1. Introduction
Idiopathic intracranial hypertension (IIH) causes challenging headaches, visual loss, and reduced quality of life [
1]. Hospital costs for IIH admissions have been found to be four times greater than for a general population-based per person admission [
2]. Both in the United Kingdom and the USA patients access care through the emergency room, and have multiple attendances [
3,
4]. The inappropriate use of emergency care and repeated disease recurrences [
5,
6] may reflect the lack of accessible disease modifying treatments [
7]. These factors coupled with the increased incidence and prevalence of IIH [
3,
8,
9] are driving rising health care costs [
2,
3].
Body weight is the main modifiable risk factor in IIH [
10,
11], specifically central adiposity [
12]. Understanding this role of weight management in the disease was set as a high research priority by physicians, carers, and patients [
13]. Guidelines for treatment of IIH have placed weight management central to modify the disease [
14,
15,
16]. However, prior to the IIH weight trial (IIH:WT) there was little evidence for the best method of weight loss to achieve sustained IIH remission [
17]. IIH:WT showed that bariatric surgery was superior to community weight management intervention in women with active IIH and a body mass index (BMI) ≥ 35 kg/m
2 in lowering intracranial pressure, improved headache outcomes, and providing improvements in quality of life [
18]. Sustained weight loss should prevent multiple relapses of the disease [
5,
6], which will translate into a substantial reduction in healthcare costs.
Herein we estimate the cost-effectiveness of bariatric surgery, as compared to a community weight management intervention, in the first 24 months following the intervention in IIH. The aim was to establish the economic value of weight management type within the IIH:WT.
2. Materials and Methods
Sixty six women were recruited to the multicentre randomised controlled trial IIH:WT, comparing the efficacy of a bariatric surgery pathway versus a community weight management intervention, Weight Watchers
TM. Participants were identified from neurology and ophthalmology clinics at seven UK National Health Service (NHS) hospitals and recruited formally from five NHS centres. All participants had active IIH with papilloedema, in accordance with agreed criteria for diagnosis of IIH. The trial was registered, clinicaltrials.gov identifier: NCT02124486. The protocol and eligibility criteria [
17] and the main study findings have previously been published [
18].
This economic evaluation was undertaken from a UK National Health Service (NHS) and Personal Social Service perspective and measured costs and outcomes after 12 and 24 months follow up. The cost-effectiveness analysis compared the incremental costs and incremental reduction in intracranial pressure (ICP) for the bariatric surgery versus the community weight management pathway, as a treatment for IIH. A 12.5% reduction in ICP was chosen as the outcome for the cost-effectiveness analysis as this equated to the difference predicted between the trial arms. The incremental cost-effectiveness ratio was the difference in costs offset against the difference in ICP expressed as cost per reduction in ICP of 12.5%. A secondary per-protocol cost-effectiveness analysis was conducted.
2.1. Resource Use and Costs
To estimate costs, resource use data were collected and combined with unit cost information, including all primary care visits (General Practitioner and Nurse); hospital inpatient stays; hospital outpatient visits; Accident and Emergency visits; and all prescription medication. Primary care resource use was obtained from study-specific questionnaires and completed by trial participants at the trial data collection points. Secondary resource use and prescription data were obtained from the trial case report forms.
Unit costs for all primary and secondary resource use were obtained from the NHS Reference costs [
19] and Unit Cost of Health and Social Care [
20]; and for prescription costs, obtained from the British National Formulary [
21]. For prescription costs, all drugs used to manage IIH related symptoms were included, and costs estimated by combining the unit price by the daily dosage and number of days of treatment. For the intervention costs, the cost of the weight management programme was obtained from the trial data and for surgery, the NHS reference cost was applied. All inpatient stays up to eleven bed-days were priced at the appropriate flat rate, stays beyond that incurred a day rate for inpatient care. All costs were in UK pounds sterling using the 2017–2018 price level.
