
Human Papillomavirus (HPV) Infection and Its Impact on Male Infertility
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Sample Collection
2.2. DNA Extraction
2.3. Detection and Type Identification of HPVs
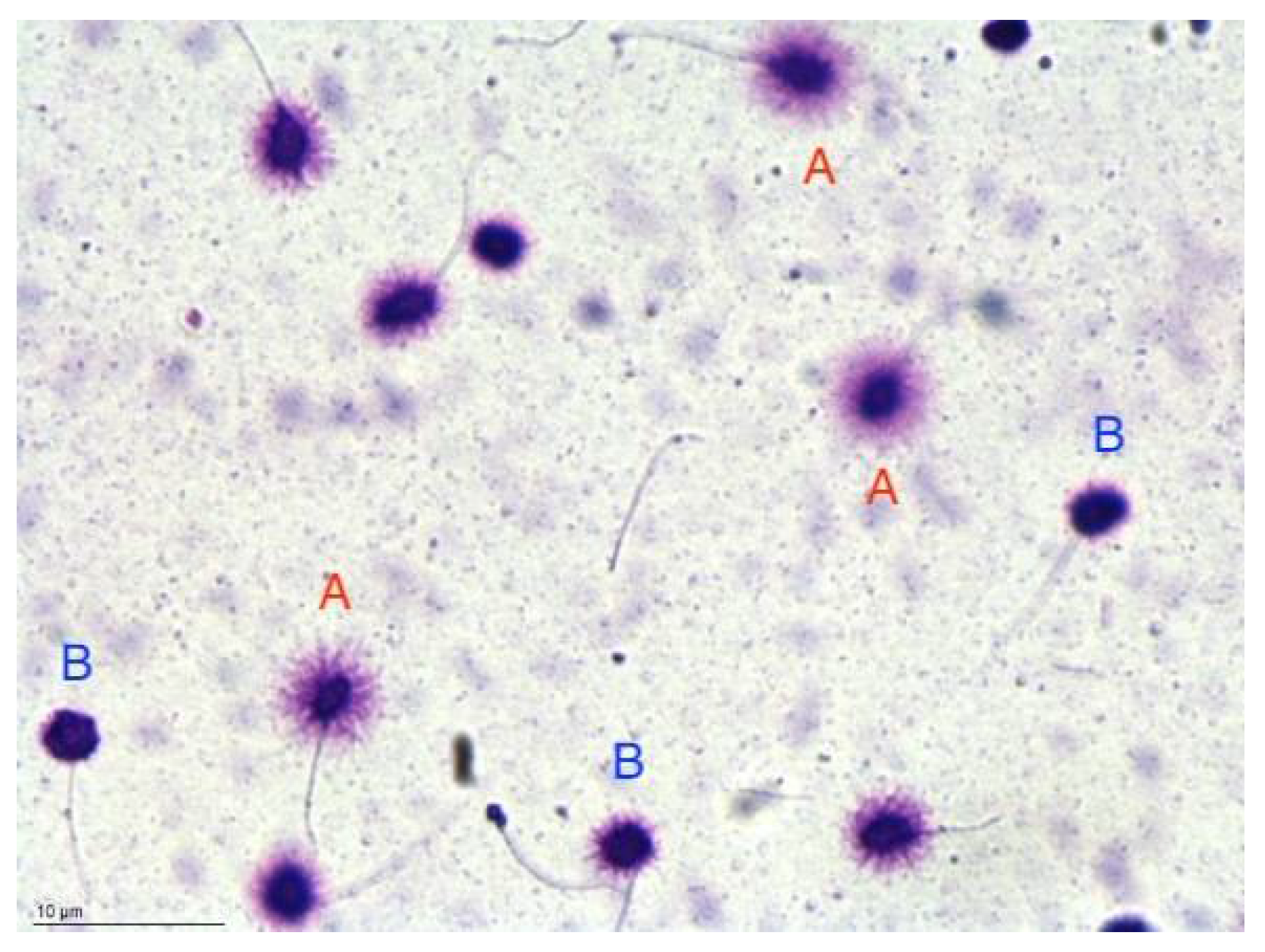
2.4. Sperm DNA Fragmentation Analysis by SCD Test
2.5. Statistical Analysis
3. Results
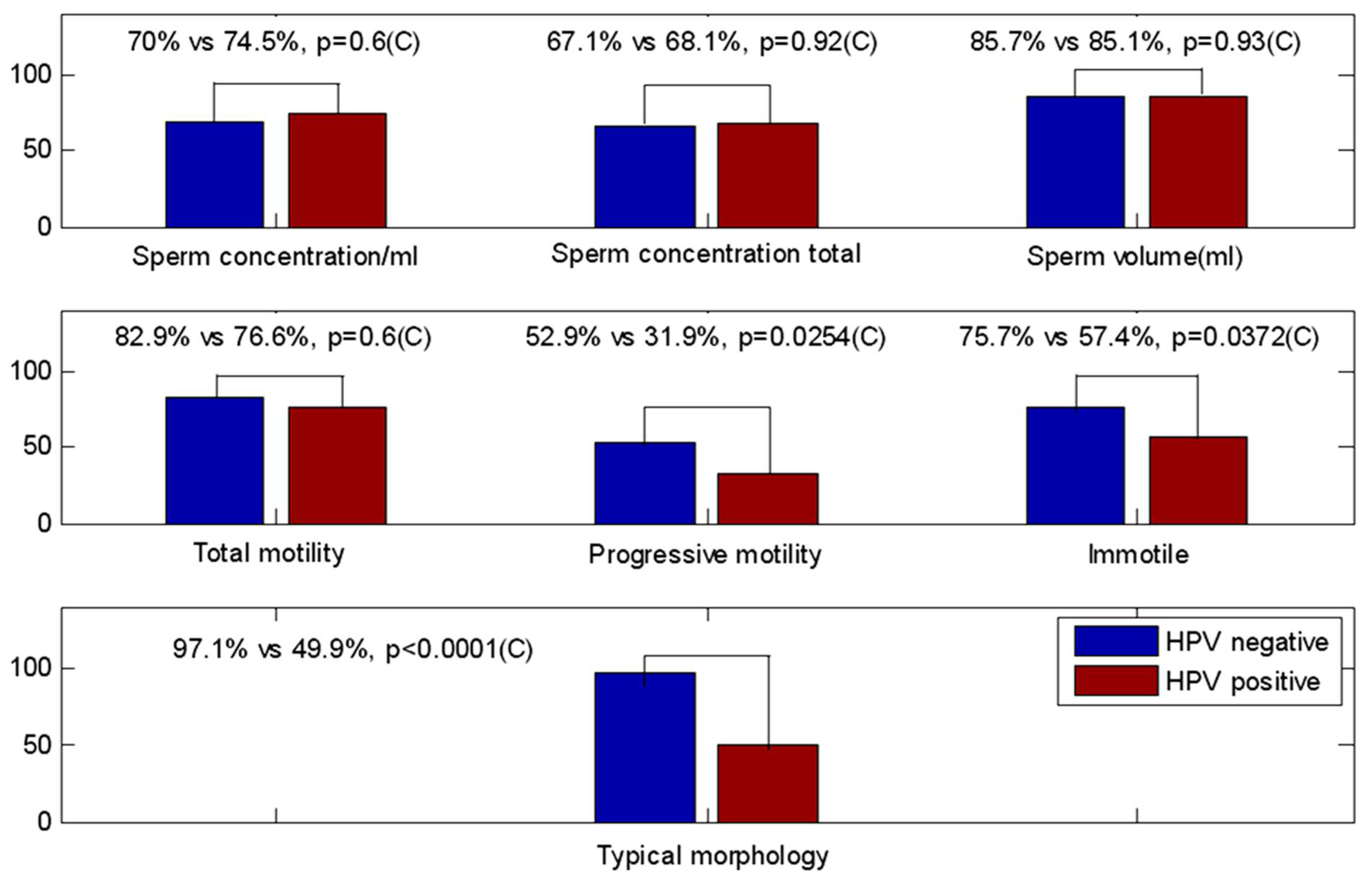
3.1. Seminal Parameters: HPV-Negative vs. HPV-Positive Samples
3.2. Seminal Sample’s Parameter Compared with Lower Reference Limits (Fifth Centiles WHO 2010)
3.3. Seminal Parameters of HPV-Positive Patients Stratified in Low and High Risk
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. International Classification of Diseases, 11th Revision (ICD-11). 2018. Available online: https://icd.who.int/en (accessed on 14 November 2022).
