
Modified VMAT Plans for Locally Advanced Centrally Located Non-Small Cell Lung Cancer (NSCLC)

Abstract
:1. Introduction
2. Materials and Methodology
2.1. Patient Selection
2.2. Simulation
2.3. Image Registration, Target Volume and OAR Contouring
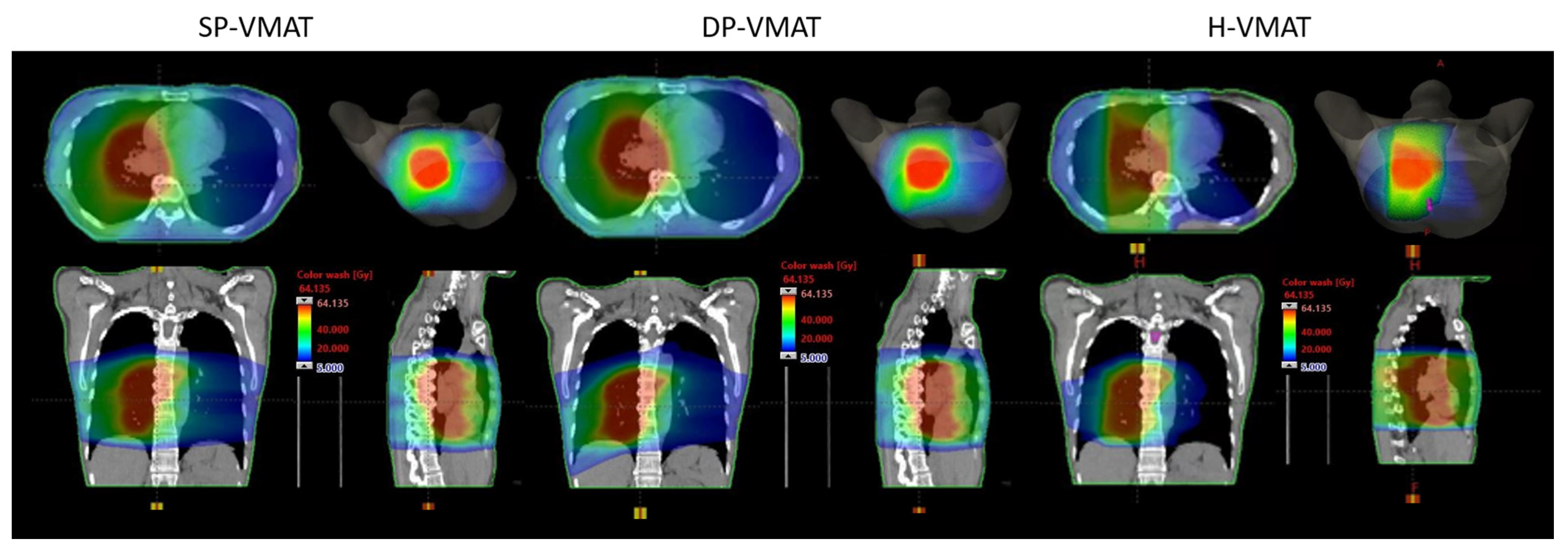
2.4. Treatment Planning
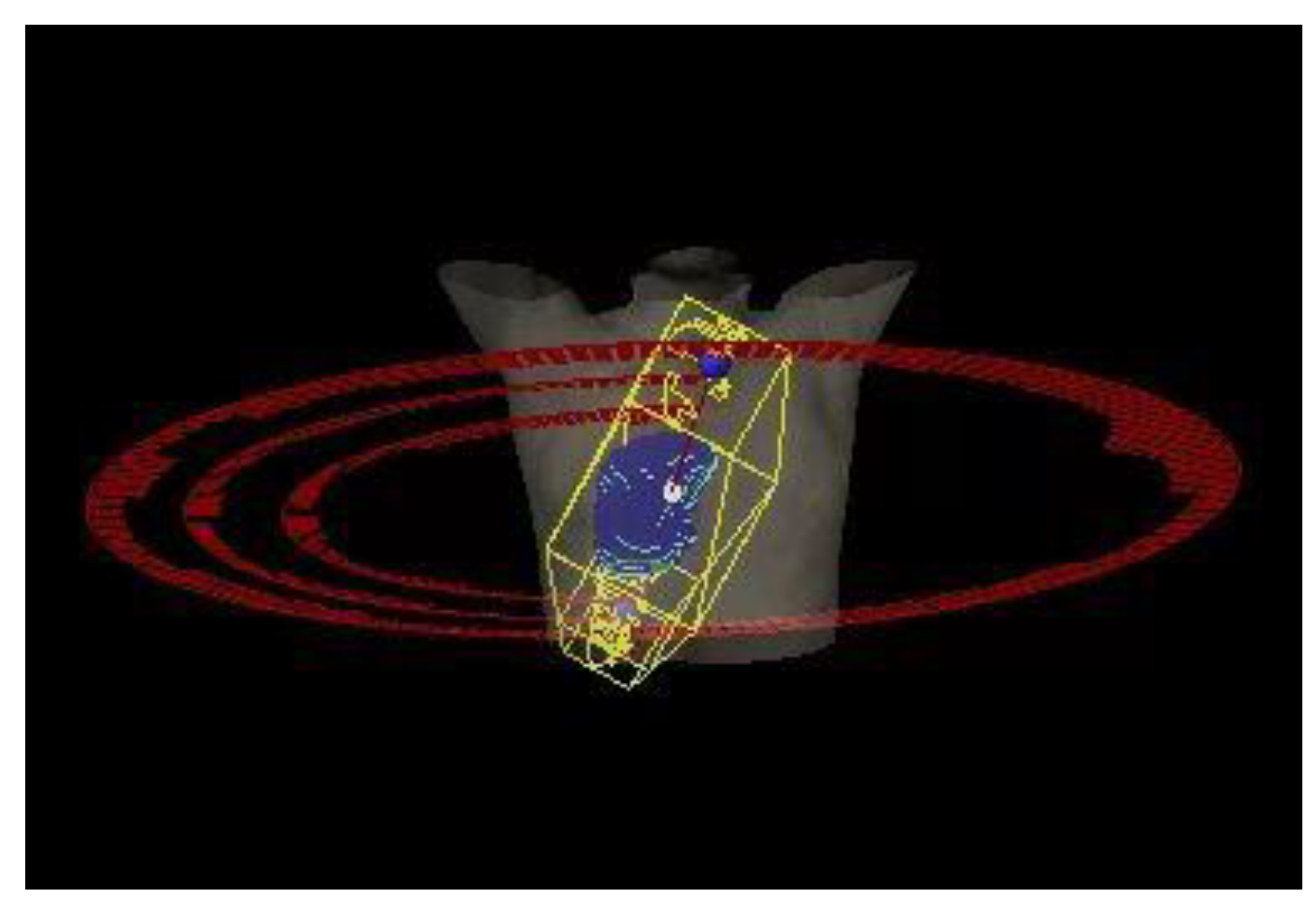
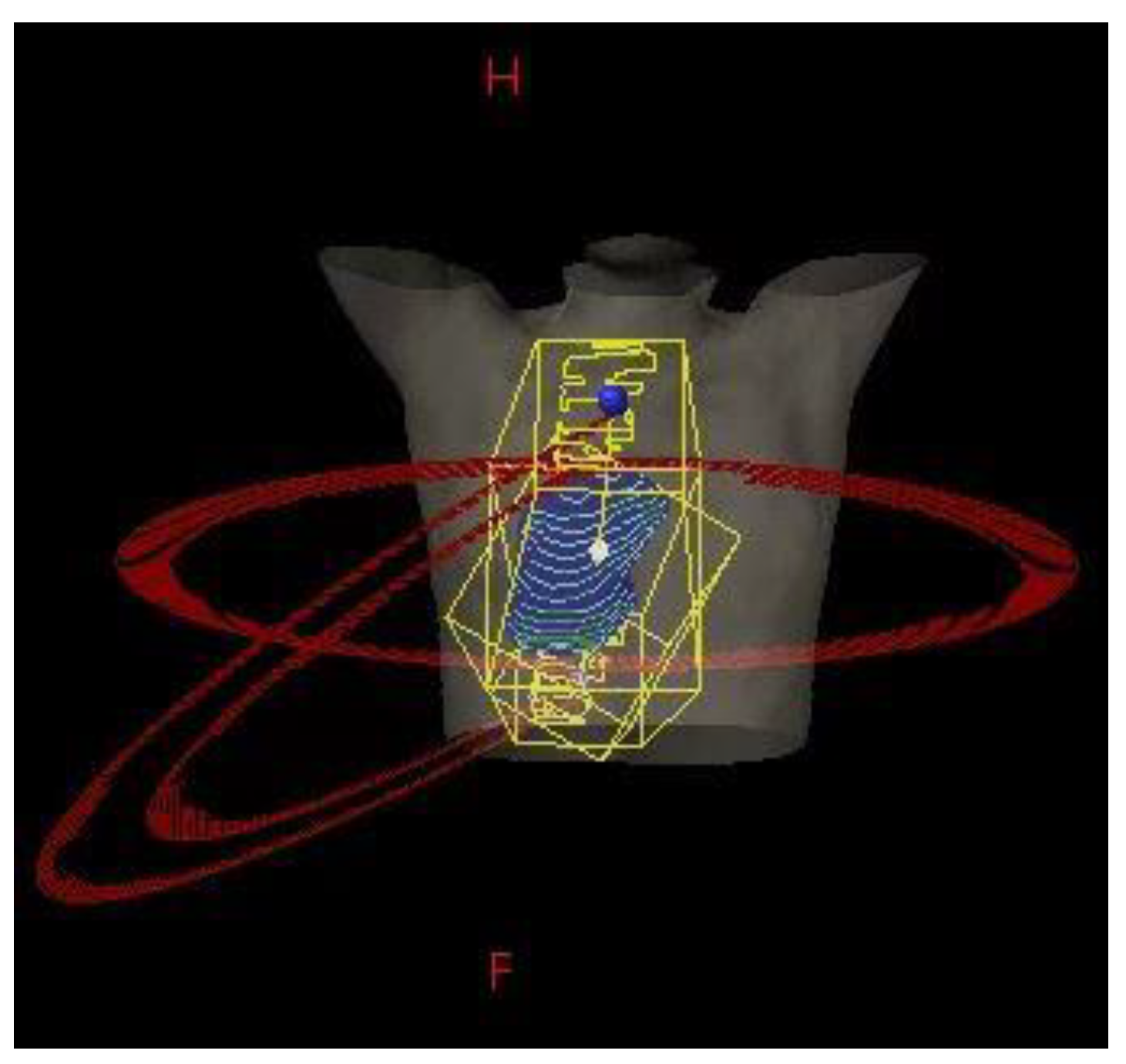
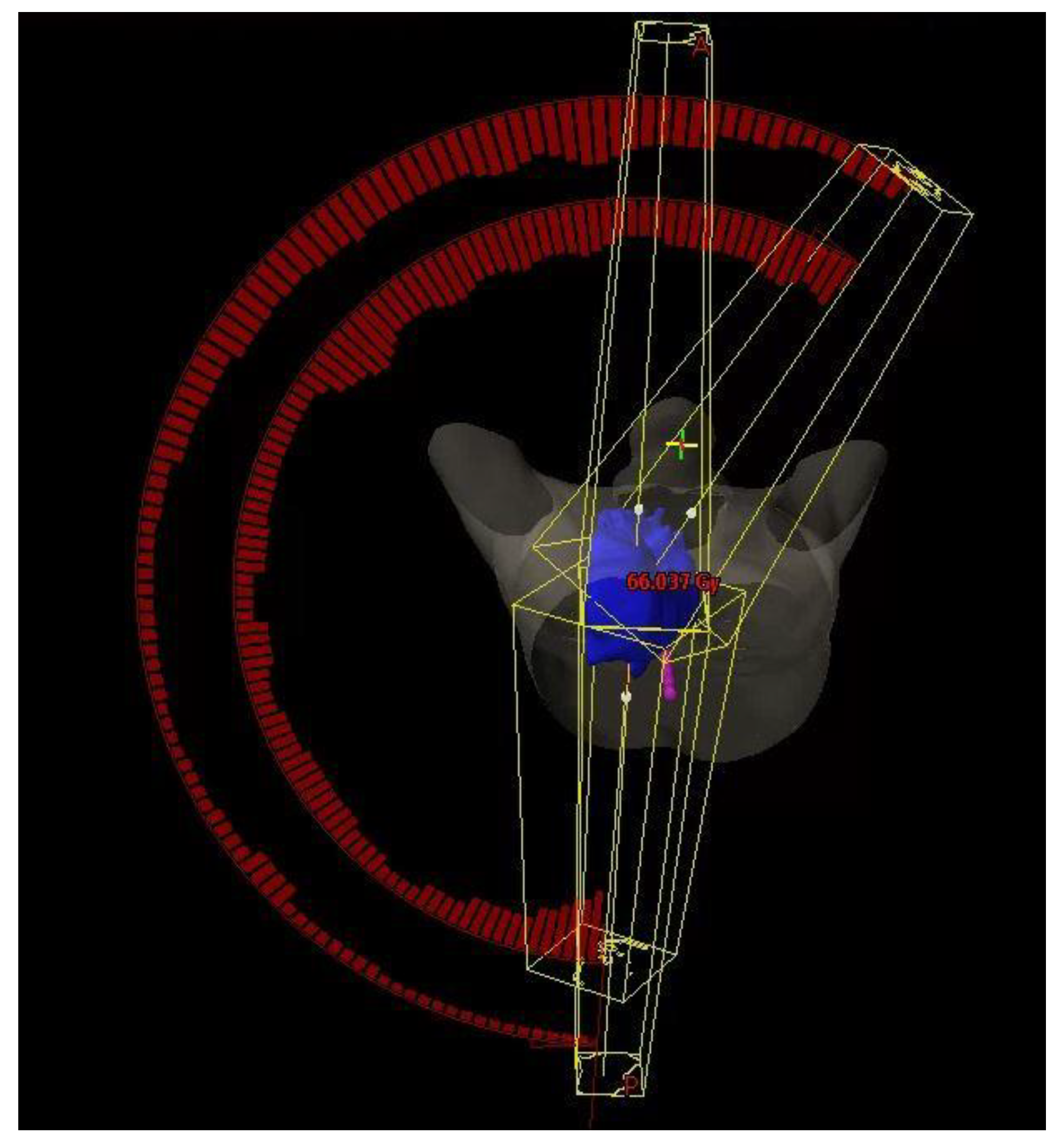
2.5. Beam and Couch Configuration
2.6. Dose Prescription
2.7. Plan Optimization
2.8. Inter-Planner Variability
2.9. Evaluation of Treatment Plans
- 100% of prescribed dose (60 Gy) should cover more than 98% of PTV
- Maximum dose of a 2% of PTV should be lower than 108% of the prescribed dose (64.8 Gy).
- Maximum point dose (i.e., hotspots outside the PTV) should be lower than 108% of the prescribed dose (64.8 Gy).
2.10. Statistical Analysis
3. Result
3.1. Patient Demographic
3.2. Dose-Volumetric of PTV
3.3. Dose-Volumetric Parameters of the Lungs
3.4. Dose-Volumetric Parameters of Centrally Located OARs
4. Discussion
4.1. Significance of the Study
4.2. Lungs Sparing
4.3. Heart Sparing
4.4. Oesophagus Sparing
4.5. Low Dose Irradiation to Normal Body Tissue
4.6. Duration of Treatment
4.7. Patient Safety
4.8. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Hong Kong Cancer Registry, Hospital Authority. Available online: https://www3.ha.org.hk/cancereg/topten.html (accessed on 3 August 2021).