Supplemental Table S1 reports all unit costs applied.
2.2. Analyses
The economic evaluation measured costs and effects at the end of 24 months, so compared the difference in costs and the difference in outcomes for weight management versus surgery, for treatment of IIH. The primary analysis adopted an ‘intention to treat’ principle. Secondary analysis also measured cost-effectiveness consistent with a ‘per protocol’ principle as per the clinical effectiveness evaluation. All statistical tests set the significance levels at 2.5% with 95% confidence intervals calculated.
The data were examined for missingness and missing data were imputed separately for GP, nurse, inpatient, outpatient, and all medication costs. Multiple imputations were performed using a chained model with 60 iterations to account for the high proportion of missing data. Multiple imputation replaced each missing value with a set of m plausible values to generate 60 replacement values (m = 60) for each of the missing cells in these data sets, using multiple linear regression models [
22]. The imputed variables were merged at 0, 12, and 24 months.
All costs and outcomes were discounted to present values at an annual rate of 3.5%, in accordance with the National Institute for Health and Care Excellence [
23].
2.3. Sensitivity Analyses
To estimate the uncertainty around the resulting incremental cost-effectiveness ratio (ICER), a probabilistic sensitivity analysis was conducted. This was done using a non-parametric bootstrap analysis, with 5000 replicates, which empirically constructs the distribution of cost-effectiveness ratios by producing 5000 paired cost/ICP estimates. We considered using only complete cases (no missing data imputation) for a further sensitivity analysis, but this was disregarded due to the high level of missing data and the strong likelihood of bias.
All analyses were conducted using Stata version 15 (StataCorp LLC, College Station, TX, USA).
3. Results
Sixty-six women, with a mean age of 32.0 years (standard deviation (SD) ± 7.8, range 20–53 years), were included in the IIH:WT. The mean body mass index was 43.9 ± 7.0 kg/m2 ranging from 35.3 to 63.3 kg/m2. The predominant surgery was Roux-en-Y gastric bypass in 12 participants (44%), followed by gastric banding in 10 participants (37%) and laparoscopic sleeve gastrectomy in five participants (19%).The mean number of Weight WatchersTM face-to-face sessions attended was 14.3 (SD 10.6), with 58% attending at least one session. The adjusted difference in intracranial pressure at 12 months between the two trial arms was −6.0 cmCSF (adjusted mean difference (95% CI): −6.0 (−9.5, −2.4); p = 0.001). The effect on intracranial pressure increased between 12 and 24 months with a mean difference between the two arms of −8.2 cmCSF (adjusted mean difference (95% CI): −8.2 (−12.2, −4.2); p < 0.001).
3.1. Resource Use and Costs
There were no statistically significant differences between the two study arms in terms of primary or secondary care resource use, for the complete cases (
Table 1).
The degree of missing resource use data was balanced across the two study arms (
supplemental Table S2). After imputation, the total mean cost, including all primary, secondary, and medical-use costs, were GBP 1353 for the weight watchers arm and GBP 5400 for the bariatric surgery arm. The mean between-group cost difference was GBP 4107 (95% CI 3334–4880). (
Table 2)
The majority of costs for the bariatric surgery arm relate to the surgical procedure itself. Interestingly the primary, secondary, and medication costs (not including intervention costs) were consistently higher in the community weight management arm, and this difference was greater at 24 months compared to 12 months.
3.2. Intracranial Pressure Outcome
The proportion of patients who achieved a 12.5% reduction in ICP at 24 months were 85% with bariatric surgery and 39% with Weight Watchers. This represents a mean difference of 45% in favour of bariatric surgery (95% CI: 24% to 66%) (
Table 3).
3.3. Incremental Analysis
When the costs and ICP differences were combined, they show that at 24 months, bariatric surgery cost GBP 8807 to achieve a 12.5% reduction in ICP, when compared to a community weight management intervention programme (
Table 4).
