
Utility of Keratins as Biomarkers for Human Oral Precancer and Cancer


{kind=link}
Abstract
:1. Classification of Oral Tumors
2. Development of Oral Precancerous Lesions and Oral Tumors
3. Biological Markers
4. Keratins
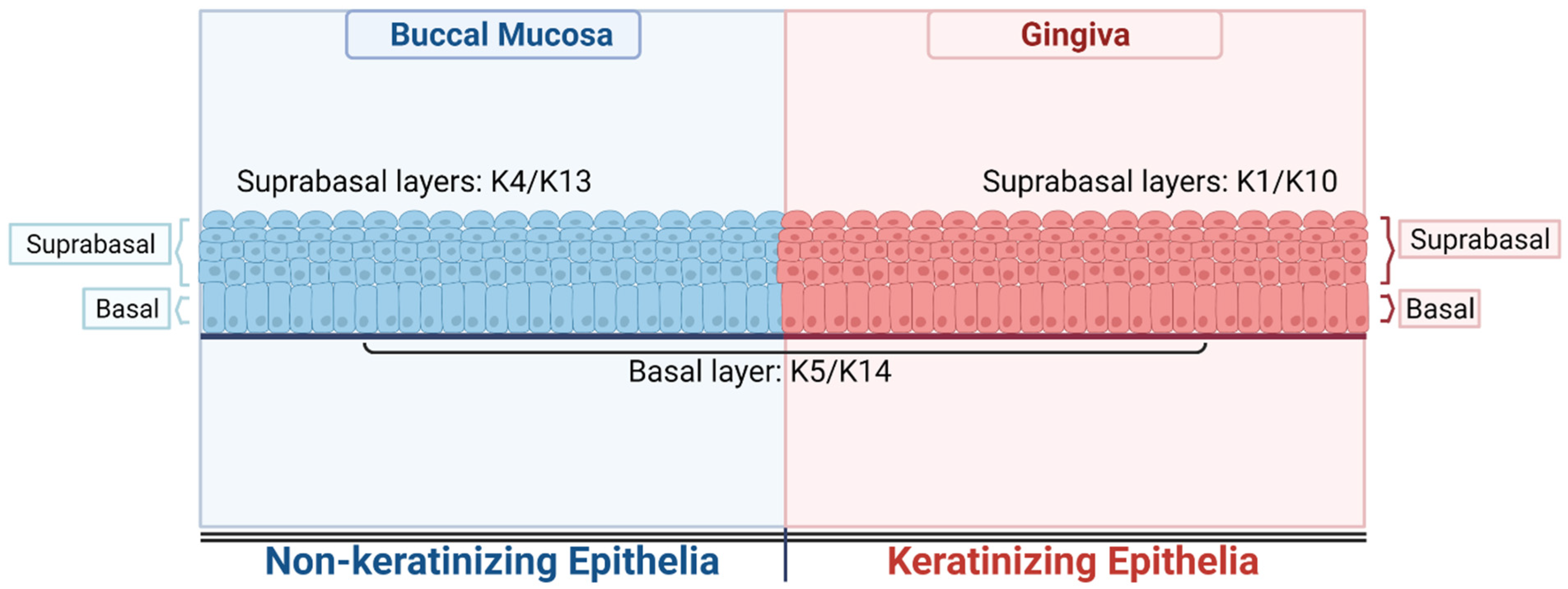
5. Keratin Expression in Normal Human Oral Cavities
6. Detection of Keratins
6.1. Transcription
6.2. Proteomics
6.3. Immunohistochemistry
7. Aberrant Keratin Expression in Oral Precancerous Lesions
8. Aberrant Expression of Keratins in OSCC
9. Correlation of Keratin Expression with Clinicopathological Parameters
10. Functional Significance of Aberrant Keratin 8/18 Expression in Oral Precancer and Cancer
11. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hillbertz, N.S.; Hirsch, J.A.N.M.; Jalouli, J.; Jalouli, M.M.; Sand, L. Viral and Molecular Aspects of Oral Cancer. Anticancer Res. 2012, 32, 4201. [Google Scholar] [PubMed]
- Sobin, L.H.; Gospodarowicz, M.K.; Wittekind, C.; Internation Union Against Cancer. TNM Classification of Malignant Tumours, 7th ed.; Sobin, L.H., Gospodarowicz, M.K., Wittekind, C., Eds.; Wiley-Blackwell: Hoboken, NJ, USA, 2009. [Google Scholar]
- Leemans, C.R.; Braakhuis, B.J.M.; Brakenhoff, R.H. The molecular biology of head and neck cancer. Nat. Rev. Cancer 2011, 11, 9–22. [Google Scholar] [CrossRef] [PubMed]
- Massano, J.; Regateiro, F.S.; Januário, G.; Ferreira, A. Oral squamous cell carcinoma: Review of prognostic and predictive factors. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontol. 2006, 102, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Lippman, S.M.; Hong, W.K. Molecular Markers of the Risk of Oral Cancer. N. Engl. J. Med. 2001, 344, 1323–1326. [Google Scholar] [CrossRef] [PubMed]
- Reibel, J. Prognosis of Oral Pre-malignant Lesions: Significance of Clinical, Histopathological, and Molecular Biological Characteristics. Crit. Rev. Oral Biol. Med. 2003, 14, 47–62. [Google Scholar] [CrossRef]
- Gupta, P.; Bhonsle, R.; Murti, P.; Daftary, D.; Mehta, F.; Pindborg, J. An Epidemiologic Assessment of Cancer Risk in Oral Precancerous Lesions in India With Special Reference to Nodular Leukoplakia. Cancer 1989, 63, 2247–2252. [Google Scholar] [CrossRef]
- Allison, P.; Locker, D.; Feine, J.S. The role of diagnostic delays in the prognosis of oral cancer: A review of the literature. Oral Oncol. 1998, 34, 161–170. [Google Scholar] [CrossRef]
- Cerezo, L.; Millan, I.; Torre, A.; Aragon, G.; Otero, J. Prognostic factors for survival and tumor control in cervical lymph node metastases from head and neck cancer. A multivariate study of 492 cases. Cancer 1992, 69, 1224–1234. [Google Scholar] [CrossRef]
- Jemal, A.; Tiwari, R.C.; Murray, T.; Ghafoor, A.; Samuels, A.; Ward, E.; Feuer, E.J.; Thun, M.J. Cancer statistics, 2004. CA Cancer J. Clin. 2004, 54, 8–29. [Google Scholar] [CrossRef]
