
Indoor Radon Concentration and Risk Assessment in 27 Districts of a Public Healthcare Company in Naples, South Italy

{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sampling Plan
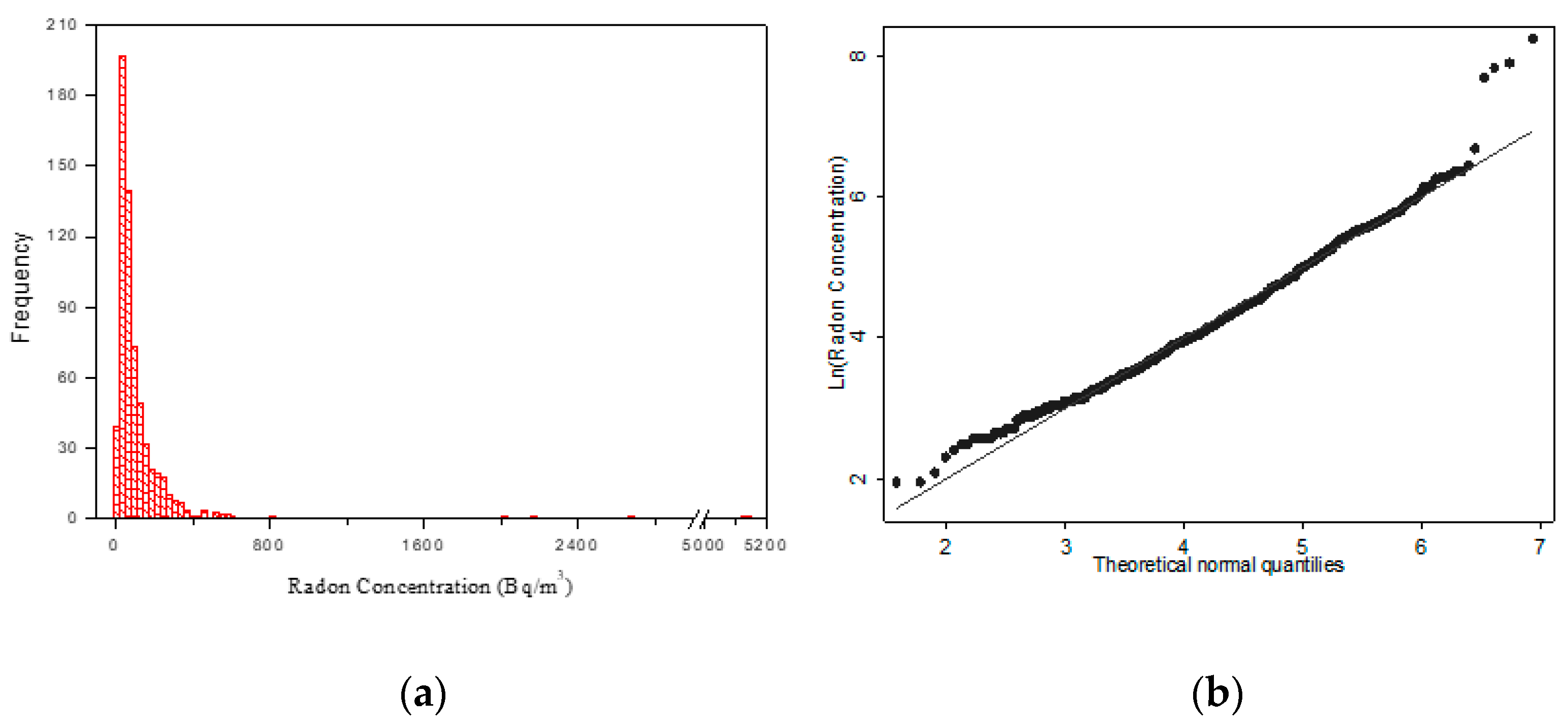
2.2. Monitoring, Detectors Analysis, and Statistical Analysis
2.3. Risk Assessment
3. Results
Risk Assessment
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gooding, T.D. An analysis of radon levels in the basements of UK workplaces and review of when employers should test. J. Radiol. Prot. 2018, 38, 247–261. [Google Scholar] [CrossRef] [PubMed]
- Kusky, T.M. Geological Hazards: A Sourcebook; Greenwood Press: Westport, CT, USA, 2003; pp. 236–239. ISBN 9781573564694. [Google Scholar]
- Barazza, F.; Murith, C.; Palacios, M.; Gfeller, W.; Crristen, E. A national survey on radon remediation in Switzerland. J. Radiol. Prot. 2018, 38, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Man-Made Mineral Fibres and Radon. In IARC Monographs on the Evaluation of the Carcinogenic Risks to Humans Volume 43; WHO IARC Publications: Lyon, France, 1988; ISBN 978-92-832-1243-0.