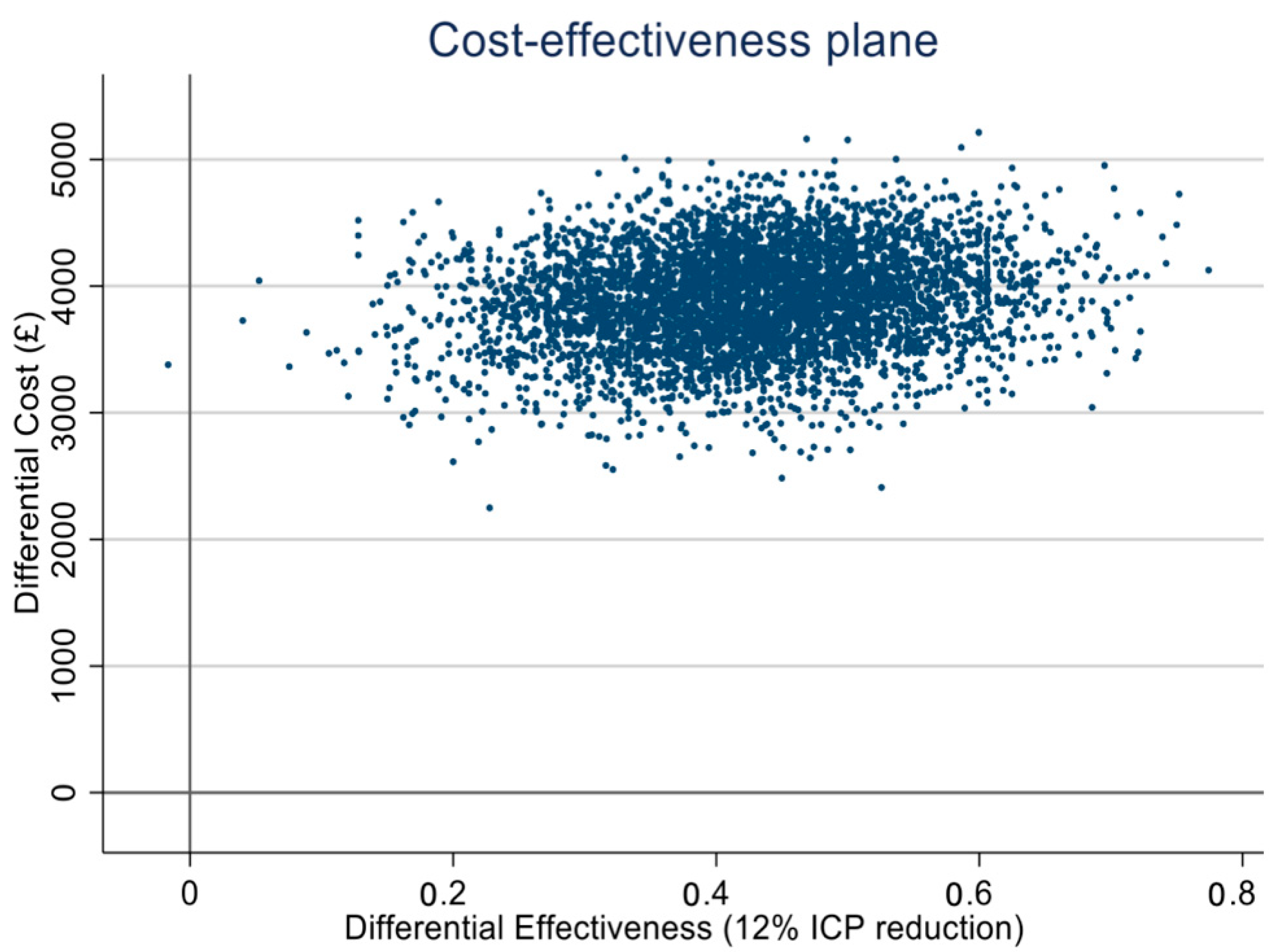
The cost-effectiveness plane presents 5000 jointly bootstrapped cost-ICP pairs distributed across four quadrants. Most of the pairs lie in the north-east quadrant indicating bariatric surgery to be more expensive and to lead to more gains in ICP reduction, relative to weight management. (
Figure 1).
