
A Minimum Set of Physiological Parameters to Diagnose Obstructive Sleep Apnea Syndrome Using Non-Invasive Portable Monitors. A Systematic Review




Abstract
:1. Introduction
1.1. Review Questions
1.1.1. Main Review Question (MRQ)
1.1.2. Specific Review Questions (SRQ)
- Does the outcome (OSA detection) improve if the number of psychological parameters measured increases?
- What are the main requirements for the application of an in-home medical device to diagnose sleep apnea?
- Is there a set of minimum physiological signals that distinguish between detection of sleep and arousal?
- How does it affect the outcome (OSA detection) when PMs do not include oximetry measurement?
- What physiological signals are included in those PMs that meet the criteria of positive likelihood ratios (LR+) of ≥5 and sensitivities (Sen) of ≥0.825?
2. Materials and Methods
2.1. Eligibility Criteria
- ▪
- Study type: randomized controlled and clinical trials, research and review articles, and conference publications, along with clinical guidelines.
- ▪
- Population: studies with adult (>18) patients referred to sleep clinics with symptoms suggestive of OSA.
- ▪
- Grouping of studies: Differentiation between review publications and any other type of publication at the end of the search.
- ▪
- Outcome: set of physiological parameters of PM (preferably type III or type IV).
- ▪
- Exclusion criteria are shown as following:
- ▪
- The articles are not in English or German.
- ▪
- Published data are not available.
- ▪
- Studies are not related to monitoring or diagnosing OSA using a PM.
- ▪
- Studies of which the publication dates are older than 10 years when the systematic review is performed (2011–2021). Collop et al. conducted a review of studies covering PMs published prior to 2011 [10].
- ▪
- Studies where there are an underlying diseases and are not entirely focused on OSA. The accuracy of PMs for the detection of OSA may be affected, if there are comorbid medical conditions such as pulmonary disease, neuromuscular disease, or congestive heart failure.
- ▪
- PM (preferably type III or type IV) with a sensitivity of <0.825.
2.2. Search Strategy and Information Sources
2.3. Selection Process and Data Extraction
