
A Comprehensive Framework to Evaluate the Effects of Anterior Cruciate Ligament Injury and Reconstruction on Graft and Cartilage Status through the Analysis of MRI T2 Relaxation Time and Knee Laxity: A Pilot Study

 ,
,  , ,
, , 
Abstract
:1. Introduction
2. Methods
2.1. Patients Enrolment
2.2. Knee Laxity Assessment
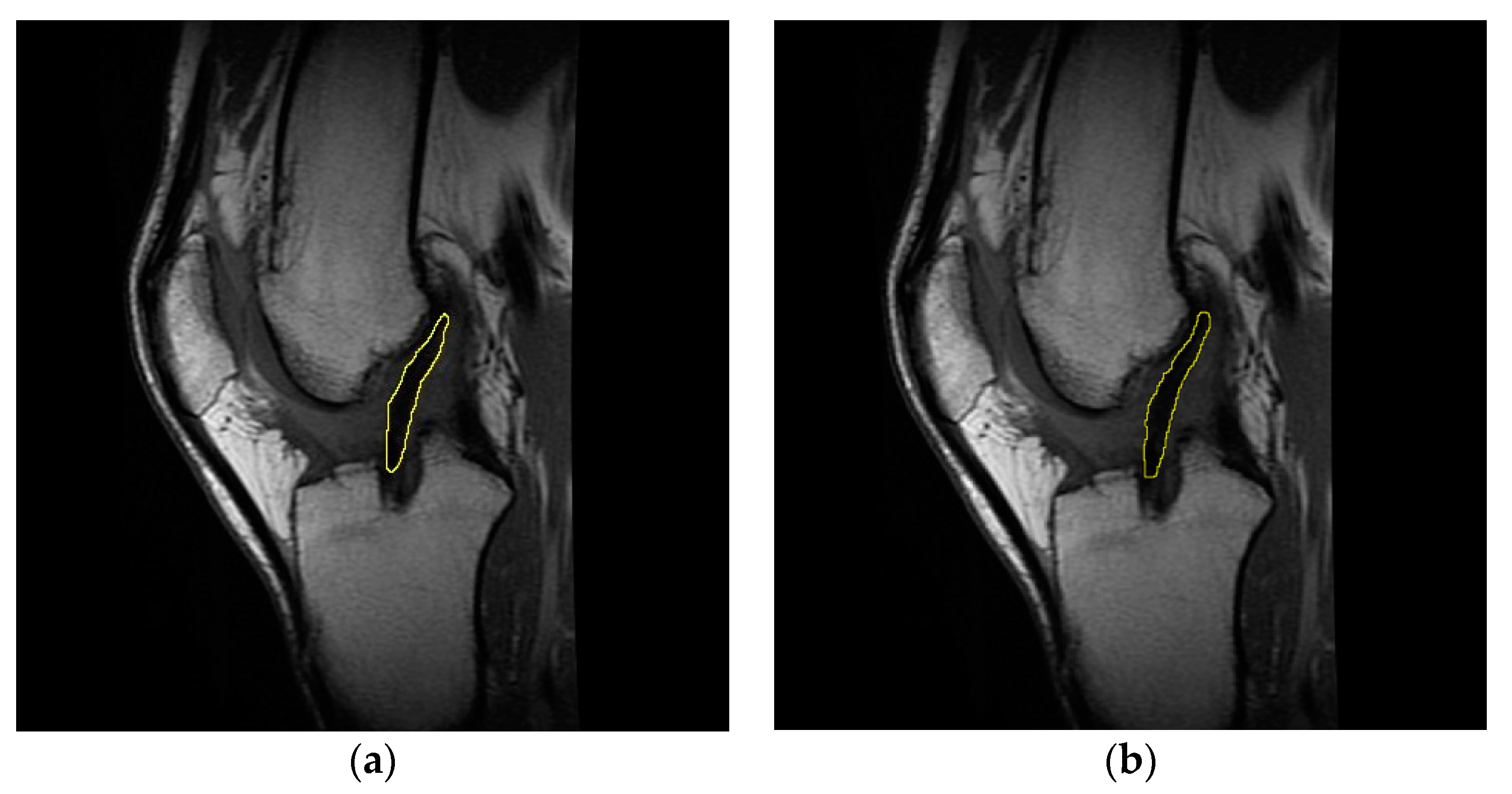
2.3. MRI Analysis
2.4. Statistical Analysis
3. Results
3.1. Knee Laxity
3.2. ACL, Graft, and Cartilage T2 Signals
3.3. Relationship between Cartilage and Graft T2 Values
3.4. Relationship between Cartilage T2 Values and Knee Laxity
3.5. Relationship between Graft T2 Signal and Knee Laxity
4. Discussion
4.1. Knee Laxity
4.2. ACL T2 Signal
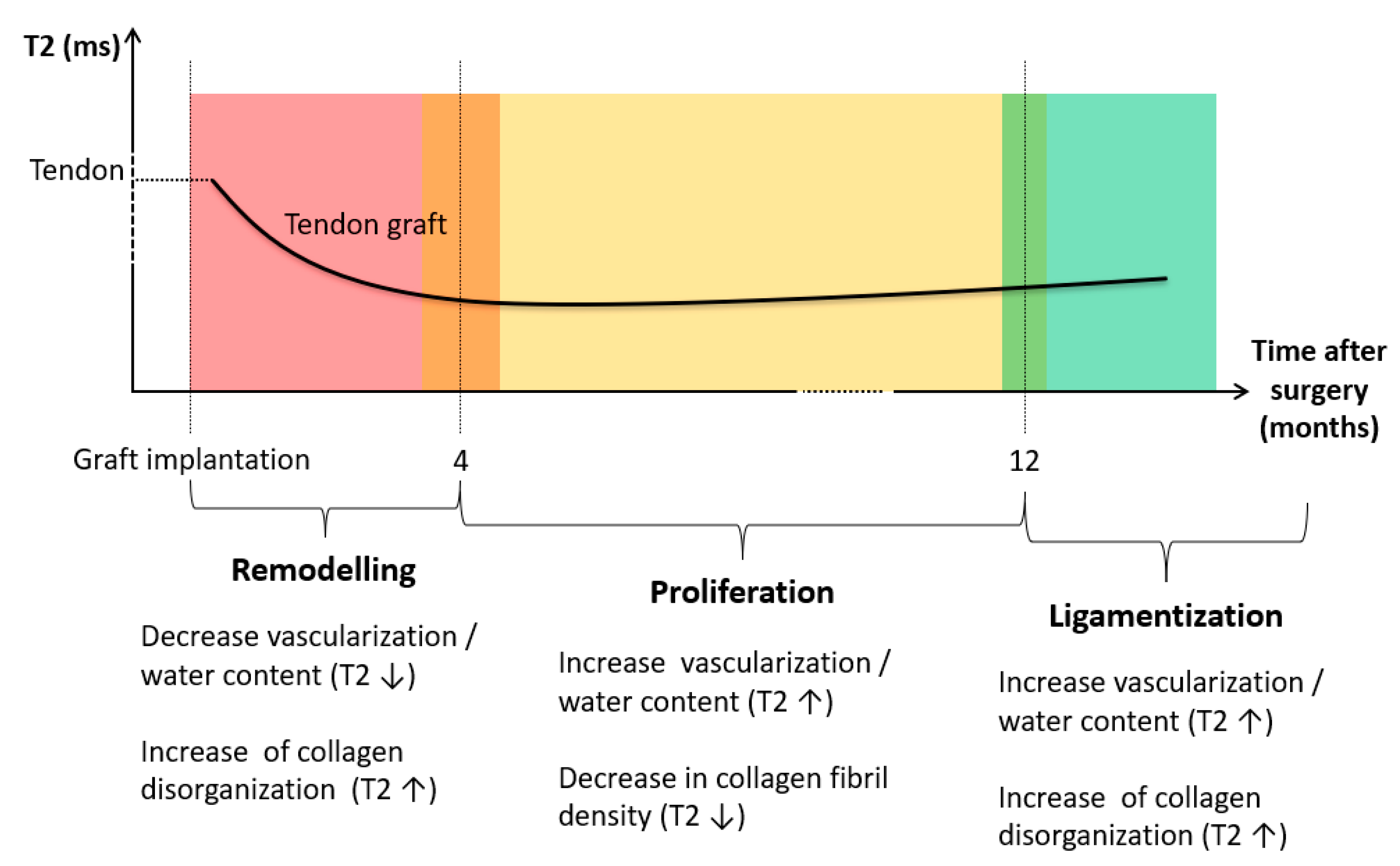
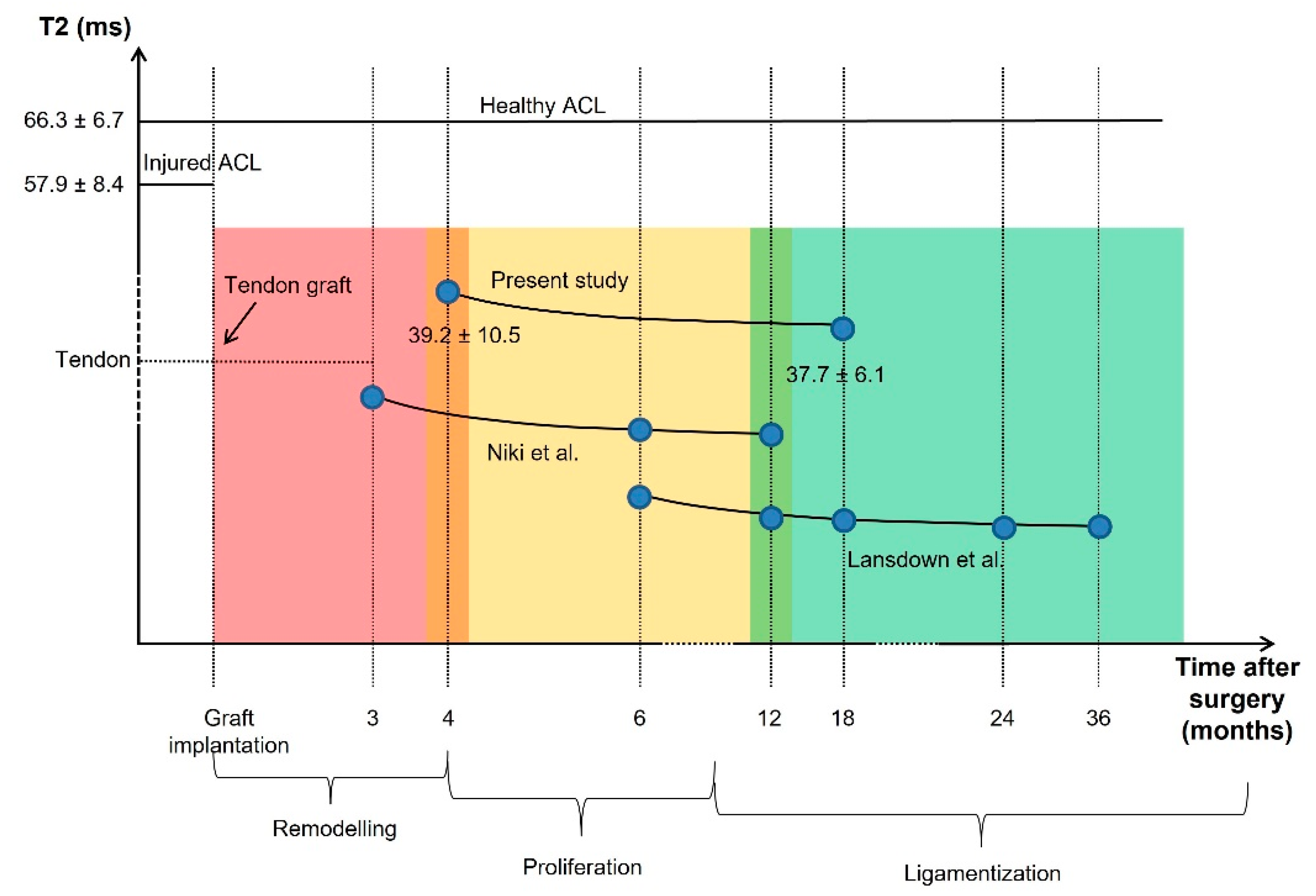
4.3. Graft T2 Signal
4.4. Cartilage T2 Signal
4.5. Relationship between Graft T2 Signal and Knee Laxity
4.6. Relationship between Cartilage T2 Signal and Knee Laxity
4.7. Relationship between Cartilage and Graft T2 Signal
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Correction Statement
References
- Saupe, N.; White, L.M.; Chiavaras, M.M.; Essue, J.; Weller, I.; Kunz, M.; Hurtig, M.; Marks, P. Anterior Cruciate Ligament Reconstruction Grafts: MR Imaging Features at Long-Term Follow-up-Correlation with Functional and Clinical Evaluation. Radiology 2008, 249, 581–590. [Google Scholar] [CrossRef]
- Neuman, P.; Kostogiannis, I.; Fridén, T.; Roos, H.; Dahlberg, L.E.; Englund, M. Knee Laxity after Complete Anterior Cruciate Ligament Tear: A Prospective Study over 15 Years. Scand. J. Med. Sci. Sports 2012, 22, 156–163. [Google Scholar] [CrossRef]
- Grassi, A.; Signorelli, C.; Lucidi, G.A.; Raggi, F.; Macchiarola, L.; di Sarsina, T.R.; Muccioli, G.M.M.; Filardo, G.; Zaffagnini, S. ACL Reconstruction with Lateral Plasty Reduces Translational and Rotatory Laxity Compared to Anatomical Single Bundle and Non-Anatomical Double Bundle Surgery: An in vivo Kinematic Evaluation with Navigation System. Clin. Biomech. 2019, 69, 1–8. [Google Scholar] [CrossRef]
- Fu, F.H.; Bennett, C.H.; Ma, C.B.; Menetrey, J.; Lattermann, C. Current Trends in Anterior Cruciate Ligament Reconstruction. Part II. Operative Procedures and Clinical Correlations. Am. J. Sports Med. 2000, 28, 124–130. [Google Scholar] [CrossRef]
- Brophy, R.H.; Pearle, A.D. Single-Bundle Anterior Cruciate Ligament Reconstruction: A Comparison of Conventional, Central, and Horizontal Single-Bundle Virtual Graft Position. Am. J. Sports Med. 2009, 37, 1317–1323. [Google Scholar] [CrossRef]
- Su, F.; Hilton, J.F.; Nardo, L.; Wu, S.; Liang, F.; Link, T.M.; Ma, C.B.; Li, X. Cartilage Morphology and T1ρ and T2 Quantification in ACL-Reconstructed Knees: A 2-Year Follow-Up. Osteoarthr. Cartil. 2013, 21, 1058–1067. [Google Scholar] [CrossRef]