3.4. Sensitivity Analysis
A sensitivity analysis performed a per-protocol analysis as two patients who were assigned to the community weight intervention had bariatric surgery between 12 and 24 months. Additionally, six participants who were assigned to the bariatric surgery arm did not have surgery and were therefore considered in the weight management arm. This per-protocol analysis showed that the ICERs were stable to these alterations, as detailed in
Table 5.
4. Discussion
The IIH:WT established that bariatric surgery was superior to a community weight management intervention in reduction of intracranial pressure, headache outcomes, and delivery of better quality of life in those with active IIH and a body mass index ≥35 kg/m
2 [
18]. This cost-effectiveness analysis reports on the economic value of bariatric surgery and details how the initial high cost of bariatric surgery is offset by these superior gains in intracranial pressure when compared to a weight management programme over 24 months. The incremental cost-effectiveness ratio at 24 months is less than at 12 months indicating that bariatric surgery appears to be more cost-effective with time in active IIH.
Bariatric surgery results in sustainable long term weight loss [
24], and in the IIH:WT reduced the intracranial pressure to below that of the diagnosis level, i.e., induced remission [
18]. The durability of bariatric surgery will therefore likely reduce the frequent relapses reported in IIH [
5,
6], which contribute to significant costly frequent hospital admissions over time [
2,
3,
4].
Bariatric surgery is known to deliver wide-reaching health benefits, as compared with conservative medical methods for weight loss [
24]. For example, Roux-en-Y gastric bypass surgery is associated with a reduced risk of cardiovascular disease when compared with routine care [
25]. These cardiovascular improvements may be of additional benefit for those with IIH, as IIH is known to be associated with a twofold increased risk of cardiovascular outcomes [
8]. This means that the cost-effectiveness results reported here represent conservative estimates as these wider cost-savings as a result of having surgery have not been included.
Roux-en-Y gastric bypass surgery has been evaluated as the most clinically effective weight loss intervention compared with other bariatric procedures and weight management programmes [
26]. This cost-effective analysis did not differentiate between the three different types of bariatric surgery offered in IIH:WT. The sample size within each surgical sub-type group was small; therefore, the differential costs and effects were not included. There is evidence that laparoscopic gastric band is associated with lower procedure costs, but has a much higher rate of revisional surgery, as well as a smaller and less well-maintained effect on body weight than Roux-en-Y gastric bypass and laparoscopic sleeve gastrectomy [
26]. However, the range and distribution of bariatric surgeries performed in the IIH:WT trial broadly reflect current practice in the UK health care system, and therefore the results are applicable to assessing bariatric surgery versus community weight management for treatment of IIH. Globally, more research is needed to fully evaluate the differential cost-effectiveness between bariatric surgery types.
This analysis was conducted from a health service perspective meaning that any out-of-pocket payments or indirect costs of IIH were not included. If these indirect costs such as days off work or time to travel to appointments to manage on-going IIH symptoms were included, then this would likely make bariatric surgery even more cost-saving. For example, in the USA total economic costs were estimated at exceeding USD 444 million in 2007 [
2], as compared in the UK to GBP 9.2 million in 2002 rising to GBP 49.9 million in 2014 [
12], when limited to health care costs alone. Likewise, the UK has a national health care system, and likely does not reflect other types of health care systems, in terms of relative costs for procedures and hospital attendances which are costed differently across private and insurance health care systems.
