
Analysis of Types of Skin Lesions and Diseases in Everyday Infectious Disease Practice—How Experienced Are We?

 ,
,
Abstract
:1. Introduction
2. Patients and Methods
3. Results
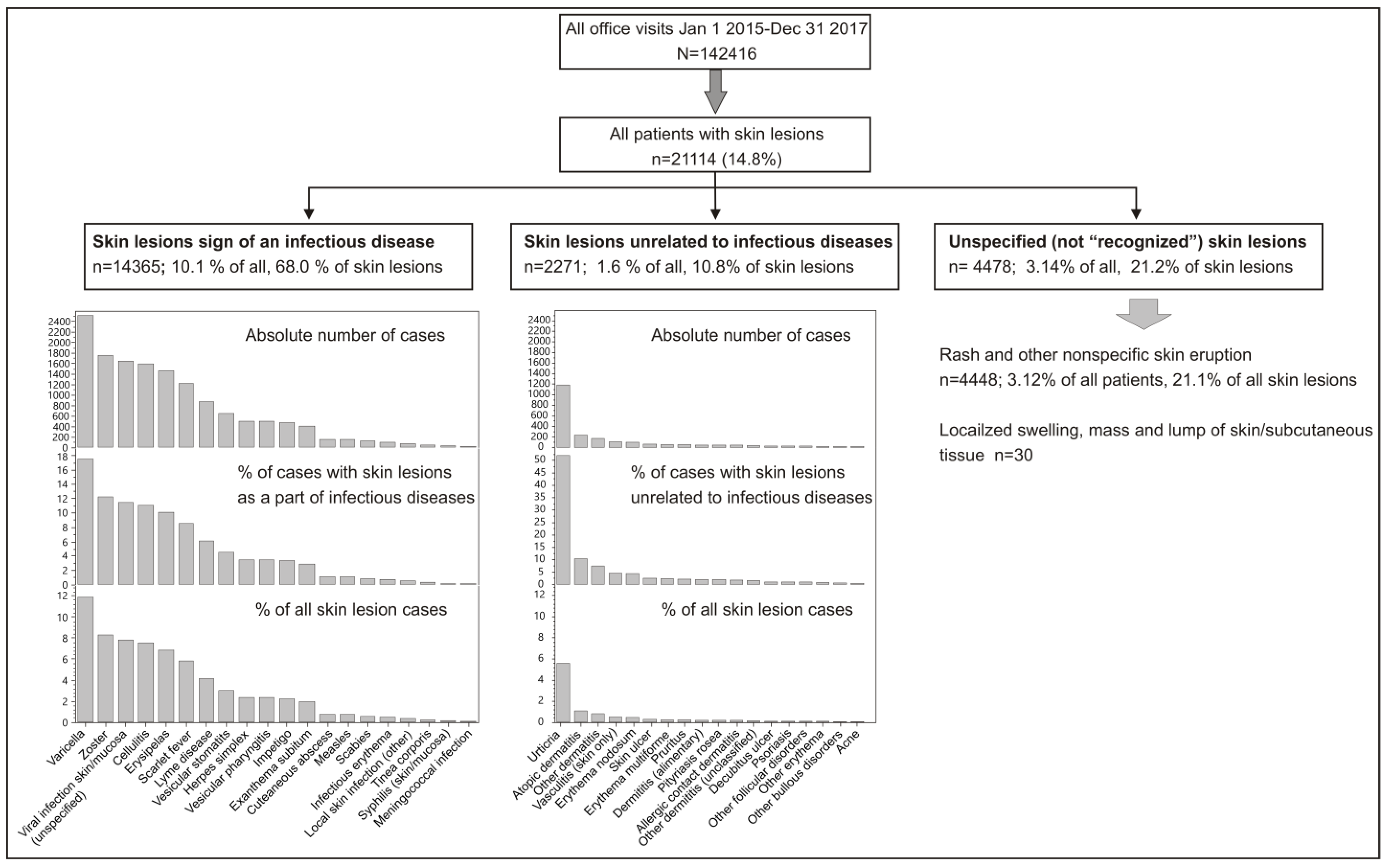
3.1. Outpatients
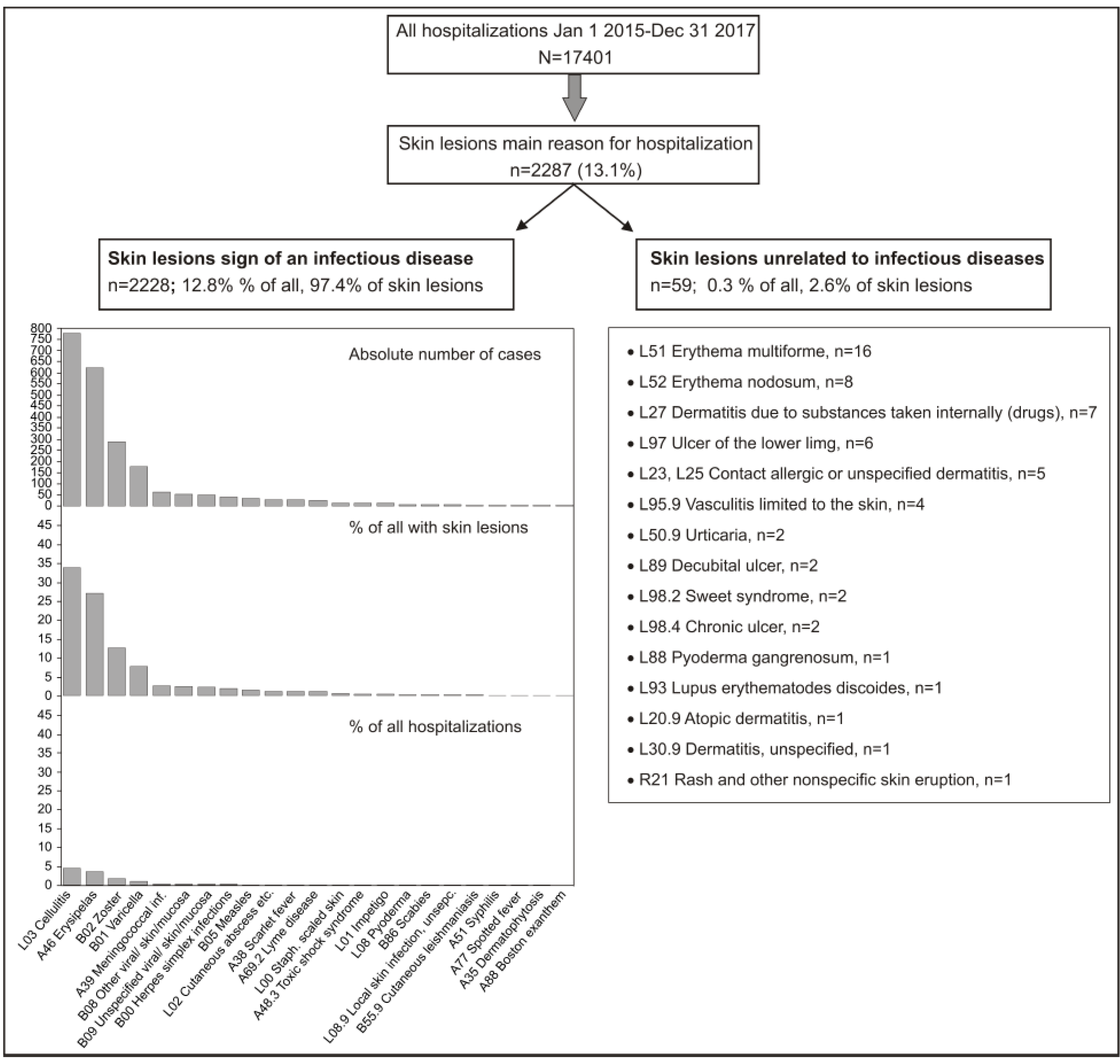
3.2. Inpatients
4. Discussion
- (1)
- Study population
- (2)
- Inclusion criteria
- (3)
- Aim
- (4)
- Study design
- (1)
- It is possible that the number of patients with skin lesions is underreported due to the exclusion of diagnoses that include skin lesions as a non-compulsory part of the clinical presentation. These diagnoses include leptospirosis, bartonellosis, rotavirus infections, dengue fever, infections caused by mycoplasma pneumoniae, human immunodeficiency virus infection, Epstein–Barr virus infections, toxoplasmosis, malaria, etc.
