
Performance of Derived Laboratory Biomarkers with Regard to 30-Day Mortality in Kidney Transplant Recipients with COVID-19
 , , and
, , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical and Institutional Considerations
2.2. Study Design and Patients
2.3. Outcomes
2.4. Data Sources and Assessment
2.5. Laboratory Analysis
2.6. Laboratory Derived Biomarkers
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Azzi, Y.; Bartash, R.; Scalea, J.; Loarte-Campos, P.; Akalin, E. COVID-19 and Solid Organ Transplantation: A Review Article. Transplantation 2021, 105, 37–55. [Google Scholar] [CrossRef] [PubMed]
- Udomkarnjananun, S.; Kerr, S.J.; Townamchai, N.; Susantitaphong, P.; Tulvatana, W.; Praditpornsilpa, K.; Eiam-Ong, S.; Avihingsanon, Y. Mortality Risk Factors of COVID-19 Infection in Kidney Transplantation Recipients: A Systematic Review and Meta-Analysis of Cohorts and Clinical Registries. Sci. Rep. 2021, 11, 20073. [Google Scholar] [CrossRef] [PubMed]
- Parohan, M.; Yaghoubi, S.; Seraji, A.; Javanbakht, M.H.; Sarraf, P.; Djalali, M. Risk Factors for Mortality in Patients with Coronavirus Disease 2019 (COVID-19) Infection: A Systematic Review and Meta-Analysis of Observational Studies. Aging Male 2020, 23, 1416–1424. [Google Scholar] [CrossRef] [PubMed]
- Dessie, Z.G.; Zewotir, T. Mortality-Related Risk Factors of COVID-19: A Systematic Review and Meta-Analysis of 42 Studies and 423,117 Patients. BMC Infect. Dis. 2021, 21, 855. [Google Scholar] [CrossRef]
- Modelli de Andrade, L.G.; de Sandes-Freitas, T.V.; Requião-Moura, L.R.; Viana, L.A.; Cristelli, M.P.; Garcia, V.D.; Alcântara, A.L.C.; Esmeraldo, R.d.M.; Abbud Filho, M.; Pacheco-Silva, A.; et al. Development and Validation of a Simple Web-Based Tool for Early Prediction of COVID-19-Associated Death in Kidney Transplant Recipients. Am. J. Transplant. 2022, 22, 610–625. [Google Scholar] [CrossRef]