- Cheung, E.C.; DiLallo, M.; Feeley, B.T.; Lansdown, D.A. Osteoarthritis and ACL Reconstruction—Myths and Risks. Curr. Rev. Musculoskelet. Med. 2020, 13, 115–122. [Google Scholar] [CrossRef]
- Øiestad, B.E.; Engebretsen, L.; Storheim, K.; Risberg, M.A. Knee Osteoarthritis after Anterior Cruciate Ligament Injury: A Systematic Review. Am. J. Sports Med. 2009, 37, 1434–1443. [Google Scholar] [CrossRef]
- Gold, G.E.; McCauley, T.R.; Gray, M.L.; Disler, D.G. What’s New in Cartilage? Radiographics 2003, 23, 1227–1242. [Google Scholar] [CrossRef]
- Williams, A.; Winalski, C.S.; Chu, C.R. Early Articular Cartilage MRI T2 Changes after Anterior Cruciate Ligament Reconstruction Correlate with Later Changes in T2 and Cartilage Thickness. J. Orthop. Res. 2017, 35, 699–706. [Google Scholar] [CrossRef]
- Niki, Y.; Yasuoka, T.; Kobayashi, S.; Harato, K.; Nagura, T.; Okuda, S.; Jinzaki, M. Feasibility of T1rho and T2 Map Magnetic Resonance Imaging for Evaluating Graft Maturation after Anatomic Double-Bundle Anterior Cruciate Ligament Reconstruction. J. Orthop. Surg. Res. 2019, 14, 140. [Google Scholar] [CrossRef]
- Matzat, S.J.; van Tiel, J.; Gold, G.E.; Oei, E.H.G. Quantitative MRI Techniques of Cartilage Composition. Quant. Imaging Med. Surg. 2013, 3, 162–174. [Google Scholar] [CrossRef]
- Plewes, D.B.; Kucharczyk, W. Physics of MRI: A primer. J. Magn. Reson. Imaging 2012, 35, 1038–1054. [Google Scholar] [CrossRef]
- Alhadlaq, H.A.; Xia, Y.; Moody, J.B.; Matyas, J.R. Detecting Structural Changes in Early Experimental Osteoarthritis of Tibial Cartialge by Microscopic Magnetic Resonance Imaging and Polarised Light Microscopy. Ann. Rheum Dis. 2004, 63, 709–717. [Google Scholar] [CrossRef]
- David-Vaudey, E.; Ghosh, S.; Ries, M.; Majumdar, S. T2 Relaxation Time Measurements in Osteoarthritis. Magn. Reson. Imaging 2004, 22, 673–682. [Google Scholar] [CrossRef]
- Wong, C.S.; Yan, C.H.; Gong, N.J.; Li, T.; Chan, Q.; Chu, Y.C. Imaging Biomarker with T1 and T2 Mappings in Osteoarthritis-in vivo Human Articular Cartilage Study. Eur. J. Radiol. 2013, 82, 647–650. [Google Scholar] [CrossRef]
- Koff, M.F.; Ameami, K.K.; Kaufman, K.R. Clinical Evaluation of T2 Values of Patellar Cartilage in Patients with Osteoarthritis. Osteoarthr. Cartil. 2007, 15, 198–204. [Google Scholar] [CrossRef]
- Lansdown, D.A.; Xiao, W.; Zhang, A.L.; Allen, C.R.; Feeley, B.T.; Li, X.; Majumdar, S.; Ma, C.B. Quantitative Imaging of Anterior Cruciate Ligament (ACL) Graft Demonstrates Longitudinal Compositional Changes and Relationships with Clinical Outcomes at 2 Years after ACL Reconstruction. J. Orthop. Res. 2020, 38, 1289–1295. [Google Scholar] [CrossRef]
- Panos, J.A.; Webster, K.E.; Hewett, T.E. Anterior Cruciate Ligament Grafts Display Differential Maturation Patterns on Magnetic Resonance Imaging Following Reconstruction: A Systematic Review. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 2124–2138. [Google Scholar] [CrossRef]
