
Anatomic Comparison of Contralateral Maxillary Second Molars Using High-Resolution Micro-CT

Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Enrolment
2.2. Micro-CT Analysis
2.3. Statistical Analysis
3. Results
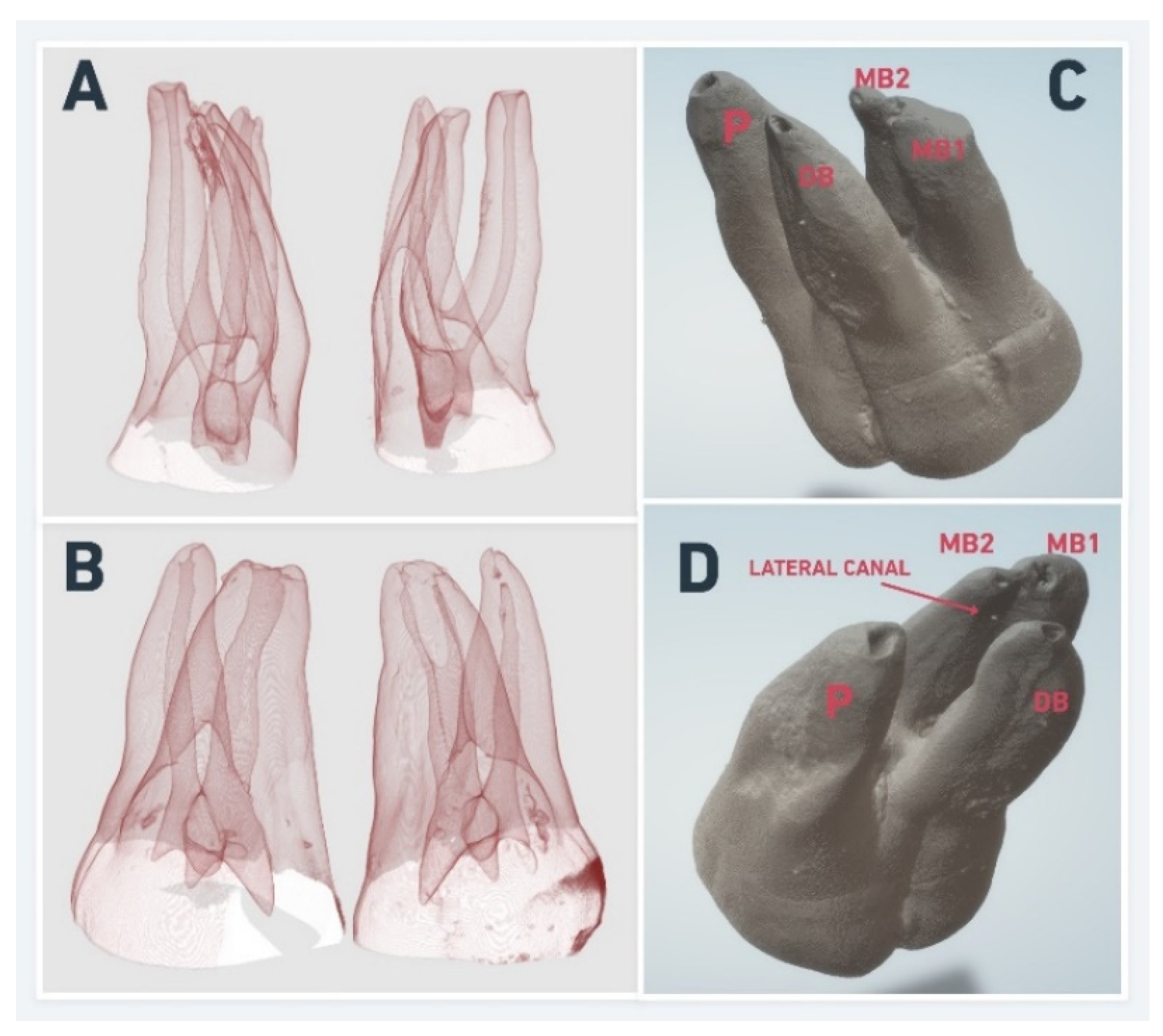
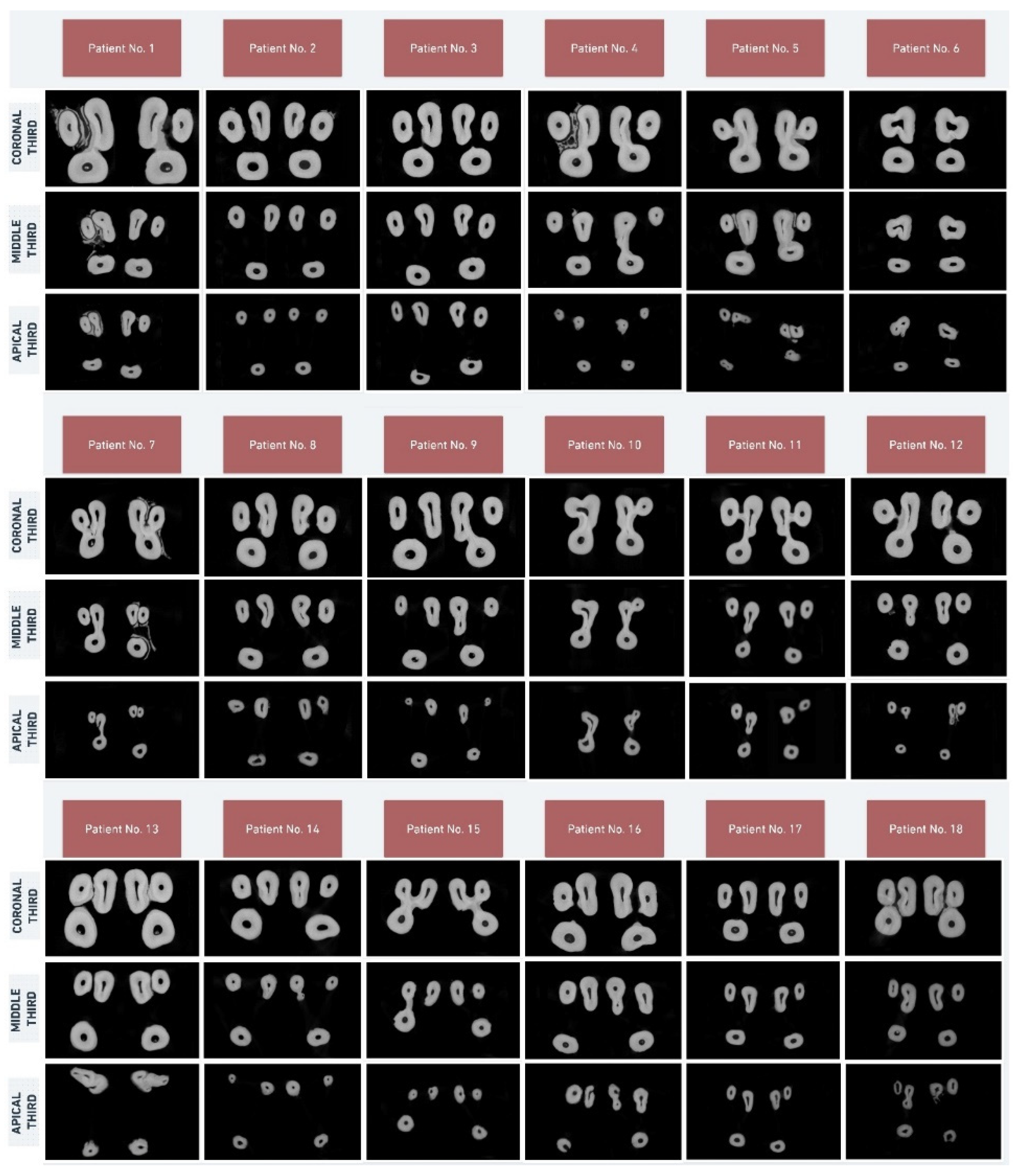
3.1. External Root and Root Canal Morphology
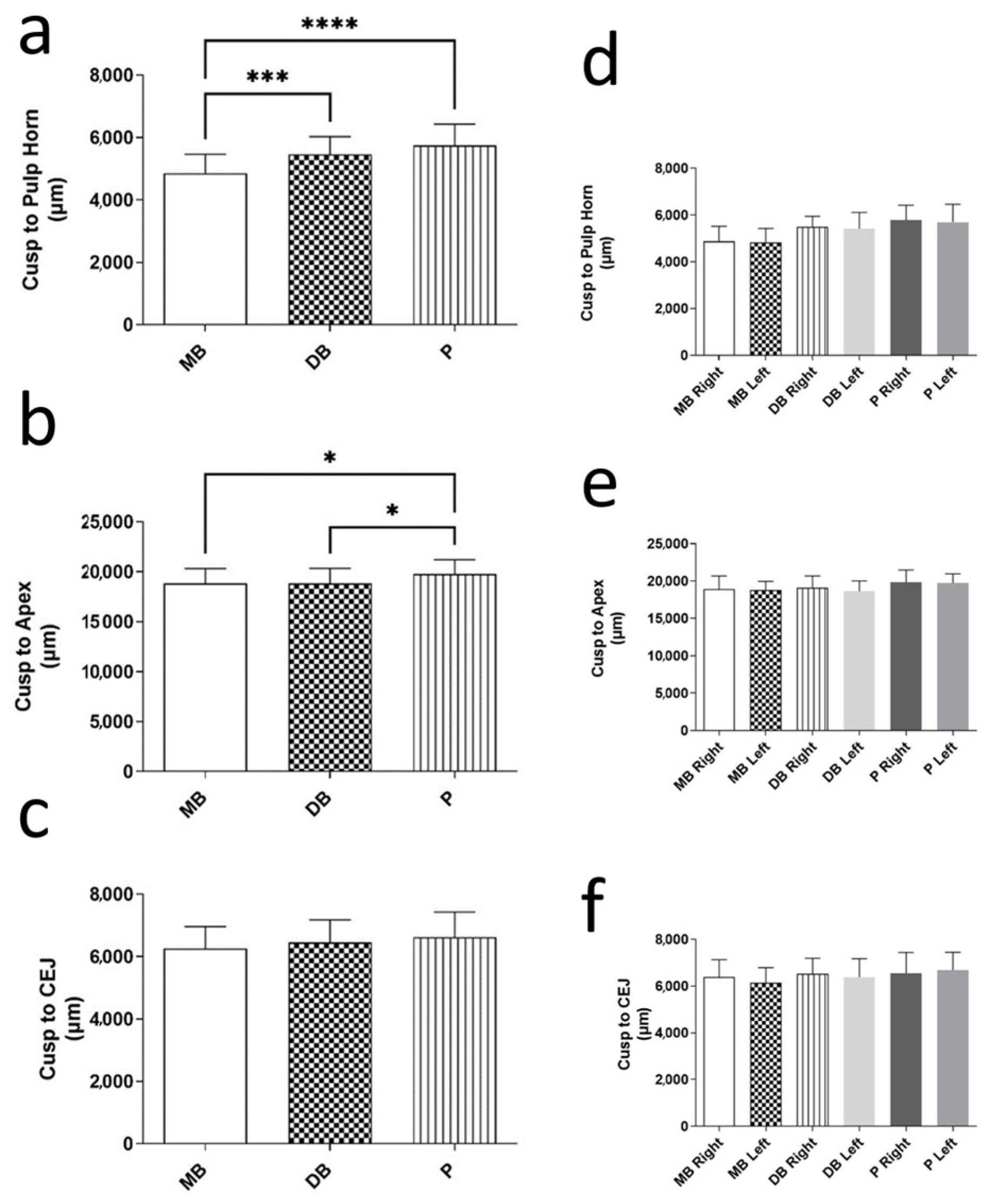
3.2. Cusp-to-Pulp Horn, Cusp-to-Apex, and Cusp-to-CEJ Distances
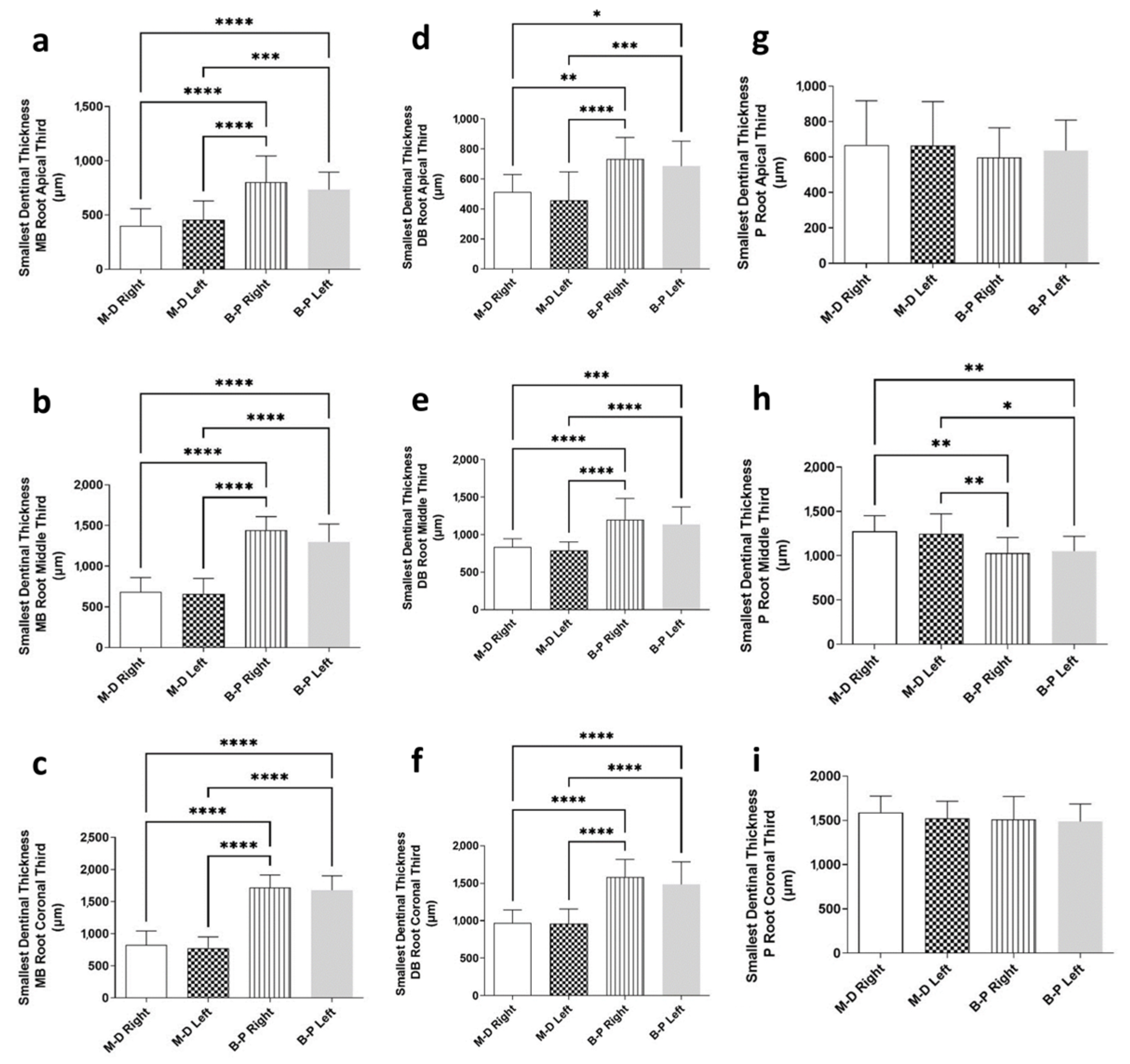
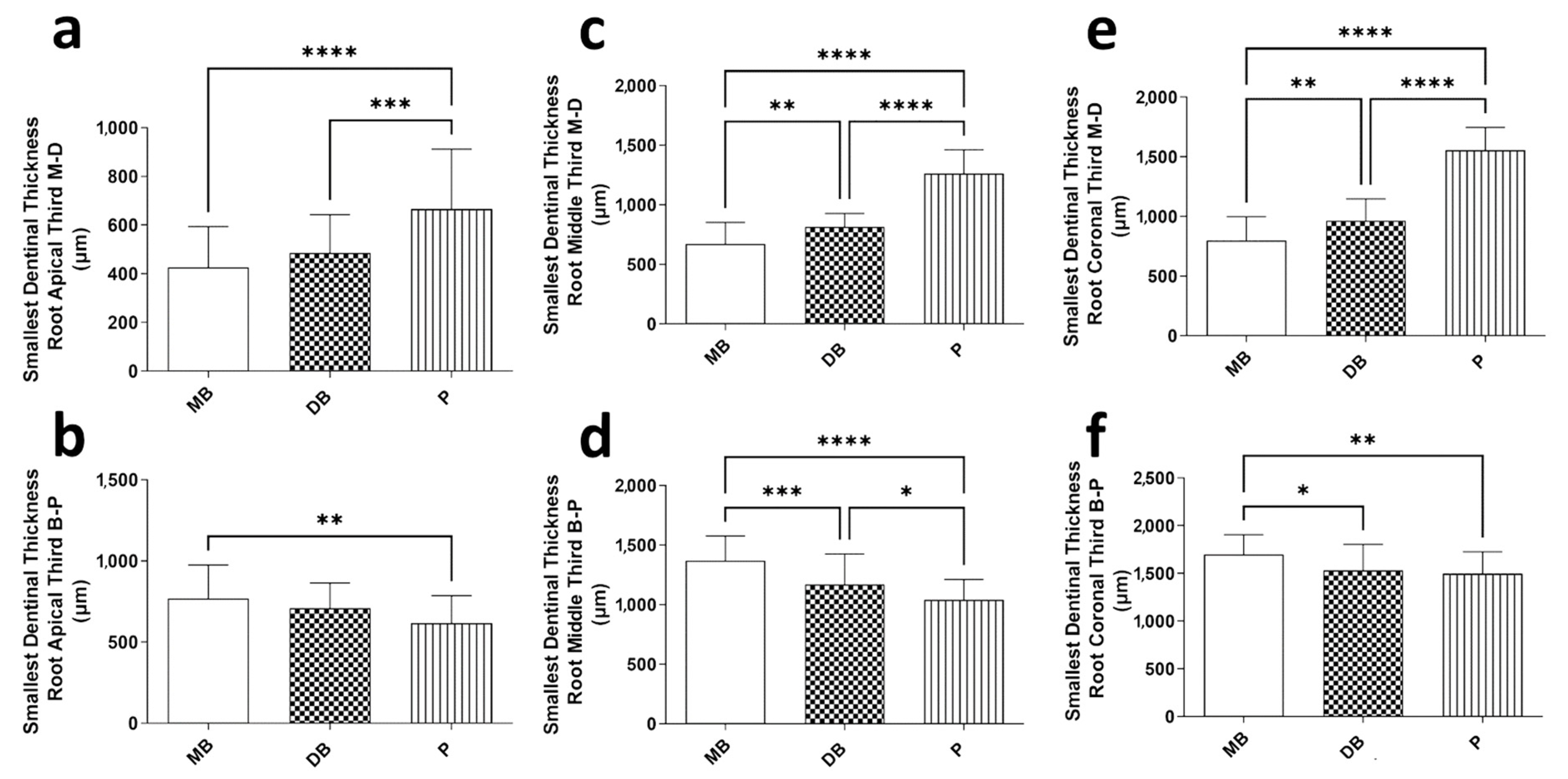
3.3. Smallest Dentinal Thickness in Apical, Middle, and Coronal Thirds
3.4. Number of Foramina and Lateral Canals and Locations of Lateral Canals
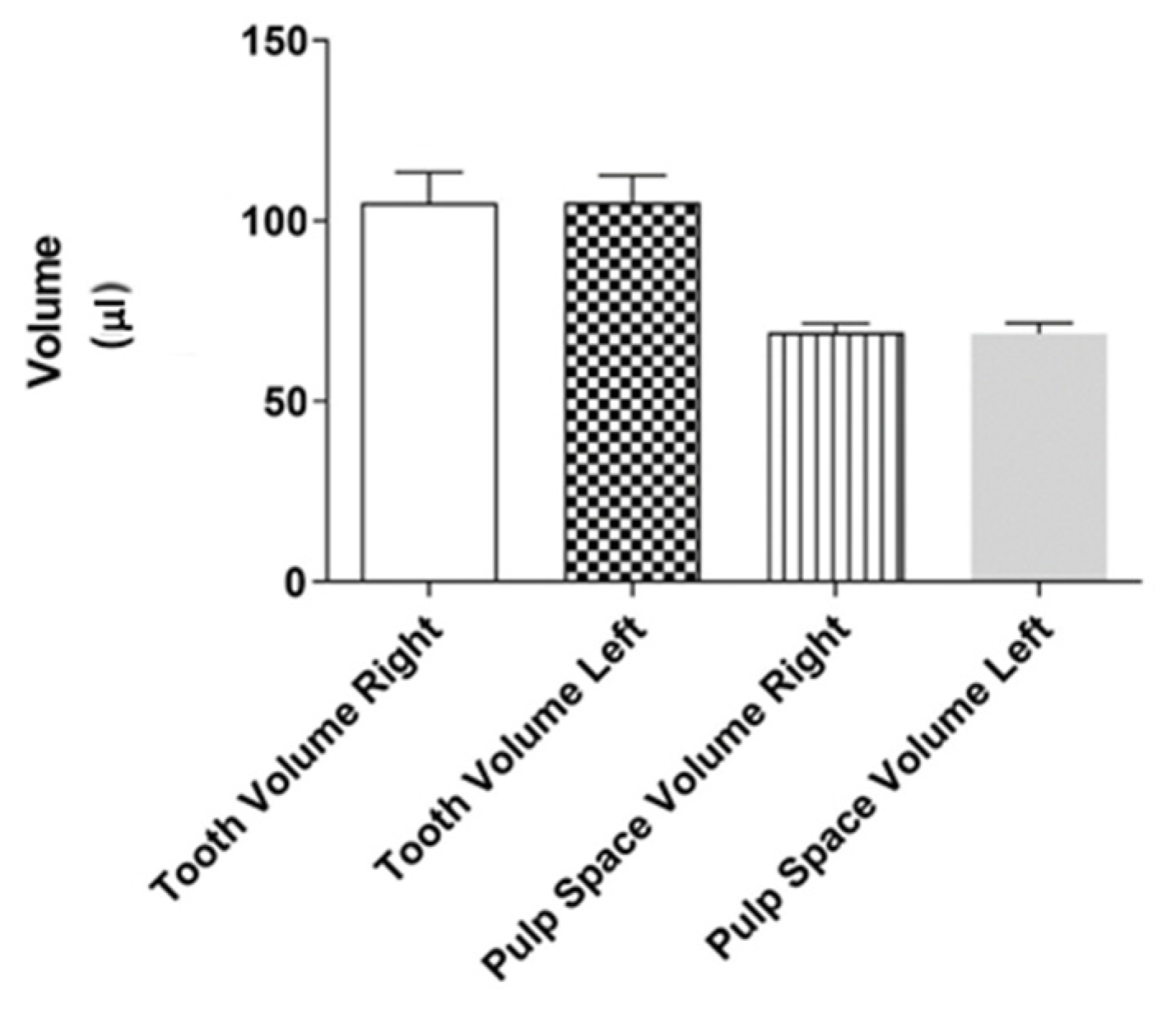
3.5. Tooth and Pulp Space Volume
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Martins, J.N.R.; Nole, C.; Ounsi, H.F.; Parashos, P.; Plotino, G.; Ragnarsson, M.F.; Aguilar, R.R.; Santiago, F.; Seedat, H.C.; Vargas, W.; et