- (2)
- It is possible that there was a greater number of hospitalized patients with skin lesions that were not included in this study, as the skin lesions they may have presented with were not the cause of hospitalization or part of the primary diagnosis.
- (3)
- The proportion of skin lesions classified as unspecified (R21 and R22) might be higher than reported due to individual classification preferences of clinicians. An example of such a preference is the fact that an unspecified cause can be also reported under L30 (Other dermatitis).
- (4)
- Not all diagnoses could be classified unanimously as infectious or unrelated to infections. One such diagnosis is erythema nodosum (L52), which can occur secondary to a wide variety of conditions; however, an infection (primarily streptococcal) is the most commonly identified etiology [51].
- (5)
- The reasons for using codes for unspecified skin lesions (R21, R22) can be multiple: (a) a skin lesion not being recognized; (b) uncertainty in the diagnosis—the coding system cannot determine the physician’s confidence in certain diagnoses; (c) a lack of code to accurately describe the condition. It is possible that not all skin lesions classified as “undiagnosed” were unrecognized.
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hay, R.J.; Johns, N.E.; Williams, H.C.; Bolliger, I.W.; Dellavalle, R.P.; Margolis, D.J.; Marks, R.; Naldi, L.; Weinstock, M.A.; Wulf, S.K.; et al. The global burden of skin disease in 2010: An analysis of the prevalence and impact of skin conditions. J. Investig. Dermatol. 2014, 134, 1527–1534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karimkhani, C.; Dellavalle, R.P.; Coffeng, L.E.; Flohr, C.; Hay, R.J.; Langan, S.M.; Nsoesie, E.O.; Ferrari, A.J.; Erskine, H.E.; Silverberg, J.I.; et al. Global Skin Disease Morbidity and Mortality: An Update from the Global Burden of Disease Study 2013. JAMA Dermatol. 2017, 153, 406–412. [Google Scholar] [CrossRef]
- Seth, D.; Cheldize, K.; Brown, D.; Freeman, E.F. Global Burden of Skin Disease: Inequities and Innovations. Curr. Dermatol. Rep. 2017, 6, 204–210. [Google Scholar] [CrossRef] [PubMed]
- Verhoeven, E.W.; Kraaimaat, F.W.; van Weel, C.; van de Kerkhof, P.C.; Duller, P.; van der Valk, P.G.; van den Hoogen, H.J.; Bor, J.H.; Schers, H.J.; Evers, A.W. Skin diseases in family medicine: Prevalence and health care use. Ann. Fam. Med. 2008, 6, 349–354. [Google Scholar] [CrossRef] [Green Version]
- Yeroushalmi, S.; Shirazi, J.Y.; Friedman, A. New Developments in Bacterial; Viral; and Fungal Cutaneous Infections. Curr. Dermatol. Rep. 2020, 9, 152–165. [Google Scholar] [CrossRef]
- Sanders, C.V.; Lopez, F.A. Cutaneous manifestations of infectious diseases: Approach to the patient with fever and rash. Trans. Am. Clin. Climatol. Assoc. 2001, 112, 235–251, discussion 251–252. [Google Scholar]
- Miró, E.M.; Sánchez, N.P. Cutaneous Manifestations of Infectious Diseases. In Atlas of Dermatology in Internal Medicine; Sánchez, N., Ed.; Springer: New York, NY, USA, 2012; pp. 77–119. [Google Scholar]
- Mims, C.A. Pathogenesis of rashes in virus diseases. Bacteriol. Rev. 1966, 30, 739–760. [Google Scholar] [CrossRef]