- Domjanović, J.; Matetic, A.; Baković Kramarić, D.; Domjanović Škopinić, T.; Borić Škaro, D.; Delić, N.; Runjić, F.; Jeličić, I. Association of the Novel CROW-65 Risk Score and Mortality in Hospitalized Kidney Transplant Recipients with COVID-19: A Retrospective Observational Study. Wien. Klin. Wochenschr. 2022. online ahead of print. [Google Scholar] [CrossRef]
- Liu, Y.; Du, X.; Chen, J.; Jin, Y.; Peng, L.; Wang, H.H.X.; Luo, M.; Chen, L.; Zhao, Y. Neutrophil-to-Lymphocyte Ratio as an Independent Risk Factor for Mortality in Hospitalized Patients with COVID-19. J. Infect. 2020, 81, e6–e12. [Google Scholar] [CrossRef]
- Li, X.; Liu, C.; Mao, Z.; Xiao, M.; Wang, L.; Qi, S.; Zhou, F. Predictive Values of Neutrophil-to-Lymphocyte Ratio on Disease Severity and Mortality in COVID-19 Patients: A Systematic Review and Meta-Analysis. Crit. Care 2020, 24, 647. [Google Scholar] [CrossRef]
- Dávila-Collado, R.; Jarquín-Durán, O.; Solís-Vallejo, A.; Nguyen, M.A.; Espinoza, J.L. Elevated Monocyte to Lymphocyte Ratio and Increased Mortality among Patients with Chronic Kidney Disease Hospitalized for COVID-19. J. Pers. Med. 2021, 11, 224. [Google Scholar] [CrossRef]
- Zinellu, A.; Arru, F.; De Vito, A.; Sassu, A.; Valdes, G.; Scano, V.; Zinellu, E.; Perra, R.; Madeddu, G.; Carru, C.; et al. The De Ritis Ratio as Prognostic Biomarker of In-Hospital Mortality in COVID-19 Patients. Eur. J. Clin. Investig. 2021, 51, e13427. [Google Scholar] [CrossRef]
- Küçükceran, K.; Ayranci, M.K.; Girişgin, A.S.; Koçak, S. Predictive Value of D-Dimer/Albumin Ratio and Fibrinogen/Albumin Ratio for in-Hospital Mortality in Patients with COVID-19. Int. J. Clin. Pract. 2021, 75, e14263. [Google Scholar] [CrossRef] [PubMed]
- Ozkok, A.; Alpay, N.; Alan, S.; Bakan, N.D.; Soysal, F.; Yazici, H.; Ekşioğlu-Demiralp, E.; Yildiz, A. Immunological Parameters Associated with the Severity of COVID-19 Pneumonia in Kidney Transplant Recipients. Int. Urol. Nephrol. 2022, 54, 1105–1116. [Google Scholar] [CrossRef] [PubMed]
- Chandler, C.M.; Reid, M.C.; Cherian, S.; Sabath, D.E.; Edlefsen, K.L. Comparison of Blood Counts and Markers of Inflammation and Coagulation in Patients With and Without COVID-19 Presenting to the Emergency Department in Seattle, WA. Am. J. Clin. Pathol. 2021, 156, 185–197. [Google Scholar] [CrossRef] [PubMed]