5. Conclusions
Bariatric surgery has been shown to be cost-effective [
26], however access to bariatric surgery within the UK health care system, the National Health Service, remains limited with less than 0.002% of the potentially eligible adults having the surgery annually [
27]. The data in this study and the original randomised control trial [
18] suggest that improved access to bariatric surgery for women with active IIH with a body mass index ≥35 kg/m
2 is likely to be cost effective, with improved savings over the longer term. Lifestyle weight management interventions currently remains the first line of treatment in patients with obesity and IIH, and if such treatment fail to achieve IIH remission, then referral to a bariatric surgery pathway should be offered.
Author Contributions
Conceptualization, E.F., Z.A. and A.J.S.; methodology, E.F and M.A.; software, E.F. and M.A.; formal analysis, E.F. and M.A.; writing—original draft preparation, E.F., M.A., and S.P.M.; writing—review and editing, J.L.M., Z.A., A.Y., R.S.O., R.S., and A.A.T.; supervision, E.F., S.P.M., and A.J.S.; project administration, R.S.O.; funding acquisition, A.J.S. All authors have read and agreed to the published version of the manuscript.
Funding
E.F. was funded by a National Institute for Health Research (NIHR) career development fellowship award (NIHR-CDF-2015-08-13) for the duration of the study. A.S. was funded by a National Institute for Health Research (NIHR) clinician scientist fellowship (NIHR-CS-011-028) and grant MR/K015184/1 from the Medical Research Council of the United Kingdom for the duration of the study. AJS is funded by a Sir Jules Thorn Award for Biomedical Science. A.T. was funded by NIHR Clinician Scientist Award for part of the duration of the study (CS-2013-13-029). The views expressed are those of the authors and not necessarily those of the UK National Health Service, the NIHR, or the UK department of Health and Social Care.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the The National Research Ethics Committee West Midlands (14/WM/0011).
Clinical Trial Registration Number
TISRCTN number, ISRCTN40152829 and ClinicalTrials.gov number, NCT02124486.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Reasonable requests will provide data beginning 12 months and ending 3 years after publication of this article to researchers whose proposed use of the data is approved by the original study investigators. Proposals should be made to the corresponding author and requesters will need to sign a data access agreement.
Acknowledgments
We acknowledge Birmingham Clinical Trials Unit (BCTU) for trial coordination and data management. We acknowledge the support of the NIHR Clinical Research Network and the Wellcome Trust Clinical Research Facilities, where IIH:WT was performed.
Conflicts of Interest
Mollan reports other Invex Therapeutics, other Heidelberg engineering during the conduct of the study; other from Chugai-Roche Ltd. (UK), other from Janssen, other from Allergan, other from Santen, other from Roche, other from Neurodiem, outside the submitted work. Tahrani reports grants from Novo Nordisk, personal fees from Novo Nordisk, non-financial support from Novo Nordisk, personal fees from Eli Lilly, non-financial support from Eli Lilly, personal fees from Janssen, personal fees from AZ, non-financial support from AZ, non-financial support from Impeto medical, non-financial support from Resmed, non-financial support from Aptiva, personal fees from BI, non-financial support from BI, personal fees from BMS, nonfinancial support from BMS, personal fees from NAPP, non-financial support from NAPP, personal fees from MSD, non-financial support from MSD, grants from Sanofi, and personal fees from Sanofi. Sinclair reports personal fees (salary and stock options) from Invex therapeutics, during the conduct of the study but outside the submitted work. All other authors declare no competing interests.