- Ettinger, D.S.; Wood, D.E.; Akerley, W.; Bazhenova, L.A.; Borghaei, H.; Camidge, D.R.; Cheney, R.T.; Chirieac, L.R.; D’Amico, T.A.; Dilling, T.J.; et al. NCCN Guidelines Insights: Non-Small Cell Lung Cancer, Version 4.2016. J. Natl. Compr. Cancer Netw. 2016, 14, 255–264. [Google Scholar] [CrossRef] [Green Version]
- Bradley, J.D.; Hu, C.; Komaki, R.R.; Masters, G.A.; Blumenschein, G.R.; Schild, S.E.; Bogart, J.A.; Forster, K.M.; Magliocco, A.M.; Kavadi, V.S.; et al. Long-Term Results of NRG Oncology RTOG 0617: Standard- Versus High-Dose Chemoradiotherapy With or Without Cetuximab for Unresectable Stage III Non-Small-Cell Lung Cancer. J. Clin. Oncol. 2020, 38, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Jia, B.; Zheng, Q.; Qi, X.; Zhao, J.; Wu, M.; An, T.; Wang, Y.; Zhuo, M.; Li, J.; Zhao, X.; et al. Survival comparison of right and left side non-small cell lung cancer in stage I–IIIA patients: A Surveillance Epidemiology and End Results (SEER) analysis. Thorac. Cancer 2019, 10, 459–471. [Google Scholar] [CrossRef]
- Palma, D.A.; Senan, S.; Oberije, C.; Belderbos, J.; DE Dios, N.R.; Bradley, J.D.; Barriger, R.B.; Moreno-Jiménez, M.; Kim, T.H.; Ramella, S.; et al. Predicting Esophagitis After Chemoradiation Therapy for Non-Small Cell Lung Cancer: An Individual Patient Data Meta-Analysis. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 690–696. [Google Scholar] [CrossRef]
- Hernando, M.L.; Marks, L.B.; Bentel, G.C.; Zhou, S.-M.; Hollis, D.; Das, S.K.; Fan, M.; Munley, M.T.; Shafman, T.D.; Anscher, M.; et al. Radiation-induced pulmonary toxicity: A dose-volume histogram analysis in 201 patients with lung cancer. Int. J. Radiat. Oncol. Biol. Phys. 2001, 51, 650–659. [Google Scholar] [CrossRef]
- Aupérin, A.; Le Péchoux, C.; Rolland, E.; Curran, W.J.; Furuse, K.; Fournel, P.; Belderbos, J.; Clamon, G.; Ulutin, H.C.; Paulus, R.; et al. Meta-Analysis of Concomitant Versus Sequential Radiochemotherapy in Locally Advanced Non–Small-Cell Lung Cancer. JCO 2010, 28, 2181–2190. [Google Scholar] [CrossRef]
- Ahn, J.S.; Ahn, Y.C.; Kim, J.-H.; Lee, C.G.; Cho, E.K.; Lee, K.C.; Chen, M.; Kim, D.-W.; Kim, H.-K.; Min, Y.J.; et al. Multinational Randomized Phase III Trial with or Without Consolidation Chemotherapy Using Docetaxel and Cisplatin After Concurrent Chemoradiation in Inoperable Stage III Non–Small-Cell Lung Cancer: KCSG-LU05-04. JCO 2015, 33, 2660–2666. [Google Scholar] [CrossRef] [Green Version]
- Antonia, S.J.; Villegas, A.; Daniel, D.; Vicente, D.; Murakami, S.; Hui, R.; Yokoi, T.; Chiappori, A.; Lee, K.H.; De Wit, M.; et al. Durvalumab after Chemoradiotherapy in Stage III Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2017, 377, 1919–1929. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.-T.; An, H.J.; Kim, J.; Yoo, J.-R.; Kim, H.J.; Park, J.M. Non-coplanar VMAT plans for lung SABR to reduce dose to the heart: A planning study. BJR 2020, 93, 20190596. [Google Scholar] [CrossRef]
- Ma, M.; Ren, W.; Li, M.; Niu, C.; Dai, J. Dosimetric comparison of coplanar and noncoplanar beam arrangements for radiotherapy of patients with lung cancer: A meta-analysis. J. Appl. Clin. Med. Phys. 2021, 22, 34–43. [Google Scholar] [CrossRef]
- Govaert, S.L.; Troost, E.G.; Schuurbiers, O.C.; de Geus-Oei, L.-F.; Termeer, A.; Span, P.N.; Bussink, J. Treatment outcome and toxicity of intensity-modulated (chemo) radiotherapy in stage III non-small cell lung cancer patients. Radiat. Oncol. 2012, 7, 150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheung, E.Y.W.; Lee, K.H.Y.; Lau, W.T.L.; Lau, A.P.; Wat, P.Y. Non-coplanar VMAT plans for postoperative primary brain tumour to reduce dose to hippocampus, temporal lobe and cochlea: A planning study. BJR Open 2021, 3, 20210009. [Google Scholar] [CrossRef]