- Collier, C.G.; Strong, J.C.; Humphreys, J.A.; Timpson, N.; Baker, S.T.; Eldred, T.; Cobbi, L.; Papworth, D.; Haylock, R. Carcinogenicity of radon/radon decay product inhalation in rats—Effect of dose, dose rate and unattached fraction. Int. J. Radiat. Biol. 2005, 81, 631–647. [Google Scholar] [CrossRef]
- United Nations Scientific Committee on the Effect of Atomic Radiation (UNSCEAR). Sources and Effects on Ionizing Radiation; United Nation: New York, NY, USA, 2000. [Google Scholar]
- Lubin, J.H.; Wang, Z.Y.; Boice, J.D.J.; Zhao, Y.X.; Blot, W.J.; De Wang, L.; Kleinerman, R.A. Risk of lung cancer and residential radon in China: Pooled results of two studies. Int. J. Cancer 2004, 109, 132–137. [Google Scholar] [CrossRef]
- Bochicchio, F.; Forastiere, F.; Farchi, S.; Quarto, M.; Axelson, O. Residential radon exposure, diet and lung cancer: A case-control study in a Mediterranean region. Int. J. Cancer 2005, 114, 983–991. [Google Scholar] [CrossRef]
- Darby, S.; Hill, D.; Auvinen, A.; Barros-Dios, J.M.; Baysson, H.; Bochicchio, F.; Deo, H.; Falk, R.; Forastiere, F.; Hakama, M.; et al. Radon in homes and lung cancer risk: Collaborative analysis of individual data from 13 European case-control studies. Br. Med. J. 2005, 330, 223–226. [Google Scholar] [CrossRef] [Green Version]
- Krewski, D.; Lubin, J.H.; Zielinski, J.M.; Alavanja, M.; Catalan, V.S.; Field, R.W.; Klotz, J.B.; Létourneau, E.G.; Lynch, C.F.; Lyon, J.I.; et al. Residential radon and risk of lung cancer: A combined analysis of 7 north american case-controls studies. Epidemiology 2005, 16, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Krewski, D.; Lubin, J.H.; Zielinski, J.M.; Alavanja, M.; Catalan, V.S.; Field, R.W.; Klotz, J.B.; Létourneau, E.G.; Lynch, C.F.; Lyon, J.L.; et al. A combined analysis of North American case–control studies of residential radon and lung cancer. J. Toxicol. Environ. Health A 2006, 69, 533–597. [Google Scholar] [CrossRef] [Green Version]
- Garzillo, C.; Pugliese, M.; Loffredo, F.; Quarto, M. Indoor radon exposure and lung cancer risk: A meta-analysis of case-control studies. Transl. Cancer Res. 2017, 6, S934–S943. [Google Scholar] [CrossRef]
- Basic Safety Standards for Protection Against the Dangers Arising from Expo-Sure to Ionizing Radiation. Council Directive 2013/59/Euratom 17 January 2014. Available online: https://eur-lex.europa.eu/LexUriServ/LexUriServ.do?uri=OJ:L:2014:013:0001:0073:EN:PDF (accessed on 20 February 2021).