References
- Virdee, J.; Larcombe, S.; Vijay, V.; Sinclair, A.J.; Dayan, M.; Mollan, S.P. Reviewing the Recent Developments in Idiopathic Intracranial Hypertension. Ophthalmol. Ther. 2020, 9, 767–781. [Google Scholar] [CrossRef]
- Friesner, D.; Rosenman, R.; Lobb, B.M.; Tanne, E. Idiopathic intracranial hypertension in the USA: The role of obesity in establishing prevalence and healthcare costs. Obes. Rev. 2011, 12, e372–e380. [Google Scholar] [CrossRef]
- Mollan, S.P.; Aguiar, M.; Evison, F.; Frew, E.; Sinclair, A.J. The expanding burden of idiopathic intracranial hypertension. Eye 2019, 33, 478–485. [Google Scholar] [CrossRef] [Green Version]
- Murphy, S.; Friesner, D.L.; Rosenman, R.; Waslo, C.S.; Au, J.; Tanne, E. Emergency department utilization among individuals with idiopathic intracranial hypertension. Int. J. Health Care Qual. Assur. 2019, 32, 152–163. [Google Scholar] [CrossRef]
- Tata, G.; Kisabay, A.; Gokcay, F.; Celebisoy, N. Idiopathic intracranial hypertension: Are there predictors for visual outcome or recurrences? Clin. Neurol. Neurosurg. 2019, 183, 105378. [Google Scholar] [CrossRef]
- Kesler, A.; Hadayer, A.; Goldhammer, Y.; Almog, Y.; Korczyn, A.D. Idiopathic intracranial hypertension: Risk of recurrences. Neurology 2004, 63, 1737–9173. [Google Scholar] [CrossRef]
- Lueck, C.; McIlwaine, G. Interventions for idiopathic intracranial hypertension. Cochrane Database Syst. Rev. 2005, 20, CD003434. [Google Scholar]
- Adderley, N.J.; Subramanian, A.; Nirantharakumar, K.; Yiangou, A.; Gokhale, K.M.; Mollan, S.P.; Sinclair, A.J. Association Between Idiopathic Intracranial Hypertension and Risk of Cardiovascular Diseases in Women in the United Kingdom. JAMA Neurol. 2019, 76, 1088–1098. [Google Scholar] [CrossRef] [PubMed]
- McCluskey, G.; Doherty-Allan, R.; McCarron, P.; Loftus, A.; McCarron, L.; Mulholland, D.; McVerry, F.; McCarron, M. Meta-analysis and systematic review of population-based epidemiological studies in idiopathic intracranial hypertension. Eur. J. Neurol. 2018, 25, 1218–1227. [Google Scholar] [CrossRef] [PubMed]
- Mollan, S.P.; Tahrani, A.A.; Sinclair, A.J. The Potentially Modifiable Risk Factor in Idiopathic Intracranial Hypertension: Body Weight. Neurol. Clin. Pract. 2021. [Google Scholar] [CrossRef]
- Mollan, S.P.; Grech, O.; Alimajstorovic, Z.; Wakerley, B.R.; Sinclair, A.J. New horizons for idiopathic intracranial hypertension: Advances and challenges. Br. Med. Bull. 2020, 136, 118–126. [Google Scholar] [CrossRef]
- Hornby, C.; Botfield, H.; O’Reilly, M.W.; Westgate, C.; Mitchell, J.; Mollan, S.P.; Manolopoulos, K.; Tomlinson, J.; Sinclair, A. Evaluating the Fat Distribution in Idiopathic Intracranial Hypertension Using Dual-Energy X-ray Absorptiometry Scanning. Neuroophthalmology 2017, 42, 99–104. [Google Scholar] [CrossRef]
- Mollan, S.; Hemmings, K.; Herd, C.P.; Denton, A.; Williamson, S.; Sinclair, A.J. What are the research priorities for idiopathic intracranial hypertension? A priority setting partnership between patients and healthcare professionals. BMJ Open 2019, 9, e026573. [Google Scholar] [CrossRef] [Green Version]
- Hoffmann, J.; Mollan, S.P.; Paemeleire, K.; Lampl, C.; Jensen, R.H.; Sinclair, A.J. European headache federation guideline on idiopathic intracranial hypertension. J. Headache Pain 2018, 19, 93. [Google Scholar] [CrossRef] [PubMed]