- Scheffler, S.U.; Unterhauser, F.N.; Weiler, A. Graft Remodelling and Ligamentization after Cruciate Ligament Reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2008, 16, 834–842. [Google Scholar] [CrossRef]
- Andriacchi, T.P.; Dyrby, C.O. Interactions between Kinematics and Loading during Walking for the Normal and ACL Deficient Knee. J. Biomech. 2005, 38, 293–298. [Google Scholar] [CrossRef]
- Chaudhari, A.M.W.; Briant, P.L.; Bevill, S.L.; Koo, S.; Andriacchi, T.P. Knee Kinematics, Cartilage Morphology, and Osteoarthritis after ACL Injury. Med. Sci. Sports Exerc. 2008, 40, 215–222. [Google Scholar] [CrossRef]
- Wilson, W.; van Burken, C.; van Donkelaar, C.; Buma, P.; van Rietbergen, B.; Huiskes, R. Causes of Mechanically Induced Collagen Damage in Articular Cartilage. J. Orthop. Res. 2006, 24, 220–228. [Google Scholar] [CrossRef]
- Zaid, M.; Lansdown, D.; Su, F.; Pedoia, V.; Tufts, L.; Rizzo, S.; Souza, R.B.; Li, X.; Ma, C.B. Abnormal Tibial Position Is Correlated to Early Degenerative Changes One Year Following ACL Reconstruction. J. Orthop. Res. 2015, 33, 1079–1086. [Google Scholar] [CrossRef]
- di Sarsina, T.R.; Macchiarola, L.; Signorelli, C.; Grassi, A.; Raggi, F.; Muccioli, G.M.M.; Zaffagnini, S. Anterior Cruciate Ligament Reconstruction with an All-Epiphyseal “Over-the-Top” Technique Is Safe and Shows Low Rate of Failure in Skeletally Immature Athletes. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 498–506. [Google Scholar] [CrossRef]
- Gage, A.; Kluczynski, M.A.; Bisson, L.J.; Marzo, J.M. Factors Associated with a Delay in Achieving Full Knee Extension before Anterior Cruciate Ligament Reconstruction. Orthop. J. Sports Med. 2019, 7. [Google Scholar] [CrossRef]
- Marcacci, M.; Zaffagnini, S.; Muccioli, G.M.M.; Neri, M.P.; Bondi, A.; Nitri, M.; Bonanzinga, T.; Grassi, A. Arthroscopic Intra- and Extra-Articular Anterior Cruciate Ligament Reconstruction with Gracilis and Semitendinosus Tendons: A Review. Curr. Rev. Musculoskelet. Med. 2011, 4, 73–77. [Google Scholar] [CrossRef]
- Pollet, V.; Barrat, D.; Meirhaeghe, E.; Vaes, P.; Handelberg, F. The Role of the Rolimeter in Quantifying Knee Instability Compared to the Functional Outcome of ACL-Reconstructed Versus Conservatively-Treated Knees. Knee Surg. Sports Traumatol. Arthrosc. 2005, 13, 12–18. [Google Scholar] [CrossRef]
- Zaffagnini, S.; Lopomo, N.; Signorelli, C.; Muccioli, G.M.M.; Bonanzinga, T.; Grassi, A.; Visani, A.; Marcacci, M. Innovative Technology for Knee Laxity Evaluation: Clinical Applicability and Reliability of Inertial Sensors for Quantitative Analysis of the Pivot-Shift Test. Clin. Sports Med. 2013, 32, 61–70. [Google Scholar] [CrossRef]
