Development of Postoperative Pain in Patients with End-Stage Knee Osteoarthritis Is Associated with Upregulation of Genes Related to Extracellular Matrix Degradation, Inflammation, and Apoptosis Measured in the Peripheral Blood before Knee Surgery

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Clinical Testing
2.3. Quantification of MMP-9 and TIMP1 Protein Levels
2.4. Total RNA Isolation and Reverse Transcriptase (RT) Reaction
2.5. Real-Time Quantitative PCR
2.6. Statistical Analysis
2.7. Ethical Approval
3. Results
3.1. Clinical Parameters of the Examined Patients with End-Stage OA before Surgery
3.2. Baseline Clinical Parameters of the Examined OA Subjects, Who Developed Post-Surgical Pain after 6 Months Compared to Pain-Free Patients
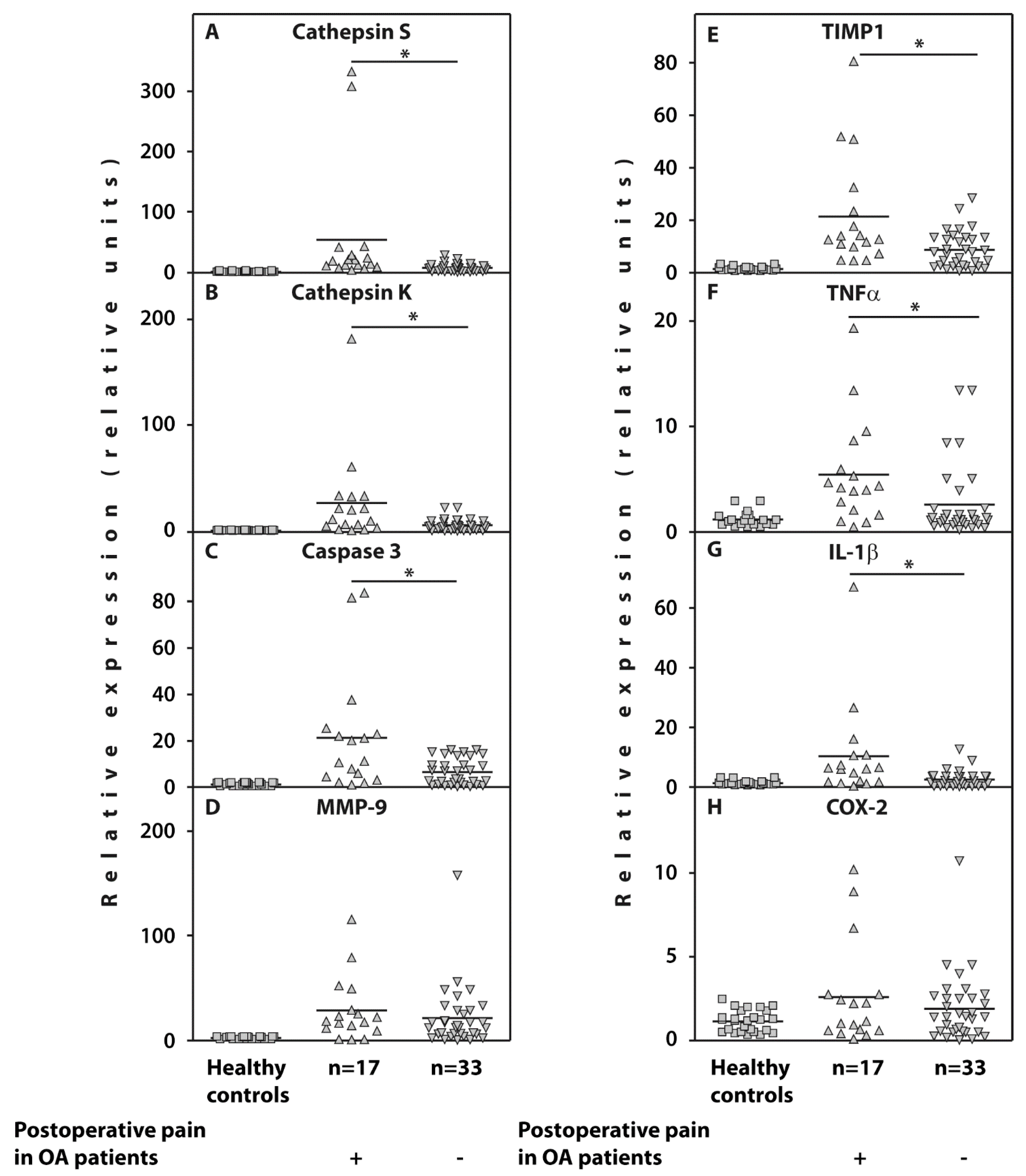
3.3. Whole Blood Gene Expression
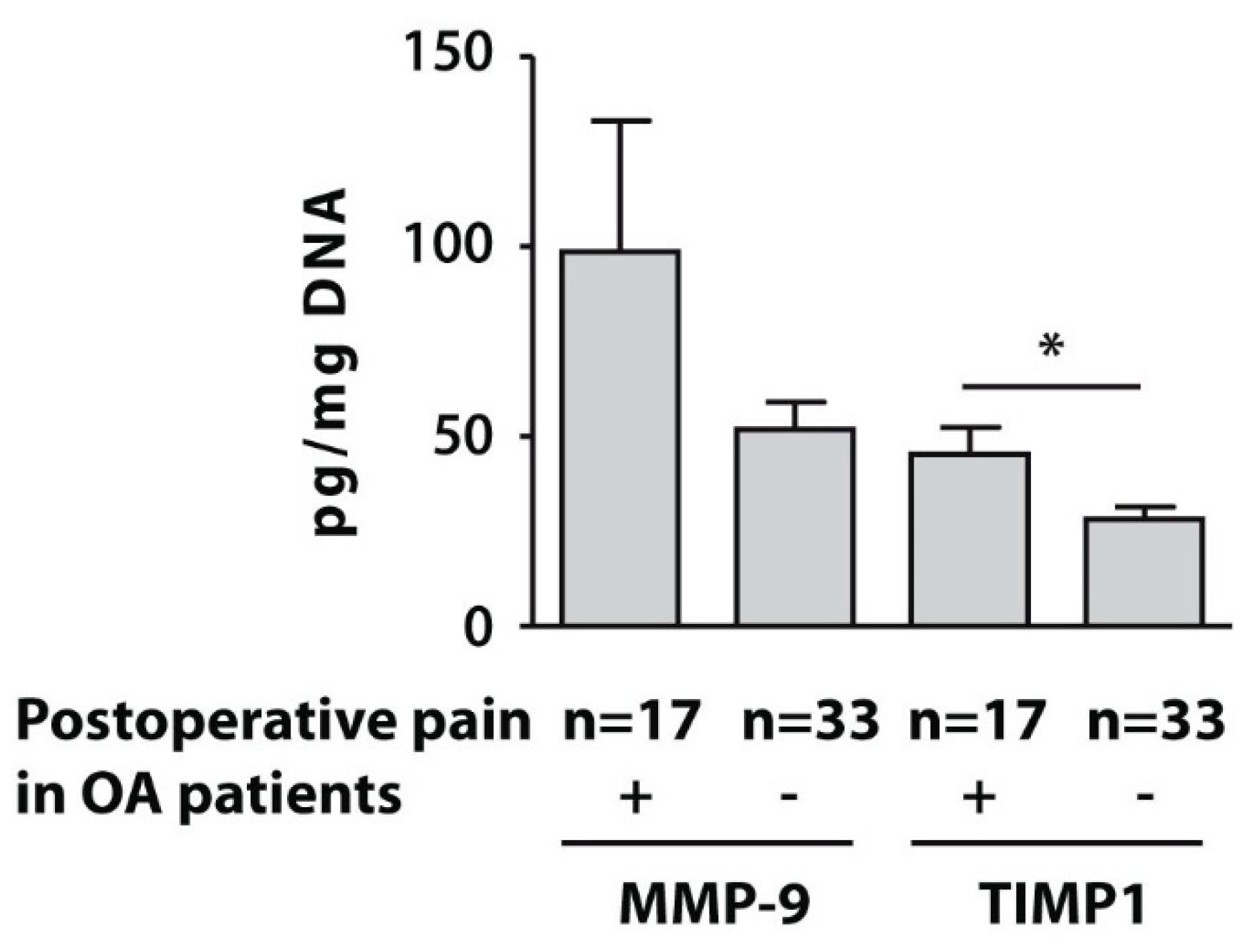
3.4. Protein Levels of MMP-9 and TIMP1 in Isolated PBMCs
3.5. Correlation Analyses of the Gene Expressions with Clinical and Radiographic Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Loeser, R.F.; Goldring, S.R.; Scanzello, C.R.; Goldring, M.B. Osteoarthritis: A disease of the joint as an organ. Arthritis Rheum. 2012, 64, 1697–1707. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurtz, S.; Ong, K.; Lau, E.; Mowat, F.; Halpern, M. Projections of primary and revision hip and knee arthroplasty in the United States from 2005 to 2030. J. Bone Jt. Surg. Am. 2007, 89, 780–785. [Google Scholar] [CrossRef]
- Wylde, V.; Hewlett, S.; Learmonth, I.D.; Dieppe, P. Persistent pain after joint replacement: Prevalence, sensory qualities, and postoperative determinants. Pain 2011, 152, 566–572. [Google Scholar] [CrossRef] [PubMed]
- Santaguida, P.L.; Hawker, G.A.; Hudak, P.L.; Glazier, R.; Mahomed, N.N.; Kreder, H.J.; Coyte, P.C.; Wright, J.G. Patient characteristics affecting the prognosis of total hip and knee joint arthroplasty: A systematic review. Can. J. Surg. 2008, 51, 428–436. [Google Scholar] [PubMed]
- Kidd, B.L.; Urban, L.A. Mechanisms of inflammatory pain. Br. J. Anaesth. 2001, 87, 3–11. [Google Scholar] [CrossRef] [Green Version]