- Bloor, B.; Seddon, S.; Morgan, P. Gene expression of differentiation-specific keratins in oral epithelial dysplasia and squamous cell carcinoma. Oral Oncol. 2001, 37, 251–261. [Google Scholar] [CrossRef]
- Fillies, T.; Jogschies, M.; Kleinheinz, J.; Brandt, B.; Joos, U.; Buerger, H. Cytokeratin alteration in oral leukoplakia and oral squamous cell carcinoma. Oncol. Rep. 2007, 18, 639–643. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coulombe, P.A.; Omary, M.B. ‘Hard’ and ‘soft’ principles defining the structure, function and regulation of keratin intermediate filaments. Curr. Opin. Cell Biol. 2002, 14, 110–122. [Google Scholar] [CrossRef]
- Pekny, M.; Lane, E. Intermediate filaments and stress. Exp. Cell Res. 2007, 313, 2244–2254. [Google Scholar] [CrossRef] [PubMed]
- Moll, R.; Franke, W.W.; Schiller, D.L.; Geiger, B.; Krepler, R. The catalog of human cytokeratins: Patterns of expression in normal epithelia, tumors and cultured cells. Cell 1982, 31, 11–24. [Google Scholar] [CrossRef]
- Takahashi, K.; Paladini, R.D.; Coulombe, P.A. Cloning and Characterization of Multiple Human Genes and cDNAs Encoding Highly Related Type II Keratin 6 Isoforms *. J. Biol. Chem. 1995, 270, 18581–18592. [Google Scholar] [CrossRef] [Green Version]
- Moll, R.; Schiller, D.L.; Franke, W.W. Identification of protein IT of the intestinal cytoskeleton as a novel type I cytokeratin with unusual properties and expression patterns. J. Cell Biol. 1990, 111, 567–580. [Google Scholar] [CrossRef]
- Schweizer, J.; Bowden, P.E.; Coulombe, P.A.; Langbein, L.; Lane, E.B.; Magin, T.M.; Maltais, L.; Omary, M.B.; Parry, D.A.D.; Rogers, M.A.; et al. New consensus nomenclature for mammalian keratins. J. Cell Biol. 2006, 174, 169–174. [Google Scholar] [CrossRef] [Green Version]
- Morgan, P.R.; Shirlaw, P.J.; Johnson, N.W.; Leigh, I.M.; Lane, E.B. Potential applications of anti-keratin antibodies in oral diagnosis. J. Oral Pathol. 1987, 16, 212–222. [Google Scholar] [CrossRef]
- Moll, R.; Divo, M.; Langbein, L. The human keratins: Biology and pathology. Histochem. Cell Biol. 2008, 129, 705–733. [Google Scholar] [CrossRef] [Green Version]
- Lane, E.B.; McLean, W.H. Keratins and skin disorders. J. Pathol. 2004, 204, 355–366. [Google Scholar] [CrossRef]
- Omary, M.B.; Coulombe, P.A.; McLean, W.H. Intermediate filament proteins and their associated diseases. N. Engl. J. Med. 2004, 351, 2087–2100. [Google Scholar] [CrossRef] [PubMed]
- Moll, R.; Krepler, R.; Franke, W.W. Complex cytokeratin polypeptide patterns observed in certain human carcinomas. Differ. Res. Biol. Divers. 1983, 23, 256–269. [Google Scholar] [CrossRef]
- Moll, R. Diversity of cytokeratins in carcinomas. Acta Histochem. 1987, 34, 37–44. [Google Scholar]
