
The Performance of Lateral Flow Tests in the Age of the Omicron: A Rapid Systematic Review
 ,
,
Abstract
:
1. Introduction
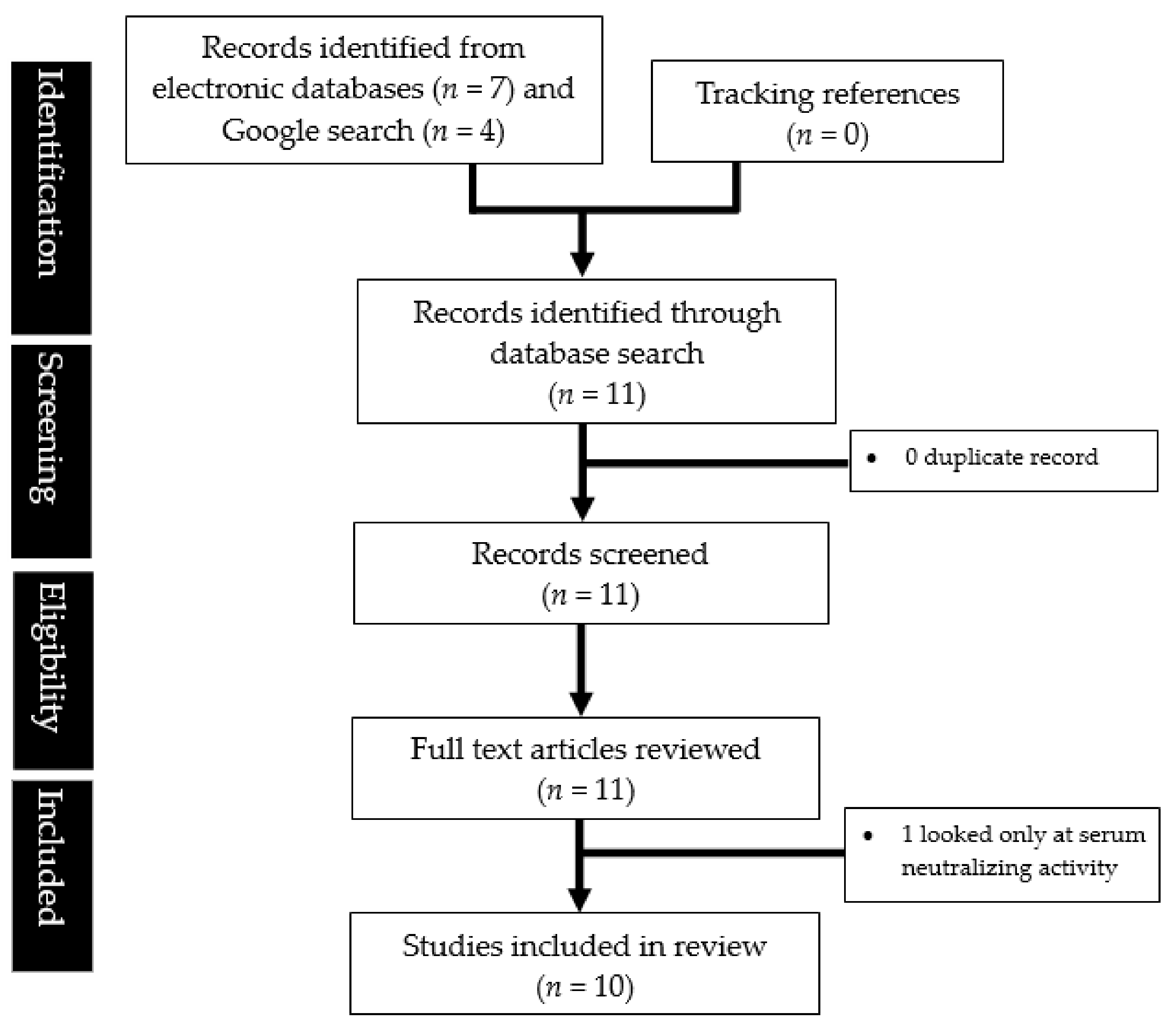
2. Methods
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- VanBlargan, L.A.; Errico, J.M.; Halfmann, P.J.; Zost, S.J.; Crowe, J.E.; Purcell, L.A.; Kawaoka, Y.; Corti, D.; Fremont, D.H.; Diamond, M.S. An infectious SARS-CoV-2 B. 1.1. 529 Omicron virus escapes neutralization by therapeutic monoclonal antibodies. Nat. Med. 2022, 28, 490–495. [Google Scholar] [CrossRef] [PubMed]
- Peeling, R.W.; Olliaro, P.L.; Boeras, D.I.; Fongwen, N. Scaling up COVID-19 rapid antigen tests: Promises and challenges. Lancet Infect. Dis. 2021, 21, e290–e295. [Google Scholar] [CrossRef]
- Wang, L.; Cheng, G. Sequence analysis of the Emerging Sars-CoV-2 Variant Omicron in South Africa. J. Med. Vi-Rology 2021, 94, 1728–1733. [Google Scholar] [CrossRef] [PubMed]
- Suratekar, R.; Ghosh, P.; Niesen, M.J.; Donadio, G.; Anand, P.; Soundararajan, V.; Venkatakrishnan, A.J. High diversity in Delta variant across countries revealed by genome-wide analysis of SARS-CoV-2 beyond the spike protein. Mol. Syst. Biol. 2022, 18, e10673. [Google Scholar] [CrossRef] [PubMed]
- Peto, T.; Affron, D.; Afrough, B.; Agasu, A.; Ainsworth, M.; Allanson, A.; Allen, K.; Allen, C.; Archer, L.; Ashbridge, N.; et al. COVID-19: Rapid antigen detection for SARS-CoV-2 by lateral flow assay: A national systematic evaluation of sensitivity and specificity for mass-testing. EClinicalMedicine 2021, 36, 100924. [Google Scholar] [CrossRef] [PubMed]
- FDA. GenBody COVID-19 Ag Rapid Diagnostic Test for the Detection of SARS-CoV-2 Antigen. Available online: https://www.fda.gov/media/150788/download (accessed on 24 September 2022).
- Qasem, A.; Shaw, A.M.; Elkamel, E.; Naser, S.A. Coronavirus Disease 2019 (COVID-19) Diagnostic Tools: A Focus on Detection Technologies and Limitations. Curr. Issues Mol. Biol. 2021, 43, 728–748. [Google Scholar] [CrossRef]