- Esposito, S.; Noviello, S.; Leone, S. Epidemiology and microbiology of skin and soft tissue infections. Curr. Opin. Infect. Dis. 2016, 29, 109–115. [Google Scholar] [CrossRef]
- Ki, V.; Rotstein, C. Bacterial skin and soft tissue infections in adults: A review of their epidemiology; pathogenesis; diagnosis; treatment and site of care. Can. J. Infect. Dis. Med. Microbiol. 2008, 19, 173–184. [Google Scholar] [CrossRef] [Green Version]
- Silverberg, B. A Structured Approach to Skin and Soft Tissue Infections (SSTIs) in an Ambulatory Setting. Clin. Pract. 2021, 11, 65–74. [Google Scholar] [CrossRef]
- Ramakrishnan, K.; Salinas, R.C.; Agudelo Higuita, N.I. Skin and Soft Tissue Infections. Am. Fam. Physician. 2015, 92, 474–483. [Google Scholar] [PubMed]
- Cherry, J.D. Contemporary infectious exanthems. Clin. Infect. Dis. 1993, 16, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Soman, L. Fever with Rashes. Indian. J. Pediatr. 2018, 85, 528–534. [Google Scholar] [CrossRef] [PubMed]
- Muzumdar, S.; Rothe, M.J.; Grant-Kels, J.M. The rash with maculopapules and fever in children. Clin. Dermatol. 2019, 37, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Drago, F.; Paolino, S.; Rebora, A.; Broccolo, F.; Drago, F.; Cardo, P.; Parodi, A. The challenge of diagnosing atypical exanthems: A clinico-laboratory study. J. Am. Acad. Dermatol. 2012, 67, 1282–1288. [Google Scholar] [CrossRef]
- Drago, F.; Ciccarese, G.; Gasparini, G.; Cogorno, L.; Javor, S.; Toniolo, A.; Broccolo, F. Contemporary infectious exanthems: An update. Future Microbiol. 2017, 12, 171–193. [Google Scholar] [CrossRef] [Green Version]
- Patel, T.; Quow, K.; Cardones, A.R. Management of Infectious Emergencies for the Inpatient Dermatologist. Curr. Dermatol. Rep. 2021, 10, 232–242. [Google Scholar] [CrossRef]
- Ely, J.W.; Seabury Stone, M. The generalized rash: Part I. Differential diagnosis. Am. Fam. Physician 2010, 81, 726–734. [Google Scholar]
- Ely, J.W.; Seabury Stone, M. The generalized rash: Part II. Diagnostic approach. Am. Fam. Physician 2010, 81, 735–739. [Google Scholar]
- Kang, J.H. Febrile Illness with Skin Rashes. Infect. Chemother. 2015, 47, 155–166. [Google Scholar] [CrossRef] [Green Version]
- Kingston, M.E.; Mackey, D. Skin clues in the diagnosis of life-threatening infections. Rev. Infect. Dis. 1986, 8, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Bigby, M. Rates of cutaneous reactions to drugs. Arch. Dermatol. 2001, 137, 765–770. [Google Scholar] [PubMed]
- Fenton, A.; Elliott, E.; Shahbandi, A.; Ezenwa, E.; Morris, C.; McLawhorn, J.; Jackson, J.G.; Allen, P.; Murina, A. Medical students’ ability to diagnose common dermatologic conditions in skin of color. J. Am. Acad. Dermatol. 2020, 83, 957–958. [Google Scholar] [CrossRef]
- Antic, M.; Conen, D.; Itin, P.H. Teaching effects of dermatological consultations on nondermatologists in the field of internal medicine. A study of 1290 inpatients. Dermatology 2004, 208, 32–37. [Google Scholar] [CrossRef]
- Wilmer, E.N.; Gustafson, C.J.; Ahn, C.S.; Davis, S.A.; Feldman, S.R.; Huang, W.W. Most common dermatologic conditions encountered by dermatologists and nondermatologists. Cutis 2014, 94, 285–292. [Google Scholar] [PubMed]