- Song, C.H.; Pyo, H.; Moon, S.H.; Kim, T.H.; Kim, D.W.; Cho, K.H. Treatment-Related Pneumonitis and Acute Esophagitis in Non–Small-Cell Lung Cancer Patients Treated with Chemotherapy and Helical Tomotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2010, 78, 651–658. [Google Scholar] [CrossRef] [PubMed]
- Steber, J.L.; Silva, S.; Harkenrider, M.M.; Surucu, M.; Choi, M. Clinical Application of a Hybrid Volumetric Arc Therapy Technique for Locally Advanced Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2015, 93, E595. [Google Scholar] [CrossRef]
- Bradley, J.D.; Paulus, R.; Komaki, R.; Masters, G.; Blumenschein, G.; Schild, S.; Bogart, J.; Hu, C.; Forster, K.; Magliocco, A.; et al. Standard-dose versus high-dose conformal radiotherapy with concurrent and consolidation carboplatin plus paclitaxel with or without cetuximab for patients with stage IIIA or IIIB non-small-cell lung cancer (RTOG 0617): A randomised, two-by-two factorial phase 3 study. Lancet Oncol. 2015, 16, 187–199. [Google Scholar] [CrossRef] [Green Version]
- Nelms, B.E.; Robinson, G.; Markham, J.; Velasco, K.; Boyd, S.; Narayan, S.; Wheeler, J.; Sobczak, M.L. Variation in external beam treatment plan quality: An inter-institutional study of planners and planning systems. Pract. Radiat. Oncol. 2012, 2, 296–305. [Google Scholar] [CrossRef]
- Kataria, T.; Sharma, K.; Subramani, V.; Karrthick, K.; Bisht, S. Homogeneity Index: An objective tool for assessment of conformal radiation treatments. J. Med. Phys. 2012, 37, 207. [Google Scholar] [CrossRef]
- Landberg, T.; Chavaudra, J.; Dobbs, J.; Gerard, J.-P.; Hanks, G.; Horiot, J.-C.; Johansson, K.-A.; Möller, T.; Purdy, J.; Suntharalingam, N.; et al. Report 62. J. Int. Comm. Radiat. Units Meas. 1999, os32, NP. [Google Scholar] [CrossRef]
- Greenland, S.; Senn, S.J.; Rothman, K.J.; Carlin, J.B.; Poole, C.; Goodman, S.N.; Altman, D.G. Statistical tests, P values, confidence intervals, and power: A guide to misinterpretations. Eur. J. Epidemiol. 2016, 31, 337–350. [Google Scholar] [CrossRef] [Green Version]
- Shi, A.; Zhu, G.; Wu, H.; Yu, R.; Li, F.; Xu, B. Analysis of clinical and dosimetric factors associated with severe acute radiation pneumonitis in patients with locally advanced non-small cell lung cancer treated with concurrent chemotherapy and intensity-modulated radiotherapy. Radiat. Oncol. 2010, 5, 35. [Google Scholar] [CrossRef] [Green Version]
- Shaikh, T.; Churilla, T.M.; Monpara, P.; Scott, W.J.; Cohen, S.J.; Meyer, J.E. Risk of radiation pneumonitis in patients receiving taxane-based trimodality therapy for locally advanced esophageal cancer. Pr. Radiat. Oncol. 2016, 6, 388–394. [Google Scholar] [CrossRef] [Green Version]
- Landman, Y.; Jacobi, O.; Kurman, N.; Yariv, O.; Peretz, I.; Rotem, O.; Dudnik, E.; Zer, A.; Allen, A.M. Durvalumab after concurrent chemotherapy and high-dose radiotherapy for locally advanced non-small cell lung cancer. OncoImmunology 2021, 10, 1959979. [Google Scholar] [CrossRef] [PubMed]
- Mayo, C.S.; Urie, M.M.; Fitzgerald, T.J.; Ding, L.; Lo, Y.C.; Bogdanov, M. Hybrid IMRT for Treatment of Cancers of the Lung and Esophagus. Int. J. Radiat. Oncol. Biol. Phys. 2008, 71, 1408–1418. [Google Scholar] [CrossRef] [PubMed]
- van Nimwegen, F.A.; Schaapveld, M.; Janus, C.P.M.; Krol, S.; Petersen, E.J.; Raemaekers, J.M.M.; Kok, W.E.M.; Aleman, B.M.P.; Van Leeuwen, F.E. Cardiovascular disease after Hodgkin lymphoma treatment: 40-year disease risk. JAMA Intern. Med. 2015, 175, 1007–1017. [Google Scholar] [CrossRef] [PubMed]