- Treede, R.D.; Jensen, T.S.; Campbell, J.N.; Cruccu, G.; Dostrovsky, J.O.; Griffin, J.W.; Treede, R.D.; Jensen, T.S.; Campbell, J.N.; Cruccu, G.; et al. Neuropathic pain: Redefinition and a grading system for clinical and research purposes. Neurology 2008, 70, 1630–1635. [Google Scholar] [CrossRef]
- Campbell, J.N.; Meyer, R.A. Mechanisms of neuropathic pain. Neuron 2006, 52, 77–92. [Google Scholar] [CrossRef] [Green Version]
- Nijs, J.; Van Houdenhove, B.; Oostendorp, R.A. Recognition of central sensitization in patients with musculoskeletal pain: Application of pain neurophysiology in manual therapy practice. Man. Ther. 2010, 15, 135–141. [Google Scholar] [CrossRef]
- Akinci, A.; Al Shaker, M.; Chang, M.H.; Cheung, C.W.; Danilov, A.; Dueñas, H.J.; Kim, Y.C.; Guillen, R.; Tassanawipas, W.; Treuer, T.; et al. Predictive factors and clinical biomarkers for treatment in patients with chronic pain caused by osteoarthritis with a central sensitisation component. Int. J. Clin. Pract. 2016, 70, 31–44. [Google Scholar] [CrossRef] [Green Version]
- Petersen, K.K.; Arendt-Nielsen, L.; Simonsen, O.; Wilder-Smith, O.; Laursen, M.B. Presurgical assessment of temporal summation of pain predicts the development of chronic postoperative pain 12 months after total knee replacement. Pain 2015, 156, 55–61. [Google Scholar] [CrossRef]
- Edwards, R.R.; Mensing, G.; Cahalan, C.; Greenbaum, S.; Narang, S.; Belfer, I.; Schreiber, K.L.; Campbell, C.; Wasan, A.D.; Jamison, R.N. Alteration in pain modulation in women with persistent pain after lumpectomy: Influence of catastrophizing. J. Pain Symptom Manag. 2013, 46, 30–42. [Google Scholar] [CrossRef] [PubMed]
- Yarnitsky, D.; Crispel, Y.; Eisenberg, E.; Granovsky, Y.; Ben-Nun, A.; Sprecher, E.; Best, L.-A.; Granot, M. Prediction of chronic post-operative pain: Preoperative DNIC testing identifies patients at risk. Pain 2008, 138, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Kurien, T.; Arendt-Nielsen, L.; Petersen, K.K.; Graven-Nielsen, T.; Scammell, B.E. Preoperative Neuropathic Pain-like Symptoms and Central Pain Mechanisms in Knee Osteoarthritis Predicts Poor Outcome 6 Months after Total Knee Replacement Surgery. J. Pain 2018, 19, 1329–1341. [Google Scholar] [CrossRef] [PubMed]