- Cassiolas, G.; Berni, M.; Marchiori, G.; Bontempi, M.; Bragonzoni, L.; Valente, G.; Grassi, A.; Zaffagnini, S.; Visani, A.; Lopomo, N.F. How Cartilage Status Can Be Related to Joint Loads in Anterior Cruciate Ligament Reconstruction: A Preliminary Analysis Including MRI t2 Mapping and Joint Biomechanics. J. Biol. Regul. Homeost. Agents 2018, 32, 35–40. [Google Scholar]
- Schmitz, R.J.; Wang, H.M.; Kraft, R.A.; Shultz, S.J.; Ross, S.E.; Henson, R.A.; Perrin, D.H. Regional Differences in Anterior Cruciate Ligament Imaging Biomarkers: T2 and T2* Values. Muscles Ligaments Tendons J. (MLTJ) 2018, 8, 238–245. [Google Scholar] [CrossRef]
- Hofbauer, M.; Soldati, F.; Szomolanyi, P.; Trattnig, S.; Bartolucci, F.; Fu, F.; Denti, M. Hamstring Tendon Autografts Do Not Show Complete Graft Maturity after 6 Months Postoperatively after Anterior Cruciate Ligament Reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Fukawa, T.; Yamaguchi, S.; Watanabe, A.; Sasho, T.; Akagi, R.; Muramatsu, Y.; Akatsu, Y.; Katsuragi, J.; Endo, J.; Osone, F.; et al. Quantitative Assessment of Tendon Healing by Using MR T2 Mapping in a Rabbit Achilles Tendon Transection Model Treated with Platet-Rich Plasma. Radiology 2015, 276, 748–755. [Google Scholar] [CrossRef]
- Watanabe, A.; Boesch, C.; Obata, T.; Anderson, S.E. Effect of Multiscale Acquisition on T1 and T2 Measurements of Articular Cartilage at 3T. J. Magn. Reson. Imaging 2007, 26, 109–117. [Google Scholar] [CrossRef]
- Fleming, B.C.; Vajapeyam, S.; Connolly, S.A.; Magarian, E.M.; Murray, M.M. The Use of Magnetic Resonance Imaging to Predict ACL Graft Structural Properties. J. Biomech. 2011, 44, 2843–2846. [Google Scholar] [CrossRef] [PubMed]
- Nishioka, H.; Hirose, J.; Nakamura, E.; Okamoto, N.; Karasugi, T.; Taniwaki, T.; Okada, T.; Yamashita, Y.; Mizuta, H. Detecting ICRS Grade 1 Cartilage Lesions in Anterior Cruciate Ligament Injury Using T1 ƍ and T2 Mapping. Eur. J. Rad. 2013, 82, 1499–1505. [Google Scholar] [CrossRef]
- Ntoulia, A.; Papadopoulou, F.; Zampeli, F.; Ristanis, S.; Argyropoulou, M.; Georgoulis, A. Evaluation with Contrast-Enhanced Magnetic Resonance Imaging of Anterior Cruciate Ligament Graft during Its Healing Process: A Two-Years Prospective Study. Skelet. Radiol. 2013, 42, 541–552. [Google Scholar] [CrossRef] [PubMed]
- Gheno, R.; Yoon, Y.C.; Wang, J.H.; Kim, K.; Baek, S.Y. Changes in the T2 Relaxation Value of the Tibiofemoral Articular Cartilage about 6 Months after Anterior Cruciate Ligament Reconstruction Using the Double-Bundle Technique. Br. J. Radiol. 2016, 89, 20151002. [Google Scholar] [CrossRef]
- Gupta, R.; Virayavanich, W.; Kuo, D.; Su, F.; Link, T.; Ma, B.; Li, X. MR T1ƍ Quantification of Cartilage Focal Lesions in Acutely Injured Knees: Correlation with Arthroscopic Evaluation. Magn. Reson. Imaging 2014, 32, 1290–1296. [Google Scholar] [CrossRef]