- Osborn, M.; van Lessen, G.; Weber, K.; Kloppel, G.; Altmannsberger, M. Differential diagnosis of gastrointestinal carcinomas by using monoclonal antibodies specific for individual keratin polypeptides. Lab. Investig. A J. Tech. Methods Pathol. 1986, 55, 497–504. [Google Scholar]
- Lazarides, E. Intermediate filaments as mechanical integrators of cellular space. Nature 1980, 283, 249–256. [Google Scholar] [CrossRef]
- Osborn, M.; Weber, K. Intermediate filaments: Cell-type-specific markers in differentiation and pathology. Cell 1982, 31, 303–306. [Google Scholar] [CrossRef]
- Blobel, G.A.; Moll, R.; Franke, W.W.; Kayser, K.W.; Gould, V.E. The intermediate filament cytoskeleton of malignant mesotheliomas and its diagnostic significance. Am. J. Pathol. 1985, 121, 235–247. [Google Scholar]
- Lindberg, K.; Rheinwald, J.G. Suprabasal 40 kd keratin (K19) expression as an immunohistologic marker of premalignancy in oral epithelium. Am. J. Pathol. 1989, 134, 89–98. [Google Scholar]
- Vigneshwaran, N.; Peters, K.-P.; Hornstein, O.P.; Haneke, E. Comparison of cytokeratin, filaggrin and involucrin profiles in oral leukoplakias and squamous carcinomas. J. Oral Pathol. Med. 1989, 18, 377–390. [Google Scholar] [CrossRef]
- Bosch, F.X.; Ouhayoun, J.P.; Bader, B.L.; Collin, C.; Grund, C.; Lee, I.; Franke, W.W. Extensive changes in cytokeratin expression patterns in pathologically affected human gingiva. Virchows Arch. 1989, 58, 59–77. [Google Scholar] [CrossRef]
- Heyden, A.; Huitfeldt, H.S.; Koppang, H.S.; Thrane, P.S.; Bryne, M.; Brandtzaeg, P. Cytokeratins as epithelial differentiation markers in premalignant and malignant oral lesions. J. Oral Pathol. Med. 1992, 21, 7–11. [Google Scholar] [CrossRef] [PubMed]
- Coulombe, P.A. The cellular and molecular biology of keratins: Beginning a new era. Curr. Opin. Cell Biol. 1993, 5, 17–29. [Google Scholar] [CrossRef]
- Fuchs, E.; Weber, K. Intermediate filaments: Structure, dynamics, function, and disease. Annu. Rev. Biochem. 1994, 63, 345–382. [Google Scholar] [CrossRef] [PubMed]
- McDonald, L.A.; Walker, D.M.; Gibbins, J.R. Cervical lymph node involvement in head and neck cancer detectable as expression of a spliced transcript of type II keratin K5. Oral Oncol. 1998, 34, 276–283. [Google Scholar] [CrossRef]
- Ida-Yonemochi, H.; Maruyama, S.; Kobayashi, T.; Yamazaki, M.; Cheng, J.; Saku, T. Loss of keratin 13 in oral carcinoma in situ: A comparative study of protein and gene expression levels using paraffin sections. Mod. Pathol. 2012, 25, 784–794. [Google Scholar] [CrossRef] [Green Version]
- Su, L.; Morgan, P.R.; Lane, E.B. Protein and mRNA expression of simple epithelial keratins in normal, dysplastic, and malignant oral epithelia. Am. J. Pathol. 1994, 145, 1349–1357. [Google Scholar]