- Kilic, D.; Yigit, O.; Kilic, T.; Buyurgan, C.S.; Dicle, O. Epidemiologic Characteristics of Patients Admitted to Emergency Department with Dermatological Complaints; a Retrospective Cross sectional Study. Arch. Acad. Emerg Med. 2019, 7, e47. [Google Scholar] [PubMed]
- Isnard, C.; Ingen-Housz-Oro, S.; Fardet, L.; Matteodo, E.; Duval, S.; Hemery, F.; Khellaf, M.; Duong, T.-A.; Chosidow, O.; Wolkenstein, P. Dermatological emergencies: Evolution from 2008 to 2014 and perspectives. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 274–279. [Google Scholar] [CrossRef]
- Martínez-Martínez, M.L.; Escario-Travesedo, E.; Rodríguez-Vázquez, M.; Azaña-Defez, J.M.; Martín de Hijas-Santos, M.C.; Juan-Pérez-García, L. Dermatology consultations in an emergency department prior to establishment of emergency dermatology cover. Actas Dermosifiliogr. 2011, 102, 39–47. [Google Scholar] [CrossRef]
- Rubegni, P.; Cevenini, G.; Lamberti, A.; Bruni, F.; Tiezzi, R.; Verzuri, A.; Barbini, P.; Manzi, P.; Fimiani, M. Dermatological conditions presenting at the Emergency Department in Siena University Hospital from 2006 to 2011. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 164–168. [Google Scholar] [CrossRef]
- Grillo, E.; Vañó-Galván, S.; Jiménez-Gómez, N.; Ballester, A.; Muñoz-Zato, E.; Jaén, P. Dermatologic emergencies: Descriptive analysis of 861 patients in a tertiary care teaching hospital. Actas. Dermosifiliogr. 2013, 104, 316–324. [Google Scholar] [CrossRef]
- Kim, J.Y.; Cho, H.H.; Hong, J.S.; Jin, S.P.; Park, H.S.; Lee, J.H.; Cho, S. Skin conditions presenting in emergency room in Korea: An eight-year retrospective analysis. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 479–485. [Google Scholar] [CrossRef] [PubMed]
- Bancalari-Díaz, D.; Gimeno-Mateos, L.I.; Cañueto, J.; Andrés-Ramos, I.; Fernández-López, E.; Román-Curto, C. Dermatologic emergencies in a tertiary hospital: A descriptive study. Actas Dermosifiliogr. 2016, 107, 666–673. [Google Scholar] [CrossRef] [PubMed]
- Ozkur, E.; Altunay, I.; Sekerlisoy, G.; Erdem, Y. Evaluation of Dermatology Consultations in a Tertiary Care Centre Emergency Service. Med. Bull. Sisli Etfal Hosp. 2020, 54, 197–200. [Google Scholar]
- Drago, F.; Gasparini, G.; Signori, A.; Campisi, C.; Cozzani, E.; Parodi, A. Dermatological consultations in an observation unit of an emergency department in Italy. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 973–980. [Google Scholar] [CrossRef] [PubMed]
- Jack, A.R.; Spence, A.A.; Nichols, B.J.; Chong, S.; Williams, D.T.; Swadron, S.P.; Peng, D.H. Cutaneous conditions leading to dermatology consultations in the emergency department. West. J. Emerg. Med. 2011, 12, 551–555. [Google Scholar] [CrossRef] [Green Version]
- Gupta, S.; Sandhu, K.; Kumar, B. Evaluation of emergency dermatological consultations in a tertiary care centre in North India. J. Eur. Acad. Dermatol. Venereol. 2003, 17, 303–305. [Google Scholar] [CrossRef]
- Murr, D.; Bocquet, H.; Bachot, N.; Bagot, M.; Revuz, J.; Roujeau, J.C. Medical activity in an emergency outpatient department dermatology. Ann. Dermatol. Venereol. 2003, 130, 167–170. [Google Scholar]