- Agarwal, A.; Mulgund, A.; Hamada, A.; Chyatte, M.R. A unique view on male infertility around the globe. Reprod. Biol. Endocrinol. 2015, 13, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cannarella, R.; Gül, M.; Rambhatla, A.; Agarwal, A. Temporal decline of sperm concentration: Role of endocrine disruptors. Endocrine 2022, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Caliskan, Z.; Kucukgergin, C.; Aktan, G.; Kadioglu, A.; Ozdemirler, G. Evaluation of sperm DNA fragmentation in male infertility. Andrologia 2022, e14587. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Laboratory Manual for the Examination and Processing of Human Semen, 5th ed.; WHO: Lyon, France, 2010; Volume 17, pp. 1059–1063. [Google Scholar]
- Yang, H.; Li, G.; Jin, H.; Guo, Y.; Sun, Y. The effect of sperm DNA fragmentation index on assisted reproductive technology outcomes and its relationship with semen parameters and lifestyle. Transl. Androl. Urol. 2019, 8, 356–365. [Google Scholar] [CrossRef]
- Elisabetta Baldi, M.M. Genetic Damage in Human Spermatozoa; Springer International Publishing: Cham, Switzerland, 2019; ISBN 9783030216634. [Google Scholar]
- Chesson, H.W.; Dunne, E.F.; Hariri, S.; Markowitz, L.E. The estimated lifetime probability of acquiring human papillomavirus in the United States. Sex. Transm. Dis. 2014, 41, 660–664. [Google Scholar] [CrossRef]
- Graham, S.V. The human papillomavirus replication cycle, and its links to cancer progression: A comprehensive review. Clin. Sci. 2017, 131, 2201–2221. [Google Scholar] [CrossRef] [Green Version]
- Radley, D.; Saah, A.; Stanley, M. Persistent infection with human papillomavirus 16 or 18 is strongly linked with high-grade cervical disease. Hum. Vaccines Immunother. 2016, 12, 768–772. [Google Scholar] [CrossRef] [Green Version]
- Kombe Kombe, A.J.; Li, B.; Zahid, A.; Mengist, H.M.; Bounda, G.A.; Zhou, Y.; Jin, T. Epidemiology and Burden of Human Papillomavirus and Related Diseases, Molecular Pathogenesis, and Vaccine Evaluation. Front. Public Health 2021, 8, 552028. [Google Scholar] [CrossRef]
- de Sanjosé, S.; Diaz, M.; Castellsagué, X.; Clifford, G.; Bruni, L.; Nubia Muñoz, F.X.B. Worldwide prevalence and genotype distribution of cervical human papillomavirus DNA in women with normal cytology: A meta-analysis. Lancet Infect. Dis. 2007, 7, 453–459. [Google Scholar] [CrossRef]
- Giovannelli, L.; Migliore, M.C.; Capra, G.; Caleca, M.P.; Bellavia, C.; Perino, A.; Viviano, E.; Matranga, D.; Ammatuna, P. Penile, urethral, and seminal sampling for diagnosis of human papillomavirus infection in men. J. Clin. Microbiol. 2007, 45, 248–251. [Google Scholar] [CrossRef]
- Gheit, T. Mucosal and cutaneous human papillomavirus infections and cancer biology. Front. Oncol. 2019, 9, 355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capra, G.; Nyitray, A.G.; Lu, B.; Perino, A.; Marci, R.; Schillaci, R.; Matranga, D.; Firenze, A.; Caleca, M.; Bellavia, C.; et al. Analysis of persistence of human papillomavirus infection in men evaluated by sampling multiple genital sites. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 4153–4163. [Google Scholar] [PubMed]