2.4. Assessment of the Risk of Bias
2.5. Synthesis Methods
3. Results
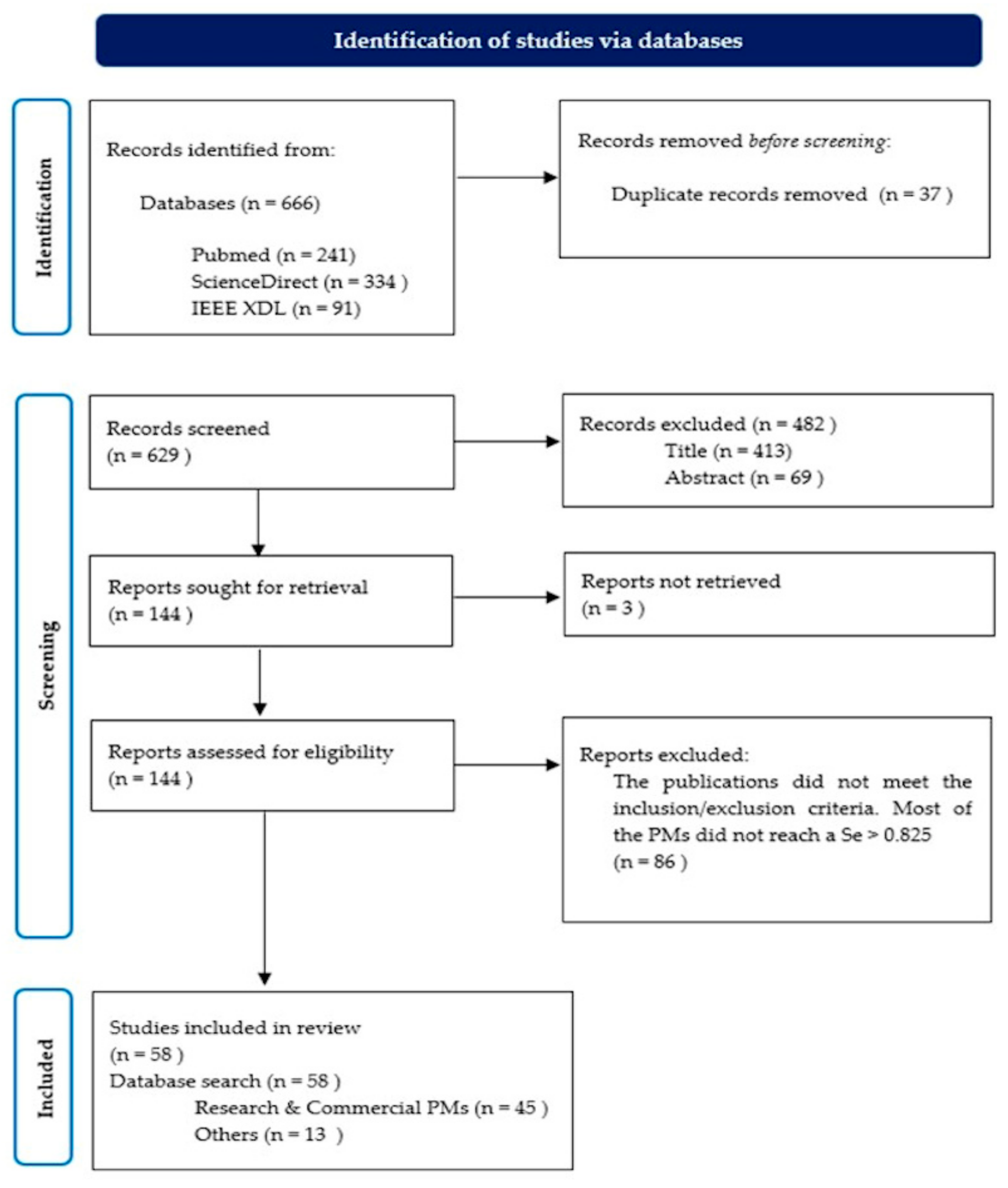
3.1. Study Selection
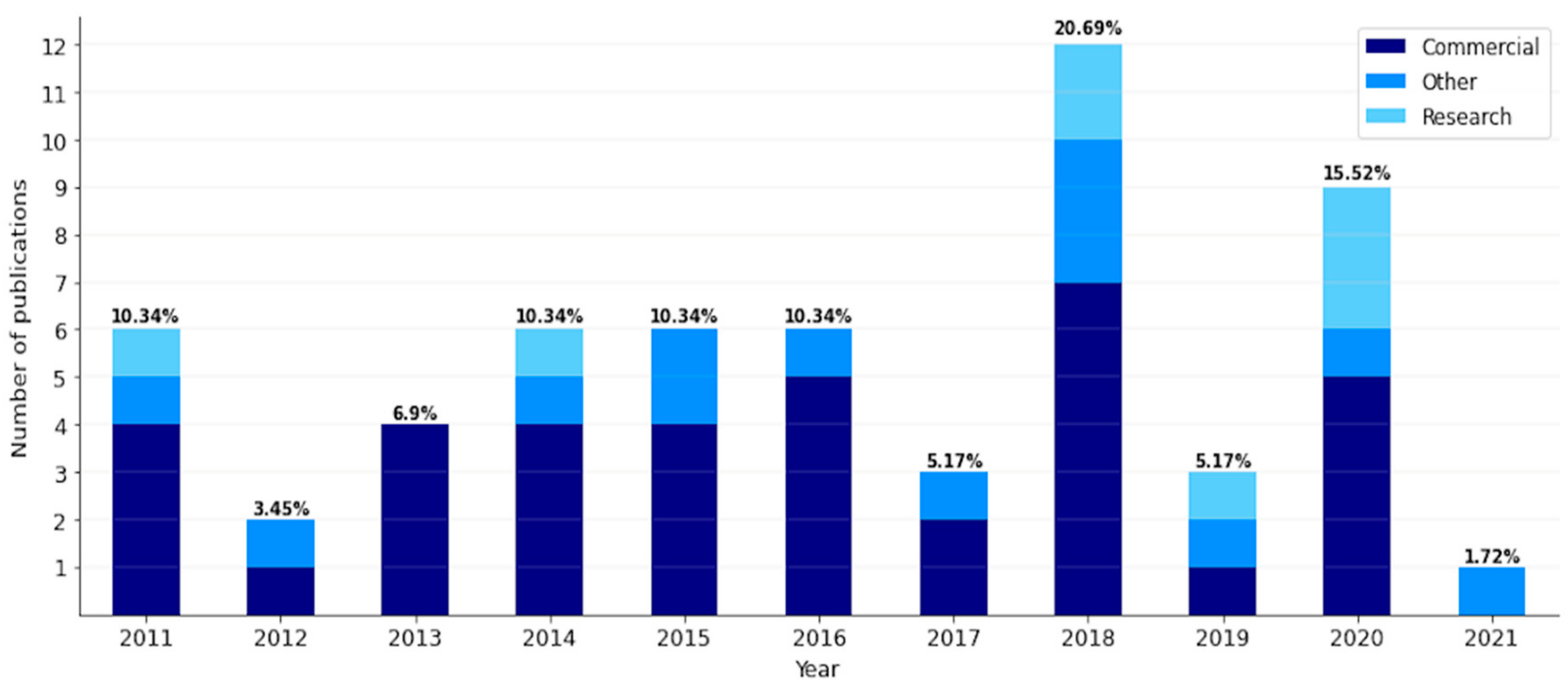
3.2. Study Characteristics and Individual Publications
3.3. Synthesis Results and Questions of Interest
3.3.1. MRQ: Is There a Minimum Set of Non-Invasive Parameters Measured to Diagnose, Detect or Monitor Sleep Apnea by In-Home PM?
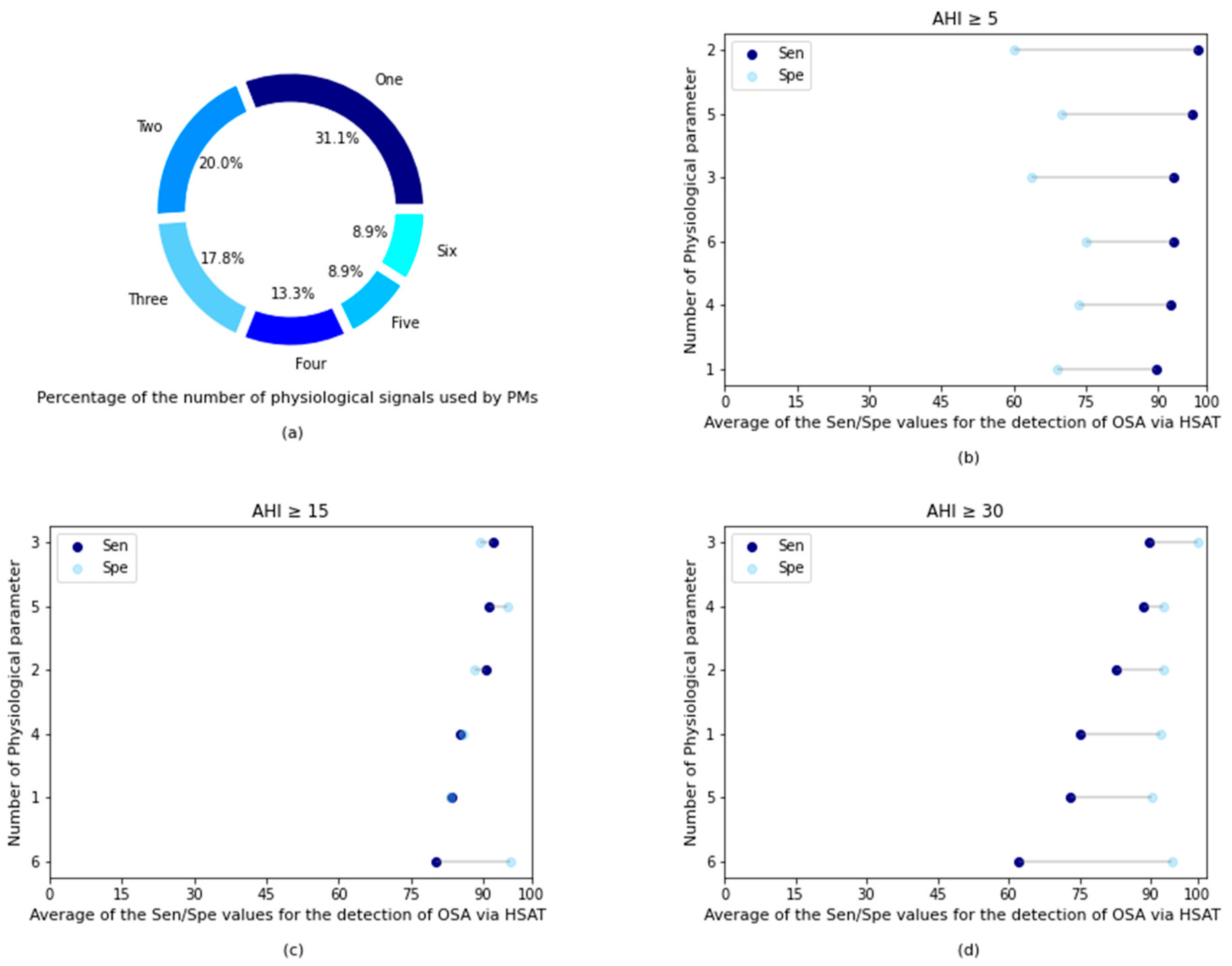
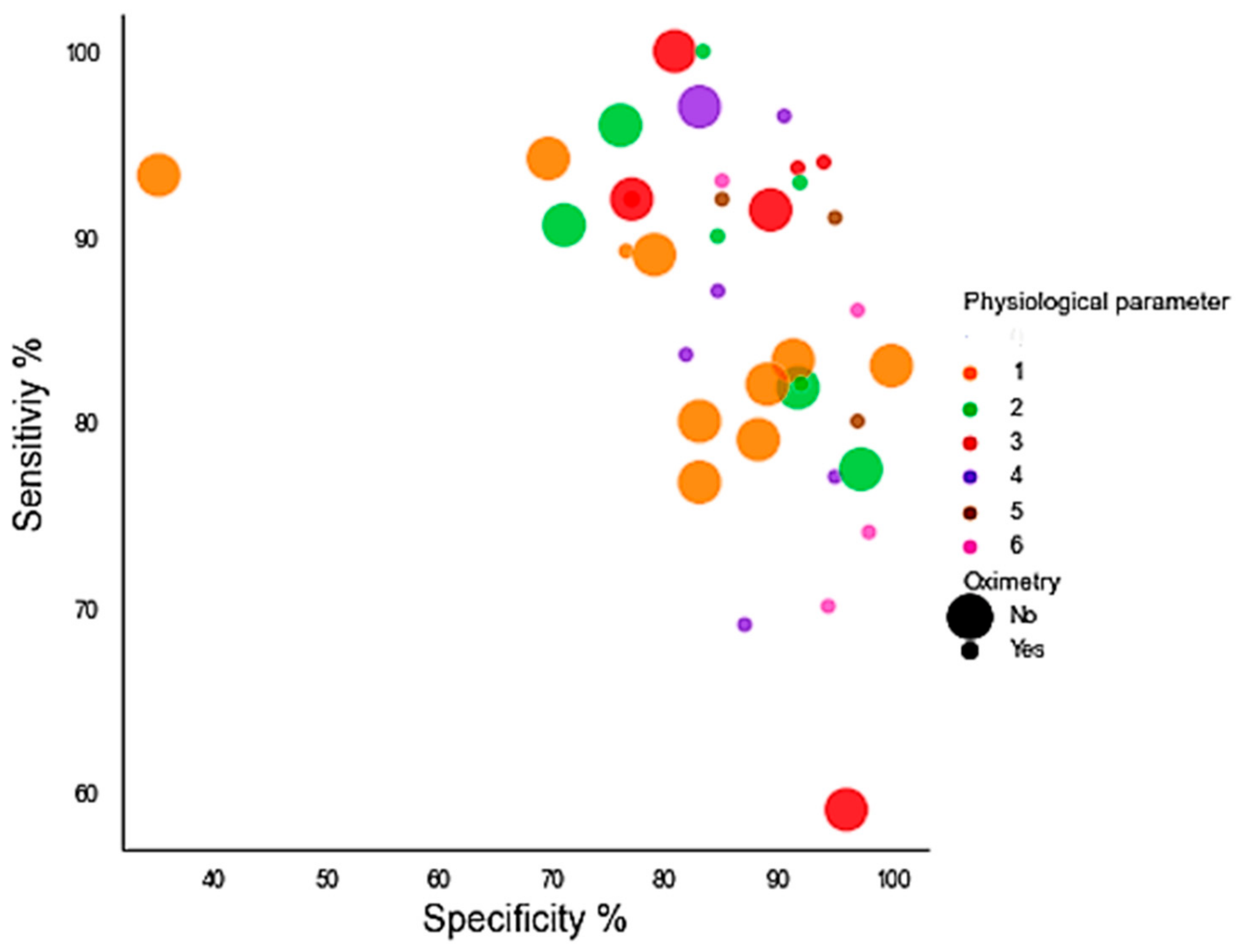
3.3.2. SRQ-1: Does the Outcome (OSA Detection) Improve if the Number of Psychological Parameters Measured Increases?
3.3.3. SRQ-2: What Are the Main Requirements for the Application of an In-Home Medical Device to Diagnose Sleep Apnea?
3.3.4. SRQ-3: Is There a Set of Minimum Physiological Signals That Distinguish between the Detection of Sleep and Arousal?
3.3.5. SRQ-4: How Does It Affect the Outcome (OSA Detection) When PMs Do Not Include Oximetry Measurements?
3.3.6. SRQ-5: What Physiological Signals Were Included in Those PMs That Met the Criteria of LR+ of ≥5 and Sensitivities (Sen) of ≥0.825?