- Ermich, T.; Schulz, J.; Raabe, G.; Schumann, D. Pattern of oral cytokeratins. III. SDS-electrophoretic analysis and immunoblotting of cytokeratins in leukoplakias and squamous cell carcinomas of the oral mucosa. Biomed. Biochim. Acta 1989, 48, 393–401. [Google Scholar]
- Vaidya, M.M.; Borges, A.M.; Pradhan, S.A.; Rajpal, R.M.; Bhisey, A.N. Altered keratin expression in buccal mucosal squamous cell carcinoma. J. Oral Pathol. Med. Off. Publ. Int. Assoc. Oral Pathol. Am. Acad. Oral Pathol. 1989, 18, 282–286. [Google Scholar] [CrossRef]
- Vaidya, M.M.; Sawant, S.S.; Borges, A.M.; Ogale, S.B.; Bhisey, A.N. Cytokeratin expression in precancerous lesions of the human oral cavity. Oral Oncol. 1998, 34, 261–264. [Google Scholar] [CrossRef]
- Vaidya, M.M.; Borges, A.M.; Pradhan, S.A.; Bhisey, A.N. Cytokeratin expression in squamous cell carcinomas of the tongue and alveolar mucosa. Eur. J. Cancer B Oral Oncol. 1996, 32B, 333–336. [Google Scholar] [CrossRef]
- Gires, O.; Mack, B.; Rauch, J.; Matthias, C. CK8 correlates with malignancy in leukoplakia and carcinomas of the head and neck. Biochem. Biophys. Res. Commun. 2006, 343, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Roman, E.; Lunde, M.L.S.; Miron, T.; Warnakulasauriya, S.; Johannessen, A.C.; Vasstrand, E.N.; Ibrahim, S.O. Analysis of Protein Expression Profile of Oral Squamous Cell Carcinoma by MALDI-TOF-MS. Anticancer Res. 2013, 33, 837. [Google Scholar] [PubMed]
- Chiang, C.-H.; Wu, C.-C.; Lee, L.-Y.; Li, Y.-C.; Liu, H.-P.; Hsu, C.-W.; Lu, Y.-C.; Chang, J.T.; Cheng, A.-J. Proteomics Analysis Reveals Involvement of Krt17 in Areca Nut-Induced Oral Carcinogenesis. J. Proteome Res. 2016, 15, 2981–2997. [Google Scholar] [CrossRef]
- Ogden, G.R.; Lane, E.B.; Hopwood, D.V.; Chisholm, D.M. Evidence for field change in oral cancer based on cytokeratin expression. Br. J. Cancer 1993, 67, 1324–1330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bloor, B.K.; Seddon, S.V.; Morgan, P.R. Gene expression of differentiation-specific keratins (K4, K13, K1 and K10) in oral non-dysplastic keratoses and lichen planus. J. Oral Pathol. Med. Off. Publ. Int. Assoc. Oral Pathol. Am. Acad. Oral Pathol. 2000, 29, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Marley, J.J.; Robinson, P.A.; Hume, W.J. Expression of human cytokeratin 14 in normal, premalignant and malignant oral tissue following isolation by plaque differential hybridisation. Eur. J. Cancer Part B Oral Oncol. 1994, 30, 305–311. [Google Scholar] [CrossRef]
- Ranganathan, K.; Kavitha, R.; Sawant, S.S.; Vaidya, M.M. Cytokeratin expression in oral submucous fibrosis—An immunohistochemical study. J. Oral Pathol. Med. 2006, 35, 25–32. [Google Scholar] [CrossRef]
- Schaaij-Visser, T.B.M.; Bremmer, J.F.; Braakhuis, B.J.M.; Heck, A.J.R.; Slijper, M.; van der Waal, I.; Brakenhoff, R.H. Evaluation of cornulin, keratin 4, keratin 13 expression and grade of dysplasia for predicting malignant progression of oral leukoplakia. Oral Oncol. 2010, 46, 123–127. [Google Scholar] [CrossRef]