- Peçanha-Pietrobom, P.M.; Leite, G.G.F.; Hunter, J.; Ferreira, P.R.A.; Burattini, M.N.; Bellei, N.; Ota-Arakaki, J.S.; Salomao, R. The Clinical Course of Hospitalized Moderately Ill COVID-19 Patients Is Mirrored by Routine Hematologic Tests and Influenced by Renal Transplantation. PLoS ONE 2021, 16, e0258987. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Lu, X.; Wang, S.; Li, H. High Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio Are Associated with Poor Survival in Patients with Hemodialysis. Biomed. Res. Int. 2021, 2021, 9958081. [Google Scholar] [CrossRef]
- Chan, A.S.; Rout, A. Use of Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios in COVID-19. J. Clin. Med. Res. 2020, 12, 448–453. [Google Scholar] [CrossRef]
- Liu, Z.; Hu, D.; Li, J.; Xia, Q.; Gong, Y.; Li, Z.; Wu, Q.; Yi, M.; Huang, Y.; Wu, M.; et al. Prognostic Potential of Liver Enzymes in Patients With COVID-19 at the Leishenshan Hospital in Wuhan. Front. Cell. Infect. Microbiol. 2021, 11, 636999. [Google Scholar] [CrossRef]
- Kalabin, A.; Mani, V.R.; Valdivieso, S.C.; Donaldson, B. Does C Reactive Protein/Albumin Ratio Have Prognostic Value in Patients with COVID-19. J. Infect. Dev. Ctries. 2021, 15, 1086–1093. [Google Scholar] [CrossRef]
- Huang, Y.; Guo, L.; Chen, J.; Wu, M.; Zhang, C.; Liu, Z.; Li, J.; Li, K.; Xiong, Z.; Wu, Q.; et al. Serum Lactate Dehydrogenase Level as a Prognostic Factor for COVID-19: A Retrospective Study Based on a Large Sample Size. Front. Med. 2022, 8, 671667. [Google Scholar] [CrossRef]
- Fouad, S.H.; Allam, M.F.; Taha, S.I.; Okba, A.A.; Hosny, A.; Moneer, M.; Roman, S.W. Comparison of Hemoglobin Level and Neutrophil to Lymphocyte Ratio as Prognostic Markers in Patients with COVID-19. J. Int. Med. Res. 2021, 49, 03000605211030124. [Google Scholar] [CrossRef]