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sateia, M.J. International Classification of Sleep Disorders-Third Edition Highlights and Modifications. Chest 2014, 146, 1387–1394. [Google Scholar] [CrossRef]
- Lo Bue, A.; Salvaggio, A.; Insalaco, G. Obstructive Sleep Apnea in Developmental Age. A Narrative Review. Eur. J. Pediatrics 2020, 179, 357–365. [Google Scholar] [CrossRef] [PubMed]
- Mendonça, F.; Mostafa, S.S.; Ravelo-García, A.G.; Morgado-Dias, F.; Penzel, T. Devices for Home Detection of Obstructive Sleep Apnea: A Review. Sleep Med. Rev. 2018, 41, 149–160. [Google Scholar] [CrossRef]
- Vat, S.; Haba-Rubio, J.; Tafti, M.; Tobback, N.; Andries, D.; Heinzer, R. Scoring Criteria for Portable Monitor Recordings: A Comparison of Four Hypopnoea Definitions in a Population-Based Cohort. Thorax 2015, 70, 1047–1053. [Google Scholar] [CrossRef] [Green Version]
- Corral-Peñafiel, J.; Pepin, J.L.; Barbe, F. Ambulatory Monitoring in the Diagnosis and Management of Obstructive Sleep Apnoea Syndrome. Eur. Respir. Rev. 2013, 22, 312–324. [Google Scholar] [CrossRef] [PubMed]
- Patil, S.P. Preoperative Evaluation of Obstructive Sleep Apnea: Home Sleep Testing versus Laboratory Testing. Sleep Med. Clin. 2013, 8, 73–91. [Google Scholar] [CrossRef]
- Kim, J.W.; Kim, T.; Shin, J.; Lee, K.; Choi, S.; Cho, S.W. Prediction of Apnea-Hypopnea Index Using Sound Data Collected by a Noncontact Device. Otolaryngol.-Head Neck Surg. 2020, 162, 392–399. [Google Scholar] [CrossRef]
- Mashaqi, S.; Staebler, D.; Mehra, R. Combined Nocturnal Pulse Oximetry and Questionnaire-Based Obstructive Sleep Apnea Screening—A Cohort Study. Sleep Med. 2020, 72, 157–163. [Google Scholar] [CrossRef]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef] [PubMed]
- Collop, N.A.; Tracy, S.L.; Kapur, V.; Mehra, R.; Kuhlmann, D.; Fleishman, S.A.; Ojile, J.M. Obstructive Sleep Apnea Devices for Out-Of-Center (OOC) Testing: Technology Evaluation. J. Clin. Sleep Med. 2011, 7, 531–548. [Google Scholar] [CrossRef] [Green Version]
- Hesselbacher, S.; Mattewal, A.; Hirshkowitz, M.; Sharafkhaneh, A. Classification, Technical Specifications, and Types of Home Sleep Testing Devices for Sleep-Disordered Breathing. Sleep Med. Clin. 2011, 6, 261–282. [Google Scholar] [CrossRef]
- Bianchi, M.T. Sleep Devices: Wearables and Nearables, Informational and Interventional, Consumer and Clinical. Metabolism 2018, 84, 99–108. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. Int. J. Surg. 2021, 88, 372. [Google Scholar] [CrossRef]
- Kirsch, D.B. PRO: Sliding into Home: Portable Sleep Testing Is Effective for Diagnosis of Obstructive Sleep Apnea. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2013, 9, 5–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jané, R.; Fiz, J.A.; Solà-Soler, J.; Mesquita, J.; Morera, J. Snoring Analysis for the Screening of Sleep Apnea Hypopnea Syndrome with a Single-Channel Device Developed Using Polysomnographic and Snoring Databases. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 8331–8333. [Google Scholar] [CrossRef]
- Driver, H.S.; Pereira, E.J.; Bjerring, K.; Toop, F.; Stewart, S.C.; Munt, P.W.; Fitzpatrick, M.F. Validation of the MediByte® Type 3 Portable Monitor Compared with Polysomnography for Screening of Obstructive Sleep Apnea. Can. Respir. J. 2011, 18, 137–143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nigro, C.A.; Dibur, E.; Aimaretti, S.; González, S.; Rhodius, E. Comparison of the Automatic Analysis versus the Manual Scoring from ApneaLinkTM Device for the Diagnosis of Obstructive Sleep Apnoea Syndrome. Sleep Breath. 2011, 15, 679–686. [Google Scholar] [CrossRef] [PubMed]
- Cheliout-Heraut, F.; Senny, F.; Djouadi, F.; Ouayoun, M.; Bour, F. Obstructive Sleep Apnoea Syndrome: Comparison between Polysomnography and Portable Sleep Monitoring Based on Jaw Recordings. Neurophysiol. Clin. 2011, 41, 191–198. [Google Scholar] [CrossRef]
- Oktay, B.; Rice, T.B.; Atwood, C.W.J.; Passero, M.J.; Gupta, N.; Givelber, R.; Drumheller, O.J.; Houck, P.; Gordon, N.; Strollo, P.J.J. Evaluation of a Single-Channel Portable Monitor for the Diagnosis of Obstructive Sleep Apnea. J. Clin. Sleep Med. 2011, 7, 384–390. [Google Scholar] [CrossRef] [Green Version]
- Ferré, A.; Sampol, G.; Jurado, M.J.; Cambrodi, R.; Lloberes, P.; Romero, O.; Ferré, Á.; Sampol, G.; Jurado, M.J.; Cambrodi, R.; et al. Neurophysiological Two-Channel Polysomnographic Device in the Diagnosis of Sleep Apnea. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2012, 8, 163–168. [Google Scholar] [CrossRef] [Green Version]
- Weimin, L.; Rongguang, W.; Dongyan, H.; Xiaoli, L.; Wei, J.; Shiming, Y. Assessment of a Portable Monitoring Device WatchPAT 200 in the Diagnosis of Obstructive Sleep Apnea. Eur. Arch. Otorhinolaryngol. 2013, 270, 3099–3105. [Google Scholar] [CrossRef]
- Masa, J. Effectiveness of Home Single-Channel Nasal Pressure for Sleep Apnea Diagnosis. Sleep Med. 2013, 14, e201. [Google Scholar] [CrossRef] [Green Version]
- Pereira, E.J.; Driver, H.S.; Stewart, S.C.; Fitzpatrick, M.F. Comparing a Combination of Validated Questionnaires and Level III Portable Monitor with Polysomnography to Diagnose and Exclude Sleep Apnea. J. Clin. Sleep Med. 2013, 9, 1259–1266. [Google Scholar] [CrossRef]