- Mikami, T.; Cheng, J.; Maruyama, S.; Kobayashi, T.; Funayama, A.; Yamazaki, M.; Adeola, H.A.; Wu, L.; Shingaki, S.; Saito, C.; et al. Emergence of keratin 17 vs. loss of keratin 13: Their reciprocal immunohistochemical profiles in oral carcinoma in situ. Oral Oncol. 2011, 47, 497–503. [Google Scholar] [CrossRef]
- Lalli, A.; Tilakaratne, W.; Ariyawardana, A.; Fitchett, C.; Leigh, I.; Hagi-Pavli, E.; Cruchley, A.; Kenneth, E.; Teh, M.-T.; Fortune, F.; et al. An altered keratinocyte phenotype in oral submucous fibrosis: Correlation of keratin K17 expression with disease severity. J. Oral Pathol. Med. Off. Publ. Int. Assoc. Oral Pathol. Am. Acad. Oral Pathol. 2008, 37, 211–220. [Google Scholar] [CrossRef]
- Sakamoto, K.; Aragaki, T.; Morita, K.; Kawachi, H.; Kayamori, K.; Nakanishi, S.; Omura, K.; Miki, Y.; Okada, N.; Katsube, K.; et al. Down-regulation of keratin 4 and keratin 13 expression in oral squamous cell carcinoma and epithelial dysplasia: A clue for histopathogenesis. Histopathology 2011, 58, 531–542. [Google Scholar] [CrossRef] [PubMed]
- Farrar, M.; Sandison, A.; Peston, D.; Gailani, M. Immunocytochemical analysis of AE1/AE3, CK 14, Ki-67 and p53 expression in benign, premalignant and malignant oral tissue to establish putative markers for progression of oral carcinoma. Br. J. Biomed. Sci. 2004, 61, 117–124. [Google Scholar] [CrossRef]
- Morifuji, M.; Taniguchi, S.; Sakai, H.; Nakabeppu, Y.; Ohishi, M. Differential expression of cytokeratin after orthotopic implantation of newly established human tongue cancer cell lines of defined metastatic ability. Am. J. Pathol. 2000, 156, 1317–1326. [Google Scholar] [CrossRef] [Green Version]
- Wei, K.J.; Zhang, L.; Yang, X.; Zhong, L.P.; Zhou, X.J.; Pan, H.Y.; Li, J.; Chen, W.-R.; Zhang, Z.Y. Overexpression of cytokeratin 17 protein in oral squamous cell carcinoma in vitro and in vivo. Oral Dis. 2009, 15, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Dmello, C.; Sawant, S.; Alam, H.; Gangadaran, P.; Mogre, S.; Tiwari, R.; D’Souza, Z.; Narkar, M.; Thorat, R.; Patil, K.J.P.O. Vimentin regulates differentiation switch via modulation of keratin 14 levels and their expression together correlates with poor prognosis in oral cancer patients. PLoS ONE 2017, 12, e0172559. [Google Scholar]
- Mogre, S.; Makani, V.; Pradhan, S.; Devre, P.; More, S.; Vaidya, M.; Dmello, C. Biomarker Potential of Vimentin in Oral Cancers. Life 2022, 12, 150. [Google Scholar] [CrossRef]
- Schulz, J.; Ermich, T.; Kasper, M.; Raabe, G.; Schumann, D. Cytokeratin pattern of clinically intact and pathologically changed oral mucosa. Int. J. Oral Maxillofac. Surg. 1992, 21, 35–39. [Google Scholar] [CrossRef]