al. Worldwide Assessment of the Mandibular First Molar Second Distal Root and Root Canal: A Cross-sectional Study with Meta-analysis. J. Endod. 2022, 48, 223–233. [Google Scholar] [CrossRef]
- Friedman, S.; Abitbol, S.; Lawrence, H.P. Treatment outcome in endodontics: The Toronto Study. Phase 1: Initial treatment. J. Endod. 2003, 29, 787–793. [Google Scholar] [CrossRef]
- Setzer, F.C.; Boyer, K.R.; Jeppson, J.R.; Karabucak, B.; Kim, S. Long-term prognosis of endodontically treated teeth: A retrospective analysis of preoperative factors in molars. J. Endod. 2011, 37, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Ran, S.J.; Yang, X.; Sun, Z.; Zhang, Y.; Chen, J.X.; Wang, D.M.; Liu, B. Effect of length of apical root resection on the biomechanical response of a maxillary central incisor in various occlusal relationships. Int. Endod. J. 2020, 53, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Baruwa, A.O.; Martins, J.N.R.; Meirinhos, J.; Pereira, B.; Gouveia, J.; Quaresma, S.A.; Monroe, A.; Ginjeira, A. The Influence of Missed Canals on the Prevalence of Periapical Lesions in Endodontically Treated Teeth: A Cross-sectional Study. J. Endod. 2020, 46, 34–39. [Google Scholar] [CrossRef] [PubMed]
- Pereira, B.; Martins, J.N.R.; Baruwa, A.O.; Meirinhos, J.; Gouveia, J.; Quaresma, S.A.; Monroe, A.; Ginjeira, A. Association between Endodontically Treated Maxillary and Mandibular Molars with Fused Roots and Periapical Lesions: A Cone-beam Computed Tomography Cross-sectional Study. J. Endod. 2020, 46, 771–777. [Google Scholar] [CrossRef]
- Markvart, M.; Tibbelin, N.; Pigg, M.; EndoReCo; Fransson, H. Frequency of additional treatments in relation to the number of root filled canals in molar teeth in the Swedish adult population. Int. Endod. J. 2021, 54, 826–833. [Google Scholar] [CrossRef]