- Sangesland, A.; Støren, C.; Vaegter, H.B. Are preoperative experimental pain assessments correlated with clinical pain outcomes after surgery? A systematic review. Scand. J. Pain 2017, 15, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Hernández, C.; Díaz-Heredia, J.; Berraquero, M.L.; Crespo, P.; Loza, E.; Ruiz Ibán, M.A. Pre-operative Predictive Factors of Post-operative Pain in Patients With Hip or Knee Arthroplasty: A Systematic Review. Reumatol. Clin. 2015, 11, 361–380. [Google Scholar] [CrossRef]
- Hilton, M.E.; Gioe, T.; Noorbaloochi, S.; Singh, J.A. Increasing comorbidity is associated with worsening physical function and pain after primary total knee arthroplasty. BMC Musculoskelet. Disord. 2016, 17, 421. [Google Scholar] [CrossRef] [Green Version]
- Hawker, G.A.; Badley, E.M.; Borkhoff, C.M.; Croxford, R.; Davis, A.M.; Dunn, S.; Gignac, M.A.; Jaglal, S.B.; Kreder, H.J.; Sale, J.E.M. Which Patients Are Most Likely to Benefit From Total Joint Arthroplasty? Arthritis Rheum. 2013, 65, 1243–1252. [Google Scholar] [CrossRef]
- Lungu, E.; Vendittoli, P.-A.; Desmeules, F. Preoperative Determinants of Patient-reported Pain and Physical Function Levels Following Total Knee Arthroplasty: A Systematic Review. Open Orthop. J. 2016, 10, 213–231. [Google Scholar] [CrossRef] [Green Version]
- Ji, R.R.; Xu, Z.Z.; Gao, Y.J. Emerging targets in neuroinflammation-driven chronic pain. Nat. Rev. Drug Discov. 2014, 13, 533–548. [Google Scholar] [CrossRef] [Green Version]
- Gandhi, R.; Santone, D.; Takahashi, M.; Dessouki, O.; Mahomed, N.N. Inflammatory Predictors of Ongoing Pain 2 Years Following Knee Replacement Surgery. Knee 2013, 20, 316–318. [Google Scholar] [CrossRef]
- Altman, R.; Asch, E.; Bloch, D. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Arthritis Rheum. 1986, 29, 1039–1052. [Google Scholar] [CrossRef] [PubMed]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteoarthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bellamy, N. WOMAC Osteoarthritis Index: A User’s Guide; University of Western Ontario: London, ON, Canada, 1995. [Google Scholar]
- Freynhagen, R.; Baron, R.; Gockel, U.; Tolle, T.R. PainDETECT: A new screening questionnaire to identify neuropathic components in patients with back pain. Curr. Med. Res. Opin. 2006, 22, 1911–1920. [Google Scholar] [CrossRef] [PubMed]