- Ogden, G.R.; Chisholm, D.M.; Adi, M.; Lane, E.B. Cytokeratin expression in oral cancer and its relationship to tumor differentiation. J. Oral Pathol. Med. Off. Publ. Int. Assoc. Oral Pathol. Am. Acad. Oral Pathol. 1993, 22, 82–86. [Google Scholar] [CrossRef]
- Xu, X.C.; Lee, J.S.; Lippman, S.M.; Ro, J.Y.; Hong, W.K.; Lotan, R. Increased expression of cytokeratins CK8 and CK19 is associated with head and neck carcinogenesis. Cancer Epidemiol. Biomark. Prev. 1995, 4, 871. [Google Scholar]
- Zhong, L.-P.; Chen, W.-T.; Zhang, C.-P.; Zhang, Z.-Y. Increased CK19 expression correlated with pathologic differentiation grade and prognosis in oral squamous cell carcinoma patients. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2007, 104, 377–384. [Google Scholar] [CrossRef]
- Cintorino, M.; Petracca, R.; Vindigni, C.; Tripodi, S.A.; Leoncini, P. Topography-related expression of individual cytokeratins in normal and pathological (non-neoplastic and neoplastic) human oral mucosa. Virchows Arch. A 1990, 417, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Jiang, W.G.; Watkins, G.; Douglas-Jones, A.; Holmgren, L.; Mansel, R.E. Angiomotin and angiomotin like proteins, their expression and correlation with angiogenesis and clinical outcome in human breast cancer. BMC Cancer 2006, 6, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthias, C.; Mack, B.; Berghaus, A.; Gires, O. Keratin 8 expression in head and neck epithelia. BMC Cancer 2008, 8, 267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crowe, D.L.; Milo, G.E.; Shuler, C.E. Keratin 19 Downregulation by Oral Squamous Cell Carcinoma Lines Increases Invasive Potential. J. Dent. Res. 1999, 78, 1256–1263. [Google Scholar] [CrossRef]
- Depondt, J.; Shabana, A.H.; Sawaf, H.; Gehanno, P.; Forest, N. Cytokeratin alterations as diagnostic and prognostic markers of oral and pharyngeal carcinomas. A prospective study. Eur. J. Oral Sci. 1999, 107, 442–454. [Google Scholar] [CrossRef]
- Schaafsma, H.E.; Van Der Velden, L.A.; Manni, J.J.; Peters, H.; Link, M.; Rutter, D.J.; Ramaekers, F.C. Increased expression of cytokeratins 8, 18 and vimentin in the invasion front of mucosal squamous cell carcinoma. J. Pathol. 1993, 170, 77–86. [Google Scholar] [CrossRef]
- Fillies, T.; Werkmeister, R.; Packeisen, J.; Brandt, B.; Morin, P.; Weingart, D.; Joos, U.; Buerger, H. Cytokeratin 8/18 expression indicates a poor prognosis in squamous cell carcinomas of the oral cavity. BMC Cancer 2006, 6, 10. [Google Scholar] [CrossRef] [Green Version]
- Dmello, C.; Sawant, S.; Chaudhari, P.R.; Dongre, H.; Ahire, C.; D’Souza, Z.C.; Charles, S.E.; Rane, P.; Costea, D.E.; Chaukar, D.J.E.; et al. Aberrant expression of vimentin predisposes oral premalignant lesion derived cells towards transformation. Exp. Mol. Pathol. 2018, 105, 243–251. [Google Scholar] [CrossRef]