- Mungan, İ.; Bostancı, E.B.; Türksal, E.; Tezcan, B.; Aktaş, M.N.; Can, M.; Kazancı, D.; Turan, S. The Predictive Power of C-Reactive Protein- Lymphocyte Ratio for in-Hospital Mortality after Colorectal Cancer Surgery. Cancer Rep. 2021, 4, e1330. [Google Scholar] [CrossRef] [PubMed]
- Yoo, J.-W.; Ju, S.; Lee, S.J.; Cho, Y.J.; Lee, J.D.; Kim, H.C. Red Cell Distribution Width/Albumin Ratio Is Associated with 60-Day Mortality in Patients with Acute Respiratory Distress Syndrome. Infect. Dis. 2020, 52, 266–270. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Yuan, J.; Liu, L.; Qie, S.; Yang, L.; Yan, Z. Platelet-to-Albumin Ratio: A Risk Factor Associated with Technique Failure and Mortality in Peritoneal Dialysis Patients. Ren. Fail. 2021, 43, 1359–1367. [Google Scholar] [CrossRef]
- Tan, J.; Song, G.; Wang, S.; Dong, L.; Liu, X.; Jiang, Z.; Qin, A.; Tang, Y.; Qin, W. Platelet-to-Albumin Ratio: A Novel IgA Nephropathy Prognosis Predictor. Front. Immunol. 2022, 13, 842362. [Google Scholar] [CrossRef] [PubMed]
- Zhan, H.; Chen, H.; Liu, C.; Cheng, L.; Yan, S.; Li, H.; Li, Y. Diagnostic Value of D-Dimer in COVID-19: A Meta-Analysis and Meta-Regression. Clin. Appl. Thromb. Hemost. 2021, 27, 10760296211010976. [Google Scholar] [CrossRef]
- Lagunas-Rangel, F.A. Neutrophil-to-lymphocyte Ratio and Lymphocyte-to-C-reactive Protein Ratio in Patients with Severe Coronavirus Disease 2019 (COVID-19): A Meta-analysis. J. Med. Virol. 2020, 92, 1733–1734. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ulloque-Badaracco, J.R.; Ivan Salas-Tello, W.; Al-Kassab-Córdova, A.; Alarcón-Braga, E.A.; Benites-Zapata, V.A.; Maguiña, J.L.; Hernandez, A.V. Prognostic Value of Neutrophil-to-Lymphocyte Ratio in COVID-19 Patients: A Systematic Review and Meta-Analysis. Int. J. Clin. Pract. 2021, 75, e14596. [Google Scholar] [CrossRef] [PubMed]
- Rostami, M.; Mansouritorghabeh, H. D-Dimer Level in COVID-19 Infection: A Systematic Review. Expert Rev. Hematol. 2020, 13, 1265–1275. [Google Scholar] [CrossRef] [PubMed]
- Yan, D.; Huang, Q.; Dai, C.; Ren, W.; Chen, S. Lactic Dehydrogenase to Albumin Ratio Is Associated With the Risk of Stroke-Associated Pneumonia in Patients With Acute Ischemic Stroke. Front. Nutr. 2021, 8, 743216. [Google Scholar] [CrossRef]