- Thomas, A.C.; Hubbard-Turner, T.; Wikstrom, E.A.; Palmieri-Smith, R.M. Epidemiology of posttraumatic osteoarthritis. J. Athl. Train. 2017, 52, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Carbone, A.; Rodeo, S. Review of Current Understanding of Post-Traumatic Osteoarthritis Resulting from Sports Injuries. J. Orthop. Res. 2017, 35, 397–405. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.J.; Zeng, N.; Yan, Z.Y.; Li, J.T.; Ni, G.X. Post-Traumatic Osteoarthritis Following ACL Injury. Arthritis Res. Ther. 2020, 22, 57. [Google Scholar] [CrossRef] [PubMed]
- Sanders, T.L.; Kremers, H.M.; Bryan, A.J.; Fruth, K.M.; Larson, D.R.; Pareek, A.; Levy, B.A.; Stuart, M.J.; Dahm, D.L.; Krych, A.J. Is Anterior Cruciate Ligament Reconstruction Effective in Preventing Secondary Meniscal Tears and Osteoarthritis? Am. J. Sports Med. 2016, 44, 1699–1707. [Google Scholar] [CrossRef] [PubMed]
- Lindanger, L.; Strand, T.; Mølster, A.O.; Solheim, E.; Inderhaug, E. Effect of Early Residual Laxity After Anterior Cruciate Ligament Reconstruction on Long-term Laxity, Graft Failure, Return to Sports, and Subjective Outcome at 25 Years. Am. J. Sports Med. 2021, 49, 1227–1235. [Google Scholar] [CrossRef] [PubMed]
- Cristiani, R.; Sarakatsianos, V.; Engström, B.; Samuelsson, K.; Forssblad, M.; Stålman, A. Increased Knee Laxity with Hamstring Tendon Autograft Compared to Patellar Tendon Autograft: A Cohort Study of 5462 Patients with Primary Anterior Cruciate Ligament Reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 381–388. [Google Scholar] [CrossRef]
- Frobell, R.B.; Le Graverand, M.-P.; Buck, R.; Roos, E.M.; Roos, H.P.; Tamez-Pena, J.; Totterman, S.; Lohmander, L.S. The Acutely ACL Injured Knee Assessed by MRI: Changes in Joint Fluid, Bone Marrow Lesions, and Cartilage during the First Year. Osteoarthr. Cartil. 2009, 17, 161–167. [Google Scholar] [CrossRef]
- Young, K.; Samiric, T.; Feller, J.; Cook, J. Extracellular Matrix Content of Ruptured Anterior Cruciate Ligament Tissue. Knee 2011, 18, 242–246. [Google Scholar] [CrossRef]
- Martirosian, P.; Grozinger, G.; Rauscher, I.; Wurslin, C.; Pohmann, R.; Springer, F.; Schick, F. Relaxometry of Tendons, Ligaments and Menisci in the Knee Joint at 3 T. In Proceedings of the 20th Annual Meeting and Exhibition of the International Society for Magnetic Resonance in Medicine, Singapore, 5–11 May 2012. [Google Scholar]
- Chu, C.R.; Williams, A.A. Quantitative MRI UTE-T2* and T2* Show Progressive and Continued Graft Maturation Over 2 Years in Human Patients After Anterior Cruciate Ligament Reconstruction. Orthop. J. Sports Med. 2019, 7, 2325967119863056. [Google Scholar] [CrossRef]
- Marieswaran, M.; Jain, I.; Garg, B.; Sharma, V.; Kalyanasundaram, D. A Review on Biomechanics of Anterior Cruciate Ligament and Materials for Reconstruction. Appl. Bionics Biomech. 2018, 2018, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Robi, K.; Jakob, N.; Matevz, K. The Physiology of Sports Injuries and Repair Processes in Current Issues in Sports and Exercise Medicine; InTech: London, UK, 2013; pp. 43–86. [Google Scholar]