- Bouhassira, D.; Attal, N.; Alchaar, H.; Boureau, F.; Brachet, B.; Bruxelle, J.; Cunin, G.; Fermanian, J.; Ginies, P.; Grun-Overdyking, A.; et al. Comparison of pain syndromes associated with nervous or somatic lesions and development of a new neuropathic pain diagnostic questionnaire (DN4). Pain 2005, 114, 29–36. [Google Scholar] [CrossRef]
- Cleeland, C.S. Measurement of pain by subjective report. In Issues in Pain Measurement. Advances in Pain Research and Therapy; Chapman, C.R., Loeser, J.D., Eds.; Raven Press: New York, NY, USA, 1989; Volume 12, pp. 391–403. [Google Scholar]
- Zigmond, A.S.; Snaith, R.P. The hospital anxiety and depression scale. Acta Psychiatr. Scand. 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Son, B.K.; Roberts, R.L.; Ank, B.J. Effects of anticoagulant, serum, and temperature on the natural killer activity of human peripheral blood mononuclear cells stored overnight. Clin. Diagn. Lab. Immunol. 1996, 3, 260–264. [Google Scholar] [CrossRef] [Green Version]
- Tchetina, E.V.; Poole, A.R.; Zaitseva, E.M.; Sharapova, E.P.; Kashevarova, N.G.; Taskina, E.A.; Alekseeva, L.I.; Semyonova, L.A.; Glukhova, S.I.; Kuzin, A.N.; et al. Differences in mTOR (mammalian target of rapamycin) gene expression in the peripheral blood and articular cartilages of osteoarthritic patients and disease activity. Arthritis 2013, 2013, 461486. [Google Scholar] [CrossRef]
- Livak, K.J. Comparative Ct method. ABI Prism 7700 sequence detection system. In User Bulletin No. 2; PE Applied Biosystems: Foster City, CA, USA, 1997. [Google Scholar]
- Lewis, G.N.; Rice, D.A.; McNair, P.J.; Kluger, M. Predictors of persistent pain after total knee arthroplasty: A systematic review and meta-analysis. Br. J. Anaesth. 2015, 114, 551–561. [Google Scholar] [CrossRef] [Green Version]
- Barroso, J.; Wakaizumi, K.; Reckziegel, D.; Pinto-Ramos, J.; Schnitzer, T.; Galhardo, V.; Apkarian, A.V. Prognostics for pain in osteoarthritis: Do clinical measures predict pain after total joint replacement? PLoS ONE 2020, 15, e0222370. [Google Scholar] [CrossRef] [Green Version]