- Scott, B.R. Residential radon appears to prevent lung cancer. Dose Response 2011, 9, 444–464. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fornalski, K.W.; Adams, R.; Allison, W.; Corric, L.E.; Cuttle, J.M.; Davey, C.; Dobrzyński, L.; Esposito, V.J.; Feinendegen, L.E.; Gomez, L.S.; et al. The assumption of radon-induced cancer risk. Cancer Causes Control 2015, 26, 1517–1518. [Google Scholar] [CrossRef] [PubMed]
- Dobrzyński, L.; Fornalski, K.W.; Reszczyńska, J. Meta-analysis of thirty-two case–control and two ecological radon studies of lung cancer. J. Radiol. Res. 2018, 59, 149–163. [Google Scholar] [CrossRef] [PubMed]
- DECRETO LEGISLATIVO 31 Luglio 2020, n. 101, in Italian. Available online: https://www.gazzettaufficiale.it/eli/id/2020/08/12/20G00121/sg (accessed on 20 February 2021).
- International Commission on Radiological Protection. Occupational Intakes of Radionuclides: Part 3. ICRP 137. Annals ICRP 2017, 36, 1–487. [Google Scholar]
- International Commission on Radiological Protection. The 2007 Recommendations of the International Commission on Radiological Protection; ICRP 103; Elsevier: Amsterdam, The Netherlands, 2007; Volume 37. [Google Scholar]
- International Commission on Radiological Protection. Lung cancer risk from exposure to radon daughters. ICRP 50. Ann. ICRP 1987, 17, 1–57. [Google Scholar]
- Ruano-Ravina, A.; Narocki, C.; Lopez-Jacob, M.J.; Garcia Oliver, A.; de la Cruz Calle Tierno, M.; Peon-Gonzalez, J.; Barros-Dios, J.M. Indoor radon in Spanish workplaces. A pilot study before the introduction of the European Directive 2013/59/Euratom. Gac. Sanit. 2019, 33, 563–567. [Google Scholar] [CrossRef]
- International Commission on Radiological Protection. Protection against Radon-222 at Home and at Work. ICRP 65. Ann. ICRP 1993, 23, 1–45. [Google Scholar]
- ICRP 115, International Commission on Radiological Protection. Lung Cancer Risk from Radon and Progeny and Statement on Radon. Ann. ICRP 2010, 40, 1–64. [Google Scholar] [CrossRef] [PubMed]
- Pugliese, M.; Quarto, M.; De Cicco, F.; De Sterlich, C.; Roca, V. Radon Exposure Assessment for Sewerage System’s Workers in Naples, South Italy. Indoor Built. Environ. 2013, 22, 575–579. [Google Scholar] [CrossRef]
- Vimercati, L.; Fucilli, F.; Cavone, D.; De Maria, L.; Birtolo, F.; Ferri, G.M.; Soleo, L.; Lovreglio, P. Radon Levels in Indoor Environments of the University Hospital in Bari-Apulia Region Southern Italy. Int. J. Environ. Res. Public Health 2018, 15, 694. [Google Scholar] [CrossRef] [Green Version]
- Bucci, S.; Pratesi, G.; Viti, M.L.; Pantani, M.; Bochicchio, F.; Venoso, G. Radon in workplaces: First results of an extensive survey and comparison with radon in homes. Radiat. Prot. Dosim. 2011, 145, 202–205. [Google Scholar] [CrossRef] [Green Version]
- Quarto, M.; Pugliese, M.; Loffredo, F.; Zambella, C.; Roca, V. Radon measurements and Effective Dose from Radon Inhalation estimation in the Neapolitan Catacombs. Radiat. Prot. Dosim. 2014, 158, 442–446. [Google Scholar] [CrossRef]
- Panatto, D.; Gasparini, R.; Nenatti, U.; Gallelli, G. Assessment and prevention of radioactive risk due to 222Radon on university premises in Genoa, Italy. J. Prev. Med. Hyg. 2007, 47, 134–137. [Google Scholar]
- L’Abbate, N.; Di Pierri, C.; Martucci, V.; Cianciaruso, G.; Ragone, M. Radon concentrations in Apulian banking workplaces. GIMLE 2010, 32 (Suppl. 4), 248–250. [Google Scholar]