- Rintala, M.A.M.; Pöllänen, P.P.; Nikkanen, V.P.; Grénman, S.E.; Syrjänen, S.M. Human papillomavirus DNA is found in the vas deferens. J. Infect. Dis. 2002, 185, 1664–1667. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Švec, A.; Mikyšková, I.; Hes, O.; Tachezy, R. Human Papillomavirus Infection of the Epididymis and Ductus Deferens: An Evaluation by Nested Polymerase Chain Reaction. Arch. Pathol. Lab. Med. 2003, 127, 1471–1474. [Google Scholar] [CrossRef] [PubMed]
- Martorell, M.; Gil-Salom, M.; Pérez-Vallés, A.; Garcia, J.A.; Rausell, N.; Senpere, A. Presence of human papillomavirus DNA in testicular biopsies from nonobstructive azoospermic men. Arch. Pathol. Lab. Med. 2005, 129, 1132–1136. [Google Scholar] [CrossRef]
- Kato, Y.; Shigehara, K.; Nakagawa, T.; Nakata, H.; Iijima, M.; Nakashima, K.; Kawaguchi, S.; Izumi, K.; Kadono, Y.; Mizokami, A. Human papillomavirus detected in sperm of Japanese infertile males affects reproductive parameters. Int. J. Infect. Dis. 2021, 112, 294–299. [Google Scholar] [CrossRef] [PubMed]
- Bosco, L.; Serra, N.; Fasciana, T.; Pistoia, D.; Vella, M.; Di Gregorio, L.; Schillaci, R.; Perino, A.; Calagna, G.; Firenze, A.; et al. Potential impact of a nonavalent anti HPV vaccine in Italian men with and without clinical manifestations. Sci. Rep. 2021, 11, 4096. [Google Scholar] [CrossRef]
- Foresta, C.; Noventa, M.; De Toni, L.; Gizzo, S.; Garolla, A. HPV-DNA sperm infection and infertility: From a systematic literature review to a possible clinical management proposal. Andrology 2015, 3, 163–173. [Google Scholar] [CrossRef]
- Garolla, A.; Engl, B.; Pizzol, D.; Ghezzi, M.; Bertoldo, A.; Bottacin, A.; Noventa, M.; Foresta, C. Spontaneous fertility and in vitro fertilization outcome: New evidence of human papillomavirus sperm infection. Fertil. Steril. 2016, 105, 65–72.e1. [Google Scholar] [CrossRef] [Green Version]
- Zacharis, K.; Messini, C.I.; Anifandis, G.; Koukoulis, G.; Satra, M.; Daponte, A. Human papilloma virus (HPV) and fertilization: A mini review. Medicina 2018, 54, 50. [Google Scholar] [CrossRef]
- Perino, A.; Giovannelli, L.; Schillaci, R.; Ruvolo, G.; Fiorentino, F.P.; Alimondi, P.; Cefal, E.; Ammatuna, P. Human papillomavirus infection in couples undergoing in vitro fertilization procedures: Impact on reproductive outcomes. Fertil. Steril. 2011, 95, 1845–1848. [Google Scholar] [CrossRef] [PubMed]
- Foresta, C.; Patassini, C.; Bertoldo, A.; Menegazzo, M.; Francavilla, F.; Barzon, L.; Ferlin, A. Mechanism of human papillomavirus binding to human spermatozoa and fertilizing ability of infected spermatozoa. PLoS ONE 2011, 6, e15036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérez-Andino, J.; Buck, C.B.; Ribbeck, K. Adsorption of Human Papillomavirus 16 to Live Human Sperm. PLoS ONE 2009, 4, e5847. [Google Scholar] [CrossRef] [PubMed]
- Depuydt, C.E.; Donders, G.G.G.; Verstraete, L.; Broeck, D.V.; Beert, J.F.A.; Salembier, G.; Bosmans, E.; DhontT, N.; van der Auwera, I.; Vandenborne, K.; et al. Time has come to include Human Papillomavirus (HPV) testing in sperm donor banks. Facts Views Vis. ObGyn 2018, 10, 201–205. [Google Scholar]
- Wang, S.; Liu, L.; Zhang, A.; Song, Y.; Kang, J.; Liu, X. Association between human papillomavirus infection and sperm quality: A systematic review and a meta-analysis. Andrologia 2021, 53, e14034. [Google Scholar] [CrossRef]
- Fedder, J.; Ørnskov, D.; Engvad, B.; Kristensen, T.K.; Lomholt, M.; Marcussen, N.; Waldström, M. Seminal human papillomavirus originates from the body surface and is not a frequent aetiological factor in azoospermia. Andrologia 2019, 51, e13202. [Google Scholar] [CrossRef] [Green Version]