- van Nimwegen, F.A.; Schaapveld, M.; Cutter, D.J.; Janus, C.P.; Krol, A.D.; Hauptmann, M.; Kooijman, K.; Roesink, J.; van der Maazen, R.; Darby, S.C.; et al. Radiation Dose-Response Relationship for Risk of Coronary Heart Disease in Survivors of Hodgkin Lymphoma. J. Clin. Oncol. 2016, 34, 235–243. [Google Scholar] [CrossRef] [Green Version]
- Hooning, M.J.; Botma, A.; Aleman, B.M.P.; Baaijens, M.H.A.; Bartelink, H.; Klijn, J.G.M.; Taylor, C.W.; Van Leeuwen, F.E. Long-term risk of cardiovascular disease in 10-year survivors of breast cancer. J. Natl. Cancer Inst. 2007, 99, 365–375. [Google Scholar] [CrossRef] [Green Version]
- Darby, S.C.; McGale, P.; Taylor, C.W.; Peto, R. Long-term mortality from heart disease and lung cancer after radiotherapy for early breast cancer: Prospective cohort study of about 300,000 women in US SEER cancer registries. Lancet Oncol. 2005, 6, 557–565. [Google Scholar] [CrossRef]
- Wang, K.; Eblan, M.J.; Deal, A.M.; Lipner, M.; Zagar, T.M.; Wang, Y.; Mavroidis, P.; Lee, C.B.; Jensen, B.C.; Rosenman, J.G.; et al. Cardiac Toxicity After Radiotherapy for Stage III Non–Small-Cell Lung Cancer: Pooled Analysis of Dose-Escalation Trials Delivering 70 to 90 Gy. JCO 2017, 35, 1387–1394. [Google Scholar] [CrossRef]
- Allan, E.; Williams, T.M.; Grecula, J.C.; Haglund, K.E.; Welliver, M.X.; Bazan, J.G. Mortality, Cardiac Toxicity, and Radiation Dose to the Heart in Patients Treated with Curative Intent Fractionated Radiation Therapy for Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2015, 93, S161. [Google Scholar] [CrossRef]
- Bourbonne, V.; Delafoy, A.; Lucia, F.; Quéré, G.; Pradier, O.; Schick, U. Toxicity after volumetric modulated arc therapy for lung cancer: A monocentric retrospective study. Transl. Lung Cancer Res. 2021, 10, 156–166. [Google Scholar] [CrossRef] [PubMed]
- Mavrogenis, A.F.; Pala, E.; Guerra, G.; Ruggieri, P. Post-radiation sarcomas. Clinical outcome of 52 Patients. J. Surg Oncol. 2012, 105, 570–576. [Google Scholar] [CrossRef]
- Smyth, G.; Evans, P.M.; Bamber, J.C.; Bedford, J.L. Recent developments in non-coplanar radiotherapy. BJR 2019, 92, 20180908. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.F.; Wang, M.S.; Lai, Y.H.; Chen, H.H.W. Comparison of Dosimetry and Efficiency of Jaw Tracking and Static Jaw Techniques Using Volumetric Modulated Arc Therapy and Intensity-Modulated Radiation Therapy in Non-Small Cell Lung Cancer. Int. J. Radiat. Oncol. Biol. Phys. 2018, 102, e496. [Google Scholar] [CrossRef] [Green Version]
- Pokhrel, D.; Sanford, L.; Halfman, M.; Molloy, J. Potential reduction of lung dose via VMAT with jaw tracking in the treatment of single-isocenter/two-lesion lung SBRT. J. Appl. Clin. Med. Phys. 2019, 20, 55–63. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, O.S.H.; Lee, M.C.H.; Hung, A.W.M.; Chang, A.T.Y.; Yeung, R.M.W.; Lee, A.W.M. The superiority of hybrid-volumetric arc therapy (VMAT) technique over double arcs VMAT and 3D-conformal technique in the treatment of locally advanced non-small cell lung cancer—A planning study. Radiother. Oncol. 2011, 101, 298–302. [Google Scholar] [CrossRef]
- Kataria, T.; Gupta, D.; Bisht, S.S.; Karthikeyan, N.; Goyal, S.; Pushpan, L.; Abhishek, A.; Govardhan, H.; Kumar, V.; Sharma, K.; et al. Adaptive radiotherapy in lung cancer: Dosimetric benefits and clinical outcome. BJR 2014, 87, 20130643. [Google Scholar] [CrossRef] [Green Version]
- Woodford, C.; Yartsev, S.; Dar, A.R.; Bauman, G.; van Dyk, J. Adaptive Radiotherapy Planning on Decreasing Gross Tumor Volumes as Seen on Megavoltage Computed Tomography Images. Int. J. Radiat. Oncol. Biol. Phys. 2007, 69, 1316–1322. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Critical Organ/Organ-at Risk | Dose Constraint |
