC, taxanes, TRA | us-cTnI | Baseline and at 3, 6, 9, 12, and 15 months | Levels of us-cTnI at the completion of AC treatment were predictive of the occurrence of cardiotoxicity |
| Kirkman et al., 2022 [56] | 94 | Secondary analysis of randomized controlled trial | Breast cancer | TRA | cTnI | Before trastuzumab treatment, post-cycle 4, and post-cycle 17 | No significant changes in cTnI were detected |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sorodoc, V.; Sirbu, O.; Lionte, C.; Haliga, R.E.; Stoica, A.; Ceasovschih, A.; Petris, O.R.; Constantin, M.; Costache, I.I.; Petris, A.O.; et al. The Value of Troponin as a Biomarker of Chemotherapy-Induced Cardiotoxicity. Life 2022, 12, 1183. https://doi.org/10.3390/life12081183
Sorodoc V, Sirbu O, Lionte C, Haliga RE, Stoica A, Ceasovschih A, Petris OR, Constantin M, Costache II, Petris AO, et al. The Value of Troponin as a Biomarker of Chemotherapy-Induced Cardiotoxicity. Life. 2022; 12(8):1183. https://doi.org/10.3390/life12081183
Chicago/Turabian StyleSorodoc, Victorita, Oana Sirbu, Catalina Lionte, Raluca Ecaterina Haliga, Alexandra Stoica, Alexandr Ceasovschih, Ovidiu Rusalim Petris, Mihai Constantin, Irina Iuliana Costache, Antoniu Octavian Petris, and et al. 2022. "The Value of Troponin as a Biomarker of Chemotherapy-Induced Cardiotoxicity" Life 12, no. 8: 1183. https://doi.org/10.3390/life12081183