
SARS-CoV-2 Infection in Patients with Cystic Fibrosis: What We Know So Far
{kind=link}
{kind=link}
Abstract
:1. Introduction
Cystic Fibrosis Lung Disease
2. Methods
2.1. The Complexity of SARS-CoV-2 Infection
2.1.1. SARS-CoV-2 Origin and Classification
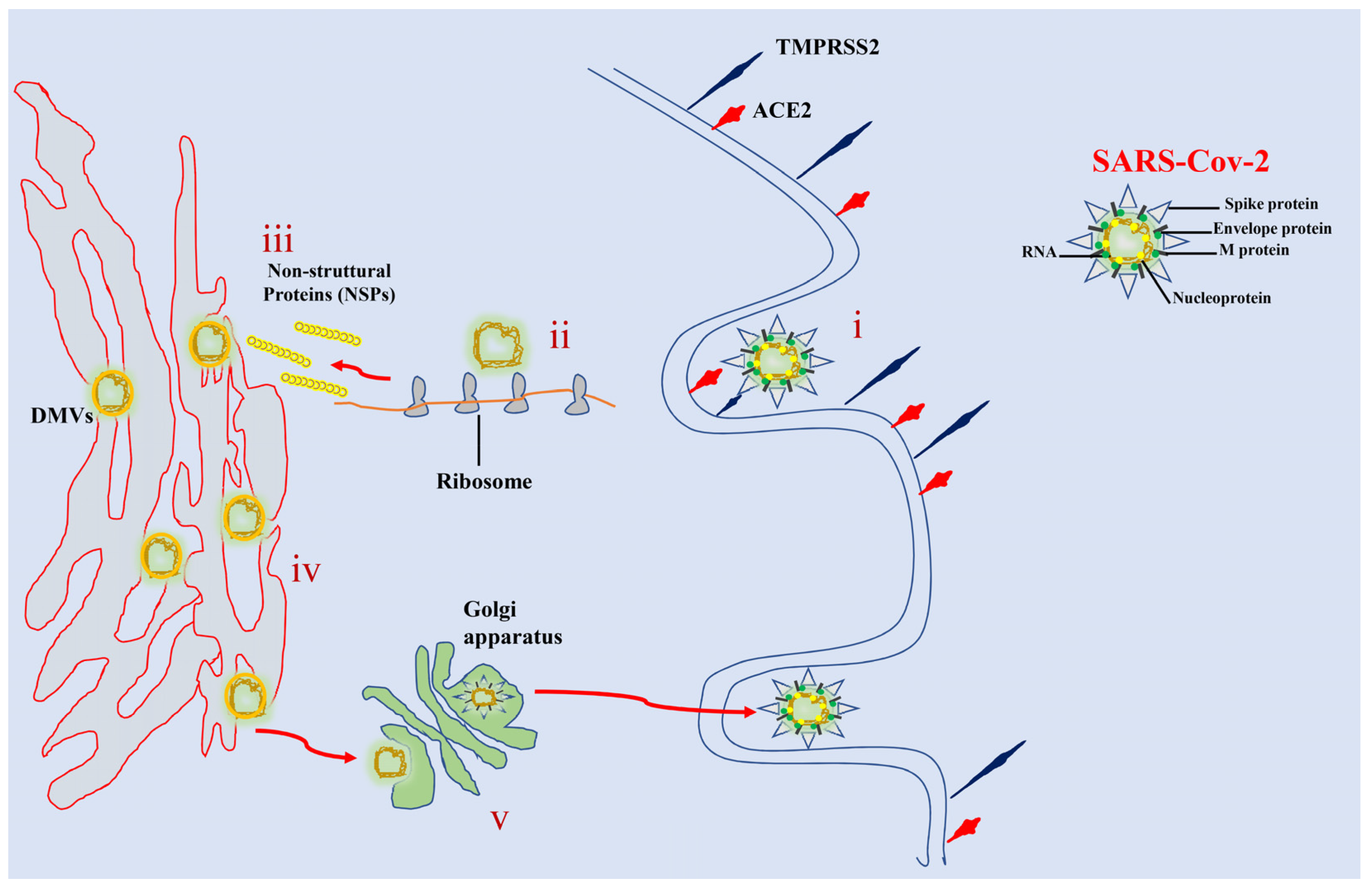
2.1.2. SARS-CoV-2 Morphology and Replication
2.1.3. SARS-CoV-2 Infection
2.2. Viral Respiratory Infections in Cystic Fibrosis
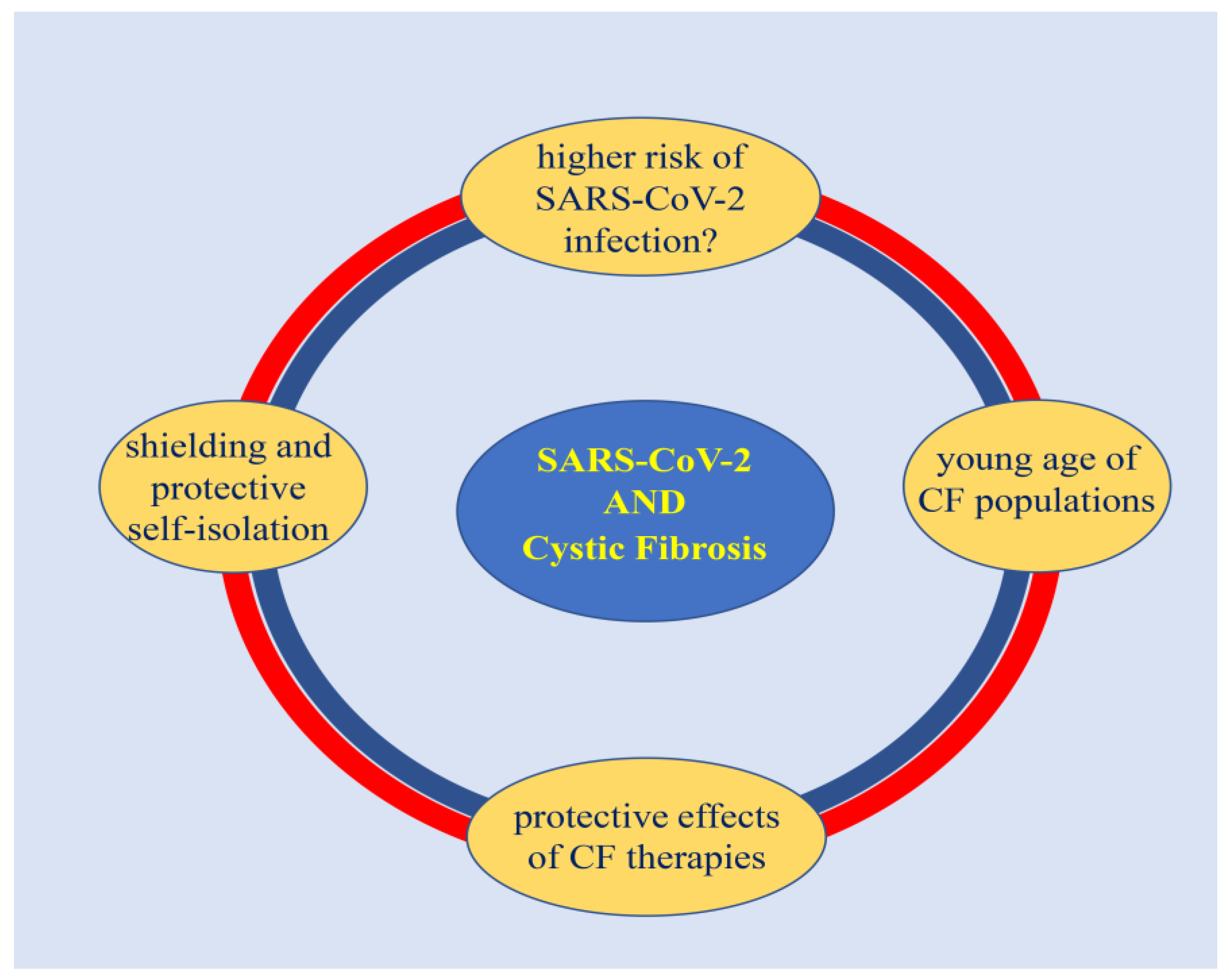
SARS-CoV-2 Infection in Cystic Fibrosis
3. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ye, Z.W.; Yuan, S.; Yuen, K.S.; Fung, S.Y.; Chan, C.P.; Jin, D.Y. Zoonotic origins of human coronaviruses. Int. J. Biol. Sci. 2020, 16, 1686–1697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef]
- International Committee on Taxonomy of Viruses Executive Committee. The new scope of virus taxonomy: Partitioning the virosphere into 15 hierarchical ranks. Nat. Microbiol. 2020, 5, 668–674. [Google Scholar] [CrossRef] [PubMed]
- Chan, J.F.; Yuan, S.; Kok, K.H.; To, K.K.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.; Poon, R.W.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ji, W.; Li, X. Response to comments on “Cross-species Transmission of the Newly Identified Coronavirus 2019-nCoV” and “Codon bias analysis may be insufficient for identifying host(s) of a novel virus”. J. Med. Virol. 2020, 92, 1440. [Google Scholar] [CrossRef]
- Ji, W.; Wang, W.; Zhao, X.; Zai, J.; Li, X. Cross-species transmission of the newly identified coronavirus 2019-nCoV. J. Med. Virol. 2020, 92, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Qian, J.; Feng, Y.; Li, J. Comments on “Cross-species transmission of the newly identified coronavirus 2019-nCoV”. J. Med. Virol. 2020, 92, 1437–1439. [Google Scholar] [CrossRef]
- Lu, R.; Zhao, X.; Li, J.; Niu, P.; Yang, B.; Wu, H.; Wang, W.; Song, H.; Huang, B.; Zhu, N.; et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. Lancet 2020, 395, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Kwok, K.O.; Wei, W.I.; Huang, Y.; Kam, K.M.; Chan, E.Y.Y.; Riley, S.; Chan, H.H.H.; Hui, D.S.C.; Wong, S.Y.S.; Yeoh, E.K. Evolving Epidemiological Characteristics of COVID-19 in Hong Kong From January to August 2020: Retrospective Study. J. Med. Internet Res. 2021, 23, e26645. [Google Scholar] [CrossRef]
- Jackson, C.B.; Farzan, M.; Chen, B.; Choe, H. Mechanisms of SARS-CoV-2 entry into cells. Nat. Rev. Mol. Cell Biol. 2022, 23, 3–20. [Google Scholar] [CrossRef]
- Fan, G.; Song, H.; Yip, S.; Zhang, T.; He, D. Impact of low vaccine coverage on the resurgence of COVID-19 in Central and Eastern Europe. One Health 2022, 14, 100402. [Google Scholar] [CrossRef] [PubMed]
- Milani, F. COVID-19 outbreak, social response, and early economic effects: A global VAR analysis of cross-country interdependencies. J. Popul. Econ. 2021, 34, 223–252. [Google Scholar] [CrossRef] [PubMed]
- Dyson, L.; Hill, E.M.; Moore, S.; Curran-Sebastian, J.; Tildesley, M.J.; Lythgoe, K.A.; House, T.; Pellis, L.; Keeling, M.J. Possible future waves of SARS-CoV-2 infection generated by variants of concern with a range of characteristics. Nat. Commun. 2021, 12, 5730. [Google Scholar] [CrossRef]
- Harvey, W.T.; Carabelli, A.M.; Jackson, B.; Gupta, R.K.; Thomson, E.C.; Harrison, E.M.; Ludden, C.; Reeve, R.; Rambaut, A.; Consortium, C.-G.U.; et al. SARS-CoV-2 variants, spike mutations and immune escape. Nat. Rev. Microbiol. 2021, 19, 409–424. [Google Scholar] [CrossRef]
- Alteri, C.; Cento, V.; Piralla, A.; Costabile, V.; Tallarita, M.; Colagrossi, L.; Renica, S.; Giardina, F.; Novazzi, F.; Gaiarsa, S.; et al. Genomic epidemiology of SARS-CoV-2 reveals multiple lineages and early spread of SARS-CoV-2 infections in Lombardy, Italy. Nat. Commun. 2021, 12, 434. [Google Scholar] [CrossRef] [PubMed]
- Gallo, L.G.; Oliveira, A.F.M.; Abrahao, A.A.; Sandoval, L.A.M.; Martins, Y.R.A.; Almiron, M.; Dos Santos, F.S.G.; Araujo, W.N.; de Oliveira, M.R.F.; Peixoto, H.M. Ten Epidemiological Parameters of COVID-19: Use of Rapid Literature Review to Inform Predictive Models During the Pandemic. Front. Public Health 2020, 8, 598547. [Google Scholar] [CrossRef]