- Golob, B.; Poljak, M.; Verdenik, I.; Kolbezen Simoniti, M.; Vrtačnik Bokal, E.; Zorn, B. High HPV infection prevalence in men from infertile couples and lack of relationship between seminal HPV infection and sperm quality. BioMed Res. Int. 2014, 2014. [Google Scholar] [CrossRef] [Green Version]
- Jaworek, H.; Koudelakova, V.; Oborna, I.; Zborilova, B.; Brezinova, J.; Ruzickova, D.; Vrbkova, J.; Kourilova, P.; Hajduch, M. Impact of human papillomavirus infection on semen parameters and reproductive outcomes. Reprod. Biol. Endocrinol. 2021, 19, 156. [Google Scholar] [CrossRef]
- Weinberg, M.; Sar-Shalom Nahshon, C.; Feferkorn, I.; Bornstein, J. Evaluation of human papilloma virus in semen as a risk factor for low sperm quality and poor in vitro fertilization outcomes: A systematic review and meta-analysis. Fertil. Steril. 2020, 113, 955–969.e4. [Google Scholar] [CrossRef]
- Foresta, C.; Pizzol, D.; Moretti, A.; Barzon, L.; Pal, G.; Garolla, A. Clinical and prognostic significance of human papillomavirus DNA in the sperm or exfoliated cells of infertile patients and subjects with risk factors. Fertil. Steril. 2010, 94, 1723–1727. [Google Scholar] [CrossRef]
- Schillaci, R.; Capra, G.; Bellavia, C.; Ruvolo, G.; Scazzone, C.; Venezia, R.; Perino, A. Detection of oncogenic human papillomavirus genotypes on spermatozoa from male partners of infertile couples. Fertil. Steril. 2013, 100, 1236–1240. [Google Scholar] [CrossRef] [PubMed]
- Garolla, A.; Pizzol, D.; Bertoldo, A.; De Toni, L.; Barzon, L.; Foresta, C. Association, prevalence, and clearance of human papillomavirus and antisperm antibodies in infected semen samples from infertile patients. Fertil. Steril. 2013, 99, 125–131.e2. [Google Scholar] [CrossRef]
- Piroozmand, A.; Nasab, S.D.M.; Erami, M.; Hashemi, S.M.A.; Khodabakhsh, E.; Ahmadi, N.; Vahedpoor, Z. Distribution of human papillomavirus and antisperm antibody in semen and its association with semen parameters among infertile men. J. Reprod. Infertil. 2020, 21, 183–188. [Google Scholar]
- Brossfield, J.E.; Chan, P.J.; Patton, W.C.; King, A. Tenacity of exogenous human papillomavirus DNA in sperm washing. J. Assist. Reprod. Genet. 1999, 16, 325–328. [Google Scholar] [CrossRef] [PubMed]
- Gizzo, S.; Ferrari, B.; Noventa, M.; Ferrari, E.; Patrelli, T.S.; Gangemi, M.; Nardelli, G.B. Male and couple fertility impairment due to HPV-DNA sperm infection: Update on molecular mechanism and clinical impact—Systematic review. BioMed Res. Int. 2014, 2014, 20–22. [Google Scholar] [CrossRef]
- Connelly, D.A.; Chan, P.J.; Patton, W.C.; King, A. Human sperm deoxyribonucleic acid fragmentation by specific types of papillomavirus. Am. J. Obstet. Gynecol. 2001, 184, 1068–1070. [Google Scholar] [CrossRef]
- Lee, C.A.; Huang, C.T.F.; King, A.; Chan, P.J. Differential effects of human papillomavirus DNA types on p53 tumor-suppressor gene apoptosis in sperm. Gynecol. Oncol. 2002, 85, 511–516. [Google Scholar] [CrossRef] [Green Version]
- Kaspersen, M.D.; Bungum, M.; Fedder, J.; Bonde, J.; Larsen, P.B.; Ingerslev, H.J.; Höllsberg, P. No increased sperm DNA fragmentation index in semen containing human papillomavirus or herpesvirus. Andrology 2013, 1, 361–364. [Google Scholar] [CrossRef]
