The Medium Is the Message: How Do Canadian University Students Want Digital Medication Information?

 ,
,
Abstract
:1. Introduction
“The medium is the message.”~Marshall McLuhan
1.1. Background
1.2. International Approaches to Digital Medication Information
1.3. Research Questions
- What format do young adults want as a DMI format (i.e., online, mobile app, or email)?
- Why do they have that DMI format preference?
2. Materials and Methods
2.1. Participants and Recruitment
2.2. Setting and Context
2.3. Procedure
- If you were to receive digital medication information, how would you like to receive it? For example, online (website), email, or a mobile app?
- Why?
2.4. Analysis
3. Results
3.1. Demographic Data
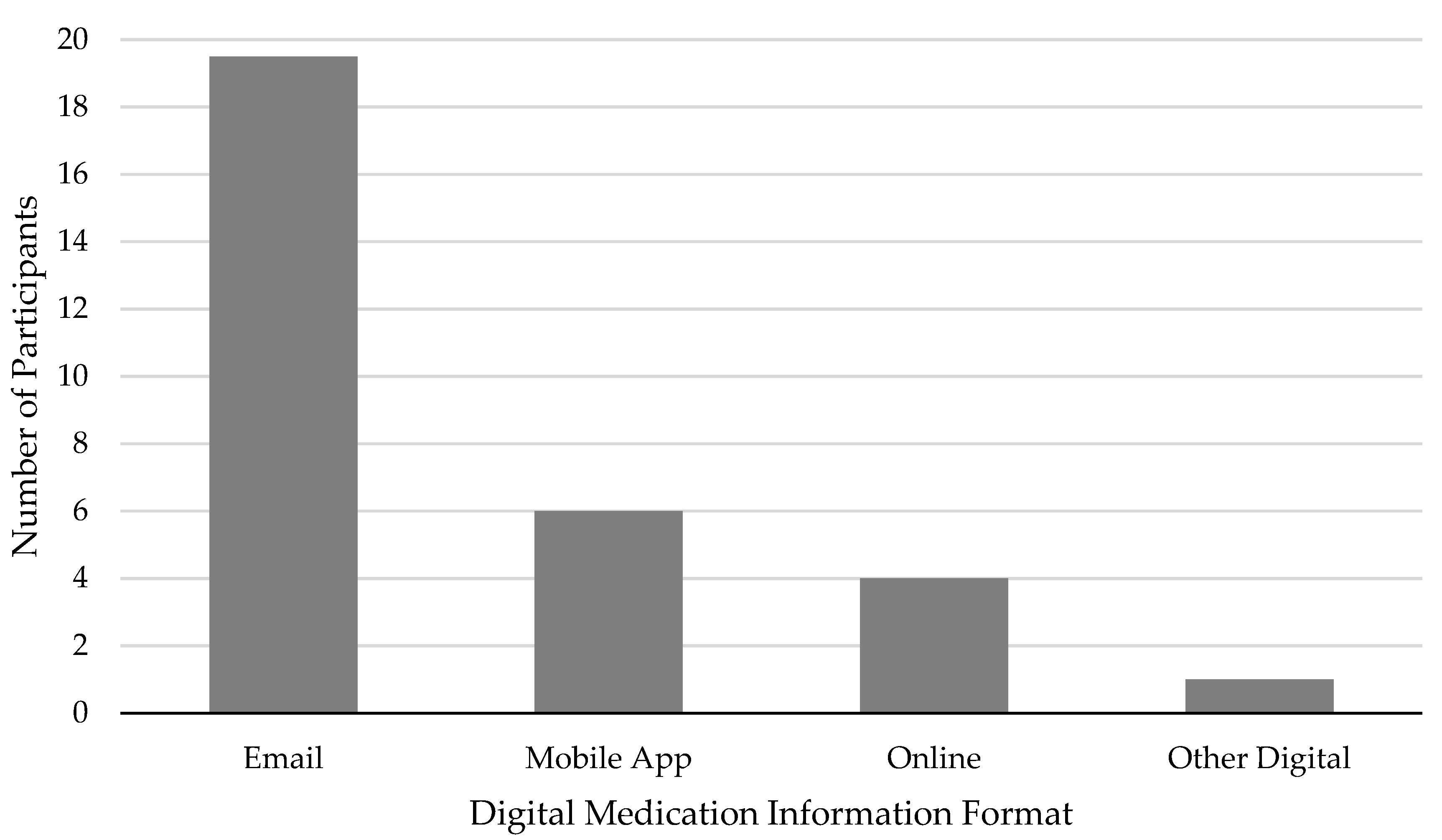
3.2. DMI Data: Which DMI Format Did Participants Prefer?
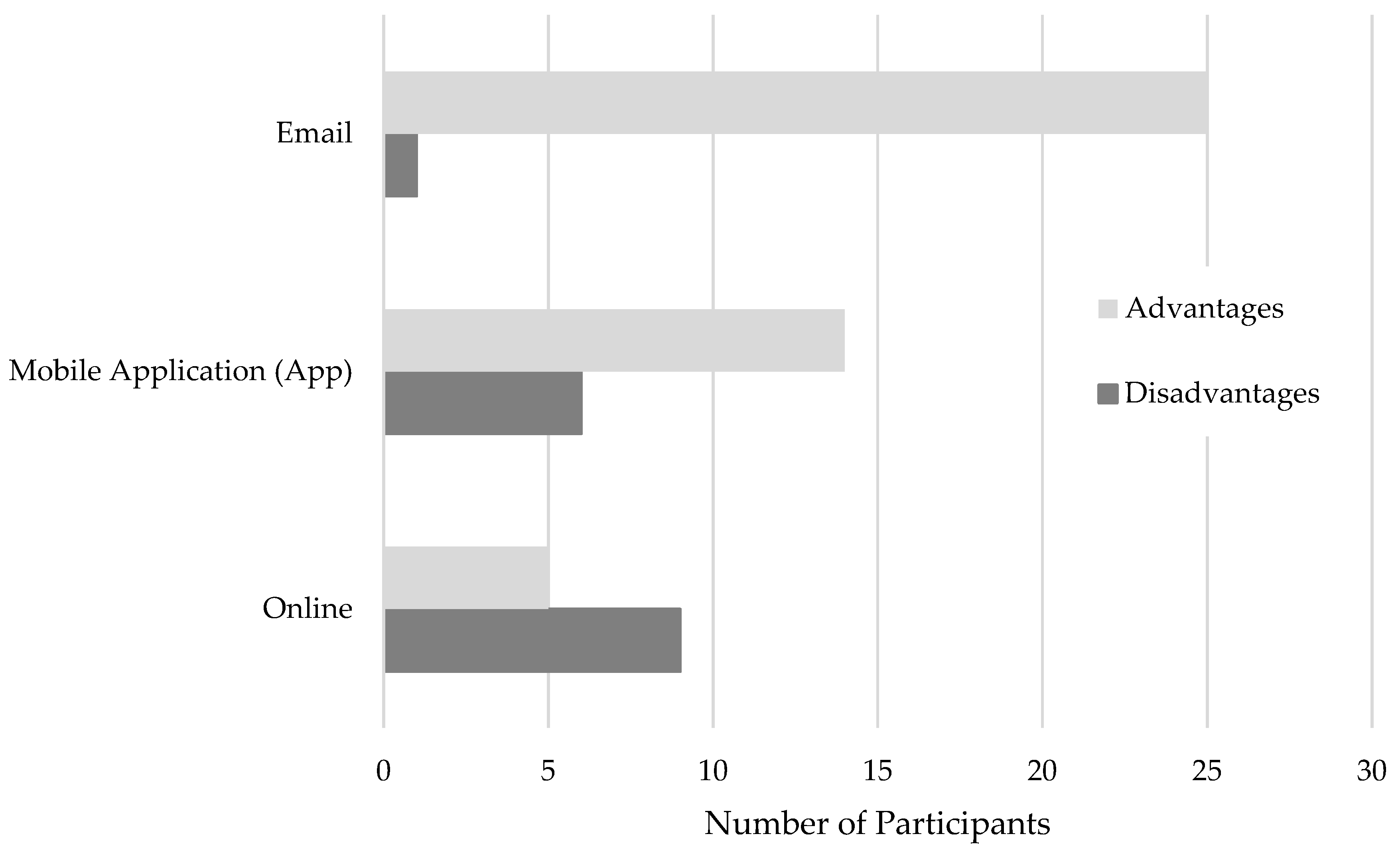
3.3. DMI Data: Why Do Participants Believe Email is Most Suitable DMI Format?
- Availability: Can be used at multiple locations;
- Ease of Access: Does not require and account or login and password;
- Findability: Easy to locate;
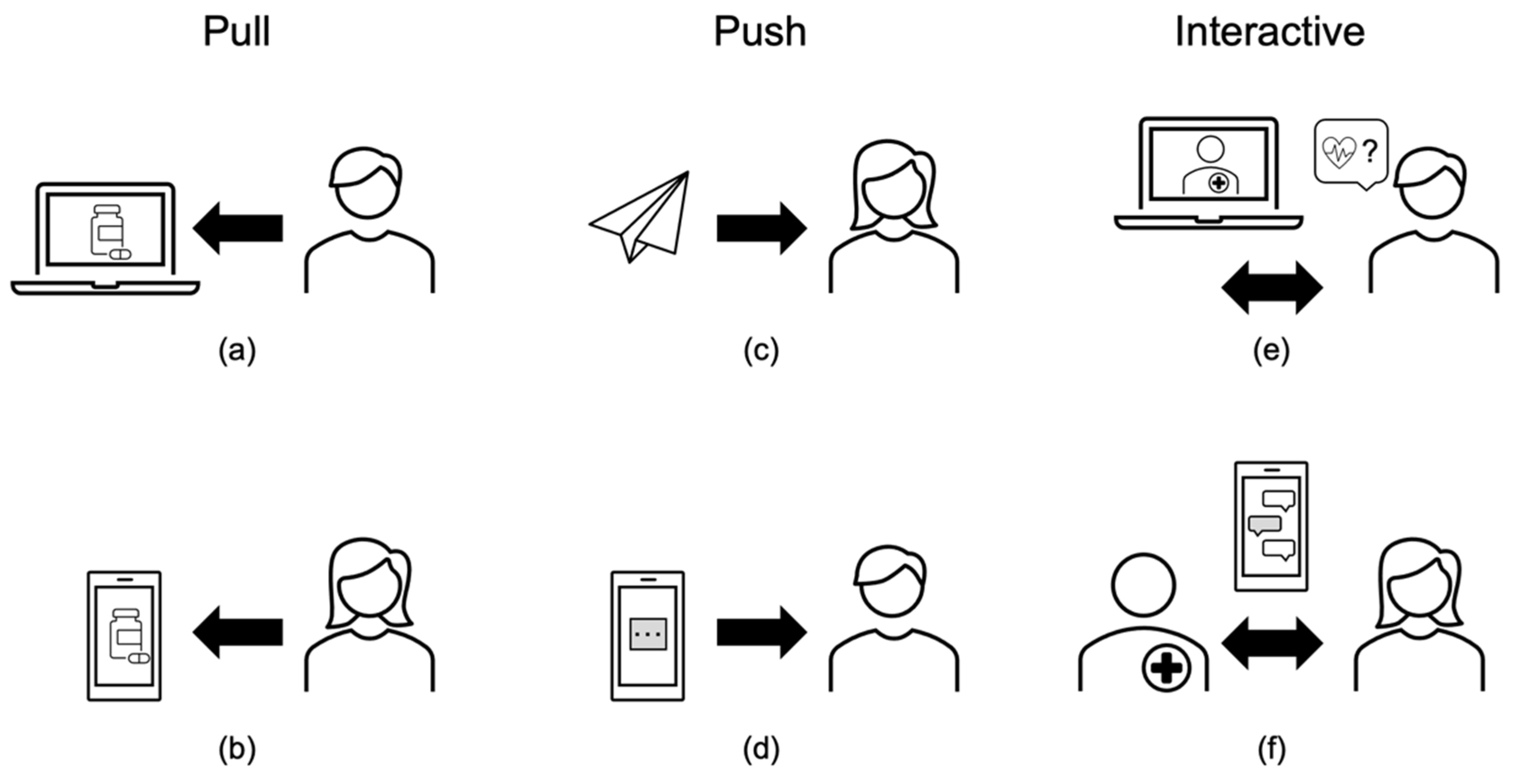
- Communication Method: Sent to users, sought out by users, or allows people to interact in real time;