- Giordano, G.; Blanchini, F.; Bruno, R.; Colaneri, P.; Di Filippo, A.; Di Matteo, A.; Colaneri, M. Modelling the COVID-19 epidemic and implementation of population-wide interventions in Italy. Nat. Med. 2020, 26, 855–860. [Google Scholar] [CrossRef]
- Block, J. Covid-19: US tracker overestimated deaths among children. BMJ 2022, 376, o831. [Google Scholar] [CrossRef]
- Ferec, C.; Scotet, V. Genetics of cystic fibrosis: Basics. Arch. De Pediatr. Organe Off. De La Soc. Fr. De Pediatr. 2020, 27, eS4–eS7. [Google Scholar] [CrossRef]
- Goetz, D.; Ren, C.L. Review of Cystic Fibrosis. Pediatr. Ann. 2019, 48, e154–e161. [Google Scholar] [CrossRef]
- Frickmann, H.; Jungblut, S.; Hirche, T.O.; Gross, U.; Kuhns, M.; Zautner, A.E. Spectrum of viral infections in patients with cystic fibrosis. Eur. J. Microbiol. Immunol. 2012, 2, 161–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Flight, W.G.; Bright-Thomas, R.J.; Tilston, P.; Mutton, K.J.; Guiver, M.; Morris, J.; Webb, A.K.; Jones, A.M. Incidence and clinical impact of respiratory viruses in adults with cystic fibrosis. Thorax 2014, 69, 247–253. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fainardi, V.; Longo, F.; Chetta, A.; Esposito, S.; Pisi, G. Sars-CoV-2 infection in patients with cystic fibrosis. An overview. Acta Bio-Med. Atenei Parm. 2020, 91, e2020035. [Google Scholar] [CrossRef]
- Goffard, A.; Lambert, V.; Salleron, J.; Herwegh, S.; Engelmann, I.; Pinel, C.; Pin, I.; Perrez, T.; Prevotat, A.; Dewilde, A.; et al. Virus and cystic fibrosis: Rhinoviruses are associated with exacerbations in adult patients. J. Clin. Virol. Off. Publ. Pan Am. Soc. Clin. Virol. 2014, 60, 147–153. [Google Scholar] [CrossRef] [PubMed]
- Kiedrowski, M.R.; Bomberger, J.M. Viral-Bacterial Co-infections in the Cystic Fibrosis Respiratory Tract. Front. Immunol. 2018, 9, 3067. [Google Scholar] [CrossRef] [Green Version]
- Mathew, H.R.; Choi, M.Y.; Parkins, M.D.; Fritzler, M.J. Systematic review: Cystic fibrosis in the SARS-CoV-2/COVID-19 pandemic. BMC Pulm. Med. 2021, 21, 173. [Google Scholar] [CrossRef]
- McClenaghan, E.; Cosgriff, R.; Brownlee, K.; Ahern, S.; Burgel, P.R.; Byrnes, C.A.; Colombo, C.; Corvol, H.; Cheng, S.Y.; Daneau, G.; et al. The global impact of SARS-CoV-2 in 181 people with cystic fibrosis. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2020, 19, 868–871. [Google Scholar] [CrossRef]
- Meyer, V.M.C.; Siqueira, M.M.; Costa, P.; Caetano, B.C.; Oliveira Lopes, J.C.; Folescu, T.W.; Motta, F.D.C. Clinical impact of respiratory virus in pulmonary exacerbations of children with Cystic Fibrosis. PLoS ONE 2020, 15, e0240452. [Google Scholar] [CrossRef]
- Mirza, A.A.; Rad, E.J.; Mohabir, P.K. Cystic fibrosis and COVID-19: Care considerations. Respir. Med. Case Rep. 2020, 31, 101226. [Google Scholar] [CrossRef]
- Peckham, D.; McDermott, M.F.; Savic, S.; Mehta, A. COVID-19 meets Cystic Fibrosis: For better or worse? Genes Immun. 2020, 21, 260–262. [Google Scholar] [CrossRef]
- Colombo, C.; Burgel, P.R.; Gartner, S.; van Koningsbruggen-Rietschel, S.; Naehrlich, L.; Sermet-Gaudelus, I.; Southern, K.W. Impact of COVID-19 on people with cystic fibrosis. Lancet Respir. Med. 2020, 8, e35–e36. [Google Scholar] [CrossRef] [PubMed]
- Colombo, C.; Cipolli, M.; Dacco, V.; Medino, P.; Alghisi, F.; Ambroni, M.; Badolato, R.; Battistini, F.; Bignamini, E.; Casciaro, R.; et al. Clinical course and risk factors for severe COVID-19 among Italian patients with cystic fibrosis: A study within the Italian Cystic Fibrosis Society. Infection 2022, 50, 671–679. [Google Scholar] [CrossRef]
- Cosgriff, R.; Ahern, S.; Bell, S.C.; Brownlee, K.; Burgel, P.R.; Byrnes, C.; Corvol, H.; Cheng, S.Y.; Elbert, A.; Faro, A.; et al. A multinational report to characterise SARS-CoV-2 infection in people with cystic fibrosis. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2020, 19, 355–358. [Google Scholar] [CrossRef] [PubMed]