- Mollan, S.P.; Davies, B.; Silver, N.C.; Shaw, S.; Mallucci, C.L.; Wakerley, B.R.; Krishnan, A.; Chavda, S.V.; Ramalingam, S.; Edwards, J.; et al. Idiopathic intracranial hypertension: Consensus guidelines on management. J. Neurol. Neurosurg. Psychiatry 2018, 89, 1088–1100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mollan, S.P.; Hornby, C.; Mitchell, J.; Sinclair, A.J. Evaluation management of adult idiopathic intracranial hypertension. Pract. Neurol. 2018, 18, 485–488. [Google Scholar] [CrossRef] [PubMed]
- Ottridge, R.; Mollan, S.P.; Botfield, H.; Frew, E.; Ives, N.J.; Matthews, T.; Mitchell, J.; Rick, C.; Singhal, R.; Woolley, R.; et al. Randomised controlled trial of bariatric surgery versus a community weight loss programme for the sustained treatment of idiopathic intracranial hypertension: The Idiopathic Intracranial Hypertension Weight Trial (IIH:WT) protocol. BMJ Open 2017, 7, e017426. [Google Scholar] [CrossRef] [Green Version]
- Mollan, S.P.; Mitchell, J.L.; Ottridge, R.S.; Aguiar, M.; Yiangou, A.; Alimajstorovic, Z.; Cartwright, D.M.; Grech, O.; Lavery, G.G.; Westgate, C.S.J.; et al. Effectiveness of Bariatric Surgery vs Community Weight Management Intervention for the Treatment of Idiopathic Intracranial Hypertension: A Randomized Clinical Trial. JAMA Neurol. 2021. [Google Scholar] [CrossRef]
- Department of Health. 2017/18 Reference Costs; National Health Service: London, UK, 2018; Available online: https://improvement.nhs.uk/resources/reference-costs/ (accessed on 3 January 2021).
- Curtis, L.; Burns, A. Personal Social Services Research Unit. Unit Costs of Health and Social Care 2017; University of Kent: Canterbury, UK, 2017. [Google Scholar]
- Joint Formulary Committee. British National Formulary; BMJ Group and Pharmaceutical Press: London, UK, 2018. [Google Scholar]
- Faria, R.; Gomes, M.; Epstein, D.; White, I.R. A guide to handling missing data in cost-effectiveness analysis conducted within randomised controlled trials. Pharmacoeconomics 2014, 32, 1157–1170. [Google Scholar] [CrossRef] [Green Version]
- National Institute for Health and Care Excellence (NICE). Developing NICE Guidelines: The Manual; National Institute for Health and Care Excellence London, UK, 2014. Available online: https://www.nice.org.uk/process/pmg20/chapter/introduction (accessed on 3 January 2021).
- Yan, G.; Wang, J.; Zhang, J.; Gao, K.; Zhao, Q.; Xu, X. Long-term outcomes of macrovascular diseases and metabolic indicators of bariatric surgery for severe obesity type 2 diabetes patients with a meta-analysis. PLoS ONE 2019, 14, e0224828. [Google Scholar] [CrossRef] [PubMed]
- Singh, P.; Subramanian, A.; Adderley, N.; Gokhale, K.; Singhal, R.; Bellary, S.; Nirantharakumar, K.; Tahrani, A.A. Impact of bariatric surgery on cardiovascular outcomes and mortality: A population-based cohort study. Br. J. Surg. 2020, 107, 432–442. [Google Scholar] [CrossRef] [PubMed]
- Colquitt, J.L.; Pickett, K.; Loveman, E.; Frampton, G.K. Surgery for weight loss in adults. Cochrane Database Syst. Rev. 2014, 8, CD003641. [Google Scholar] [CrossRef] [PubMed]
- Hazlehurst, J.M.; Logue, J.; Parretti, H.M.; Abbott, S.; Brown, A.; Pournaras, D.J.; Tahrani, A.A. Developing Integrated Clinical Pathways for the Management of Clinically Severe Adult Obesity: A Critique of NHS England Policy. Curr Obes Rep. 2020, 9, 530–543. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 

{kind=link}