- Storage: Easy to keep, requires limited storage space;
- Security: Ensuring one’s prescribed medications are kept secure and confidential;
- Flexibility: Offers different ways of sharing, storing, or using the information;
- Personalization: Tailored to an individual’s situation;
- Searchability: Can search the document for specific information;
- Frequency of Use: How often people would need to refer to the information;
- Trustworthiness: Comes from a reputable source;
- Comprehensiveness: Contains all prescription medication related information in one place;
- Layered Content: Provides different levels of detail;
- Helpful in an Emergency: Provides access to prescribed medications to first responders;
- Medication Reminders: Provides notifications to support medication adherence.
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Beynon-Davies, P. Communication: The medium is not the message. In Significance: Exploring the Nature of Information, Systems and Technology; Beynon-Davies, P., Ed.; Palgrave Macmillan: London, UK, 2011; pp. 58–76. ISBN 978-0-230-29502-5. [Google Scholar]
- Sarnak, D.O.; Squires, D.; Bishop, S. Prescription Drug Spending Why Is the U.S. an Outlier? Available online: https://www.commonwealthfund.org/publications/issue-briefs/2017/oct/paying-prescription-drugs-around-world-why-us-outlier (accessed on 12 September 2020).
- Yuan, H.-C.T.; Raynor, D.K.; Aslani, P. Comparison of International Regulations for Written Medicine Information (WMI) on Prescription Medicines. Ther. Innov. Regul. Sci. 2019, 53, 215–226. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. Frequently Asked Questions: Product Monographs Posted to the Health Canada Website. Available online: https://www.canada.ca/en/health-canada/services/drugs-health-products/drug-products/applications-submissions/guidance-documents/product-monograph/frequently-asked-questions-product-monographs-posted-health-canada-website.html (accessed on 17 September 2020).
- Monkman, H.; Kushniruk, A.W. Consumer Medication Information: Similarities and Differences between Three Canadian Pharmacies. Stud. Health Technol. Inform. 2017, 234, 238–242. [Google Scholar] [PubMed]
- Monkman, H.; Kushniruk, A.W. All Consumer Medication Information Is Not Created Equal: Implications for Medication Safety. Stud. Health Technol. Inform. 2017, 234, 233–237. [Google Scholar] [PubMed]