- Ebrahimi Chaharom, F.; Pourafkari, L.; Ebrahimi Chaharom, A.A.; Nader, N.D. Effects of corticosteroids on Covid-19 patients: A systematic review and meta-analysis on clinical outcomes. Pulm. Pharmacol. Ther. 2022, 72, 102107. [Google Scholar] [CrossRef] [PubMed]
- Decaro, N.; Lorusso, A. Novel human coronavirus (SARS-CoV-2): A lesson from animal coronaviruses. Vet. Microbiol. 2020, 244, 108693. [Google Scholar] [CrossRef] [PubMed]
- Rajapakse, N.; Dixit, D. Human and novel coronavirus infections in children: A review. Paediatr. Int. Child Health 2021, 41, 36–55. [Google Scholar] [CrossRef]
- Santacroce, L.; Charitos, I.A.; Carretta, D.M.; De Nitto, E.; Lovero, R. The human coronaviruses (HCoVs) and the molecular mechanisms of SARS-CoV-2 infection. J. Mol. Med. 2021, 99, 93–106. [Google Scholar] [CrossRef]
- Sharma, H.N.; Latimore, C.O.D.; Matthews, Q.L. Biology and Pathogenesis of SARS-CoV-2: Understandings for Therapeutic Developments against COVID-19. Pathogens 2021, 10, 1218. [Google Scholar] [CrossRef]
- Latif, A.A.; Mukaratirwa, S. Zoonotic origins and animal hosts of coronaviruses causing human disease pandemics: A review. Onderstepoort J. Vet. Res. 2020, 87, e1–e9. [Google Scholar] [CrossRef]
- Wen, C.; Sun, L.; Zhao, M.C.; Duan, S.X.; Wang, L.; Cui, X.W. Clinical Study of Human Coronavirus NL63, OC43, 229E, HKU1 Infentions in Hospitalized Children from 2015 to 2020. Infect. Drug Resist. 2022, 15, 1093–1101. [Google Scholar] [CrossRef]
- Jo, K.J.; Choi, S.H.; Oh, C.E.; Kim, H.; Choi, B.S.; Jo, D.S.; Park, S.E. Epidemiology and Clinical Characteristics of Human Coronaviruses-Associated Infections in Children: A Multi-Center Study. Front. Pediatr. 2022, 10, 877759. [Google Scholar] [CrossRef] [PubMed]
- Irani, S. Immune Responses in SARS-CoV-2, SARS-CoV, and MERS-CoV Infections: A Comparative Review. Int. J. Prev. Med. 2022, 13, 45. [Google Scholar] [CrossRef] [PubMed]
- Abdelrahman, Z.; Li, M.; Wang, X. Comparative Review of SARS-CoV-2, SARS-CoV, MERS-CoV, and Influenza A Respiratory Viruses. Front. Immunol. 2020, 11, 552909. [Google Scholar] [CrossRef] [PubMed]
- Kahn, J.S.; McIntosh, K. History and recent advances in coronavirus discovery. Pediatr. Infect. Dis. J. 2005, 24, S223–S227, discussion S226. [Google Scholar] [CrossRef]
- Cascella, M.; Rajnik, M.; Aleem, A.; Dulebohn, S.C.; Di Napoli, R. Features, Evaluation, and Treatment of Coronavirus (COVID-19). In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Cekmen, N.; Ersoy, Z.; Gunay, Y.I.; Ghavam, A.A.; Tufan, M.Y.S.; Sahin, I.M. Evaluation of coronavirus diseases (COVID-19) in terms of epidemiological and clinical features, comorbidities, diagnostic methods, treatment, and mortality. J. Educ. Health Promot. 2022, 11, 236. [Google Scholar] [CrossRef]
- Aslan, A.; Aslan, C.; Zolbanin, N.M.; Jafari, R. Acute respiratory distress syndrome in COVID-19: Possible mechanisms and therapeutic management. Pneumonia 2021, 13, 14. [Google Scholar] [CrossRef]
- Goh, K.J.; Choong, M.C.; Cheong, E.H.; Kalimuddin, S.; Duu Wen, S.; Phua, G.C.; Chan, K.S.; Haja Mohideen, S. Rapid Progression to Acute Respiratory Distress Syndrome: Review of Current Understanding of Critical Illness from Coronavirus Disease 2019 (COVID-19) Infection. Ann. Acad. Med. Singap. 2020, 49, 108–118. [Google Scholar] [CrossRef]
- COVID-19 Excess Mortality Collaborators. Estimating excess mortality due to the COVID-19 pandemic: A systematic analysis of COVID-19-related mortality, 2020–2021. Lancet 2022, 399, 1513–1536. [Google Scholar] [CrossRef]
- Adam, D. Covid’s True Death Toll: Much Higher Than Official Records. Nature 2022, 603, 562. [Google Scholar] [CrossRef]
- Klein, S.; Cortese, M.; Winter, S.L.; Wachsmuth-Melm, M.; Neufeldt, C.J.; Cerikan, B.; Stanifer, M.L.; Boulant, S.; Bartenschlager, R.; Chlanda, P. SARS-CoV-2 structure and replication characterized by in situ cryo-electron tomography. Nat. Commun. 2020, 11, 5885. [Google Scholar] [CrossRef]
- Malik, Y.A. Properties of Coronavirus and SARS-CoV-2. Malays. J. Pathol. 2020, 42, 3–11. [Google Scholar] [PubMed]