- Zhu, J.; Zhang, X.; Ma, Y.; Zhou, C.; Ao, Y. Ultrastructural and Morphological Characteristics of Human Anterior Cruciate Ligament and Hamstring Tendons. Anat. Rec. (Hoboken) 2012, 295, 1430–1436. [Google Scholar] [CrossRef]
- Rumian, A.P.; Wallace, A.L.; Birch, H.L. Tendons and Ligaments Are Anatomically Distinct But Overlap in Molecular and Morphological Features-A Comparative Study in an Ovine Model. J. Orthop. Res. 2007, 25, 458–464. [Google Scholar] [CrossRef]
- Janssen, R.P.A.; Scheffler, S.U. Intra-Articular Remodelling of Hamstring Tendon Grafts after Anterior Cruciate Ligament Reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 2102–2108. [Google Scholar] [CrossRef] [PubMed]
- Falconiero, R.P.; DiStefano, V.J.; Cook, T.M. Revascularization and Ligamentization of Autogenous Anterior Cruciate Ligament Grafts in Human. Arthroscopy 1998, 14, 197–205. [Google Scholar] [CrossRef]
- Pauzenberger, L.; Syré, S.; Schurz, M. “Ligamentization” in Hamstring Tendon Grafts After Anterior Cruciate Ligament Reconstruction: A Systematic Review of the Literature and a Glimpse into the Future. Arthroscopy 2013, 29, 1712–1721. [Google Scholar] [CrossRef]
- Rougraff, B.; Shelbourne, K.D.; Gerth, P.K.; Warner, J. Arthroscopic and Histologic Analysis of Human Patellar Tendon Autografts Used for Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 1993, 21, 277–284. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, M.; Anitua, E.; Azofra, J.; Prado, R.; Muruzabal, F.; Andia, I. Ligamentization of Tendon Grafts Treated with and Endogenous Preparation Rich in Growth Factors: Gross Morphology and Histology. Arthroscopy 2010, 26, 470–480. [Google Scholar] [CrossRef]
- Nieminen, M.T.; Rieppo, J.; Töyräs, J.; Hakumäki, J.M.; Silvennoinen, J.; Hyttinen, M.M.; Helminen, H.J.; Jurvelin, J.S. T2 Relaxation Reveals Spatial Collagen Architecture in Articular Cartilage: A Comparative Quantitative MRI and Polarized Light Microscopic Study. Magn. Reson. Med. 2001, 46, 487–493. [Google Scholar] [CrossRef]
- Liebl, H.; Joseph, G.; Nevitt, M.C.; Singh, N.; Heilmeier, U.; Subburaj, K.; Jungmann, P.M.; McCulloch, C.E.; Lynch, J.A.; Lane, N.E.; et al. Early T2 Changes Predict Onset of Radiographic Knee Osteoarthritis: Data from the Osteoarthritis Initiative. Ann. Rheum. Dis. 2015, 74, 1353–1359. [Google Scholar] [CrossRef] [PubMed]
- Williams, J.R.; Neal, K.; Alfayyadh, A.; Lennon, K.; Capin, J.J.; Khandha, A.; Manal, K.; Potter, H.G.; Snyder-Mackler, L.; Buchanan, T.S. Knee Cartilage T2 Relaxation Times 3 Months after ACL Reconstruction are Associated with Knee Gait Variables Linked to Knee Osteoarthritis. J. Orthop. Res. 2021, 1–8. [Google Scholar] [CrossRef]