- Fransson, H.; Dawson, V.S.; Frisk, F.; Bjørndal, L.; EndoReCo; Kvist, T. Survival of Root-filled Teeth in the Swedish Adult Population. J. Endod. 2016, 42, 216–220. [Google Scholar] [CrossRef]
- Martins, J.N.; Mata, A.; Marques, D.; Caramês, J. Prevalence of Root Fusions and Main Root Canal Merging in Human Upper and Lower Molars: A Cone-beam Computed Tomography In Vivo Study. J. Endod. 2016, 42, 900–908. [Google Scholar] [CrossRef] [PubMed]
- Mashyakhy, M.; Chourasia, H.R.; Jabali, A.; Almutairi, A.; Gambarini, G. Analysis of Fused Rooted Maxillary First and Second Molars with Merged and C-shaped Canal Configurations: Prevalence, Characteristics, and Correlations in a Saudi Arabian Population. J. Endod. 2019, 45, 1209–1218. [Google Scholar] [CrossRef]
- Zhang, Q.; Chen, H.; Fan, B.; Fan, W.; Gutmann, J.L. Root and root canal morphology in maxillary second molar with fused root from a native Chinese population. J. Endod. 2014, 40, 871–875. [Google Scholar] [CrossRef] [PubMed]
- Aksoy, U.; Küçük, M.; Versiani, M.A.; Orhan, K. Publication trends in micro-CT endodontic research: A bibliometric analysis over a 25-year period. Int. Endod. J. 2021, 54, 343–353. [Google Scholar] [CrossRef]
- Plotino, G.; Tocci, L.; Grande, N.M.; Testarelli, L.; Messineo, D.; Ciotti, M.; Glassman, G.; D’ambrosio, F.; Gambarini, G. Symmetry of root and root canal morphology of maxillary and mandibular molars in a white population: A cone-beam computed tomography study in vivo. J. Endod. 2013, 39, 1545–1548. [Google Scholar] [CrossRef]