- Kaul, D. An overview of coronaviruses including the SARS-2 coronavirus—Molecular biology, epidemiology and clinical implications. Curr. Med. Res. Pract. 2020, 10, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Satija, N.; Lal, S.K. The molecular biology of SARS coronavirus. Ann. N. Y. Acad. Sci. 2007, 1102, 26–38. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.; Petitjean, S.J.L.; Koehler, M.; Zhang, Q.; Dumitru, A.C.; Chen, W.; Derclaye, S.; Vincent, S.P.; Soumillion, P.; Alsteens, D. Author Correction: Molecular interaction and inhibition of SARS-CoV-2 binding to the ACE2 receptor. Nat. Commun. 2021, 12, 2996. [Google Scholar] [CrossRef] [PubMed]
- Kuba, K.; Yamaguchi, T.; Penninger, J.M. Angiotensin-Converting Enzyme 2 (ACE2) in the Pathogenesis of ARDS in COVID-19. Front. Immunol. 2021, 12, 732690. [Google Scholar] [CrossRef]
- Camargo, R.L.; Bombassaro, B.; Monfort-Pires, M.; Mansour, E.; Palma, A.C.; Ribeiro, L.C.; Ulaf, R.G.; Bernardes, A.F.; Nunes, T.A.; Agrela, M.V.; et al. Plasma Angiotensin II Is Increased in Critical Coronavirus Disease 2019. Front. Cardiovasc. Med. 2022, 9, 847809. [Google Scholar] [CrossRef]
- Santos, S.H.; Andrade, J.M. Angiotensin 1-7: A peptide for preventing and treating metabolic syndrome. Peptides 2014, 59, 34–41. [Google Scholar] [CrossRef]
- Shang, J.; Wan, Y.; Luo, C.; Ye, G.; Geng, Q.; Auerbach, A.; Li, F. Cell entry mechanisms of SARS-CoV-2. Proc. Natl. Acad. Sci. USA 2020, 117, 11727–11734. [Google Scholar] [CrossRef]
- Malone, B.; Urakova, N.; Snijder, E.J.; Campbell, E.A. Structures and functions of coronavirus replication-transcription complexes and their relevance for SARS-CoV-2 drug design. Nat. Rev. Mol. Cell Biol. 2022, 23, 21–39. [Google Scholar] [CrossRef]
- Romano, M.; Ruggiero, A.; Squeglia, F.; Maga, G.; Berisio, R. A Structural View of SARS-CoV-2 RNA Replication Machinery: RNA Synthesis, Proofreading and Final Capping. Cells 2020, 9, 1267. [Google Scholar] [CrossRef]
- V’Kovski, P.; Kratzel, A.; Steiner, S.; Stalder, H.; Thiel, V. Coronavirus biology and replication: Implications for SARS-CoV-2. Nat. Rev. Microbiol. 2021, 19, 155–170. [Google Scholar] [CrossRef] [PubMed]
- Letko, M.; Marzi, A.; Munster, V. Functional assessment of cell entry and receptor usage for SARS-CoV-2 and other lineage B betacoronaviruses. Nat. Microbiol. 2020, 5, 562–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wan, Y.; Shang, J.; Graham, R.; Baric, R.S.; Li, F. Receptor Recognition by the Novel Coronavirus from Wuhan: An Analysis Based on Decade-Long Structural Studies of SARS Coronavirus. J. Virol. 2020, 94, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, H.; Rao, Z. Structural biology of SARS-CoV-2 and implications for therapeutic development. Nat. Rev. Microbiol. 2021, 19, 685–700. [Google Scholar] [CrossRef] [PubMed]
- Saraste, J.; Prydz, K. Assembly and Cellular Exit of Coronaviruses: Hijacking an Unconventional Secretory Pathway from the Pre-Golgi Intermediate Compartment via the Golgi Ribbon to the Extracellular Space. Cells 2021, 10, 503. [Google Scholar] [CrossRef] [PubMed]
- Scherer, K.M.; Mascheroni, L.; Carnell, G.W.; Wunderlich, L.C.S.; Makarchuk, S.; Brockhoff, M.; Mela, I.; Fernandez-Villegas, A.; Barysevich, M.; Stewart, H.; et al. SARS-CoV-2 nucleocapsid protein adheres to replication organelles before viral assembly at the Golgi/ERGIC and lysosome-mediated egress. Sci. Adv. 2022, 8, eabl4895. [Google Scholar] [CrossRef]
- Darif, D.; Hammi, I.; Kihel, A.; El Idrissi Saik, I.; Guessous, F.; Akarid, K. The pro-inflammatory cytokines in COVID-19 pathogenesis: What goes wrong? Microb. Pathog. 2021, 153, 104799. [Google Scholar] [CrossRef]
- Tay, M.Z.; Poh, C.M.; Renia, L.; MacAry, P.A.; Ng, L.F.P. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef]
- Ferreira, A.C.; Soares, V.C.; de Azevedo-Quintanilha, I.G.; Dias, S.; Fintelman-Rodrigues, N.; Sacramento, C.Q.; Mattos, M.; de Freitas, C.S.; Temerozo, J.R.; Teixeira, L.; et al. SARS-CoV-2 engages inflammasome and pyroptosis in human primary monocytes. Cell Death Discov. 2021, 7, 43. [Google Scholar] [CrossRef]