- Pearsall, B.M.; Araojo, R.; Hinton, D. Essential Medication Information for Patients: Ensuring Access. Ther. Innov. Regul. Sci. 2014, 48, 162–164. [Google Scholar] [CrossRef] [PubMed]
- Kish-Doto, J.; Scales, M.; Eguino-Medina, P.; Fitzgerald, T.; Tzeng, J.P.; McCormack, L.A.; O’Donoghue, A.; Oguntimein, O.; West, S.L. Preferences for Patient Medication Information: What Do Patients Want? J. Health Commun. 2014, 19, 77–88. [Google Scholar] [CrossRef] [PubMed]
- Boudewyns, V.; O’Donoghue, A.C.; Kelly, B.; West, S.L.; Oguntimein, O.; Bann, C.M.; McCormack, L.A. Influence of patient medication information format on comprehension and application of medication information: A randomized, controlled experiment. Patient Educ. Couns. 2015, 98, 1592–1599. [Google Scholar] [CrossRef] [PubMed]
- Monkman, H.; Schmidt, T.; Nøhr, C. Online Medication Information for Citizens: A Comparison of Demands on eHealth Literacy. Stud. Health Technol. Inform. 2020, 270, 1026–1030. [Google Scholar] [CrossRef] [PubMed]
- London Drugs—Apps on Google Play. Available online: https://play.google.com/store/apps/details?id=com.mobify.builds.ldextras&hl=en_CA&gl=US (accessed on 2 December 2020).