- Kirmizi, D.; Aksoy, U.; Orhan, K. Efficacy of Laser-Activated Irrigation and Conventional Techniques in Calcium Hydroxide Removal from Simulated Internal Resorption Cavities: Micro-CT Study. Photobiomodul. Photomed. Laser Surg. 2021, 39, 674–681. [Google Scholar] [CrossRef] [PubMed]
- Ordinola-Zapata, R.; Bramante, C.M.; Versiani, M.A.; Moldauer, B.I.; Topham, G.; Gutmann, J.L.; Nuñez, A.; Duarte, M.A.; Abella, F. Comparative accuracy of the Clearing Technique, CBCT and Micro-CT methods in studying the mesial root canal configuration of mandibular first molars. Int. Endod. J. 2017, 50, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Johnsen, G.F.; Dara, S.; Asjad, S.; Sunde, P.T.; Haugen, H.J. Anatomic Comparison of Contralateral Premolars. J. Endod. 2017, 43, 956–963. [Google Scholar] [CrossRef] [PubMed]
- Johnsen, G.F.; Sundnes, J.; Wengenroth, J.; Haugen, H.J. Methodology for Morphometric Analysis of Modern Human Contralateral Premolars. J. Comput. Assist. Tomogr. 2016, 40, 617–625. [Google Scholar] [CrossRef]
- Feldkamp, L.A.; Goldstein, S.A.; Parfitt, A.M.; Jesion, G.; Kleerekoper, M. The direct examination of three-dimensional bone architecture in vitro by computed tomography. J. Bone Miner Res. 1989, 4, 3–11. [Google Scholar] [CrossRef]
- Alavi, A.M.; Opasanon, A.; Ng, Y.L.; Gulabivala, K. Root and canal morphology of Thai maxillary molars. Int. Endod. J. 2002, 35, 478–485. [Google Scholar] [CrossRef]
- Divine, K.A.; McClanahan, S.B.; Fok, A. Anatomic Analysis of Palatal Roots of Maxillary Molars Using Micro-computed Tomography. J. Endod. 2019, 45, 724–728. [Google Scholar] [CrossRef]
- American Association of Endodontists. Glossary of Endodontic Terms, 10th ed.; American Association of Endodontists: Chicago, IL, USA, 2020; Available online: https://www.aae.org/specialty/clinical-resources/glossary-endodontic-terms/ (accessed on 22 January 2023).