|---|---|
| Spinal Cord | Maximum dose < 45 Gy |
| Non-PTV Lung | Mean dose < 20 Gy V20 < 35% V5 < 65% |
| Oesophagus | Maximum dose < 63 Gy (105% of prescribed dose) Mean dose < 34 Gy |
| Heart | Mean dose < 35 Gy V40 < 80% V45 < 60% V60 < 30% |
| Structure | Dose Constraint | Weight |
|---|---|---|
| PTV | Maximum dose < 60 Gy Minimum dose > 57 Gy | 100 100 |
| Spinal Cord | Maximum dose < 45 Gy | 100 |
| Non-PTV lung | Mean dose < 20 Gy V20 < 35% | 50 |
| Heart | Mean dose < 35 Gy | 50 |
| Oesophagus | Maximum dose <63 Gy | 20 |
| PTV DV Parameters | SP-VMAT | DP-VMAT | H-VMAT | (DP-VMAT Minus SP-VMAT) | (H-VMAT Minus SP-VMAT) | ||
|---|---|---|---|---|---|---|---|
| Mean ± S.D. | Mean ± S.D. | Mean ± S.D. | Diff | p | Diff | p | |
| Maximum Dose (Gy) | 64.59 ± 0.67 | 64.68 ± 0.81 | 65.54 ± 0.57 | 0.09 | 0.472 | 0.95 | 0.23 |
| Mean Dose (Gy) | 61.49 ± 0.17 | 61.45 ± 0.26 | 61.71 ± 0.26 | −0.04 | 0.446 | 0.23 | 0.22 |
| Minimum Dose (Gy) | 55.25 ± 1.14 | 57.15 ± 1.09 | 54.26 ± 2.08 | 1.92 | 0.43 | 9.01 | 0.60 |
| D98% (Gy) | 60.42 ± 0.34 | 60.37 ± 0.34 | 60.54 ± 0.26 | −0.05 | 0.248 | 0.12 | 0.33 |
| D95% (Gy) | 60.75 ± 0.21 | 60.69 ± 0.24 | 60.77 ± 0.27 | −0.06 | 0.267 | 0.02 | 0.95 |
| D50% (Gy) | 61.51 ± 0.17 | 61.46 ± 0.28 | 61.66 ± 0.32 | −0.05 | 0.36 | 0.16 | 0.12 |
| D2% (Gy) | 62.49 ± 0.244 | 62.48 ± 0.36 | 63.25 ± 0.35 | −0.01 | 0.744 | 0.75 | 0.26 |
| Homogeneity Index | 0.0338 ± 0.006 | 0.0354 ± 0.01 | 0.0447 ± 0.01 | 0.0016 | 0.215 | 0.01 | 0.1 |
| Conformity Index | 1.1889 ± 0.09 | 1.1894 ± 0.07 | 1.2165 ± 0.089 | 0.0006 | 0.943 | 0.03 | 0.132 |
| DV Parameters | SP-VMAT | DP-VMAT | H-VMAT | DP-VMAT Minus SP-VMAT | H-VMAT Minus SP-VMAT | |||
|---|---|---|---|---|---|---|---|---|
| Mean ± S.D. | Mean ± S.D. | Mean ± S.D. | Diff | p | Diff | p | ||
| Non-PTV lung | Mean Dose (Gy) | 15.24 ± 3.18 | 15.53 ± 2.76 | 13.19 ± 2.47 | 0.28 | 0.112 | −2.05 * | <0.0001 |
| V20 Gy (%) | 28.3 ± 6.98 | 28.52 ± 6.97 | 21.83 ± 4.26 | 0.22 | 0.647 | −6.47 * | <0.0001 | |
| V10 Gy (%) | 51.73 ± 12.05 | 51.46 ± 9.93 | 35.84 ± 6.08 | −0.26 | 0.695 | −15.89 * | <0.0001 | |
| V5 Gy (%) | 57.95 ± 14.65 | 61.41 ± 11.83 | 49.29 ± 9.51 | 3.45 * | 0.006 | −11.66 * | <0.0001 | |
| D1500 (Gy) | 10.44 ± 4.26 | 10.54 ± 3.92 | 6.29 ± 2.34 | 0.097 | 0.948 | −4.17 * | <0.0001 | |
| D1000 (Gy) | 16.67 ± 5.34 | 17.12 ± 4.89 | 11.19 ± 3.88 | 0.458 | 0.349 | −5.47 * | <0.0001 | |
| Both Lungs | Mean Dose (Gy) | 17.31 ± 3.59 | 17.58 ± 3.16 | 15.31 ± 2.98 | 0.27 * | 0.002 | −2.00 | <0.0001 |
| V20 Gy (%) | 31.51 ± 7.36 | 31.73 ± 7.37 | 25.23 ± 5.01 | 0.22 | 0.231 | −6.27 * | <0.0001 | |
| V10 Gy (%) | 53.87 ± 12.03 | 53.64 ± 9.88 | 38.64 ± 6.65 | −0.22 * | 0.001 | −15.23 * | <0.0001 | |
| V5 Gy (%) | 59.34 ± 14.39 | 62.69 ± 11.54 | 48.16 ± 9.81 | 3.34 * | <0.0001 | −11.19 * | <0.0001 | |
| D1500 (Gy) | 12.17 ± 5.04 | 12.18 ± 4.78 | 7.37 ± 3.08 | 0.02 * | 0.002 | −4.80 * | <0.0001 | |
| D1000 (Gy) | 19.68 ± 7.27 | 20.39 ± 7.04 | 14.52 ± 7.12 | 0.71 * | 0.012 | −5.16 * | <0.0001 | |
| Ipsilateral Lung | Mean Dose (Gy) | 24.46 ± 5.55 | 25.64 ± 5.03 | 23.88 ± 5.12 | 1.18 * | 0.002 | −0.58 | 0.058 |
| V20 Gy (%) | 52.0 ± 12.75 | 53.58 ± 11.85 | 45.72 ± 9.53 | 1.58 | 0.231 | −6.82 * | <0.0001 | |
| V10 Gy (%) | 63.48 ± 14.88 | 69.81 ± 11.74 | 59.30 ± 12.11 | 6.32 * | 0.001 | −4.18 * | 0.002 | |
| V5 Gy (%) | 61.99 ± 16.18 | 69.74 ± 11.80 | 59.37 ± 16.77 | 7.75 * | <0.0001 | −2.62 * | 0.004 | |
| D1500 (Gy) | 2.05 ± 2.61 | 3.06 ± 4.10 | 1.69 ± 2.09 | 1.01 * | 0.002 | −0.36 * | 0.003 | |