- Silva, M.J.A.; Rodrigues, Y.C.; Lima, K.V.B.; Lima, L. Innate immunity to SARS-CoV-2 infection: A review. Epidemiol. Infect. 2022, 150, e142. [Google Scholar] [CrossRef]
- Polgreen, P.M.; Comellas, A.P. Clinical Phenotypes of Cystic Fibrosis Carriers. Annu. Rev. Med. 2022, 73, 563–574. [Google Scholar] [CrossRef]
- Michels, M.; Matte, U.; Fraga, L.R.; Mancuso, A.C.B.; Ligabue-Braun, R.; Berneira, E.F.R.; Siebert, M.; Sanseverino, M.T.V. Determining the pathogenicity of CFTR missense variants: Multiple comparisons of in silico predictors and variant annotation databases. Genet. Mol. Biol. 2019, 42, 560–570. [Google Scholar] [CrossRef] [Green Version]
- Arslan, A.B.; Zamani, A.G.; Pekcan, S.; Yildirim, M.S. A Novel Pathogenic Variant of the CFTR Gene in a Patient with Cystic Fibrosis Phenotype-c.4096A > T. J. Pediatr. Genet. 2020, 9, 40–43. [Google Scholar] [CrossRef]
- Lukacs, G.L.; Verkman, A.S. CFTR: Folding, misfolding and correcting the DeltaF508 conformational defect. Trends Mol. Med. 2012, 18, 81–91. [Google Scholar] [CrossRef] [Green Version]
- Caverly, L.J.; LiPuma, J.J. Cystic fibrosis respiratory microbiota: Unraveling complexity to inform clinical practice. Expert Rev. Respir. Med. 2018, 12, 857–865. [Google Scholar] [CrossRef]
- Scotet, V.; L’Hostis, C.; Ferec, C. The Changing Epidemiology of Cystic Fibrosis: Incidence, Survival and Impact of the CFTR Gene Discovery. Genes 2020, 11, 589. [Google Scholar] [CrossRef]
- Madacsy, T.; Pallagi, P.; Maleth, J. Cystic Fibrosis of the Pancreas: The Role of CFTR Channel in the Regulation of Intracellular Ca2+ Signaling and Mitochondrial Function in the Exocrine Pancreas. Front. Physiol. 2018, 9, 1585. [Google Scholar] [CrossRef] [Green Version]
- Freswick, P.N.; Reid, E.K.; Mascarenhas, M.R. Pancreatic Enzyme Replacement Therapy in Cystic Fibrosis. Nutrients 2022, 14, CD008227. [Google Scholar] [CrossRef]
- Ong, T.; Marshall, S.G.; Karczeski, B.A.; Sternen, D.L.; Cheng, E.; Cutting, G.R. Cystic Fibrosis and Congenital Absence of the Vas Deferens. In GeneReviews®; Adam, M.P., Everman, D.B., Mirzaa, G.M., Pagon, R.A., Wallace, S.E., Bean, L.J.H., Gripp, K.W., Amemiya, A., Eds.; University of Washington: Seattle, WA, USA, 1993. [Google Scholar]
- Lukasiak, A.; Zajac, M. The Distribution and Role of the CFTR Protein in the Intracellular Compartments. Membranes 2021, 11, 804. [Google Scholar] [CrossRef]
- Gentzsch, M.; Mall, M.A. Ion Channel Modulators in Cystic Fibrosis. Chest 2018, 154, 383–393. [Google Scholar] [CrossRef]
- Hill, D.B.; Long, R.F.; Kissner, W.J.; Atieh, E.; Garbarine, I.C.; Markovetz, M.R.; Fontana, N.C.; Christy, M.; Habibpour, M.; Tarran, R.; et al. Pathological mucus and impaired mucus clearance in cystic fibrosis patients result from increased concentration, not altered pH. Eur. Respir. J. 2018, 52, 1801297. [Google Scholar] [CrossRef] [PubMed]
- Mall, M.A. Unplugging Mucus in Cystic Fibrosis and Chronic Obstructive Pulmonary Disease. Ann. Am. Thorac. Soc. 2016, 13 (Suppl. S2), S177–S185. [Google Scholar] [CrossRef] [PubMed]
- Kunzi, L.; Easter, M.; Hirsch, M.J.; Krick, S. Cystic Fibrosis Lung Disease in the Aging Population. Front. Pharmacol. 2021, 12, 601438. [Google Scholar] [CrossRef] [PubMed]
- Averna, M.; Melotti, P.; Sorio, C. Revisiting the Role of Leukocytes in Cystic Fibrosis. Cells 2021, 10, 3380. [Google Scholar] [CrossRef]
- McKelvey, M.C.; Weldon, S.; McAuley, D.F.; Mall, M.A.; Taggart, C.C. Targeting Proteases in Cystic Fibrosis Lung Disease. Paradigms, Progress, and Potential. Am. J. Respir. Crit. Care Med. 2020, 201, 141–147. [Google Scholar] [CrossRef] [Green Version]
- Wang, H.; Cebotaru, L.; Lee, H.W.; Yang, Q.; Pollard, B.S.; Pollard, H.B.; Guggino, W.B. CFTR Controls the Activity of NF-kappaB by Enhancing the Degradation of TRADD. Cell. Physiol. Biochem. Int. J. Exp. Cell. Physiol. Biochem. Pharmacol. 2016, 40, 1063–1078. [Google Scholar] [CrossRef] [Green Version]
- Hampton, T.H.; Ballok, A.E.; Bomberger, J.M.; Rutkowski, M.R.; Barnaby, R.; Coutermarsh, B.; Conejo-Garcia, J.R.; O’Toole, G.A.; Stanton, B.A. Does the F508-CFTR mutation induce a proinflammatory response in human airway epithelial cells? Am. J. Physiol. Lung Cell. Mol. Physiol. 2012, 303, L509–L518. [Google Scholar] [CrossRef]