- Li, L.; Li, Z.; Li, Y.; Hu, X.; Zhang, Y.; Fan, P. Profiling of inflammatory mediators in the synovial fluid related to pain in knee osteoarthritis. BMC Musculoskelet. Disord. 2020, 21, 99. [Google Scholar] [CrossRef] [Green Version]
- Knight, B.E.; Kozlowski, N.; Havelin, J.; King, T.; Crocker, S.J.; Young, E.E.; Baumbauer, K.M. TIMP-1 Attenuates the Development of Inflammatory Pain through MMP-Dependent and Receptor-Mediated Cell Signaling Mechanisms. Front. Mol. Neurosci. 2019, 12, 220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eckert, W.A., III; Wiener, J.J.M.; Cai, H.; Ameriks, M.K.; Zhu, J.; Ngo, K.; Nguyen, S.; Fung-Leung, W.-P.; Thurmond, R.L.; Grice, C.; et al. Selective Inhibition of Peripheral Cathepsin S Reverses Tactile Allodynia Following Peripheral Nerve Injury in Mouse. Eur. J. Pharmacol. 2020, 880, 173171. [Google Scholar] [CrossRef] [PubMed]
- Nwosu, L.N.; Gowler, P.R.W.; Burston, J.J.; Rizoska, B.; Tunblad, K.; Lindström, E.; Grabowska, U.; Li, L.; McWilliams, D.F.; Walsh, D.A.; et al. Analgesic effects of the cathepsin K inhibitor L-006235 in the monosodium iodoacetate model of osteoarthritis pain. Pain Rep. 2018, 3, e685. [Google Scholar] [CrossRef] [PubMed]
- Hulse, R.P.; Beazley-Long, N.; Ved, N.; Bestall, S.M.; Riaz, H.; Singhal, P.; Ballmer, A.; Hofer, K.; Harper, S.J.; Bates, D.O.; et al. Vascular endothelial growth factor-A165b prevents diabetic neuropathic pain and sensory neuronal degeneration. Clin. Sci. 2015, 129, 741–756. [Google Scholar] [CrossRef]
- Katz, N.P.; Paillard, F.C.; Ekman, E. Determining the clinical importance of treatment benefits for interventions for painful orthopedic conditions. J. Orthop. Surg. Res. 2015, 10, 24. [Google Scholar] [CrossRef] [Green Version]
- Mai, L.; Zhu, X.; Huang, F.; He, H.; Fan, W. p38 Mitogen-Activated Protein Kinase and Pain. Life Sci. 2020, 256, 117885. [Google Scholar] [CrossRef]
- Lingard, E.A.; Katz, J.N.; Wright, E.A.; Sledge, C.B.; Kinemax Outcomes Group. Predicting the outcome of total knee arthroplasty. J. Bone Jt. Surg. Am. 2004, 86, 2179–2186. [Google Scholar] [CrossRef]
- Rajamäki, T.J.; Puolakka, P.A.; Hietaharju, A.; Moilanen, T.; Jämsen, E. Predictors of the use of analgesic drugs 1 year after joint replacement: A single-center analysis of 13,000 hip and knee replacements. Arthritis Res. Ther. 2020, 22, 89. [Google Scholar] [CrossRef] [Green Version]