- Cortés-Gutiérrez, E.I.; Dávila-Rodríguez, M.I.; Fernández, J.L.; de la O-Pérez, L.O.; Garza-Flores, M.E.; Eguren–Garza, R.; Gosálvez, J. The presence of human papillomavirus in semen does not affect the integrity of sperm DNA. Andrologia 2017, 49, e12774. [Google Scholar] [CrossRef]
- Boeri, L.; Capogrosso, P.; Ventimiglia, E.; Pederzoli, F.; Cazzaniga, W.; Chierigo, F.; Pozzi, E.; Clementi, M.; Viganò, P.; Montanari, E.; et al. High-risk human papillomavirus in semen is associated with poor sperm progressive motility and a high sperm DNA fragmentation index in infertile men. Hum. Reprod. 2019, 34, 209–217. [Google Scholar] [CrossRef]
- Tangal, S.; Taşçı, Y.; Pabuçcu, E.G.; Çağlar, G.S.; Haliloğlu, A.H.; Yararbaş, K. DNA fragmentation index and human papilloma virus in males with previous assisted reproductive technology failures. Turk. J. Urol. 2019, 45, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Depuydt, C.E.; Beert, J.; Bosmans, E.; Salembier, G. Human Papillomavirus (HPV) virion induced cancer and subfertility, two sides of the same coin. Facts Views Vis. Obstet. Gynaecol. 2016, 8, 211–222. [Google Scholar]
- Depuydt, C.E.; Donders, G.G.G.; Verstraete, L.; Vanden Broeck, D.; Beert, J.F.A.; Salembier, G.; Bosmans, E.; Ombelet, W. Infectious human papillomavirus virions in semen reduce clinical pregnancy rates in women undergoing intrauterine insemination. Fertil. Steril. 2019, 111, 1135–1144. [Google Scholar] [CrossRef] [PubMed]
- Luttmer, R.; Dijkstra, M.G.; Snijders, P.J.F.; Hompes, P.G.A.; Pronk, D.T.M.; Hubeek, I.; Berkhof, J.; Heideman, D.A.M.; Meijer, C.J.L.M. Presence of human papillomavirus in semen in relation to semen quality. Hum. Reprod. 2016, 31, 280–286. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The World Medical Association Inc. World Medical Association Declaration of Helsinki, Ethical Principles for Medical Research Involving Human Subjects. Bull. World Health Organ. 2001, 79, 373. [Google Scholar]
- IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Biological Agents, Vol. 100B, Human Papillomaviruses; International Agency for Research on Cancer: Geneva, Switzerland, 2012; pp. 255–295. [Google Scholar]
- Fernández, J.L.; Muriel, L.; Rivero, M.T.; Goyanes, V.; Vazquez, R.; Alvarez, J.G. The sperm chromatin dispersion test: A simple method for the determination of sperm DNA fragmentation. J. Androl. 2003, 24, 59–66. [Google Scholar]
- Bosco, L.; Notari, T.; Ruvolo, G.; Roccheri, M.C.; Martino, C.; Chiappetta, R.; Carone, D.; Lo Bosco, G.; Carrillo, L.; Raimondo, S.; et al. Sperm DNA fragmentation: An early and reliable marker of air pollution. Environ. Toxicol. Pharmacol. 2018, 58, 243–249. [Google Scholar] [CrossRef]
- Leslie, S.W.; Siref, L.E.; Soon-Sutton, T.L.; Khan, M.A.B. Male Infertility. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Moreno-Sepulveda, J.; Rajmil, O. Seminal human papillomavirus infection and reproduction: A systematic review and meta-analysis. Andrology 2021, 9, 478–502. [Google Scholar] [CrossRef]
- Rintala, M.A.M.; Grénman, S.E.; Pöllänen, P.P.; Suominen, J.J.O.; Syrjänen, S.M. Detection of high-risk HPV DNA in semen and its association with the quality of semen. Int. J. STD AIDS 2004, 15, 740–743. [Google Scholar] [CrossRef]
- Foresta, C.; Garolla, A.; Zuccarello, D.; Pizzol, D.; Moretti, A.; Barzon, L.; Palù, G. Human papillomavirus found in sperm head of young adult males affects the progressive motility. Fertil. Steril. 2010, 93, 802–806. [Google Scholar] [CrossRef]