- Su, F.; Pedoia, V.; Teng, H.L.; Kretzschmar, M.; Lau, B.C.; McCulloch, C.E.; Link, T.M.; Ma, C.B.; Li, X. The Association between MR T1rho and T2 of Cartilage and Patient-Reported Outcomes after ACL Injury and Reconstruction. Osteoarthr. Cartil. 2016, 24, 1180–1189. [Google Scholar] [CrossRef]
- Eagle, S.; Potter, H.G.; Koff, M.F. Morphologic and Quantitative Magnetic Resonance Imaging of Knee Articular Cartilage for the Assessment of Post-Traumatic Osteoarthritis. J. Orthop. Res. 2017, 35, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Wrigley, T.V.; Bennell, K.L.; Wang, Y.; Fortin, K.; Cicuttini, F.M.; Lloyd, D.G.; Bryant, A.L. Cartilage Quantitative T2 Relaxation Time 2–4 Years Following Isolated Anterior Cruciate Ligament Reconstruction. J. Orthop. Res. 2018, 36, 2022–2029. [Google Scholar] [CrossRef]
- Li, H.; Chen, S.; Tao, H.; Chen, S. Quantitative MRI t2 Relaxation Time Evaluation of Knee Cartilage: Comparison of Meniscus-intact and Injured Knees after Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 2015, 43, 865–872. [Google Scholar] [CrossRef] [PubMed]
- van Ginckel, A.; Verdonk, P.; Victor, J.; Witvrouw, E. Cartilage status in Relation to Return to Sports after Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 2013, 41, 550–559. [Google Scholar] [CrossRef] [PubMed]
- Teng, H.L.; Wu, D.; Su, F.; Pedoia, V.; Souza, R.B.; Ma, C.B.; Li, X. Gait Characteristics Associated with a Greater Increase in Medial Knee Cartilage T1rho and T2 Relaxation Times in Patients Undergoing Anterior Cruciate Ligament Reconstruction. Am. J. Sports Med. 2017, 45, 3262–3271. [Google Scholar] [CrossRef]
- Potter, H.G.; Jain, S.K.; Ma, Y.; Black, B.R.; Fung, S.; Lyman, S. Cartilage Injury After Acute, Isolated Anterior Cruciate Ligament Tear. Am. J. Sports Med. 2012, 40, 276–285. [Google Scholar] [CrossRef]
- Zdanowicz, U.; Paśnik, B.C.M.; Drwięga, M.; Ratajczak, K.; Fulawka, K.; Lee, Y.C.; Śmigielski, R. Evaluation of ACL Graft Remodeling and Prediction of Graft Insufficiency in Sequenced MRI—Two-Year Follow-up. Appl. Sci. 2021, 11, 5278. [Google Scholar] [CrossRef]
- Kester, B.S.; Carpenter, P.M.; Yu, H.J.; Nozaki, T.; Kaneko, Y.; Yoshioka, H.; Schwarzkopf, R. T1ρ/T2 Mapping and Histopathology of Degenerative Cartilage in Advanced Knee Osteoarthritis. World J. Orthop. 2017, 8, 350–356. [Google Scholar] [CrossRef]
- Na, H.; Yan, Z.; Min, S.; Wu, Z.; Jin, J.; Fei, B.; Wei, M.; Jin, X.; Bo, J.; Dong, L.; et al. T2 Mapping of Articular Cartilage in Knee Osteoarthritis Using a Magnetic Resonance Staging. Zhongguo Yi Xue Ke Xue Yuan Xue Bao 2011, 33, 169–174. [Google Scholar] [CrossRef]
- Mittal, S.; Pradhan, G.; Singh, S.; Batra, R. T1 and T2 Mapping of Articular Cartilage and Menisci in Early Osteoarthritis of the Knee Using 3-Tesla Magnetic Resonance Imaging. Pol. J. Radiol. 2019, 84, e549–e564. [Google Scholar] [CrossRef]