- Rehman, Y.; Lindberg, M.F.; Arnljot, K.; Gay, C.L.; Lerdal, A.; Aamodt, A. More Severe Radiographic Osteoarthritis Is Associated With Increased Improvement in Patients’ Health State Following a Total Knee Arthroplasty. J. Arthroplast. 2020, in press. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indices | Patients Who Developed Pain 6 Months after Surgery N = 17 | Pain-Free Patients 6 Months after Surgery N = 33 | p-Value (Mann-Whitney U-Test) |
|---|---|---|---|
| Patients age, years | 70 (64;75) | 68 (61;72) | 0.70 |
| Gender males females | 3 (18%) 14 (86%) | 10 (30%) 23 (70%) | 0.36 |
| Average Kellgren & Lowrence radiological stage | |||
| III | 12 (71%) | 23 (70%) | 0.94 |
| IV | 5 (29%) | 10 (30%) | 0.94 |
| BMI, kg/m2 | 32.4 (27.1;34.5) | 29.1 (27.3;32.1) | 0.31 |
| Disease duration, years | 8 (5.5;12) | 10 (5;14) | 0.90 |
| Erythrocyte Sedimentation Rate (ESR), mm/h | 8.5 (5.5;19) | 12 (10;25) | 0.27 |
| Pain (VAS), mm | 60 (60;70) | 70 (60;70) | 0.89 |
| DN4 score | 2 (1.5;3) | 2 (1;2) | 0.24 |
| PainDETECT score | 7 (4;9) | 4 (2;9) | 0.28 |
| HADS anxiety score | 7 (4.5;9.5) | 5.5 (3.5;7.5) | 0.07 |
| HADS depression score | 8.5 (6;10.5) | 7 (6;9) | 0.25 |
| BPI pain severity score | 4.5 (3.9;5.4) | 5.5 (4.5;5.8) | 0.07 |
| Total WOMAC, mm | 1130 (1020;1260) | 1150 (950;1200) | 0.99 |
| Total pain | 230 (195;260) | 230 (205;270) | 0.72 |
| Total stiffness | 100 (75;110) | 100 (80;115) | 0.65 |
| Total physical function | 820 (710;855) | 760 (685;830) | 0.48 |
| Comorbidities | |||
| Healthy weight, (BMI 18.29–24.9 kg/m2) | 1 (6%) | 2 (6%) | 1.00 |
| Overweight (BMI 25.0–29.9 kg/m2) | 5 (29%) | 17 (51.5%) | 0.14 |
| Obesity Class I (BMI 30.0–34.9 kg/m2) | 10 (59%) | 11 (33.5%) | 0.08 |
| Obesity Class II (BMI 35.0–39.9 kg/m2) | 1 (6%) | 3 (9%) | 0.71 |
| Arterial hypertension (%) | 65 | 30 | <0.01 |
| Cardiovascular disease (%) | 6 | 15 | 0.35 |
| Genes | Gene Expression in Patients Who Developed Pain 6 Months after Surgery N = 17 | Gene Expression in Pain-Free Patients 6 Months after Surgery N = 33 | p-Value (Mann-Whitney U-Test) |
|---|---|---|---|