- Moghimi, M.; Zabihi-Mahmoodabadi, S.; Kheirkhah-Vakilabad, A.; Kargar, Z. Significant correlation between high-risk hpv dna in semen and impairment of sperm quality in infertile men. Int. J. Fertil. Steril. 2019, 12, 306–309. [Google Scholar] [CrossRef]
- Yang, Y.; Jia, C.W.; Ma, Y.M.; Zhou, L.Y.; Wang, S.Y. Correlation between HPV sperm infection and male infertility. Asian J. Androl. 2013, 15, 529–532. [Google Scholar] [CrossRef] [Green Version]
- Bungum, M.; Humaidan, P.; Axmon, A.; Spano, M.; Bungum, L.; Erenpreiss, J.; Giwercman, A. Sperm DNA integrity assessment in prediction of assisted reproduction technology outcome. Hum. Reprod. 2007, 22, 174–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruvolo, G.; Fattouh, R.R.; Bosco, L.; Brucculeri, A.M.; Cittadini, E. New molecular markers for the evaluation of gamete quality. J. Assist. Reprod. Genet. 2013, 30, 207–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agarwal, A.; Majzoub, A.; Esteves, S.C.; Ko, E.; Ramasamy, R.; Zini, A. Clinical utility of sperm DNA fragmentation testing: Practice recommendations based on clinical scenarios. Transl. Androl. Urol. 2016, 5, 935–950. [Google Scholar] [CrossRef]
- Esteves, S.C.; Agarwal, A.; Majzoub, A. Live birth must be the primary reproductive endpoint in IVF/ICSI studies evaluating sperm DNA fragmentation testing. Transl. Androl. Urol. 2017, 6, S564–S565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gallegos, G.; Ramos, B.; Santiso, R.; Goyanes, V.; Gosálvez, J.; Fernández, J.L. Sperm DNA fragmentation in infertile men with genitourinary infection by Chlamydia trachomatis and Mycoplasma. Fertil. Steril. 2008, 90, 328–334. [Google Scholar] [CrossRef] [PubMed]
- Satta, A.; Stivala, A.; Garozzo, A.; Morello, A.; Perdichizzi, A.; Vicari, E.; Salmeri, M.; Calogero, A.E. Experimental Chlamydia trachomatis infection causes apoptosis in human sperm. Hum. Reprod. 2006, 21, 134–137. [Google Scholar] [CrossRef] [Green Version]
- Kang, X.J.; Xie, Q.D.; Zhou, X.L.; Li, F.Z.; Huang, J.H.; Liu, D.L.; Huang, T.H. Effects of hepatitis B virus S protein exposure on sperm membrane integrity and functions. PLoS ONE 2012, 7, e33471. [Google Scholar] [CrossRef] [Green Version]
- Capra, G.; Schillaci, R.; Bosco, L.; Roccheri, M.C.; Perino, A.; Ragusa, M.A. HPV infection in semen: Results from a new molecular approach. Epidemiol. Infect. 2019, 147, E177. [Google Scholar] [CrossRef] [Green Version]
- ESHRE Guideline Group on Viral Infection/Disease; Mocanu, E.; Drakeley, A.; Kupka, M.S.; Lara-Molina, E.E.; le Clef, N.; Ombelet, W.; Patrat, C.; Pennings, G.; Semprini, A.E.; et al. ESHRE guideline: Medically assisted reproduction in patients with a viral infection/disease. Hum. Reprod. Open 2021, 2021. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Parameters | Total | HPV Negative | HPV Positive | HPV-Negative vs. Positive p-Value (Test) |
|---|---|---|---|---|
| Patients | 117 | 70 | 47 | |
| DFI% | 28.7 ± 12.9 | 28.5 ± 14.3 | 28.9 ± 10.6 | |
| 27.5 (20–35) | 25.1 (19–33.75) | 28.5 (23.65–35.5) | p = 0.32 (MW) | |
| Sperm concentration/mL | 45.0 ± 47.6 | 49.6 ± 51.9 | 38.3 ± 40.0 | |
| 30 (13–58) | 30 (8.5–70) | 29 (14.5–52) | p = 0.41 (MW) | |
| Total sperm number | 120.7 ± 137.1 | 123.5 ± 144.9 | 116.5 ± 125.9 | |