- Kobayashi, M.; Namba, K.; Tsuiki, S.; Nakamura, M.; Hayashi, M.; Mieno, Y.; Imizu, H.; Fujita, S.; Yoshikawa, A.; Sakakibara, H.; et al. Validity of Sheet-Type Portable Monitoring Device for Screening Obstructive Sleep Apnea Syndrome. Sleep Breath. 2013, 17, 589–595. [Google Scholar] [CrossRef]
- Meissner, W.G.; Flabeau, O.; Perez, P.; Taillard, J.; Marquant, F.; Dupouy, S.; Tison, F.; Philip, P.; Ghorayeb, I. Accuracy of Portable Polygraphy for the Diagnosis of Sleep Apnea in Multiple System Atrophy. Sleep Med. 2014, 15, 476–479. [Google Scholar] [CrossRef] [PubMed]
- Cairns, A.; Wickwire, E.; Schaefer, E.; Nyanjom, D. A Pilot Validation Study for the NOX T3(TM) Portable Monitor for the Detection of OSA. Sleep Breath. 2014, 18, 609–614. [Google Scholar] [CrossRef]
- Fredheim, J.M.; Røislien, J.; Hjelmesæth, J. Validation of a Portable Monitor for the Diagnosis of Obstructive Sleep Apnea in Morbidly Obese Patients. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2014, 10, 751–775. [Google Scholar] [CrossRef] [Green Version]
- Garg, N.; Rolle, A.J.; Lee, T.A.; Prasad, B. Home-Based Diagnosis of Obstructive Sleep Apnea in an Urban Population. J. Clin. Sleep Med. 2014, 10, 879–885. [Google Scholar] [CrossRef]
- Rodriguez-Villegas, E.; Chen, G.; Radcliffe, J.; Duncan, J. A Pilot Study of a Wearable Apnoea Detection Device. BMJ Open 2014, 4, e005299. [Google Scholar] [CrossRef] [PubMed]
- Levendowski, D.J.; Veljkovic, B.; Seagraves, S.; Westbrook, P.R. Capability of a Neck Worn Device to Measure Sleep/Wake, Airway Position, and Differentiate Benign Snoring from Obstructive Sleep Apnea. J. Clin. Monit. Comput. 2015, 29, 53–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Vries, G.E.; van der Wal, H.H.; Kerstjens, H.A.M.; van Deursen, V.M.; Stegenga, B.; van Veldhuisen, D.J.; van der Hoeven, J.H.; van der Meer, P.; Wijkstra, P.J. Validity and Predictive Value of a Portable Two-Channel Sleep-Screening Tool in the Identification of Sleep Apnea in Patients with Heart Failure. J. Card. Fail. 2015, 21, 848–855. [Google Scholar] [CrossRef] [PubMed]
- Zou, J.; Meng, L.; Liu, Y.; Xu, X.; Liu, S.; Guan, J.; Yin, S.; Yi, H. Evaluation of a 2-Channel Portable Device and a Predictive Model to Screen for Obstructive Sleep Apnea in a Laboratory Environment. Respir. Care 2015, 60, 356–362. [Google Scholar] [CrossRef] [Green Version]
- Alshaer, H.; Fernie, G.R.; Tseng, W.H.; Bradley, T.D. Comparison of In-Laboratory and Home Diagnosis of Sleep Apnea Using a Cordless Portable Acoustic Device. Sleep Med. 2015, 22, 91–96. [Google Scholar] [CrossRef]
- Gutiérrez-Tobal, G.C.; Álvarez, D.; Crespo, A.; Arroyo, C.A.; Vaquerizo-Villar, F.; Barroso-García, V.; del Campo, F.; Hornero, R. Multi-Class Adaboost to Detect Sleep Apnea-Hypopnea Syndrome Severity from Oximetry Recordings Obtained at Home. In Proceedings of the 2016 Global Medical Engineering Physics Exchanges/Pan American Health Care Exchanges (GMEPE/PAHCE), Madrid, Spain, 4–9 April 2016; pp. 1–5. [Google Scholar] [CrossRef] [Green Version]
- Alakuijala, A.; Salmi, T. Predicting Obstructive Sleep Apnea with Periodic Snoring Sound Recorded at Home. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2016, 12, 953–958. [Google Scholar] [CrossRef] [PubMed]
- Nagubadi, S.; Mehta, R.; Abdoh, M.; Nagori, M.; Littleton, S.; Gueret, R.; Tulaimat, A. The Accuracy of Portable Monitoring in Diagnosing Significant Sleep Disordered Breathing in Hospitalized Patients. PLoS ONE 2016, 11, e0168073. [Google Scholar] [CrossRef]
- Ryan, C.M.; Wilton, K.; Bradley, T.D.; Alshaer, H. In-Hospital Diagnosis of Sleep Apnea in Stroke Patients Using a Portable Acoustic Device. Sleep Breath. 2016, 21, 453–460. [Google Scholar] [CrossRef]
- Álvarez, D.; Gutiérrez-Tobal, G.C.; Vaquerizo-Villar, F.; Barroso-García, V.; Crespo, A.; Arroyo, C.A.; Del Campo, F.; Hornero, R. Automated Analysis of Unattended Portable Oximetry by Means of Bayesian Neural Networks to Assist in the Diagnosis of Sleep Apnea. In Proceedings of the 2016 Global Medical Engineering Physics Exchanges/Pan American Health Care Exchanges (GMEPE/PAHCE), Madrid, Spain, 4–9 April 2016; pp. 1–4. [Google Scholar] [CrossRef] [Green Version]
- Durán-Cantolla, J.; Zamora Almeida, G.; Vegas Diaz de Guereñu, O.; Saracho Rotaeche, L.; Hamdan Alkhraisat, M.; Durán Carro, J.; Egea Santaolalla, C.; Anitua, E. Validation of a New Domiciliary Diagnosis Device for Automatic Diagnosis of Patients with Clinical Suspicion of OSA. Respirology 2017, 22, 378–385. [Google Scholar] [CrossRef] [PubMed]
- Xu, L.; Han, F.; Keenan, B.T.; Kneeland-Szanto, E.; Yan, H.; Dong, X.; Chang, Y.; Zhao, L.; Zhang, X.; Li, J.; et al. Validation of the Nox-T3 Portable Monitor for Diagnosis of Obstructive Sleep Apnea in Chinese Adults. J. Clin. Sleep Med. 2017, 13, 675–683. [Google Scholar] [CrossRef] [Green Version]
- Barbieri, F.; Dichtl, W.; Heidbreder, A.; Brandauer, E.; Stefani, A.; Adukauskaite, A.; Senoner, T.; Schgör, W.; Hintringer, F.; Högl, B. Sleep Apnea Detection by a Cardiac Resynchronization Device Integrated Thoracic Impedance Sensor: A Validation Study against the Gold Standard Polysomnography. PLoS ONE 2018, 13, e0195573. [Google Scholar] [CrossRef]