- Tun, K.; Shurko, J.F.; Ryan, L.; Lee, G.C. Age-based health and economic burden of skin and soft tissue infections in the United States, 2000 and 2012. PLoS ONE 2018, 13, e0206893. [Google Scholar] [CrossRef]
- Kaye, K.S.; Petty, L.A.; Shorr, A.F.; Zilberberg, M.D. Current Epidemiology, Etiology, and Burden of Acute Skin Infections in the United States. Clin. Infect. Dis. 2019, 68, S193–S199. [Google Scholar] [CrossRef] [Green Version]
- Kawai, K.; Gebremeskel, B.G.; Acosta, C.J. Systematic review of incidence and complications of herpes zoster: Towards a global perspective. BMJ Open 2014, 4, e004833. [Google Scholar] [CrossRef] [Green Version]
- Kawai, K.; Yawn, B.P.; Wollan, P.; Harpaz, R. Increasing Incidence of Herpes Zoster Over a 60-year Period from a Population-based Study. Clin. Infect. Dis. 2016, 63, 221–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmader, K. Herpes zoster in older adults. Clin. Infect. Dis. 2001, 32, 1481–1486. [Google Scholar] [PubMed]
- Goodyear, H.M.; Laidler, P.W.; Price, E.H.; Kenny, P.A.; Harper, J.I. Acute infectious erythemas in children: A clinico-microbiological study. Br. J. Dermatol. 1991, 124, 433–438. [Google Scholar] [PubMed]
- Drago, F.; Rampini, P.; Rampini, E.; Rebora, A. Atypical exanthems: Morphology and laboratory investigations may lead to an aetiological diagnosis in about 70% of cases. Br. J. Dermatol. 2002, 147, 255–260. [Google Scholar] [CrossRef]
- Tabak, F.; Murtezaoglu, A.; Tabak, O.; Ozaras, R.; Mete, B.; Kutlubay, Z.; Mert, A.; Ozturk, R. Clinical Features and Etiology of Adult Patients with Fever and Rash. Ann. Dermatol. 2012, 24, 420–425. [Google Scholar] [CrossRef] [Green Version]
- Onsoi, W.; Chaiyarit, J.; Techasatian, L. Common misdiagnoses and prevalence of dermatological disorders at a pediatric tertiary care center. J. Int. Med. Res. 2020, 48, 300060519873490. [Google Scholar] [CrossRef] [Green Version]
- Zhang, H.; Tang, K.; Fang, R.; Jin, H.; Sun, Q. Inpatient Dermatology Consultations in a General Surgery Ward in a Tertiary Hospital in China: A Retrospective Study of 251 Patients. Dermatol Ther. 2021, 11, 961–970. [Google Scholar] [CrossRef]
- Maron, R.C.; Utikal, J.S.; Hekler, A.; Hauschild, A.; Sattler, E.; Sondermann, W.; Haferkamp, S.; Schilling, B.; Heppt, M.V.; Jansen, P.; et al. Artificial Intelligence and Its Effect on Dermatologists’ Accuracy in Dermoscopic Melanoma Image Classification: Web-Based Survey Study. J. Med. Internet Res. 2020, 22, e18091. [Google Scholar] [CrossRef]
- Dildar, M.; Akram, S.; Irfan, M.; Khan, H.U.; Ramzan, M.; Mahmood, A.R.; Alsaiari, S.A.; Saeed, A.H.M.; Alraddadi, M.O.; Mahnashi, M.H. Skin Cancer Detection: A Review Using Deep Learning Techniques. Int. J. Environ. Res. Public Health. 2021, 18, 5479. [Google Scholar] [CrossRef]
- Requena, L.; Requena, C. Erythema nodosum. Dermatol. Online J. 2002, 8, 4. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Bacterial diseases A25 Rat-bite fevers | B35.0 Tinea barbae and tinea capitis B35.1 Tinea unguium |
| A26 Erysipeloid | B35.3 Tinea pedis |
| A31.1 Cutaneous mycobacterial infection | B35.4 Tinea corporis |
| A32.0 Cutaneous listeriosis | B35.5 Tinea imbricata |