- U.S. Food & Drug Administration. Useful Written Consumer Medication Information (CMI). Available online: https://www.fda.gov/regulatory-information/search-fda-guidance-documents/useful-written-consumer-medication-information-cmi (accessed on 1 December 2020).
- U.S. Food & Drug Administration. Drug Information for Consumers. Available online: https://www.fda.gov/drugs/resources-you-drugs/drug-information-consumers (accessed on 1 December 2020).
- Sage, A.; Blalock, S.J.; Carpenter, D. Extending FDA guidance to include consumer medication information (CMI) delivery on mobile devices. Res. Soc. Adm. Pharm. 2017, 13, 209–213. [Google Scholar] [CrossRef] [PubMed]
- Hammar, T.; Nilsson, A.-L.; Hovstadius, B. Patients’ views on electronic patient information leaflets. Pharm. Pract. 2016, 14, 702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Consumer Medicine Information (CMI). Explained. Available online: https://www.nps.org.au/consumers/consumer-medicine-information-cmi (accessed on 1 December 2020).
- MedicineWise: Manage Medicine. Available online: https://apps.apple.com/au/app/medicinewise-manage-medicine/id777483494 (accessed on 2 December 2020).
- Eurostat: Statistics Explained File: Demographic Balance, 2019 (Thousands).png—Statistics Explained. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=File:Demographic_balance,_2019_(thousands).png (accessed on 9 October 2020).
- About Medicin.dk—Medicin.dk. Available online: https://www.indlaegssedler.dk/OmMedicinDk/OmMedicinDK/1 (accessed on 13 October 2020).
- Indlægssedler.dk—Information about Medicine. Available online: https://www.indlaegssedler.dk/ (accessed on 18 September 2020).
- Marstrand Reersted, T. SV: Besøgsdata på Min. Medicin 2020.
- Monkman, H.; Nøhr, C.; Kushniruk, A.W. A Comparison of Danish and Canadian Consumer Medication Information. Stud. Health Technol. Inform. 2017, 241, 147–152. [Google Scholar] [PubMed]
- Monkman, H.; Kushniruk, A.W.; Barnett, J.; Borycki, E.M.; Sheets, D. We Built It, But They Are Not Coming: Exploring Deterrents to Consumer Medication Information Use. Stud. Health Technol. Inform. 2019, 265, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Monkman, H. Consumer Medication Information: Memory, Perceptions, Preferences, and Information Needs. Available online: http://dspace.library.uvic.ca/bitstream/handle/1828/10431/Monkman_Helen_PhD_2018.pdf?sequence=1&isAllowed=y (accessed on 4 October 2020).
- Monkman, H.; Kushniruk, A.W.; Borycki, E.M.; Sheets, D.J.; Barnett, J. Differences in Memory, Perceptions, and Preferences of Multimedia Consumer Medication Information: Experimental Performance and Self-Report Study. JMIR Hum. Factors 2020, 7, e15913. [Google Scholar] [CrossRef] [PubMed]
- Weiss, B.D. Quick Assessment of Literacy in Primary Care: The Newest Vital Sign. Ann. Fam. Med. 2005, 3, 514–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norman, C.D.; Skinner, H.A. eHEALS: The eHealth Literacy Scale. J. Med. Internet Res. 2006, 8, e27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsieh, H.-F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Monkman, H.; Kushniruk, A.W.; Barnett, J.; Borycki, E.M.; Greiner, L.E.; Sheets, D. Are Health Literacy and eHealth Literacy the Same or Different? Stud. Health Technol. Inform. 2017, 245, 178–182. [Google Scholar] [PubMed]
- Monkman, H.; Kushniruk, A.W.; Borycki, E.M.; Sheets, D.; Barnett, J.; Park, H. Opportunities for Improving How and When Canadians Are Informed About New Prescription Medications. Manuscript Submitted. Manuscript Submitted.