- Lee, B.-K.; Ryu, S.; Oh, S.-K.; Ahn, H.-J.; Jeon, S.-Y.; Jeong, W.-J.; Cho, Y.-C.; Park, J.-S.; You, Y.-H.; Kang, C.-S. Lactate Dehydrogenase to Albumin Ratio as a Prognostic Factor in Lower Respiratory Tract Infection Patients. Am. J. Emerg. Med. 2022, 52, 54–58. [Google Scholar] [CrossRef]
- Alizadeh, N.; Tabatabaei, F.-S.; Azimi, A.; Faraji, N.; Akbarpour, S.; Dianatkhah, M.; Moghaddas, A. Lactate Dehydrogenase to Albumin Ratio as a Predictive Factor of COVID-19 Patients’ Outcome; a Cross-Sectional Study. Arch. Acad. Emerg. Med. 2022, 10, e63. [Google Scholar] [CrossRef] [PubMed]
- Kljakovic Gaspic, T.; Pavicic Ivelja, M.; Kumric, M.; Matetic, A.; Delic, N.; Vrkic, I.; Bozic, J. In-Hospital Mortality of COVID-19 Patients Treated with High-Flow Nasal Oxygen: Evaluation of Biomarkers and Development of the Novel Risk Score Model CROW-65. Life 2021, 11, 735. [Google Scholar] [CrossRef] [PubMed]
- Hanley, J.A.; McNeil, B.J. A Method of Comparing the Areas under Receiver Operating Characteristic Curves Derived from the Same Cases. Radiology 1983, 148, 839–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiu, Y.; Su, Y.; Tu, G.-W.; Ju, M.-J.; He, H.-Y.; Gu, Z.-Y.; Yang, C.; Luo, Z. Neutrophil-to-Lymphocyte Ratio Predicts Mortality in Adult Renal Transplant Recipients with Severe Community-Acquired Pneumonia. Pathogens 2020, 9, 913. [Google Scholar] [CrossRef] [PubMed]
- Cravedi, P.; Mothi, S.S.; Azzi, Y.; Haverly, M.; Farouk, S.S.; Pérez-Sáez, M.J.; Redondo-Pachón, M.D.; Murphy, B.; Florman, S.; Cyrino, L.G.; et al. COVID-19 and Kidney Transplantation: Results from the TANGO International Transplant Consortium. Am. J. Transpl. 2020, 20, 3140–3148. [Google Scholar] [CrossRef] [PubMed]
- Demir, E.; Ucar, Z.A.; Dheir, H.; Danis, R.; Yelken, B.; Uyar, M.; Parmaksiz, E.; Artan, A.S.; Sinangil, A.; Merhametsiz, O.; et al. COVID-19 in Kidney Transplant Recipients: A Multicenter Experience from the First Two Waves of Pandemic. BMC Nephrol. 2022, 23, 183. [Google Scholar] [CrossRef]