- Gumb, T.; Twumasi, A.; Alimokhtari, S.; Perez, A.; Black, K.; Rapoport, D.M.; Sunderram, J.; Ayappa, I. Comparison of Two Home Sleep Testing Devices with Different Strategies for Diagnosis of OSA. Sleep Breath. 2018, 22, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Mosquera-Lopez, C.; Leitschuh, J.; Condon, J.; Hagen, C.C.; Hanks, C.; Jacobs, P.G. In-Home Sleep Apnea Severity Classification Using Contact-Free Load Cells and an AdaBoosted Decision Tree Algorithm. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; pp. 6044–6047. [Google Scholar] [CrossRef]
- Massie, F.; Mendes de Almeida, D.; Dreesen, P.; Thijs, I.; Vranken, J.; Klerkx, S. An Evaluation of the NightOwl Home Sleep Apnea Testing System. J. Clin. Sleep Med. 2018, 14, 1791–1796. [Google Scholar] [CrossRef]
- Weinreich, G.; Terjung, S.; Wang, Y.; Werther, S.; Zaffaroni, A.; Teschler, H. Validation of a Non-Contact Screening Device for the Combination of Sleep-Disordered Breathing and Periodic Limb Movements in Sleep. Sleep Breath. 2018, 22, 131–138. [Google Scholar] [CrossRef]
- Magnusdottir, S.; Hilmisson, H. Ambulatory Screening Tool for Sleep Apnea: Analyzing a Single-Lead Electrocardiogram Signal (ECG). Sleep Breath. 2018, 22, 421–429. [Google Scholar] [CrossRef]
- Araújo, I.; Marques, F.; André, S.; Araújo, M.; Marques, S.; Ferreira, R.; Moniz, P.; Proença, M.; Borrego, P.; Fonseca, C. Diagnosis of Sleep Apnea in Patients with Stable Chronic Heart Failure Using a Portable Sleep Test Diagnostic Device. Sleep Breath. 2018, 22, 749–755. [Google Scholar] [CrossRef]
- Bonnesen, M.P.; Sorensen, H.B.D.; Jennum, P. Mobile Apnea Screening System for At-Home Recording and Analysis of Sleep Apnea Severity. In Proceedings of the 2018 40th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Honolulu, HI, USA, 18–21 July 2018; pp. 457–460. [Google Scholar] [CrossRef]
- Faßbender, P.; Haddad, A.; Bürgener, S.; Peters, J. Validation of a Photoplethysmography Device for Detection of Obstructive Sleep Apnea in the Perioperative Setting. J. Clin. Monit. Comput. 2018, 33, 341–345. [Google Scholar] [CrossRef]
- Mosquera-Lopez, C.; Leitschuh, J.; Condon, J.; Hagen, C.C.; Rajhbeharrysingh, U.; Hanks, C.; Jacobs, P.G. Design and Evaluation of a Non-Contact Bed-Mounted Sensing Device for Automated in-Home Detection of Obstructive Sleep Apnea: A Pilot Study. Biosensors 2019, 9, 90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, Y.; Xu, L.; Han, F.; Keenan, B.T.; Kneeland-Szanto, E.; Zhang, R.; Zhang, W.; Yu, Y.; Zuo, Y.; Pack, A.I.; et al. Validation of the NOX-T3 Portable Monitor for Diagnosis of Obstructive Sleep Apnea in Patients with Chronic Obstructive Pulmonary Disease. J. Clin. Sleep Med. 2019, 15, 587–596. [Google Scholar] [CrossRef] [PubMed]
- Hayanoid, J.; Yamamoto, H.; Nonaka, I.; Komazawaid, M.; Itao, K.; Ueda, N.; Tanaka, H.; Yuda, E. Quantitative Detection of Sleep Apnea with Wearable Watch Device. PLoS ONE 2020, 15, e0237279. [Google Scholar] [CrossRef]
- Fitzpatrick, M.; Rac, V.E.; Mitsakakis, N.; Abrahamyan, L.; Pechlivanoglou, P.; Chung, S.; Carcone, S.M.; Pham, B.; Kendzerska, T.; Zwarenstein, M.; et al. SIESTA-Home Sleep Study with BresoDx for Obstructive Sleep Apnea: A Randomized Controlled Trial. Sleep Med. 2020, 65, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.; Park, J.; Hay, K.; Hoey, L.; Leong, G.; Leong, M.; Downey, C.; Curtin, D.; Tay, G. Use of a Limited-Channel Device for Obstructive Sleep Apnoea Diagnosis in a Tertiary Sleep Disorders Centre. Intern. Med. J. 2020, 50, 1109–1114. [Google Scholar] [CrossRef]
- Młyńczak, M.; Valdez, T.A.; Kukwa, W. Joint Apnea and Body Position Analysis for Home Sleep Studies Using a Wireless Audio and Motion Sensor. IEEE Access 2020, 8, 170579–170587. [Google Scholar] [CrossRef]
- Saha, S.; Kabir, M.; Montazeri Ghahjaverestan, N.; Hafezi, M.; Gavrilovic, B.; Zhu, K.; Alshaer, H.; Yadollahi, A. Portable Diagnosis of Sleep Apnea with the Validation of Individual Event Detection. Sleep Med. 2020, 69, 51–57. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y.; Kasagi, S.; Tamura, H.; Kawana, F.; Tomita, Y.; Narui, K.; Kasai, T. Clinical Utility of a Type 4 Portable Device for In-Home Screening of Sleep Disordered Breathing. Ann. Cardiothorac. Surg. 2020, 9, 2895–2902. [Google Scholar] [CrossRef]
- Dzięciołowska-Baran, E.; Gawlikowska-Sroka, A.; Szczurowski, J. Diagnosis of Sleep-Disordered Breathing in the Home Environment. In Advances in Experimental Medicine and Biology; Springer: Berlin/Heidelberg, Germany, 2020; Volume 1271, pp. 107–112. [Google Scholar] [CrossRef]
- Ferrer-Lluis, I.; Castillo-Escario, Y.; Montserrat, J.M.; Jané, R. Analysis of Smartphone Triaxial Accelerometry for Monitoring Sleep-Disordered Breathing and Sleep Position at Home. IEEE Access 2020, 8, 71231–71244. [Google Scholar] [CrossRef]
- Berry, R.B. Chapter 13-Polysomnography, Portable Monitoring, and Actigraphy; Berry, R.B., Ed.; W.B. Saunders: Saint Louis, MI, USA, 2012; pp. 189–218. [Google Scholar] [CrossRef]
- El Shayeb, M.; Topfer, L.-A.; Stafinski, T.; Pawluk, L.; Menon, D. Diagnostic Accuracy of Level 3 Portable Sleep Tests versus Level 1 Polysomnography for Sleep-Disordered Breathing: A Systematic Review and Meta-Analysis. Can. Med. Assoc. J. 2014, 186, E25–E51. [Google Scholar] [CrossRef] [Green Version]