| D1000 (Gy) | 13.23 ± 10.03 | 15.85 ± 9.07 | 10.26 ± 8.10 | 2.61 * | 0.012 | −2.97 * | 0.002 | |
| Contralateral Lung | Mean Dose (Gy) | 9.41 ± 2.56 | 8.71 ± 1.72 | 5.82 ± 1.75 | −0.7 * | 0.002 | −3.59 * | <0.0001 |
| V20 Gy (%) | 8.71 ± 7.54 | 7.42 ± 5.18 | 2.62 ± 3.13 | −1.29 | 0.231 | −6.09 * | <0.0001 | |
| V10 Gy (%) | 42.63 ± 16.45 | 35.36 ± 11.69 | 15.37 ± 9.97 | −7.27 * | 0.001 | −27.27 * | <0.0001 | |
| V5 Gy (%) | 66.04 ± 14.36 | 64.65 ± 12.59 | 43.89 ± 14.38 | −1.39 | <0.0001 | −22.14 * | <0.0001 | |
| D1500 (Gy) | 0.78 ± 1.15 | 0.688 ± 1.01 | 0.54 ± 0.75 | −0.1 * | 0.002 | −0.24 * | 0.017 | |
| D1000 (Gy) | 5.08 ± 3.84 | 4.33 ± 2.60 | 5.86 ± 13.32 | −0.75 * | 0.012 | 0.77 * | 0.006 | |
| DV Parameters | SP-VMAT | DP-VMAT | H-VMAT | DP-VMAT Minus SP-VMAT | H-VMAT Minus SP-VMAT | |||
|---|---|---|---|---|---|---|---|---|
| Mean ± S.D. | Mean ± S.D. | Mean ± S.D. | Diff | p | Diff | p | ||
| Oesophagus | Max Dose (Gy) | 59.94 ± 9.15 | 60.16 ± 8.42 | 59.87 ± 11.42 | 0.22 | 0.679 | −0.08 | 0.744 |
| Mean Dose (Gy) | 24.33 ± 6.71 | 24.54 ± 6.02 | 22.60 ± 7.44 | 0.20 | 0.472 | −1.73 * | 0.02 | |
| V30 Gy (%) | 39.54 ± 13.49 | 37.93 ± 13.67 | 33.99 ± 14.17 | −1.61 | 0.193 | −5.54 * | 0.003 | |
| V18.8 Gy (%) | 49.57 ± 13.53 | 49.03 ± 10.62 | 42.44 ± 14.80 | −0.54 | 0.647 | −7.13 * | 0.002 | |
| Spinal Cord | Max Dose (Gy) | 35.87 ± 7.26 | 35.3 ± 7.65 | 41.19 ± 3.83 | −0.14 | 0.679 | 5.32 * | 0.002 |
| D0.1cc (Gy) | 33.42 ± 7.53 | 33.4 ± 7.52 | 39.29 ± 3.93 | −0.06 | 0.811 | 5.83 * | 0.02 | |
| Heart | Max Dose (Gy) | 57.85 ± 16.58 | 58.87 ± 14.37 | 62.51 ± 7.56 | 1.02 | 0.102 | 4.67 * | 0.002 |
| Mean Dose (Gy) | 13.66 ± 8.66 | 12.20 ± 8.33 | 13.74 ± 8.68 | −1.45 * | <0.001 | 0.08 | 0.879 | |
| V60 Gy (%) | 2.15 ± 2.31 | 2.2 ± 2.39 | 2.56 ± 2.15 | 0.05 | 0.217 | 0.41 | 0.079 | |
| V45 Gy (%) | 5.472 ± 5.21 | 5.472 ± 5.1 | 9.61 ± 8.23 | 0.00 | 0.99 | 4.14 * | 0.003 | |
| V40 Gy (%) | 7.22 ± 6.56 | 7.03 ± 6.61 | 12.88 ± 11.21 | −0.19 | 0.28 | 5.86 * | 0.001 | |
| V20 Gy (%) | 26.37 ± 20.63 | 21.57 ± 19.03 | 23.03 ± 18.06 | −4.8 * | 0.001 | −3.34 * | 0.02 | |
| V10 Gy (%) | 47.25 ± 33.39 | 40.14 ± 30.59 | 39.3 ± 25.82 | −7.11 * | <0.001 | −7.94 * | 0.007 | |
| D0.1cc (Gy) | 56.94 ± 16.80 | 57.8 ± 14.91 | 61.48 ± 8.65 | 0.86 | 0.094 | 3.68 * | 0.001 | |
| D2% (Gy) | 48.8 ± 18.17 | 48.55 ± 18.66 | 53.86 ± 14.29 | −0.25 | 0.811 | 5.31 * | 0.002 | |
| Body | Mean Dose (Gy) | 8.34 ± 2.40 | 8.41 ± 2.23 | 7.64 ± 2.11 | 0.07 | 0.327 | −0.70 * | <0.001 |
| V10% (%) | 32.80 ± 8.36 | 33.64 ± 7.36 | 25.46 ± 6.43 | 0.84 * | 0.037 | −7.34 * | <0.001 | |
| V30% (%) | 16.15 ± 5.13 | 15.30 ± 4.97 | 13.37 ± 3.97 | −0.86 * | 0.001 | −2.78 * | <0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheung, E.Y.W.; Kwong, V.H.Y.; Chan, F.Y.C.; Cheng, D.Y.T.; Cheng, J.K.Y.; Yung, S.H.Y.; Chan, K.T.K.; Cheung, K.T.Y.; Cheung, T.S.W.; Yiu, J.C.L. Modified VMAT Plans for Locally Advanced Centrally Located Non-Small Cell Lung Cancer (NSCLC). Life 2021, 11, 1085. https://doi.org/10.3390/life11101085
Cheung EYW, Kwong VHY, Chan FYC, Cheng DYT, Cheng JKY, Yung SHY, Chan KTK, Cheung KTY, Cheung TSW, Yiu JCL. Modified VMAT Plans for Locally Advanced Centrally Located Non-Small Cell Lung Cancer (NSCLC). Life. 2021; 11(10):1085. https://doi.org/10.3390/life11101085
Chicago/Turabian StyleCheung, Eva Y. W., Virginia H. Y. Kwong, Fandy Y. C. Chan, Dominic Y. T. Cheng, Janice K. Y. Cheng, Sapphire H. Y. Yung, Kiris T. K. Chan, Kelly T. Y. Cheung, Tracy S. W. Cheung, and Janna C. L. Yiu. 2021. "Modified VMAT Plans for Locally Advanced Centrally Located Non-Small Cell Lung Cancer (NSCLC)" Life 11, no. 10: 1085. https://doi.org/10.3390/life11101085