- Oto, O.A.; Ozturk, S.; Turgutalp, K.; Arici, M.; Alpay, N.; Merhametsiz, O.; Sipahi, S.; Ogutmen, M.B.; Yelken, B.; Altiparmak, M.R.; et al. Predicting the Outcome of COVID-19 Infection in Kidney Transplant Recipients. BMC Nephrol. 2021, 22, 100. [Google Scholar] [CrossRef] [PubMed]
- Al-Farabi, M.J.; Nugraha, R.A.; Marsudi, B.A.; Azmi, Y. Biomarkers of Endothelial Dysfunction and Outcomes in Coronavirus Disease 2019 (COVID-19) Patients: A Systematic Review and Meta-Analysis. Microvasc. Res. 2021, 138, 104224. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
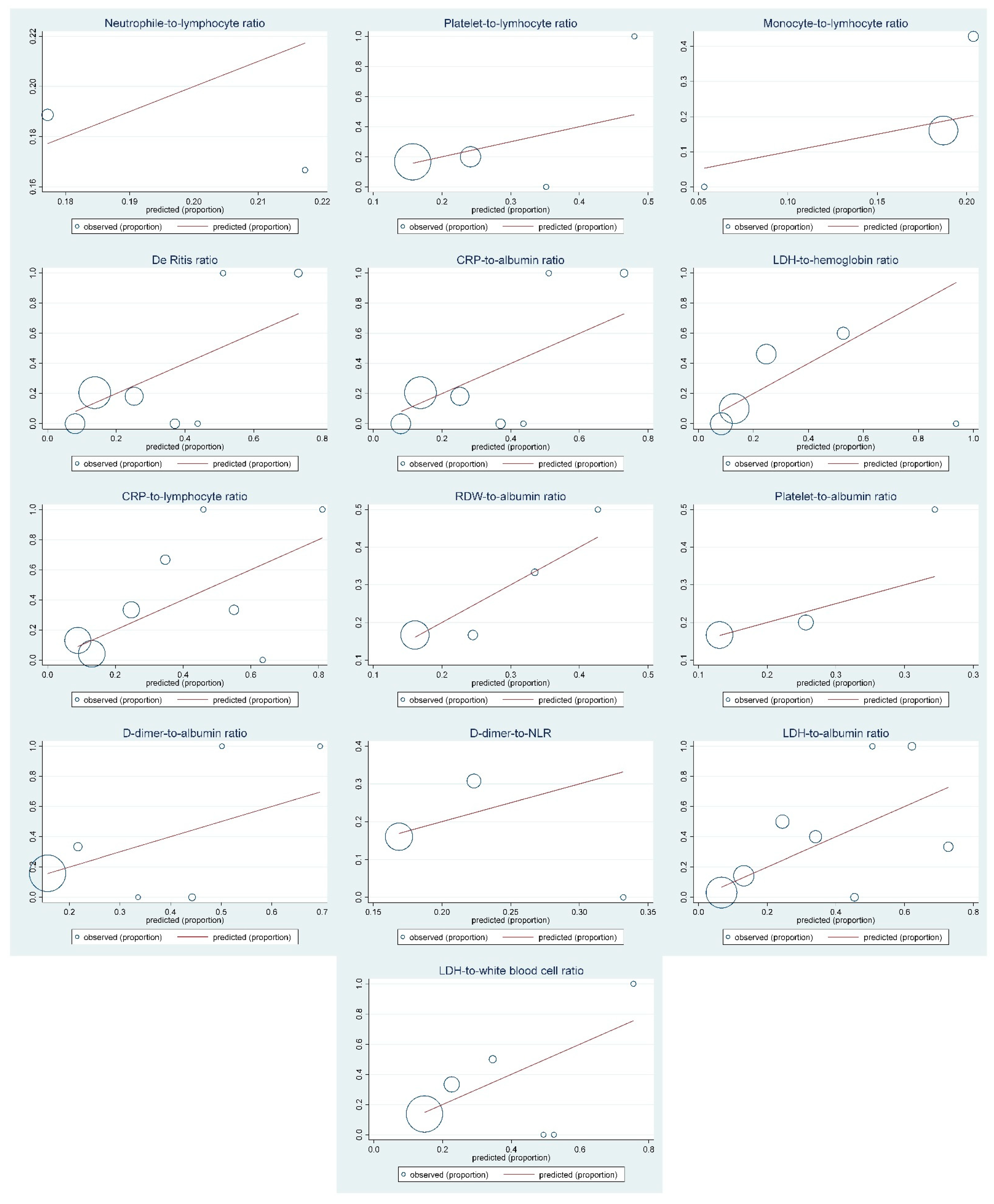
| Biomarkers | 30-Day Mortality | |||
|---|---|---|---|---|
| HR (95% CI), p-Value * | Harrell’s C Concordance Index | Somers’ D Index | Hosmer–Lemeshow Test, p-Value | |
| Neutrophile-to-lymphocyte ratio | 1.02 (0.94–1.12), p = 0.634 | 0.597 | 0.194 | 6.00, p = 0.815 |
| Platelet-to-lymphocyte ratio | 1.00 (0.99–1.01), p = 0.086 | 0.580 | 0.160 | 12.53, p = 0.251 |
| Monocyte-to-lymphocyte ratio | 0.88 (0.43–1.81), p = 0.724 | 0.537 | 0.074 | 10.18, p = 0.425 |
| De Ritis ratio | 3.83 (1.57–9.35), p = 0.003 | 0.691 | 0.382 | 12.65, p = 0.244 |
| CRP-to-albumin ratio | 1.36 (1.13–1.64), p = 0.001 | 0.733 | 0.466 | 9.40, p = 0.401 |
| LDH-to-hemoglobin ratio | 1.44 (1.07–1.92), p = 0.015 | 0.808 | 0.616 | 8.38, p = 0.592 |
| CRP-to-lymphocyte ratio | 1.03 (1.01–1.07), p = 0.003 | 0.681 | 0.361 | 7.19, p = 0.707 |
| RDW-to-albumin ratio | 7.44 (0.31–11.62), p = 0.601 | 0.525 | 0.049 | 6.94, p = 0.731 |
| Platelet-to-albumin ratio | 1.08 (0.82–1.42), p = 0.597 | 0.540 | 0.080 | 4.74, p = 0.908 |
| D-Dimer-to-albumin ratio | 4.94 (1.38–7.24), p = 0.038 | 0.571 | 0.143 | 6.02, p = 0.734 |
| D-Dimer-to-NLR | 1.05 (0.67–1.65), p = 0.821 | 0.504 | 0.008 | 7.45, p = 0.682 |
| LDH-to-albumin ratio | 1.20 (1.05–1.36), p = 0.008 | 0.751 | 0.502 | 7.07, p = 0.719 |
| LDH-to-WBC ratio | 1.03 (1.01–1.05), p = 0.024 | 0.629 | 0.259 | 8.94, p = 0.538 |
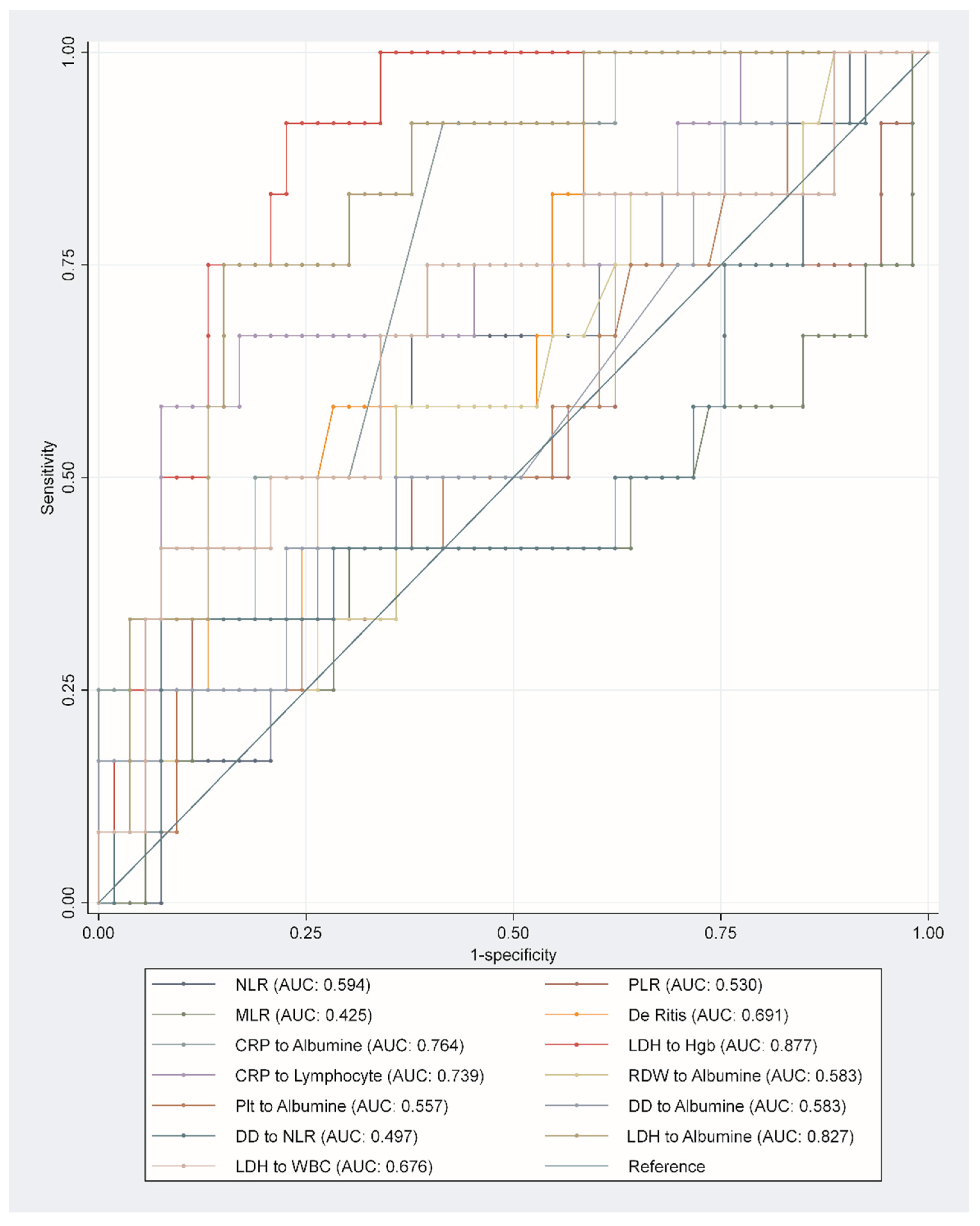