- Schwalbe, K. Information Technology Project Management, 9th ed.; Cengage: Boston, MA, USA, 2019; ISBN 978-1-337-10135-6. [Google Scholar]
- Peterson, G.; Aslani, P.; Williams, K.A. How do Consumers Search for and Appraise Information on Medicines on the Internet? A Qualitative Study Using Focus Groups. J. Med. Internet Res. 2003, 5, e33. [Google Scholar] [CrossRef] [PubMed]
- Pew Research Center Internet Health Resources. Pew Research Center: Internet, Science & Technology; Pew Research Center: Washington, DC, USA, 2003. [Google Scholar]
- Beasley, J.W.; Wetterneck, T.B.; Temte, J.; Lapin, J.A.; Smith, P.; Rivera-Rodriguez, A.J.; Karsh, B.-T. Information Chaos in Primary Care: Implications for Physician Performance and Patient Safety. J. Am. Board Fam. Med. 2011, 24, 745–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Patel, H.K.; Bapat, S.S.; Bhansali, A.H.; Sansgiry, S.S. Development of Prescription Drug Information Leaflets: Impact of Cognitive Effort and Patient Involvement on Prescription Medication Information Processing. Ther. Innov. Regul. Sci. 2018, 52, 118–129. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Theme | Advantage (+) or Disadvantage (−) Reported for | ||
|---|---|---|---|
| Mobile App | Online | ||
| Availability | + | + | + |
| Ease of Access | + | (−) | ± |
| Findability | ± | ± | |
| Communication Method | + | + | (−) |
| Storage | + | (−) | |
| Security | (−) | + | |
| Flexibility | + | ||
| Personalization | + | ||
| Searchability | + | ||
| Frequency of Use | + | ± | |
| Trustworthiness | + | + | |
| Comprehensiveness | + | + | |
| Layered Content | + | ||
| Helpful in an Emergency | + | ||
| Medication Reminders | + | ||
| Theme | + or (−) | Illustrating Quote |
|---|---|---|
| Availability | + | Participant 1: “And just having it on my email, then I can access it wherever, whenever.” |
| Ease of Access | + | Participant 1: “I think in an email, where it’s like, I don’t have to make extra accounts for logging into a patient portal or anything like that.” |
| Findability | ± | Participant 9: “I can keep a digital version on email whenever I need it, I can find it.” Participant 3: “Because I find emails—you have to go through your emails, and search.” |
| Communication Method | + | Participant 15: “Email would be good because it would be straight to me … an app, you have to actually go and get it, or a website database … it’s not like it’s coming to you, you have to go to it, and I don’t think I would do that yet.” (push communication) Participant 7: “If I knew that I was able to respond to that email and be like, “I’m having this reaction. Should I go to the doctor?” Or, “Is this normal?” … as opposed to going into a pharmacy or having to go back to a walk-in clinic.” (interactive communication) |
| Storage | + | Participant 17: “Emails I can keep forever.” |
| Security | (−) | Participant 8: “If you’re emailing things to people it’s not really secure, and then people can potentially find out what kind of medications you’re taking and all that.” |
| Flexibility | + | Participant 13: “If it’s on your email, then you could potentially print it out. You could back it up. You could save it to a Google drive. You could do a lot of things with it.” |
| Personalization | + | Participant 7: “Email … I feel like if it was an app or a website, it would get right back to that really medically, jargony, generic information. Whereas if there would be a way to get the instructions that were more specific and simplified to me, I would prefer that.” |
| Searchability | + | Participant 2: “I can also search in it, if it’s a PDF, for specific things so it’s easier to find what I’m looking for.” |
| Frequency of Use | + | Participant 22: “Email because I get all my emails to my phone … every time I get an email, I’m really good about checking them right away … I would read through that.” |
| Trustworthiness | + | Participant 21: “That would be nice because then I would know that’s a valid resource.” |
| Theme | + or (−) | Illustrating Quote |
|---|---|---|
| Availability | + | Participant 23: “It’s nice when they give you a sheet but obviously, you’re prone to losing it so it become a nice to be able to have a backup copy, like if you could access it through that app.” |