- Li, X.; Kuo, D.; Theologis, A.; Carballido-Gamio, J.; Stehling, C.; Link, T.M.; Ma, C.B.; Majumdar, S. Cartilage in Anterior Cruciate Ligament–Reconstructed Knees: MR Imaging T1ρ and T2—Initial Experience with 1-year Follow-up. Radiology 2011, 258, 505–514. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age at Surgery (Years) | Treated | 21.2 ± 4.1 |
| Control | 28.8 ± 14.9 | |
| Time Injury-to-Surgery (Months) | 3.9 ± 2.3 | |
| BMI (kg/m2) | Pre-op | 23.5 ± 2.8 |
| FU4 | 23.0 ± 2.6 | |
| FU18 | 23.0 ± 2.6 | |
| Control | 22.4 ± 3.67 |
| KT-Load (mm) | KT-Man (mm) | Rolimeter (mm) | Kira (m/s2) | |||||
|---|---|---|---|---|---|---|---|---|
| Treated | Cont | Treated | Cont | Treated | Cont | Treated | Cont | |
| Pre-op | 8.5 ± 2.0 $* | 5.5 ± 2.1 * | 12.1 ± 2.7 * | 7.4 ± 2.0 * | 6.9 ± 1.7 $ @ | 4.7 ± 1.9 @ | 5.4 ± 1.9 | 3.6 ± 1.1 |
| FU4 | 7.1 ± 2.0 | 5.9 ± 2.1 | 10.9 ± 2.3 @ | 8.7 ± 2.1 @ | 5.6 ± 2.0 | 5.2 ± 2.6 | 3.1 ± 0.8 | 3.3 ± 0.8 |
| FU18 | 6.9 ± 2.5 $ @ | 5.1 ± 1.6 @ | 10.9 ± 3.1 @ | 8.6 ± 2.0 @ | 4.3 ± 1.7 $ | 4.0 ± 1.4 | 4.0 ± 1.9 | 3.8 ± 1.8 |
| T2 (ms) | Injured ACL | Pre-op | 57.9 ± 8.4 $ |
| Healthy ACL | Control | 66.3 ± 6.7 £ | |
| Graft | FU4 | 39.2 ± 10.5 $ £ | |
| Graft | FU18 | 37.7 ± 6.1 $ £ |
| T2 (ms) | pLTP | cMTP | cMFC | |
| Pre-op | 42.2 ± 3.9 | 37.1 ± 3.4 | 35.7 ± 5.2 | |
| FU4 | 42.2 ± 4.2 | 36.8 ± 3.4 | 33.7 ± 4.0 | |
| FU18 | 42.7 ± 3.7 | 35.4 ± 3.1 | 35.0 ± 4.3 | |
| Control | 38.3 ± 3.4 | 38.0 ± 5.4 | 33.9 ± 4.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marchiori, G.; Cassiolas, G.; Berni, M.; Grassi, A.; Dal Fabbro, G.; Fini, M.; Filardo, G.; Zaffagnini, S.; Lopomo, N.F. A Comprehensive Framework to Evaluate the Effects of Anterior Cruciate Ligament Injury and Reconstruction on Graft and Cartilage Status through the Analysis of MRI T2 Relaxation Time and Knee Laxity: A Pilot Study. Life 2021, 11, 1383. https://doi.org/10.3390/life11121383
Marchiori G, Cassiolas G, Berni M, Grassi A, Dal Fabbro G, Fini M, Filardo G, Zaffagnini S, Lopomo NF. A Comprehensive Framework to Evaluate the Effects of Anterior Cruciate Ligament Injury and Reconstruction on Graft and Cartilage Status through the Analysis of MRI T2 Relaxation Time and Knee Laxity: A Pilot Study. Life. 2021; 11(12):1383. https://doi.org/10.3390/life11121383
Chicago/Turabian StyleMarchiori, Gregorio, Giorgio Cassiolas, Matteo Berni, Alberto Grassi, Giacomo Dal Fabbro, Milena Fini, Giuseppe Filardo, Stefano Zaffagnini, and Nicola Francesco Lopomo. 2021. "A Comprehensive Framework to Evaluate the Effects of Anterior Cruciate Ligament Injury and Reconstruction on Graft and Cartilage Status through the Analysis of MRI T2 Relaxation Time and Knee Laxity: A Pilot Study" Life 11, no. 12: 1383. https://doi.org/10.3390/life11121383