- How Does the Cost of Rapid Testing in the US Compare to Other Countries? [Internet]. The Independent. 2022. Available online: https://www.independent.co.uk/news/world/americas/rapid-test-biden-free-mail-b1992860.html (accessed on 23 June 2022).
- Mistry, D.A.; Wang, J.Y.; Moeser, M.E.; Starkey, T.; Lee, L.Y. A systematic review of the sensitivity and specificity of lateral flow devices in the detection of SARS-CoV-2. BMC Infect. Dis. 2021, 21, 828. [Google Scholar] [CrossRef]
- Deerain, J.; Druce, J.; Tran, T.; Batty, M.; Yoga, Y.; Fennell, M.; Dwyer, D.E.; Kok, J.; Williamson, D.A. Assessment of the analytical sensitivity of ten lateral flow devices against the SARS-CoV-2 omicron variant. J. Clin. Microbiol. 2021, 60, e02479-21. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int. J. Surg. 2021, 88, 105906. [Google Scholar] [CrossRef]
- Joanna Briggs Institute. Joanna Briggs Institute Reviewers’ Manual: 2014 Edition; The Joanna Briggs institute: Adelaide, Australia, 2014; Volume 197. [Google Scholar]
- Bayart, J.L.; Degosserie, J.; Favresse, J.; Gillot, C.; Didembourg, M.; Djokoto, H.P.; Verbelen, V.; Roussel, G.; Maschietto, C.; Mullier, F.; et al. Analytical Sensitivity of Six SARS-CoV-2 Rapid Antigen Tests for Omicron versus Delta Variant. Viruses 2022, 14, 654. [Google Scholar] [CrossRef]
- Gourgeon, A.; Soulier, A.; Audureau, É.; Khouider, S.; Galbin, A.; Langlois, C.; Bouvier-Alias, M.; Rodriguez, C.; Chevaliez, S.; Pawlotsky, J.M.; et al. Performance of 22 Rapid Lateral Flow Tests for SARS-CoV-2 Antigen Detection and Influence of “Variants of Concern”: Implications for Clinical Use. Microbiol. Spectr. 2022, 10, e0115722. [Google Scholar] [CrossRef] [PubMed]
- Stanley, S.; Hamel, D.J.; Wolf, I.D.; Riedel, S.; Dutta, S.; Contreras, E.; Callahan, C.J.; Cheng, A.; Arnaout, R.; Kirby, J.E.; et al. Limit of Detection for Rapid Antigen Testing of the SARS-CoV-2 Omicron and Delta Variants of Concern Using Live-Virus Culture. J. Clin. Microbiol. 2022, 60, e00140-22. [Google Scholar] [CrossRef] [PubMed]