| A36.3 Cutaneous diphtheria | B35.6 Tinea inguinalis (Tinea cruris) |
| A39 Meningococcal infection | B35.8 Other dermatophytoses |
| A43.1 Cutaneous nocardiosis | B35.9 Dermatophytosis, unspecified |
| A44.1 Cutaneous and mucocutaneous bartonellosis | B36 Other superficial mycoses |
| A46 Erysipelas | B36.0 Pityriasis versicolor |
| A48.3 Toxic shock syndrome | B36.1 Tinea nigra |
| A51.3 Secondary syphilis of skin and mucous membranes | B36.2 White piedra |
| A69.2 Lyme disease | B36.3 Black piedra |
| A75 Typhus fever | B36.8 Other specified superficial mycoses |
| A77.1 Spotted fever due to Rickettsia conorii | B36.9 Superficial mycosis, unspecified |
| A79.1 Rickettsial pox due to Rickettsia akari | B37.2 Candidiasis of skin and nail |
| Viral diseases | B38.3 Cutaneous coccidioidomycosis |
| A88.0 Enteroviral exanthematous fever (Boston exanthem) | B40.3 Cutaneous blastomycosis |
| A91 Dengue hemorrhagic fever | B43.0 Cutaneous chromomycosis |
| A92.0 Chikungunya virus disease | B45.2 Cutaneous cryptococcosis |
| B00 Herpes viral (herpes simplex) infections | B46.3 Cutaneous mucormycosis |
| B01 Varicella (chickenpox) | Parasitic diseases |
| B02 Zoster (herpes zoster) | B55.1 Cutaneous leishmaniasis |
| B03 Smallpox | B55.2 Mucocutaneous leishmaniasis |
| B04 Monkeypox | B65.3 Cercarial dermatitis |
| B05 Measles | B72 Dracunculiasis |
| B06 Rubella | B74 Filariasis |
| B07 Viral warts | B78.1 Cutaneous strongyloidiasis |
| B08 Other viral infections characterized by skin and mucous membrane lesions, not elsewhere classified | B85 Pediculosis and phthiriasis |
| B08.0 Other orthopoxvirus infections | B86 Scabies |
| B08.1 Molluscum contagiosum | B88.0 Other acariasis |
| B08.2 Exanthema subitum (sixth disease) | Diseases caused by infectious agent |
| B08.3 Erythema infectiosum (fifth disease) | L00 Staphylococcal scalded skin syndrome |
| B08.4 Enteroviral vesicular stomatitis with exanthem | L01 Impetigo |
| B08.5 Enteroviral vesicular pharyngitis | L02 Cutaneous abscess, furuncle and carbuncle |
| B08.8 Other specified viral infections characterized by skin and mucous membrane lesions | L03 Cellulitis |
| B09 Unspecified viral infection characterized by skin and mucous membrane lesions | L08 Other local infections of skin and subcutaneous tissue |
| Fungal diseases | L30.3 Infective dermatitis |
| B35 Dermatophytosis | L44.4 Infantile papular acrodermatitis (Giannotti–Crosti) |
| L10 Pemphigus |
| L12 Pemphigoid |
| L13 Other bullous disorders |
| L20 Atopic dermatitis |
| L21 Seborrhoeic dermatitis |
| L22 Diaper [napkin] dermatitis |
| L23 Allergic contact dermatitis |
| L24 Irritant contact dermatitis |
| L25 Unspecified contact dermatitis |
| L26 Exfoliative dermatitis |
| L27 Dermatitis due to substances taken internally |
| L29 Pruritus |
| L30 Other dermatitis (except L30.3) |
| L40 Psoriasis |
| L41 Parapsoriasis |
| L42 Pityriasis rosea |
| L43 Lichen planus |
| L50 Urticaria |
| L51 Erythema multiforme |
| L52 Erythema nodosum |
| L53 Other erythematous conditions |
| L54 Erythema in diseases classified elsewhere |
| L55 Sunburn |
| L56 Other acute skin changes due to ultraviolet radiation |
| L70 Acne |
| L71 Rosacea |