- Sawant, S.; Vaidya, M.; Chaukar, D.; Alam, H.; Dmello, C.; Gangadaran, P.; Kannan, S.; Kane, S.; Dange, P.; Dey, N.; et al. Clinical significance of aberrant vimentin expression in oral premalignant lesions and carcinomas. Oral Dis. 2014, 20, 453–465. [Google Scholar] [CrossRef]
- Dmello, C.; Srivastava, S.S.; Tiwari, R.; Chaudhari, P.R.; Sawant, S.; Vaidya, M.M. Multifaceted role of keratins in epithelial cell differentiation and transformation. J. Biosci. 2019, 44, 33. [Google Scholar] [CrossRef]
- Kitamura, R.; Toyoshima, T.; Tanaka, H.; Kawano, S.; Kiyosue, T.; Matsubara, R.; Goto, Y.; Hirano, M.; Oobu, K.; Nakamura, S. Association of cytokeratin 17 expression with differentiation in oral squamous cell carcinoma. J. Cancer Res. Clin. Oncol. 2012, 138, 1299–1310. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawant, S.; Vaidya, M.; Chaukar, D.; Gangadaran, P.; Singh, A.; Rajadhyax, S.; Kannan, S.; Kane, S.; Pagare, S.; Ranganathan, K.; et al. Clinicopathological features and prognostic implications of loss of K5 and gain of K1, K8 and K18 in oral potentially malignant lesions and squamous cell carcinomas: Immunohistochemical analysis. Tumor Biol. 2014, 1, 1–22. [Google Scholar]
- Garrel, R.; Dromard, M.; Costes, V.; Barbotte, E.; Comte, F.; Gardiner, Q.; Cartier, C.; Makeieff, M.; Crampette, L.; Guerrier, B.; et al. The Diagnostic Accuracy of Reverse Transcription-PCR Quantification of Cytokeratin mRNA in the Detection of Sentinel Lymph Node Invasion in Oral and Oropharyngeal Squamous Cell Carcinoma: A Comparison with Immunohistochemistry. Clin. Cancer Res. 2006, 12, 2498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chisholm, J.C.; Houliston, E. Cytokeratin filament assembly in the preimplantation mouse embryo. Development 1987, 101, 565–582. [Google Scholar] [CrossRef]
- Oshima, R.G.; Baribault, H.; Caulín, C. Oncogenic regulation and function of keratins 8 and 18. Cancer Metastasis Rev. 1996, 15, 445–471. [Google Scholar] [CrossRef]
- Bauman, P.A.; Dalton, W.S.; Anderson, J.M.; Cress, A.E. Expression of cytokeratin confers multiple drug resistance. Proc. Natl. Acad. Sci. USA 1994, 91, 5311. [Google Scholar] [CrossRef] [Green Version]
- Chu, Y.W.; Seftor, E.A.; Romer, L.H.; Hendrix, M.J. Experimental coexpression of vimentin and keratin intermediate filaments in human melanoma cells augments motility. Am. J. Pathol. 1996, 148, 63–69. [Google Scholar]
- Hendrix, M.J.; Seftor, E.A.; Chu, Y.W.; Seftor, R.E.; Nagle, R.B.; McDaniel, K.M.; Leong, S.P.; Yohem, K.H.; Leibovitz, A.M.; Meyskens, F.L., Jr. Coexpression of vimentin and keratins by human melanoma tumor cells: Correlation with invasive and metastatic potential. J. Natl. Cancer Inst. 1992, 84, 165–174. [Google Scholar] [CrossRef] [Green Version]