- Tsao, J.; Kussman, A.L.; Costales, C.; Pinsky, B.A.; Abrams, G.D.; Hwang, C.E. Accuracy of Rapid Antigen vs Reverse Transcriptase-Polymerase Chain Reaction Testing for SARS-CoV-2 Infection in College Athletes During Prevalence of the Omicron Variant. JAMA Netw Open 2022, 5, e2217234. [Google Scholar] [CrossRef]
- Weishampel, Z.A.; Young, J.; Fischl, M.; Fischer, R.J.; Donkor, I.O.; Riopelle, J.C.; Schulz, J.E.; Port, J.R.; Saturday, T.A.; van Doremalen, N.; et al. OraSure InteliSwab™ Rapid Antigen Test Performance with the SARS-CoV-2 Variants of Concern—Alpha, Beta, Gamma, Delta, and Omicron. Viruses 2022, 14, 543. [Google Scholar] [CrossRef] [PubMed]
- Adamson, B.J.; Sikka, R.; Wyllie, A.L.; Premsrirut, P.K. Discordant SARS-CoV-2 PCR and Rapid Antigen Test Results When Infectious: A December 2021 Occupational Case Series. medRxiv 2022. [Google Scholar] [CrossRef]
- Bekliz, M.; Adea, K.; Alvarez, C.; Essaidi-Laziosi, M.; Escadafal, C.; Kaiser, L.; Eckerle, I. Analytical sensitivity of seven SARS-CoV-2 antigen-detecting rapid tests for Omicron variant. medRxiv 2022. [Google Scholar] [CrossRef]
- Kanjilal, S.; Chalise, S.; Shah, A.S.; Cheng, C.A.; Senussi, Y.; Springer, M.; Walt, D.R. Analytic sensitivity of the Abbott BinaxNOW lateral flow immunochromatographic assay for the SARS-CoV-2 Omicron variant. medRxiv 2022. [Google Scholar] [CrossRef]
- Schrom, J.; Marquez, C.; Pilarowski, G.; Wang, G.; Mitchell, A.; Puccinelli, R.; Black, D.; Rojas, S.; Riberio, S.; Martinez, J.; et al. Direct Comparison of SARS Co-V-2 Nasal RT-PCR and Rapid Antigen Test (BinaxNOW (TM)) at a Community Testing Site During an Omicron Surge. medRxiv 2022. [Google Scholar] [CrossRef]
- Belogiannis, K.; Florou, V.A.; Fragkou, P.C.; Ferous, S.; Chatzis, L.; Polyzou, A.; Lagopati, N.; Vassilakos, D.; Kittas, C.; Tzioufas, A.G.; et al. SARS-CoV-2 Antigenemia as a Confounding Factor in Immunodiagnostic Assays: A Case Study. Viruses 2021, 13, 1143. [Google Scholar] [CrossRef]
- Chin, E.T.; Huynh, B.Q.; Chapman, L.A.; Murrill, M.; Basu, S.; Lo, N.C. Frequency of routine testing for coronavirus disease 2019 (COVID-19) in high-risk healthcare environments to reduce outbreaks. Clin. Infect. Dis. 2021, 73, e3127-9. [Google Scholar] [CrossRef]