- Duckworth, L.T.; Frank-Stromborg, M.; Oleckno, W.; Duffy, P.; Burns, K. Relationship of Perception of Radon as a Health Risk and Willingness to Engage in Radon Testing and Mitigation. Oncol. Nurs. Forum 2002, 29, 1099–1107. [Google Scholar] [CrossRef] [PubMed]
- Loffredo, F.; Savino, F.; Serra, M.; Tafuri, D.; Quarto, M. Cognitive investigation on the knowledge of the risk deriving from radon exposure: Preliminary results. Acta Med. Mediterr. 2020, 36, 1265–1267. [Google Scholar]
- Bochicchio, F.; Campos Venuti, G.; Piermattei, S.; Nuccetelli, C.; Risica, S.; Tommasino, L.; Torri, G.; Magnoni, M.; Agnesod, G.; Sgorbati, G.; et al. Annual average and seasonal variations of residential radon concentration for all the Italian Regions. Radiat. Meas. 2005, 40, 686–694. [Google Scholar] [CrossRef]
- Trevisi, R.; Orlando, C.; Orlando, P.; Amici, M.; Simeoni, C. Radon levels in underground workplaces—Results of a nationwide survey in Italy. Radiat. Meas. 2012, 47, 178–181. [Google Scholar] [CrossRef]
- Rossetti, M.; Esposito, M. Radon levels in underground workplaces: A map of the Italian region. Radiat. Prot. Dosim. 2014, 164, 392–397. [Google Scholar] [CrossRef]
- Kunovska, B.; Ivanova, K.; Badulin, V.; Cenova, M.; Angelova, A. Assessment of residential exposure in Bulgaria. Radiat. Prot. Dosim. 2018, 181, 34–37. [Google Scholar] [CrossRef]
- Bossew, P. Radon: Exploring the log-normal mystery. J. Environ. Radioact. 2010, 101, 826–834. [Google Scholar] [CrossRef]
- World Health Organization. Handbook on Indoor Radon; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Bochicchio, F.; Antignani, S.; Venoso, G.; Forastiere, F. Quantitative evaluation of the lung cancer deaths attributable to residential radon: A simple method and results for all the 21 Italian Regions. Radiat. Meas. 2012, 50, 121–126. [Google Scholar] [CrossRef]
- International Commission on Radiological Protection. Radiological Protection against Radon Exposure. ICRP 126. Ann. ICRP 2014, 43, 1–73. [Google Scholar]
- Bochicchio, F.; Campos Venuti, G.; Nucciatelli, C.; Piermattei, S.; Risica, S.; Tommasino, L.; Torri, G. Results of the representative italian national survey on radon indoors. Health Phys. 1996, 71, 721–748. [Google Scholar] [CrossRef] [PubMed]
- Sabbarese, C.; Ambrosino, F.; D’Onofrio, A.; Pugliese, M.; La Verde, G.; D’Avino, V.; Roca, V. The first radon potential map of the Campania region (southern Italy). Appl. Geochem. 2021, 126, 104890. [Google Scholar] [CrossRef]
- Loffredo, F.; Scala, A.; Adinolfi, G.M.; Savino, F.; Quarto, M. A new geostatistical tool for the analysis of the geographical variability of the indoor radon activity. Nukleonika 2020, 65, 99–104. [Google Scholar] [CrossRef]


Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loffredo, F.; Savino, F.; Amato, R.; Irollo, A.; Gargiulo, F.; Sabatino, G.; Serra, M.; Quarto, M. Indoor Radon Concentration and Risk Assessment in 27 Districts of a Public Healthcare Company in Naples, South Italy. Life 2021, 11, 178. https://doi.org/10.3390/life11030178
Loffredo F, Savino F, Amato R, Irollo A, Gargiulo F, Sabatino G, Serra M, Quarto M. Indoor Radon Concentration and Risk Assessment in 27 Districts of a Public Healthcare Company in Naples, South Italy. Life. 2021; 11(3):178. https://doi.org/10.3390/life11030178
Chicago/Turabian StyleLoffredo, Filomena, Federica Savino, Roberto Amato, Alfredo Irollo, Francesco Gargiulo, Giuseppe Sabatino, Marcello Serra, and Maria Quarto. 2021. "Indoor Radon Concentration and Risk Assessment in 27 Districts of a Public Healthcare Company in Naples, South Italy" Life 11, no. 3: 178. https://doi.org/10.3390/life11030178