| 73.6 (26–153) | 75 (23.5–149.8) | 68.2 (30.85–157.5) | p = 0.95(MW) | |
| Semen volume (mL) | 2.9 ± 1.6 | 2.8 ± 1.6 | 3.0 ± 1.7 | |
| 2.7 (1.8–3.5) | 2.5 (1.7–3.2) | 3 (2–4) | p = 0.36 (MW) | |
| Progressive motility% | 28.8 ± 15.3 | 29.6 ± 15.0 | 27.7 ± 15.8 | |
| 30 (20–40) | 35 (20–40) | 25 (20–36.5) | p = 0.21 (MW) | |
| Non-progressive% | 16.2 ± 9.4 | 16.4 ± 10.4 | 16.0 ± 7.6 | |
| 15 (10–20) | 13.5 (10–20) | 15 (10–20) | p = 0.68 (MW) | |
| Total motility% | 45.0 ± 16.4 | 46.0 ± 16.8 | 43.7 ± 15.9 | |
| 50 (40–55) | 50 (40.75–55) | 45 (40–50) | p = 0.13 (MW) | |
| Immotile% | 54.2 ± 16.7 | 52.7 ± 17.2 | 56.3 ± 15.9 | |
| 50 (45–60) | 50 (45–56.5) | 55 (50–60) | p = 0.08 (MW) | |
| Normal forms% | 6.8 ± 5.1 | 8.5 ± 5.4 | 4.4 ± 3.4 | |
| 6 (2–10) | 8 (4–12) | 3 (2–6.5) | p < 0.0001 * (MW) | |
| Head defects% | 67.8 ± 16.9 | 64.1 ± 16.2 | 73.1 ± 16.7 | p = 0.0047 * (T) |
| 67 (56–80) | 65 (55–74) | 71 (59.5–90) | ||
| Neck and midpiece defects% | 11.8 ± 8.5 | 9.2 ± 7.0 | 15.5 ± 9.1 | |
| 10 (5–17) | 8 (3–15) | 15 (8.5–20) | p = 0.0002 * (MW) | |
| Tail defects% | 8.2 ± 8.5 | 6.1 ± 6.1 | 11.2 ± 10.5 | |
| 5 (2–13.25) | 4 (1–10) | 10 (3.5–16) | p = 0.0033 * (MW) | |
| Amorphous% | 15.7 ± 8.0 | 15.4 ± 7.8 | 16.2 ± 8.2 | |
| 15 (10–20) | 15 (10–21) | 15 (10–20) | p = 0.83 (MW) | |
| HPV | 40.2% (47) | — | — | — |
| Parameters | Low Risk | High Risk | p-Value (Test) |
|---|---|---|---|
| Patients | 11 | 36 | |
| DFI% | 22.9 ± 8.7 | 30.8 ± 10.5 | p = 0.0283 * (T) |
| 25 (16–28) | 31 (25–37.5) | ||
| Sperm concentration/mL | 34.6 ± 26.0 | 39.4 ± 43.6 | |
| 32 (18–53.5) | 27 (13.75–50.5) | p = 0.78 (MW) | |
| Total sperm number | 114.1 ± 106.6 | 117.3 ± 132.6 | |
| 68.2 (46.3–178.7) | 69 (27.1–146.8) | p = 0.78 (MW) | |
| Semen volume (mL) | 3.0 ± 1.2 | 3.0 ± 1.8 | |
| 3.1 (2.2–4) | 2.7 (1.95–3.85) | p = 0.59 (MW) | |
| Progressive motility% | 29.6 ± 18.9 | 27.1 ± 15.0 | p = 0.66 (T) |
| 35 (20–40) | 25 (20–31.25) | ||
| Non-progressive% | 13.2 ± 9.3 | 16.9 ± 7.0 | p = 0.16 (T) |
| 10 (10–15) | 20 (10–20) | ||
| Total motility% | 42.7 ± 22.7 | 43.9 ± 13.6 | |
| 50 (35–55) | 45 (40–50) | p = 0.57 (MW) | |
| Immotile% | 57.3 ± 22.7 | 56.1 ± 13.6 | |
| 50 (45–65) | 55 (50–60) | p = 0.57 (MW) | |
| Normal forms% | 4.6 ± 3.3 | 4.4 ± 3.5 | |
| 3 (2.5–6.5) | 3.5 (2–6.3) | p = 0.75 (MW) | |
| Head defects% | 70.0 ± 16.1 | 74.0 ± 17.0 | |
| 62 (59–80.5) | 76 (61.3–90) | p = 0.55 (MW) | |
| Neck and midpiece defects% | 16.6 ± 6.7 | 15.2 ± 9.8 | p = 0.68 (T) |
| 20 (12.5–20) | 15 (7–20.5) | ||
| Tail defects% | 10.7 ± 9.8 | 11.3 ± 10.9 | |
| 5 (4.5–17) | 10 (3–15) | p = 0.92 (MW) | |
| Amorphous% | 16.2 ± 8.3 | 16.3 ± 8.3 | |
| 15 (10–20) | 15 (10.75–20) | p = 0.89 (MW) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Capra, G.; Notari, T.; Buttà, M.; Serra, N.; Rizzo, G.; Bosco, L. Human Papillomavirus (HPV) Infection and Its Impact on Male Infertility. Life 2022, 12, 1919. https://doi.org/10.3390/life12111919
Capra G, Notari T, Buttà M, Serra N, Rizzo G, Bosco L. Human Papillomavirus (HPV) Infection and Its Impact on Male Infertility. Life. 2022; 12(11):1919. https://doi.org/10.3390/life12111919
Chicago/Turabian StyleCapra, Giuseppina, Tiziana Notari, Michela Buttà, Nicola Serra, Giovanni Rizzo, and Liana Bosco. 2022. "Human Papillomavirus (HPV) Infection and Its Impact on Male Infertility" Life 12, no. 11: 1919. https://doi.org/10.3390/life12111919