- Backer, J.A.; Eggink, D.; Andeweg, S.P.; Veldhuijzen, I.K.; van Maarseveen, N.; Vermaas, K.; Vlaemynck, B.; Schepers, R.; van den Hof, S.; Reusken, C.B.; et al. Shorter serial intervals in SARS-CoV-2 cases with Omicron BA.1 variant compared with Delta variant, the Netherlands, 13 to 26 December 2021. Eurosurveillance 2022, 27, 2200042. [Google Scholar] [CrossRef] [PubMed]
- Juanola-Falgarona, M.; Peñarrubia, L.; Jiménez-Guzmán, S.; Porco, R.; Congost-Teixidor, C.; Varo-Velázquez, M.; Rao, S.N.; Pueyo, G.; Manissero, D.; Pareja, J. Ct values as a diagnostic tool for monitoring SARS-CoV-2 viral load using the QIAstat-Dx® Respiratory SARS-CoV-2 Panel. Int. J. Infect. Dis. 2022, 122, 930–935. [Google Scholar] [CrossRef] [PubMed]
- Platten, M.; Hoffmann, D.; Grosser, R.; Wisplinghoff, F.; Wisplinghoff, H.; Wiesmüller, G.; Schildgen, O.; Schildgen, V. SARS-CoV-2, CT-Values, and Infectivity-Conclusions to Be Drawn from Side Observations. Viruses 2021, 13, 1459. [Google Scholar] [CrossRef] [PubMed]
- Rathinasamy, M.; Kandhasamy, S. An exploratory study on the propagation of SARS-CoV-2 variants: Omicron is the most predominant variant. J. Med. Virol. 2022, 94, 2414–2421. [Google Scholar] [CrossRef] [PubMed]
- Gottlieb, R.L.; Vaca, C.E.; Paredes, R.; Mera, J.; Webb, B.J.; Perez, G.; Oguchi, G.; Ryan, P.; Nielsen, B.U.; Brown, M.; et al. Early remdesivir to prevent progression to severe Covid-19 in outpatients. N. Engl. J. Med. 2022, 386, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Hammond, J.; Leister-Tebbe, H.; Gardner, A.; Abreu, P.; Bao, W.; Wisemandle, W.; Baniecki, M.; Hendrick, V.M.; Damle, B.; Simón-Campos, A.; et al. Oral nirmatrelvir for high-risk, nonhospitalized adults with COVID-19. N. Engl. J. Med. 2022, 386, 1397–1408. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Antigen-Detection in the Diagnosis of SARS-CoV-2 Infection, Interim Guidance. 2021 Oct. Available online: https://www.who.int/publications/i/item/antigen-detection-in-the-diagnosis-of-sars-cov-2infection-using-rapid-immunoassays (accessed on 23 September 2022).