- Aghasafari, P.; George, U.; Pidaparti, R. A review of inflammatory mechanism in airway diseases. Inflamm. Res. Off. J. Eur. Histamine Res. Soc. 2019, 68, 59–74. [Google Scholar] [CrossRef]
- Hartl, D.; Gaggar, A.; Bruscia, E.; Hector, A.; Marcos, V.; Jung, A.; Greene, C.; McElvaney, G.; Mall, M.; Doring, G. Innate immunity in cystic fibrosis lung disease. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2012, 11, 363–382. [Google Scholar] [CrossRef] [Green Version]
- John, G.; Yildirim, A.O.; Rubin, B.K.; Gruenert, D.C.; Henke, M.O. TLR-4-mediated innate immunity is reduced in cystic fibrosis airway cells. Am. J. Respir. Cell Mol. Biol. 2010, 42, 424–431. [Google Scholar] [CrossRef]
- Ralhan, A.; Laval, J.; Lelis, F.; Ballbach, M.; Grund, C.; Hector, A.; Hartl, D. Current Concepts and Controversies in Innate Immunity of Cystic Fibrosis Lung Disease. J. Innate Immun. 2016, 8, 531–540. [Google Scholar] [CrossRef]
- Camus, L.; Briaud, P.; Vandenesch, F.; Moreau, K. How Bacterial Adaptation to Cystic Fibrosis Environment Shapes Interactions Between Pseudomonas aeruginosa and Staphylococcus aureus. Front. Microbiol. 2021, 12, 617784. [Google Scholar] [CrossRef]
- Briaud, P.; Camus, L.; Bastien, S.; Doleans-Jordheim, A.; Vandenesch, F.; Moreau, K. Coexistence with Pseudomonas aeruginosa alters Staphylococcus aureus transcriptome, antibiotic resistance and internalization into epithelial cells. Sci. Rep. 2019, 9, 16564. [Google Scholar] [CrossRef] [Green Version]
- Reece, E.; Bettio, P.H.A.; Renwick, J. Polymicrobial Interactions in the Cystic Fibrosis Airway Microbiome Impact the Antimicrobial Susceptibility of Pseudomonas aeruginosa. Antibiotics 2021, 10, 827. [Google Scholar] [CrossRef] [PubMed]
- Somayaji, R.; Goss, C.H.; Khan, U.; Neradilek, M.; Neuzil, K.M.; Ortiz, J.R. Cystic Fibrosis Pulmonary Exacerbations Attributable to Respiratory Syncytial Virus and Influenza: A Population-Based Study. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2017, 64, 1760–1767. [Google Scholar] [CrossRef] [Green Version]
- Wiltshire, D.A.; Vahora, I.S.; Tsouklidis, N.; Kumar, R.; Khan, S. H1N1 Influenza Virus in Patients With Cystic Fibrosis: A Literature Review Examining Both Disease Entities and Their Association in Light of the 2009 Pandemic. Cureus 2020, 12, e9218. [Google Scholar] [CrossRef]
- Viviani, L.; Assael, B.M.; Kerem, E.; The ECFS (A) H1N1 Study Group. Impact of the A (H1N1) pandemic influenza (season 2009–2010) on patients with cystic fibrosis. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2011, 10, 370–376. [Google Scholar] [CrossRef] [Green Version]
- Riccetto, A.G.; Ribeiro, J.D.; Silva, M.T.; Almeida, R.S.; Arns, C.W.; Baracat, E.C. Respiratory syncytial virus (RSV) in infants hospitalized for acute lower respiratory tract disease: Incidence and associated risks. Braz. J. Infect. Dis. Off. Publ. Braz. Soc. Infect. Dis. 2006, 10, 357–361. [Google Scholar] [CrossRef] [Green Version]
- Kiedrowski, M.R.; Gaston, J.R.; Kocak, B.R.; Coburn, S.L.; Lee, S.; Pilewski, J.M.; Myerburg, M.M.; Bomberger, J.M. Staphylococcus aureus Biofilm Growth on Cystic Fibrosis Airway Epithelial Cells Is Enhanced during Respiratory Syncytial Virus Coinfection. mSphere 2018, 3, e00341-18. [Google Scholar] [CrossRef] [Green Version]
- Terlizzi, V.; Motisi, M.A.; Pellegrino, R.; Padoan, R.; Chiappini, E. Risk factors for severe COVID-19 in people with cystic fibrosis: A systematic review. Front. Pediatr. 2022, 10, 958658. [Google Scholar] [CrossRef]
- Simonson, J.L.; Esposito, C.; Frantzen, T.; Henthorne, K.; Espinal, A.; Romano, S.; Ramdeo, R.; Trentacoste, J.; Tsang, D.; LaVecchia, G.; et al. The clinical impact of the Covid-19 pandemic first wave on patients with cystic fibrosis in New York. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2022, 21, e176–e183. [Google Scholar] [CrossRef] [PubMed]