| Cathepsin S | 19.5(10.5;35.9) | 7.2(2.5;11.1) | 0.0001 |
| Cathepsin K | 11.8(4.5;33.5) | 4.6(2.2;9.6) | 0.005 |
| Caspase 3 | 11.2(3.9;24.1) | 3.6(1.3;11.5) | 0.008 |
| TIMP1 | 12.4(8.2;27.5) | 7.6(2.4;13.0) | 0.005 |
| TNFα | 4.2(1.8;7.3) | 1.1(0.7;2.2) | 0.01 |
| IL-1β | 5.9(1.6;10.5) | 1.6(.3;3.5) | 0.002 |
| MMP-9 | 18.0(10.0;38.9) | 12.0(5.8;28.2) | 0.28 |
| COX-2 | 1.1(0.5;2.7) | 1.3(0.5;2.5) | 0.75 |
| Pain at Night (VAS), mm | Total Pain | Total Physical Function | Total WOMAC | DN4 Scores | HADS Depression Scores | |
|---|---|---|---|---|---|---|
| K&L radiological stage | 0.442 p = 0.04 | 0.512 p = 0.01 | ||||
| PainDETECT scores | 0.525 p = 0.01 | 0.708 p < 0.01 | 0.546 p = 0.03 | |||
| HADS anxiety scores | 0.551 p = 0.01 | 0.472 p = 0.03 | 0.678 p < 0.01 | |||
| HADS depression scores | 0.312 p = 0.03 | |||||
| BPI pain severity scores | 0.628 p < 0.01 | 0.541 p = 0.01 | 0.590 p < 0.01 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tchetina, E.V.; Glemba, K.E.; Markova, G.A.; Naryshkin, E.A.; Taskina, E.A.; Makarov, M.A.; Lila, A.M. Development of Postoperative Pain in Patients with End-Stage Knee Osteoarthritis Is Associated with Upregulation of Genes Related to Extracellular Matrix Degradation, Inflammation, and Apoptosis Measured in the Peripheral Blood before Knee Surgery. Life 2020, 10, 224. https://doi.org/10.3390/life10100224
Tchetina EV, Glemba KE, Markova GA, Naryshkin EA, Taskina EA, Makarov MA, Lila AM. Development of Postoperative Pain in Patients with End-Stage Knee Osteoarthritis Is Associated with Upregulation of Genes Related to Extracellular Matrix Degradation, Inflammation, and Apoptosis Measured in the Peripheral Blood before Knee Surgery. Life. 2020; 10(10):224. https://doi.org/10.3390/life10100224
Chicago/Turabian StyleTchetina, Elena V., Kseniya E. Glemba, Galina A. Markova, Evgeniy A. Naryshkin, Elena A. Taskina, Maksim A. Makarov, and Aleksandr M. Lila. 2020. "Development of Postoperative Pain in Patients with End-Stage Knee Osteoarthritis Is Associated with Upregulation of Genes Related to Extracellular Matrix Degradation, Inflammation, and Apoptosis Measured in the Peripheral Blood before Knee Surgery" Life 10, no. 10: 224. https://doi.org/10.3390/life10100224