- Lee, R.A.; Herigon, J.C.; Benedetti, A.; Pollock, N.R.; Denkinger, C.M. Performance of saliva, oropharyngeal swabs, and nasal swabs for SARS-CoV-2 molecular detection: A systematic review and meta-analysis. J. Clin. Microbiol. 2021, 59, e02881-20. [Google Scholar] [CrossRef]
- Nalumansi, A.; Lutalo, T.; Kayiwa, J.; Watera, C.; Balinandi, S.; Kiconco, J.; Nakaseegu, J.; Olara, D.; Odwilo, E.; Serwanga, J.; et al. Field evaluation of the performance of a SARS-CoV-2 antigen rapid diagnostic test in Uganda using nasopharyngeal samples. Int. J. Infect. Dis. 2021, 104, 282–286. [Google Scholar] [CrossRef]
- Savage, H.R.; Finch, L.; Body, R.; Watkins, R.L.; LSTM Diagnostics Group; CONDOR Steering Group; Hayward, G.; Cook, E.; Cubas-Atienzar, A.I.; Cuevas, L.E.; et al. A prospective diagnostic evaluation of accuracy of self-taken and healthcare worker-taken swabs for rapid COVID-19 testing. PLoS ONE 2022, 17, e0270715. [Google Scholar] [CrossRef]
- Higgins, T.S.; Wu, A.W.; Ting, J.Y. SARS-CoV-2 Nasopharyngeal Swab Testing-False-Negative Results from a Pervasive Anatomical Misconception. JAMA Otolaryngol. Head Neck Surg. 2020, 146, 993–994. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Study | Type of Lateral Flow Tests | Type of Swab Sample | Sample Size | Key Findings | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Adamson, 2022 [18] † |
| Anterior nasal | n = 30 |
| |||||||
| Bayart, 2022 [13] |
| Nasopharyngeal | n = 60 |
| |||||||
| Population | Variant | Clinitest | New-Gene | Boson | Flowflex | Sejoy | Roche | ||||
| Ct ≤ 25 | Delta | 95.6 (84.9–99.5) | 95.6 (84.9–99.5) | 97.8 (88.2–99.9) | 97.8 (88.2–99.9) | 95.6 (84.9–99.5) | 100 (92.1–100) | ||||
| Omicron | 94.1 (80.3–99.3) | 97.1 (84.7–99.9) | 97.1 (84.7–99.9) | 91.2 (76.3–98.1) | 97.1 (84.7–99.9) | 100 (89.4–100) | |||||
| Ct ≥ 25 | Delta | 32.0 (15.0–53.5) | 40.0 (21.1–61.3) | 40.0 (21.1–61.3) | 20.0 (6.8–40.7) | 36.0 (18.0–57.5) | 80.0 (59.3–93.2) | ||||
| Delta | 32.0 (15.0–53.5) | 40.0 (21.1–61.3) | 40.0 (21.1–61.3) | 20.0 (6.8–40.7) | 36.0 (18.0–57.5) | 80.0 (59.3–93.2) | |||||
| Bekliz, 2022 [19] † |
| Nasopharyngeal | n = 18 |
| |||||||
| Brand | Omicron | Delta | p value | ||||||||
| Panbio | 36.1% | 67.6% | < 0.001 | ||||||||
| Standard Q | 22.2% | 52.9% | < 0.001 | ||||||||
| Sure Status | 27.8% | 52.9% | < 0.001 | ||||||||
| Onsite | 47.2% | 64.7% | < 0.001 | ||||||||
| Wondfo | 75.0% | 76.5% | 0.984 | ||||||||
| Tigsun | 47.2% | 52.9% | 0.634 | ||||||||
| Wondfo | 75.0% | 76.5% | 0.984 | ||||||||
| Deerain, 2021 [10] |
| In vitro study; cell cultures | Not applicable |
| |||||||
| Gourgeon, 2022 [14] |
| Nasopharyngeal | n = 179 |
| |||||||
| Brand | Omicron (BA.1) | Delta | Alpha | ||||||||
| AAZ-LMB | 70.0 (55.4–82.1) | 88.9 (77.4–95.8) | 88.9 (77.4–95.8) | ||||||||
| AMP | 70.0 (55.4–82.1) | 90.7 (79.7–96.9) | 90.7 (79.7–96.9) | ||||||||
| Novel | 70.0 (55.4–82.1) | 86.5 (74.2–94.4) | 86.5 (74.2–94.4) | ||||||||