- Colombo, C.; Alicandro, G.; Dacco, V.; Gagliano, V.; Morlacchi, L.C.; Casciaro, R.; Pisi, G.; Francalanci, M.; Badolato, R.; Bignamini, E.; et al. SARS-CoV-2 infection in cystic fibrosis: A multicentre prospective study with a control group, Italy, February-July 2020. PLoS ONE 2021, 16, e0251527. [Google Scholar] [CrossRef] [PubMed]
- Naehrlich, L.; Orenti, A.; Dunlevy, F.; Kasmi, I.; Harutyunyan, S.; Pfleger, A.; Keegan, S.; Daneau, G.; Petrova, G.; Tjesic-Drinkovic, D.; et al. Incidence of SARS-CoV-2 in people with cystic fibrosis in Europe between February and June 2020. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2021, 20, 566–577. [Google Scholar] [CrossRef]
- Mondejar-Lopez, P.; Quintana-Gallego, E.; Giron-Moreno, R.M.; Cortell-Aznar, I.; Ruiz de Valbuena-Maiz, M.; Diab-Caceres, L.; Prados-Sanchez, C.; Alvarez-Fernandez, A.; Garcia-Marcos, P.W.; Penalver-Mellado, C.; et al. Impact of SARS-CoV-2 infection in patients with cystic fibrosis in Spain: Incidence and results of the national CF-COVID19-Spain survey. Respir. Med. 2020, 170, 106062. [Google Scholar] [CrossRef]
- Berardis, S.; Verroken, A.; Vetillart, A.; Struyf, C.; Gilbert, M.; Gruson, D.; Gohy, S. SARS-CoV-2 seroprevalence in a Belgian cohort of patients with cystic fibrosis. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2020, 19, 872–874. [Google Scholar] [CrossRef]
- Kaya, G.; Issi, F.; Guven, B.; Ozkaya, E.; Buruk, C.K.; Cakir, M. SARS-CoV-2 Antibodies in Children with Chronic Disease from a Pediatric Gastroenterology Outpatient Clinic. Pediatr. Gastroenterol. Hepatol. Nutr. 2022, 25, 422–431. [Google Scholar] [CrossRef]
- Heiss, R.; Tan, L.; Schmidt, S.; Regensburger, A.P.; Ewert, F.; Mammadova, D.; Buehler, A.; Vogel-Claussen, J.; Voskrebenzev, A.; Rauh, M.; et al. Pulmonary Dysfunction after Pediatric COVID-19. Radiology 2022, 221250. [Google Scholar] [CrossRef]
- Bain, R.; Cosgriff, R.; Zampoli, M.; Elbert, A.; Burgel, P.R.; Carr, S.B.; Castanos, C.; Colombo, C.; Corvol, H.; Faro, A.; et al. Clinical characteristics of SARS-CoV-2 infection in children with cystic fibrosis: An international observational study. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2021, 20, 25–30. [Google Scholar] [CrossRef]
- Bezzerri, V.; Lucca, F.; Volpi, S.; Cipolli, M. Does cystic fibrosis constitute an advantage in COVID-19 infection? Ital. J. Pediatr. 2020, 46, 143. [Google Scholar] [CrossRef]
- Giron Moreno, R.M.; Garcia-Clemente, M.; Diab-Caceres, L.; Martinez-Vergara, A.; Martinez-Garcia, M.A.; Gomez-Punter, R.M. Treatment of Pulmonary Disease of Cystic Fibrosis: A Comprehensive Review. Antibiotics 2021, 10, 486. [Google Scholar] [CrossRef]
- Mitri, C.; Xu, Z.; Bardin, P.; Corvol, H.; Touqui, L.; Tabary, O. Novel Anti-Inflammatory Approaches for Cystic Fibrosis Lung Disease: Identification of Molecular Targets and Design of Innovative Therapies. Front. Pharmacol. 2020, 11, 1096. [Google Scholar] [CrossRef] [PubMed]
- Nichols, D.P.; Singh, P.K.; Baines, A.; Caverly, L.J.; Chmiel, J.F.; RL, G.I.; Lascano, J.; Morgan, S.J.; Retsch-Bogart, G.; Saiman, L.; et al. Testing the effects of combining azithromycin with inhaled tobramycin for P. aeruginosa in cystic fibrosis: A randomised, controlled clinical trial. Thorax 2022, 77, 581–588. [Google Scholar] [CrossRef] [PubMed]
- Dinwiddie, R. Anti-inflammatory therapy in cystic fibrosis. J. Cyst. Fibros. Off. J. Eur. Cyst. Fibros. Soc. 2005, 4 (Suppl. S2), 45–48. [Google Scholar] [CrossRef] [Green Version]
- Ahmed, M.H.; Hassan, A. Dexamethasone for the Treatment of Coronavirus Disease (COVID-19): A Review. SN Compr. Clin. Med. 2020, 2, 2637–2646. [Google Scholar] [CrossRef] [PubMed]
- Hasan, S.S.; Capstick, T.; Ahmed, R.; Kow, C.S.; Mazhar, F.; Merchant, H.A.; Zaidi, S.T.R. Mortality in COVID-19 patients with acute respiratory distress syndrome and corticosteroids use: A systematic review and meta-analysis. Expert Rev. Respir. Med. 2020, 14, 1149–1163. [Google Scholar] [CrossRef] [PubMed]
- Echeverria-Esnal, D.; Martin-Ontiyuelo, C.; Navarrete-Rouco, M.E.; De-Antonio Cusco, M.; Ferrandez, O.; Horcajada, J.P.; Grau, S. Azithromycin in the treatment of COVID-19: A review. Expert Rev. Anti-Infect. Ther. 2021, 19, 147–163. [Google Scholar] [CrossRef]