- Chu, Y.W.; Runyan, R.B.; Oshima, R.G.; Hendrix, M.J. Expression of complete keratin filaments in mouse L cells augments cell migration and invasion. Proc. Natl. Acad. Sci. USA 1993, 90, 4261–4265. [Google Scholar] [CrossRef] [Green Version]
- Raul, U.; Sawant, S.; Dange, P.; Kalraiya, R.; Ingle, A.; Vaidya, M. Implications of Cytokeratin 8/18 filament formation in stratified epithelial cells: Induction of transformed phenotype. Int. J. Cancer 2004, 111, 662–668. [Google Scholar] [CrossRef]
- Casanova, M.L.; Bravo del Moral, A.; Martinez-Palacio, J.; Fernández-Aceñero, M.J.; Villanueva, C.; Larcher, F.; Conti, C.; Jorcano, J. Epidermal abnormalities and increased malignancy of skin tumors in human epidermal keratin 8-expressing transgenic mice. FASEB J. Off. Publ. Fed. Am. Soc. Exp. Biol. 2004, 18, 1556–1558. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bordeleau, F.; Galarneau, L.; Gilbert, S.; Loranger, A.; Marceau, N. Keratin 8/18 modulation of protein kinase C-mediated integrin-dependent adhesion and migration of liver epithelial cells. Mol. Biol. Cell 2010, 21, 1698–1713. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaudhari, P.R.; Vaidya, M.M. Versatile hemidesmosomal linker proteins: Structure and function. Histol. Histopathol. 2015, 30, 425–434. [Google Scholar] [CrossRef] [PubMed]
- Geerts, D.; Fontao, L.; Nievers, M.G.; Schaapveld, R.Q.; Purkis, P.E.; Wheeler, G.N.; Lane, E.B.; Leigh, I.M.; Sonnenberg, A. Binding of integrin alpha6beta4 to plectin prevents plectin association with F-actin but does not interfere with intermediate filament binding. J. Cell Biol. 1999, 147, 417–434. [Google Scholar] [CrossRef] [Green Version]
- Dmello, C.; Sawant, S.; Alam, H.; Gangadaran, P.; Tiwari, R.; Dongre, H.; Rana, N.; Barve, S.; Costea, D.E.; Chaukar, D.; et al. Vimentin-mediated regulation of cell motility through modulation of beta4 integrin protein levels in oral tumor derived cells. Int. J. Biochem. Cell Biol. 2016, 70, 161–172. [Google Scholar] [CrossRef]
- Alam, H.; Kundu, S.T.; Dalal, S.N.; Vaidya, M.M. Loss of keratins 8 and 18 leads to alterations in α6β4-integrin-mediated signalling and decreased neoplastic progression in an oral-tumour-derived cell line. J. Cell Sci. 2011, 124, 2096–2106. [Google Scholar] [CrossRef] [Green Version]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vaidya, M.; Dmello, C.; Mogre, S. Utility of Keratins as Biomarkers for Human Oral Precancer and Cancer. Life 2022, 12, 343. https://doi.org/10.3390/life12030343
Vaidya M, Dmello C, Mogre S. Utility of Keratins as Biomarkers for Human Oral Precancer and Cancer. Life. 2022; 12(3):343. https://doi.org/10.3390/life12030343
Chicago/Turabian StyleVaidya, Milind, Crismita Dmello, and Saie Mogre. 2022. "Utility of Keratins as Biomarkers for Human Oral Precancer and Cancer" Life 12, no. 3: 343. https://doi.org/10.3390/life12030343