| Biomarkers | C-Statistic (95% CI) | p-Value | Sensitivity/Specificity | Youden’s Index |
|---|---|---|---|---|
| Neutrophile-to-lymphocyte ratio | 0.594 (0.420–0.768) | 0.310 | 0.67/0.62 | >6.17 |
| Platelet-to-lymphocyte ratio | 0.530 (0.321–0.739) | 0.748 | 0.50/0.62 | >290.84 |
| Monocyte-to-lymphocyte ratio | 0.425 (0.209–0.642) | 0.422 | 0.42/0.70 | >0.59 |
| De Ritis ratio | 0.691 (0.537–0.845) | 0.040 | 0.58/0.72 | >1.48 |
| CRP-to-albumin ratio | 0.764 (0.632–0.897) | 0.005 | 0.92/0.58 | >2.06 |
| LDH-to-hemoglobin ratio | 0.877 (0.793–0.962) | <0.001 | 0.92/0.77 | >2.21 |
| CRP-to-lymphocyte ratio | 0.739 (0.570–0.908) | 0.010 | 0.67/0.70 | >77.80 |
| RDW-to-albumin ratio | 0.583 (0.405–0.761) | 0.370 | 0.58/0.64 | >0.42 |
| Platelet-to-albumin ratio | 0.557 (0.376–0.737) | 0.543 | 0.42/0.72 | >6.79 |
| D-Dimer-to-albumin ratio | 0.583 (0.400–0.766) | 0.370 | 0.42/0.77 | >0.04 |
| D-Dimer-to-NLR | 0.497 (0.288–0.706) | 0.973 | 0.33/0.92 | >0.39 |
| LDH-to-albumin ratio | 0.827 (0.712–0.942) | <0.001 | 0.75/0.85 | >10.78 |
| LDH-to-WBC ratio | 0.676 (0.492–0.860) | 0.058 | 0.75/0.60 | >43.13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Domjanović, J.; Domjanović Škopinić, T.; Radić, J.; Luketin, M.; Jeličić, I.; Matetic, A. Performance of Derived Laboratory Biomarkers with Regard to 30-Day Mortality in Kidney Transplant Recipients with COVID-19. Life 2022, 12, 2068. https://doi.org/10.3390/life12122068
Domjanović J, Domjanović Škopinić T, Radić J, Luketin M, Jeličić I, Matetic A. Performance of Derived Laboratory Biomarkers with Regard to 30-Day Mortality in Kidney Transplant Recipients with COVID-19. Life. 2022; 12(12):2068. https://doi.org/10.3390/life12122068
Chicago/Turabian StyleDomjanović, Josipa, Tea Domjanović Škopinić, Josipa Radić, Mirko Luketin, Ivo Jeličić, and Andrija Matetic. 2022. "Performance of Derived Laboratory Biomarkers with Regard to 30-Day Mortality in Kidney Transplant Recipients with COVID-19" Life 12, no. 12: 2068. https://doi.org/10.3390/life12122068