- Poddighe, D.; Aljofan, M. Clinical evidences on the antiviral properties of macrolide antibiotics in the COVID-19 era and beyond. Antivir. Chem. Chemother. 2020, 28, 2040206620961712. [Google Scholar] [CrossRef]
- Oliver, M.E.; Hinks, T.S.C. Azithromycin in viral infections. Rev. Med. Virol. 2021, 31, e2163. [Google Scholar] [CrossRef]
- Pani, A.; Lauriola, M.; Romandini, A.; Scaglione, F. Macrolides and viral infections: Focus on azithromycin in COVID-19 pathology. Int. J. Antimicrob. Agents 2020, 56, 106053. [Google Scholar] [CrossRef]
- Lidington, D.; Bolz, S.S. A Scientific Rationale for Using Cystic Fibrosis Transmembrane Conductance Regulator Therapeutics in COVID-19 Patients. Front. Physiol. 2020, 11, 583862. [Google Scholar] [CrossRef]
- Regard, L.; Martin, C.; Burnet, E.; Da Silva, J.; Burgel, P.R. CFTR Modulators in People with Cystic Fibrosis: Real-World Evidence in France. Cells 2022, 11, 1769. [Google Scholar] [CrossRef] [PubMed]
- Lotti, V.; Merigo, F.; Lagni, A.; Di Clemente, A.; Ligozzi, M.; Bernardi, P.; Rossini, G.; Concia, E.; Plebani, R.; Romano, M.; et al. CFTR Modulation Reduces SARS-CoV-2 Infection in Human Bronchial Epithelial Cells. Cells 2022, 11, 1347. [Google Scholar] [CrossRef] [PubMed]
- Cheemarla, N.R.; Watkins, T.A.; Mihaylova, V.T.; Wang, B.; Zhao, D.; Wang, G.; Landry, M.L.; Foxman, E.F. Dynamic innate immune response determines susceptibility to SARS-CoV-2 infection and early replication kinetics. J. Exp. Med. 2021, 218, e20210583. [Google Scholar] [CrossRef] [PubMed]
- Merigo, F.; Lotti, V.; Bernardi, P.; Conti, A.; Clemente, A.D.; Ligozzi, M.; Lagni, A.; Sorio, C.; Sbarbati, A.; Gibellini, D. Ultrastructural Characterization of Human Bronchial Epithelial Cells during SARS-CoV-2 Infection: Morphological Comparison of Wild-Type and CFTR-Modified Cells. Int. J. Mol. Sci. 2022, 23, 9724. [Google Scholar] [CrossRef]
- Flume, P.A.; Saiman, L.; Marshall, B. The Impact of COVID-19 in Cystic Fibrosis. Arch. De Bronconeumol. 2021. [Google Scholar] [CrossRef] [PubMed]
- Thee, S.; Busack, L.M.; Mall, M.A.; Stahl, M. Impact of lockdown during the COVID-19 pandemic on health status in patients with cystic fibrosis: A mono-centre observational study. ERJ Open Res. 2022, 8, 00588-2021. [Google Scholar] [CrossRef]
- Costa, R.L.F.; Costa, R.F.; Goncalves, C.P.; Cohen, R.W.F.; Santana, N.N. Telemedicine of patients with cystic fibrosis during the COVID-19 pandemic. Rev. Paul. De Pediatr. Orgao Of. Da Soc. De Pediatr. De Sao Paulo 2022, 40, e2021118. [Google Scholar] [CrossRef]
- Rad, E.J.; Mirza, A.A.; Chhatwani, L.; Purington, N.; Mohabir, P.K. Cystic fibrosis telemedicine in the era of COVID-19. JAMIA Open 2022, 5, ooac005. [Google Scholar] [CrossRef]
- Compton, M.; List, R.; Starheim, E.; Somerville, L.; Williamson, L.; Murray, R.; Jennings, D.; Bruschwein, H.; Albon, D. Home spirometry utilisation in telemedicine clinic for cystic fibrosis care during COVID-19 pandemic: A quality improvement process. BMJ Open Qual. 2021, 10, e001529. [Google Scholar] [CrossRef]
- Dixon, E.; Dick, K.; Ollosson, S.; Jones, D.; Mattock, H.; Bentley, S.; Saunders, C.; Matthews, J.; Dobra, B.; King, J.; et al. Telemedicine and cystic fibrosis: Do we still need face-to-face clinics? Paediatr. Respir. Rev. 2022, 42, 23–28. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Biondo, C.; Midiri, A.; Gerace, E.; Zummo, S.; Mancuso, G. SARS-CoV-2 Infection in Patients with Cystic Fibrosis: What We Know So Far. Life 2022, 12, 2087. https://doi.org/10.3390/life12122087
Biondo C, Midiri A, Gerace E, Zummo S, Mancuso G. SARS-CoV-2 Infection in Patients with Cystic Fibrosis: What We Know So Far. Life. 2022; 12(12):2087. https://doi.org/10.3390/life12122087
Chicago/Turabian StyleBiondo, Carmelo, Angelina Midiri, Elisabetta Gerace, Sebastiana Zummo, and Giuseppe Mancuso. 2022. "SARS-CoV-2 Infection in Patients with Cystic Fibrosis: What We Know So Far" Life 12, no. 12: 2087. https://doi.org/10.3390/life12122087