| Biospeedia | 70.0 (55.4–82.1) | 88.5 (76.6–95.6) | 88.5 (76.6–95.6) | ||||||||
| R-Biopharm | 58.0 (43.2–71.8) | 86.0 (73.3–94.2) | 86.0 (73.3–94.2) | ||||||||
| Siemens | 68.0 (53.3–80.5) | 88.9 (77.4–95.8) | 88.9 (77.4–95.8) | ||||||||
| Abbott | 56.0 (41.3–70.0) | 77.4 (63.8–97.7) | 77.4 (63.8–87.7) | ||||||||
| Biosynex | 58.0 (43.2–71.8) | 87.0 (75.1–94.6) | 87.0 (75.1–94.6) | ||||||||
| Reported test sensitivities for Ct ≤30 (95% CI): | |||||||||||
| Brand | Omicron (BA.1) | Delta | Alpha | ||||||||
| AAZ-LMB | 89.5 (75.2–97.1) | 81.5 (68.6–90.7) | 92.3 (81.5–97.9 | ||||||||
| AMP | 92.1 (78.6–98.3) | 92.6 (82.1–97.9) | 94.2 (84.1–98.8) | ||||||||
| Novel | 89.5 (75.2–97.1) | 87.0 (75.1–94.6) | 90.0 (78.2–96.7) | ||||||||
| Biospeedia | 89.5 (75.2–97.1) | 88.9 (77.4–95.8) | 92.0 (80.8–97.8) | ||||||||
| R-Biopharm | 73.7 (56.9–86.6) | 77.8 (64.4–88.0) | 87.5 (74.8–95.3) | ||||||||
| Siemens | 86.8 (71.9–95.6) | 85.2 (72.9–93.4) | 92.3 (81.5–97.9) | ||||||||
| Abbott | 71.1 (54.1–84.6) | 75.9 (62.4–86.5) | 80.4 (66.9–90.2) | ||||||||
| Biosynex | 73.7 (56.9–86.6) | 83.3 (70.7–92.1) | 90.4 (79.0–96.8) | ||||||||
| Kanjilal, 2022 [20] † |
| Anterior nasal | n = 32 |
| |||||||
| Schrom, 2022 [21] † |
| Anterior nasal, cheek and oral tonsillar | n = 296 (98.5% of a random sample of 75 persons were found to have the omicron variant) |
| |||||||
| Ct cutoff | Sensitivity (95% CI) | Specificity (95% CI) | |||||||||
| 30 | 95.2% (91.0–97.8%) | 96.5% (94.6–97.9%) | |||||||||
| 35 | 82.1% (76.6–86.8%) | 99.4% (98.2–99.9%) | |||||||||
| No cutoff | 65.2% (59.5–70.6%) | 99.3% (98.0–99.9%) | |||||||||
| Stanley, 2022 [15] |
| In vitro study; live-virus culture | Not applicable |
| |||||||
| Brand | Omicron | Delta | |||||||||
| Abbott | 8.3 × 101 | 1.0 × 104 | |||||||||
| Access Bio | 2.8 × 103 | 3.5 × 103 | |||||||||
| GenBody | 2.5 × 102 | 3.5 × 104 | |||||||||
| Tsao, 2022 [16] |
| Not specified; self-administered | n = 723 (95.7% (44 out of 46) positive cases were found to have the omicron variant) |
| |||||||
| Weishampel, 2022 [17] |
| Live virus cultures and oropharyngeal swabs from hamsters inoculated with SARS-CoV-2 | Not applicable |
| |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ng, Q.X.; Lim, Y.L.; Han, M.X.; Teoh, S.E.; Thumboo, J.; Tan, B.H. The Performance of Lateral Flow Tests in the Age of the Omicron: A Rapid Systematic Review. Life 2022, 12, 1941. https://doi.org/10.3390/life12111941
Ng QX, Lim YL, Han MX, Teoh SE, Thumboo J, Tan BH. The Performance of Lateral Flow Tests in the Age of the Omicron: A Rapid Systematic Review. Life. 2022; 12(11):1941. https://doi.org/10.3390/life12111941
Chicago/Turabian StyleNg, Qin Xiang, Yu Liang Lim, Ming Xuan Han, Seth En Teoh, Julian Thumboo, and Ban Hock Tan. 2022. "The Performance of Lateral Flow Tests in the Age of the Omicron: A Rapid Systematic Review" Life 12, no. 11: 1941. https://doi.org/10.3390/life12111941