- Dawson, A.; Loving, R.T.; Gordon, R.M.; Abel, S.L.; Loewy, D.; Kripke, D.F.; Kline, L.E. Type III Home Sleep Testing versus Pulse Oximetry: Is the Respiratory Disturbance Index Better than the Oxygen Desaturation Index to Predict the Apnoea-Hypopnoea Index Measured during Laboratory Polysomnography? BMJ Open 2015, 5, e007956. [Google Scholar] [CrossRef] [Green Version]
- Cooksey, J.A.; Balachandran, J.S. Portable Monitoring for the Diagnosis of OSA. Chest 2016, 149, 1074–1081. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, M.T.; Goparaju, B. Potential Underestimation of Sleep Apnea Severity by At-Home Kits: Rescoring In-Laboratory Polysomnography Without Sleep Staging. J. Clin. Sleep Med. JCSM Off. Publ. Am. Acad. Sleep Med. 2017, 13, 551–555. [Google Scholar] [CrossRef]
- Jiang, P.; Zhu, R.; Dong, X.; Chang, Y. Combination Mode of Physiological Signals for Diagnosis of OSAS Using Portable Monitor. Sleep Breath. 2018, 22, 123–129. [Google Scholar] [CrossRef]
- Light, M.P.; Casimire, T.N.; Chua, C.; Koushyk, V.; Burschtin, O.E.; Ayappa, I.; Rapoport, D.M. Addition of Frontal EEG to Adult Home Sleep Apnea Testing: Does a More Accurate Determination of Sleep Time Make a Difference? Sleep Breath. 2018, 22, 1179–1188. [Google Scholar] [CrossRef] [PubMed]
- Lachapelle, P.; Cascon, J.; Pamidi, S.; Kimoff, R.J. Accuracy of Portable Devices in Sleep Apnea Using Oximetry-Derived Heart Rate Increases as a Surrogate Arousal Marker. Sleep Breath. 2019, 23, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Collop, N. Chapter 5-Home Sleep Testing, 2nd ed.; Friedman, M., Jacobowitz, O.B.T.-S.A., Eds.; Elsevier: London, UK, 2020; pp. 32–34. [Google Scholar] [CrossRef]
- Kwon, S.; Kim, H.; Yeo, W.-H.H. Recent Advances in Wearable Sensors and Portable Electronics for Sleep Monitoring. iScience 2021, 24, 102461. [Google Scholar] [CrossRef] [PubMed]
- Collop, N.A.; Anderson, W.M.D.; Boehlecke, B.; Claman, D.; Goldberg, R.; Gottlieb, D.J.; Hudgel, D.; Sateia, M.; Schwab, R. Clinical Guidelines for the Use of Unattended Portable Monitors in the Diagnosis of Obstructive Sleep Apnea in Adult Patients. J. Clin. Sleep Med. 2007, 3, 737–747. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Publication | SCOPER Cat | Sen | Spe | AHI | Pop | Type Device |
|---|---|---|---|---|---|---|
| Jané, R. et al., 2011 [15] | R5A1 | 83 | 100 | 15 | 35 | Research |
| Driver et al., 2011 [16] | S3C4O1xP2E4R2 | 97 | 67 | 5 | 73 | Commercial |
| 80 | 97 | 15 | ||||
| 70 | 100 | 30 | ||||
| Nigro et al., 2011 [17] | R2 | 89.3 | 60 | 5 | 96 | Commercial |
| 76.7 | 83 | 15 | ||||
| 88.5 | 95.3 | 30 | ||||
| Cheliout-Heraut et al., 2011 [18] | S3O1xP2E2Rx | 83.6 | 81.8 | 5 | 90 | Commercial |
| 15 | ||||||
| 30 | ||||||
| Oktay et al., 2011 [19] | R2 | 90 | 76.9 | 5 | 53 | Commercial |
| 79 | 88.2 | 15 | ||||
| 66.7 | 95.9 | 30 | ||||
| Ferré et al., 2012 [20] | S2C4OxP2ExR2 | 91 | 77 | 5 | 68 | Commercial |
| 86 | 97 | 15 | ||||
| 61 | 96 | 30 | ||||
| Weimin et al., 2013 [21] | S3C2O1x | 95.8 | 100 | 5 | 28 | Commercial |
| 93.7 | 91.7 | 15 | ||||
| 85.7 | 100 | 30 | ||||
| Masa et al., 2013 [22] | R2 | 94 | 35 | 5 | 595 | Commercial |
| 80 | 83 | 15 | ||||
| Pereira et al., 2013 [23] | O1xPxE1R2 | 87 | 67 | 5 | 128 | Commercial |
| 77 | 95 | 15 | ||||
| 50 | 93 | 30 | ||||
| Kobayashi et al., 2013 [24] | O1xC4P2R5 | 100 | 66.7 | 5 | 60 | Commercial |
| 96.9 | 90.5 | 15 | ||||
| Meissner et al., 2014 [25] | O1xR2E1 | 87.5 | 80 | 5 | 23 | Commercial |
| Cairns et al., 2014 [26] | S3O1xP2E1R2Ax | 100 | 70 | 5 | 32 | Commercial |
| 92 | 85 | 15 | ||||
| Fredheim et al., 2014 [27] | C4O1xR2 | 93 | 71 | 5 | 99 | Commercial |
| 94 | 94 | 15 | ||||
| 90 | 1.0 | 30 | ||||
| Garg et al., 2014 [28] | S3C2O1x | 96 | 43 | 5 | 75 | Commercial |
| 92 | 77 | 15 | ||||
| Rodriguez-Villegas et al., 2014 [29] | R5Ax | 89 | 100 | - | 30 | Research |
| Levendowski et al., 2015 [30] | P2R5A1 | 85 | 90 | 5 | 24 | Commercial |
| 100 | 80.8 | 15 | ||||
| de Vries et al., 2015 [31] | C4O1xR2 | 98.2 | 60.0 | 5 | 90 | Commercial |
| 92.9 | 91.9 | 15 | ||||
| Zou et al., 2015 [32] | C4O1xR2 | 80.28 | 95.45 | 5 | 93 | Commercial |
| 87.04 | 84.62 | 15 | ||||
| 94.87 | 92.59 | 30 | ||||
| Alshaer et al., 2015 [33] | R5A1 | 98.1 | 82.8 | 5 | 135 | Commercial |
| 77.4 | 97.3 | 15 | ||||
| 65.6 | 100 | 30 | ||||
| Gutiérrez-Tobal et al., 2016 [34] | O1 | 90.6 | 80 | 5 | 320 | Commercial |
| 89.2 | 76.5 | 15 | ||||
| 63.9 | 89.1 | 30 | ||||
| Alakuijala et al., 2016 [35] | R5A1 | 93.3 | 35.1 | 15 | 211 | Commercial |
| Nagubadi et al., 2016 [36] | S3O1xE4R1 | 69 | 87 | 15 | 71 | Commercial |
| 87 | 66 | 30 | ||||
| Ryan, C.M. et al., 2016 [37] | R5A1 | 90 | 84.6 | 15 | 23 | Commercial |
| 100 | 85.7 | 30 | ||||
| Álvarez et al., 2016 [38] | O1 | 94.2 | 69.6 | 15 | 320 | Commercial |
| Durán-Cantolla et al., 2017 [39] | S3C4O1P2E4R2A2 | 88.2 | 72.7 | 5 | 28 | Commercial |
| 70.0 | 94.4 | 15 | ||||
| 100 | 92.6 | 30 | ||||
| Xu et al., 2017 [40] | S3O1xP2E1R2Ax | 95 | 69 | 5 | 80 | Commercial |
| 93 | 85 | 15 | ||||
| 63 | 93 | 30 | ||||
| Barbieri et al., 2018 [41] | R5 | 83.3 | 60 | 30 | 21 | Commercial |
| Gumb et al., 2018 [42] | O1 | 85.9 | 76.5 | 5 | 178 | Research |
| Mosquera-López et al., 2018 [43] | P2R5 | 81.82 | 91.7 | 15 | 14 | Commercial |
| Massie et al., 2018 [44] | S4C2O1xP2 | 98 | 80 | 5 | 101 | Commercial |
| 97 | 83 | 15 | ||||
| 90 | 97 | 30 | ||||