| Ease of Access | (−) | Participant 25: “I feel like the app would just be clumsy and a lot of steps to have to go through to get to the thing.” |
| Communication Method | + | Participant 18: “I think the mobile app would be … ideal if my physician or family practice … or even the pharmacy. If they had their own personalized application that they had their patients sign up on, that would be great. So some sort of portal that connects the patient to the provider absolutely.” |
| Storage | (−) | Participant 13: “I wouldn’t like the idea of having to have a specific app that takes up space on my phone, just so that I could look up these things.” |
| Frequency of Use | + | Participant 9: “I’d use the app more often.” |
| (−) | Participant 35: “I think an app wouldn’t necessarily be that practical for me. Like I said, I don’t have very many prescriptions.” | |
| Comprehensiveness | + | Participant 3: “It would give me my need, like, ‘I’m taking this. Oh, I’d better refill this. It’s time to get some more.’” |
| Layered Content | + | Participant 27: “That could have a simplified version … it can be a bunch of text and pictures and stuff, and you can click the button and it simplifies everything. You can always have something like that, that’s just like, ‘Here’s the basic points,’ and then another tab that’s like, ‘Here’s the really detailed information.’ So, I think an app would be kind of cool.” |
| Helpful in an Emergency | + | Participant 10: “I think that a key feature for that actually might be that the app would push a link directly to a phone’s home screen. So, if someone needed to respond to an emergency, like an outside person, they could find this phone and then they’d have access to this information without knowing the password of this individual’s phone.” |
| Medication Reminders | + | Participant 16: “Maybe if I had something chronic that I did need reminders, and it was a little bit more encompassing, like I don’t know, diabetes or something, where I needed to do the tests and it was a bit more complicated, maybe an app would be useful.” |
| Theme | + or − | Illustrating Quote |
|---|---|---|
| Availability | + | Participant 3: “Online, that would be great. Because then, I would be able to access it whenever I needed to.” |
| Ease of Access | + | Participant 25: “Just a link on the website or like—on the London Drugs [Canadian pharmacy chain] website would work or on the manufacturer’s website or just somewhere.” |
| (−) | Participant 13: “I wouldn’t like the idea that the only way for me to get my prescription medication [information] would be for me to make an account with a username and a password that I have to remember.” | |
| Findability | + | Participant 6: “If there was a master website that you could always you could just Google and find out, then that would be nice.” |
| (−) | Participant 13: “I have to remember the website.” | |
| Communication Method | (−) | Participant 2: “If it was just found online, I probably wouldn’t take it upon myself to go look for it.” |
| Security | + | Participant 8: “I think if there was a database that you could look up, or some kind of secure access point, just because—I don’t really care, personally, but I would be concerned about confidentiality for other people.” |
| Trustworthiness | + | Participant 32: “online format that I knew was reliable, because it was from my pharmacy or Health Canada or something.” |
| Layered Content | + | Participant 32: “I think if it were just a website that had a directory of all the medications would be useful.” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Monkman, H.; Kushniruk, A.; Borycki, E.; Sheets, D.; Barnett, J.; Nøhr, C. The Medium Is the Message: How Do Canadian University Students Want Digital Medication Information? Life 2020, 10, 339. https://doi.org/10.3390/life10120339
Monkman H, Kushniruk A, Borycki E, Sheets D, Barnett J, Nøhr C. The Medium Is the Message: How Do Canadian University Students Want Digital Medication Information? Life. 2020; 10(12):339. https://doi.org/10.3390/life10120339
Chicago/Turabian StyleMonkman, Helen, Andre Kushniruk, Elizabeth Borycki, Debra Sheets, Jeff Barnett, and Christian Nøhr. 2020. "The Medium Is the Message: How Do Canadian University Students Want Digital Medication Information?" Life 10, no. 12: 339. https://doi.org/10.3390/life10120339