| L73 Other follicular disorders |
| L84 Corns and callosities |
| L85 Other epidermal thickening |
| L88 Pyoderma gangrenosum |
| L89 Decubitus ulcer and pressure area |
| L90 Atrophic disorders of skin |
| L91 Hypertrophic disorders of skin |
| L92 Granulomatous disorders of skin and subcutaneous tissue |
| L93 Lupus erythematosus |
| L94 Other localized connective tissue disorders |
| L95 Vasculitis limited to skin, not elsewhere classified |
| L97 Ulcer of lower limb, not elsewhere classified |
| L98 Other disorders of skin and subcutaneous tissue, not elsewhere classified |
| R21 Rash and other nonspecific skin eruption |
| R22 Localized swelling, mass and lump of skin and subcutaneous tissue |
| Diagnosis | n | Age (Years) | Men | Hospital Stay (Days) |
|---|---|---|---|---|
| All | 2287 | 59 (34–74; <1–101) | 1119 (48.9) | 8 (6–11; 1–119) |
| All infectious | 2228 | 59 (34–74; <1–101) | 1097 (49.2) | 8 (6–11; 1–119) |
| All non-infectious | 59 | 44 (15–60; <1–90) | 22 (37.3) | 8 (5–14; 1–40) |
| Cellulitis | 776 | 66 (51–76; <1–101) | 355 (45.8) | 9 (7–12; 1–33) |
| Erysipelas | 620 | 64 (54–75; 2–94) | 316 (51.0) | 8 (6–10; 1–44) |
| Herpes zoster | 287 | 73 (58–79; 8–97) | 135 (47.0) | 8 (6–11; 2–60) |
| Chickenpox | 177 | 6 (2–28; <1–69) | 100 (56.5) | 5 (3–7; 1–23) |
| Meningococcal infection | 61 | 2 (<1–15; <1–69) | 31 (50.8) | 10 (8–13; 1–49) |
| Erythema multiforme/nodosum | 24 | 44 (29–55; 8–72) | 9 (37.5) | 8 (5–12; 3–22) |
| Authors | Year of Publication | No. of Patients | Characteristics of Patients | Inclusion Criteria | Undiagnosed |
|---|---|---|---|---|---|
| Goodyear HM, Laidler PW, Price EH, Kenny PA, Harper JI | 1991 | 100 | Children | Acute erythematous rash and a febrile illness of short duration Patients with recognizable rashes were excluded | n= 35, 35% |
| Drago F, Rampini P, Rampini E, Rebora A | 2002 | 112 | Children and adults | Rash other than classical exanthems | n = 36, 32% |
| Tabak F, Murtezaoglu A, Tabak O, Ozaras R, Mete B, Kutlubay Z, Mert A, Ozturk R | 2012 | 100 | Adults | Rash and fever | n = 10, 10% |
| Drago F, Paolino S, Rebora A, Broccolo F, Drago F, Cardo P, Parodi A | 2012 | 260 | Children and adults | Atypical exanthems other than classical exanthems | n = 59, 23% |
| Skuhala T, Trkulja V, Rimac M, Dragobratović A, Desnica B | 21,114 | Children and adults | All types of skin lesions | n= 4478, 21.1% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Skuhala, T.; Trkulja, V.; Rimac, M.; Dragobratović, A.; Desnica, B. Analysis of Types of Skin Lesions and Diseases in Everyday Infectious Disease Practice—How Experienced Are We? Life 2022, 12, 978. https://doi.org/10.3390/life12070978
Skuhala T, Trkulja V, Rimac M, Dragobratović A, Desnica B. Analysis of Types of Skin Lesions and Diseases in Everyday Infectious Disease Practice—How Experienced Are We? Life. 2022; 12(7):978. https://doi.org/10.3390/life12070978
Chicago/Turabian StyleSkuhala, Tomislava, Vladimir Trkulja, Marin Rimac, Anja Dragobratović, and Boško Desnica. 2022. "Analysis of Types of Skin Lesions and Diseases in Everyday Infectious Disease Practice—How Experienced Are We?" Life 12, no. 7: 978. https://doi.org/10.3390/life12070978