| Weinreich et al., 2018 [45] | P2R5 | 97.9 | 41.7 | 5 | 57 | Commercial |
| 90.6 | 71.0 | 15 | ||||
| Magnusdottir et al., 2018 [46] | C3 | 89 | 79 | 15 | 47 | Commercial |
| Araújo et al., 2018 [47] | R2 | 81.8 | 61.5 | 5 | 35 | Research |
| 83.3 | 91.3 | 15 | ||||
| Bonnesen et al., 2018 [48] | P2A1 | 100 | - | 5 | 23 | Commercial |
| 92.3 | - | 15 | ||||
| Faßbender et al., 2018 [49] | O1xR2 | 100 | 44 | 5 | 48 | Research |
| 92 | 77 | 15 | ||||
| Mosquera-López et al., 2019 [50] | P2R5 | 88.9 | 76.5 | 15 | 14 | Commercial |
| Chang et al., 2019 [51] | S3C4O1xP2E1R2Ax | 95 | 78 | 5 | 90 | Commercial |
| 74 | 98 | 15 | ||||
| 58 | 98 | 30 | ||||
| Hayano et al., 2020 [52] | C5 | 82 | 89 | 15 | 41 | Commercial |
| Fitzpatrick et al., 2020 [53] | P2R5A1 | 85 | 48 | 5 | 233 | Commercial |
| 59 | 96 | 15 | ||||
| Smith et al., 2020 [54] | O1xR2 | 82 | 92 | 15 | 100 | Research |
| Mlynczak et al., 2020 [55] | S3P2A1 | 96 | 76 | 15 | 30 | Research |
| Saha et al., 2020 [56] | S3P2R5A1 | 93.12 | 56.06 | 5 | 69 | Commercial |
| 91.42 | 89.29 | 15 | ||||
| 89.70 | 98.03 | 30 | ||||
| Yamada et al., 2020 [57] | O1xP2R1,5A1 | 82.8 | 76 | 5 | 387 | Commercial |
| 75.8 | 80.4 | 30 | ||||
| Dzieciolowska-Baran et al., 2020 [58] | C4O1xExRx | 91 | 95 | 15 | 68 | Research |
| Ferrer-Lluis et al., 2020 [59] | S3P2 | 90 | - | 15 | 13 | Research |
| Publication | Objective | Type of Publication |
|---|---|---|
| Hesselbacher et al., 2011 [11] | Discussing the technical aspects and options available for portable home testing devices to diagnose sleep apnea. | Review article |
| Berry et al., 2012 [60] | Polysomnography (PSG), portable monitoring, and actigraphy when it comes to detecting OSA. | Book chapter |
| Shayeb et al., 2014 [61] | Systematic review and meta-analysis of comparative studies of level 3 versus level 1 sleep tests in adults with suspected sleep-disordered breathing. | Review article |
| Dawson et al., 2015 [62] | Comparison between the ability of the oxygen desaturation index (ODI) based on oximetry alone with a standalone pulse oximeter (SPO) and the respiratory disturbance index (RDI) to predict the AHI. | Research article |
| Vat et al., 2015 [4] | Investigating the performance of four different hypopnea scoring criteria, using 3% or 4% oxygen desaturation levels, with or without PWA drops as surrogates for electroencephalogram (EEG) arousals, and determine the impact of the measured versus the reported sleep time on OSA diagnosis. | Research article |
| Cooksey et al., 2016 [63] | Discussing society guidelines and recent research in the growing field of portable monitoring for OSA detection. | Review article |
| Bianchi et al., 2017 [64] | Studying the feasibility of home sleep apnea tests (HSAT) kits as they are known to underestimate the severity of sleep apnea, in part due to lack of sleep staging to provide total sleep time. | Research article |
| Jiang et al., 2018 [65] | Evaluating the combination modes of key physiological signals collected by portable sensor modules for OSA detection compared to PSG. | Research article |
| Light et al., 2018 [66] | Validating a single-channel frontal EEG for scoring sleep versus wake against full EEG during PSG and then examining the utility of adding this single-channel EEG to standard HSAT to prevent false-negative results. | Research article |
| Mendonça et al., 2018 [3] | Reviewing publications that show the performances of different devices for the ambulatory diagnosis of sleep apnea. | Review article |
| Lachapelle et al., 2018 [67] | Testing the hypothesis that scoring hypopneas using heart rate accelerations as a surrogate marker for cortical arousal (autonomic hypopnea; AnH) improves the accuracy of HSAT for OSA diagnosis, using PSG as the diagnostic gold standard. | Research article |
| Collop et al., 2020 [68] | HSAT overview. | Book chapter |
| Kwon et al., 2021 [69] | Summarizing recent results in the development of novel portable and wearable sensors for sleep monitoring. | Review article |
| Publication | SCOPER Cat | AHI-5-Sen | AHI-5-Spe | Pop | LR+ | LR− |
|---|---|---|---|---|---|---|
| Weimin et al., 2013 [21] | S3C2O1x | 95.80 | 100.00 | 28 | inf | 99.04 |
| Levendowski et al., 2015 [30] | P2R5A1 | 85.00 | 90.00 | 24 | 8.5 | 99.05 |
| Zou et al., 2015 [32] | C4O1xR2aAx | 80.28 | 95.45 | 93 | 17.6 | 99.15 |
| Alshaer et al., 2015 [33] | R5A1 | 98.10 | 82.80 | 135 | 5.7 | 98.8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Serrano Alarcón, Á.; Martínez Madrid, N.; Seepold, R. A Minimum Set of Physiological Parameters to Diagnose Obstructive Sleep Apnea Syndrome Using Non-Invasive Portable Monitors. A Systematic Review. Life 2021, 11, 1249. https://doi.org/10.3390/life11111249
Serrano Alarcón Á, Martínez Madrid N, Seepold R. A Minimum Set of Physiological Parameters to Diagnose Obstructive Sleep Apnea Syndrome Using Non-Invasive Portable Monitors. A Systematic Review. Life. 2021; 11(11):1249. https://doi.org/10.3390/life11111249
Chicago/Turabian StyleSerrano Alarcón, Ángel, Natividad Martínez Madrid, and Ralf Seepold. 2021. "A Minimum Set of Physiological Parameters to Diagnose Obstructive Sleep Apnea Syndrome Using Non-Invasive Portable Monitors. A Systematic Review" Life 11, no. 11: 1249. https://doi.org/10.3390/life11111249