- Aktuna Belgin, C.; Serindere, G.; Orhan, K. Accuracy and reliability of enamel and dentin thickness measurements on micro-computed tomography and digital periapical radiographs#. J. Foren. Rad. Imag. 2019, 18, 32–36. [Google Scholar]
- Fernandes, N.A.; Herbst, D.; Postma, T.C.; Bunn, B.K. The prevalence of second canals in the mesiobuccal root of maxillary molars: A cone beam computed tomography study. Aust. Endod. J. 2019, 45, 46–50. [Google Scholar] [CrossRef] [PubMed]
- Kalender, A.; Celikten, B.; Tufenkci, P.; Aksoy, U.; Basmacı, F.; Kelahmet, U.; Orhan, K. Cone beam computed tomography evaluation of maxillary molar root canal morphology in a Turkish Cypriot population. Biotech. Biotechn. Equip. 2016, 30, 145–150. [Google Scholar] [CrossRef]
- Reis, A.G.; Grazziotin-Soares, R.; Barletta, F.B.; Fontanella, V.R.; Mahl, C.R. Second canal in mesiobuccal root of maxillary molars is correlated with root third and patient age: A cone-beam computed tomographic study. J. Endod. 2013, 39, 588–592. [Google Scholar] [CrossRef]
- Martins, J.N.R.; Marques, D.; Silva, E.J.N.L.; Caramês, J.; Mata, A.; Versiani, M.A. Second mesiobuccal root canal in maxillary molars-A systematic review and meta-analysis of prevalence studies using cone beam computed tomography. Arch. Oral Biol. 2020, 113, 104589. [Google Scholar] [CrossRef]
- Baltacıoğlu, İ.H.; Demirel, G.; Kolsuz, M.E.; Orhan, K. In-vitro analysis of maxillary first molars morphology using three dimensional Micro-CT imaging: Considerations for restorative dentistry. Eur. Oral Res. 2018, 52, 75–81. [Google Scholar] [CrossRef]
- Carrion, S.J.; Coelho, M.S.; Soares, A.J.; Frozoni, M. Apical periodontitis in mesiobuccal roots of maxillary molars: Influence of anatomy and quality of root canal treatment, a CBCT study. Restor. Dent. Endod. 2022, 19, e37. [Google Scholar] [CrossRef] [PubMed]
- Kalender, A.; Orhan, K.; Aksoy, U.; Basmaci, F.; Er, F.; Alankus, A. Influence of the quality of endodontic treatment and coronal restorations on the prevalence of apical periodontitis in a Turkish Cypriot population. Med. Princ. Pract. 2013, 22, 173–177. [Google Scholar] [CrossRef]
- Ordinola-Zapata, R.; Martins, J.N.R.; Versiani, M.A.; Bramante, C.M. Micro-CT analysis of danger zone thickness in the mesiobuccal roots of maxillary first molars. Int. Endod. J. 2019, 52, 524–529. [Google Scholar] [CrossRef]
- Vertucci, F.J. Root canal anatomy of the human permanent teeth. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 1984, 58, 589–599. [Google Scholar] [CrossRef]
- Wolf, T.G.; Paqué, F.; Woop, A.C.; Willershausen, B.; Briseño-Marroquín, B. Root canal morphology and configuration of 123 maxillary second molars by means of micro-CT. Int. J. Oral Sci. 2017, 9, 33–37. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient No. | Right | Left | Symmetry in No. of Roots | Symmetry in Root Canal Configurations | ||||
|---|---|---|---|---|---|---|---|---|
| No. of Roots | Root | Vertucci’s Classification | No. of Roots | Root | Vertucci’s Classification | |||
| 1 | 3 | MB | Type V | 3 | MB | Type I | Yes | No |
| DB | Type I | DB | Type I | Yes | ||||
| P | Type I | P | Type I | Yes | ||||
| 2 | 3 | MB | Type I | 3 | MB | Type I | Yes | Yes |
| DB | Type I | DB | Type I | Yes | ||||
| P | Type I | P | Type I | Yes | ||||
| 3 | 3 | MB | Type I | 3 | MB | Type I | Yes | Yes |
| DB | Type I | DB | Type I | Yes | ||||
| P | Type I | P | Type I | Yes | ||||
| 4 | 3 | MB | Type I | 3 | MB | Type II | Yes | No |
| DB | Type I | DB | Type I | Yes | ||||
| P | Type I | P | Type I | Yes | ||||
| 5 | 3 | MB | Type V | 3 | MB | Type III | Yes | No |
| DB | Type I | DB | Type I | Yes | ||||
| P | Type I | P | Type V | No | ||||
| 6 | 2 | B | Type I | 2 | B | Type V | Yes | No |
| P | Type I | P | Type I | Yes | ||||
| 7 | 3 | MB | Type I | 3 | MB | Type I | Yes | Yes |
| DB | Type I | DB | Type I | Yes | ||||
| P | Type I | P | Type I | Yes | ||||
| 8 | 3 | MB | Type II | 3 | MB | Type II | Yes | Yes |
| DB | Type I | DB | Type I | Yes | ||||
| P | Type I | P | Type I | Yes | ||||
| 9 | 3 | MB | Type I | 3 | MB | Type II | Yes | No |
| DB | Type I | DB | Type I | Yes | ||||
| P | Type I | P | Type I | Yes | ||||
| 10 | 2 | B | Type V | 3 | MB | Type I | No | No |
| DB | Type I | No | ||||||
| P | Type I | P | Type I | Yes | ||||
| 11 | 3 | MB | Type I | 3 | MB | Type I | Yes | Yes |
| DB | Type I | DB | Type I | Yes | ||||
| P | Type I | P | Type I | Yes | ||||
| 12 | 3 | MB | Type III | 3 | MB | Type V | Yes | No |
| DB | Type I | DB | Type I | Yes | ||||
| P | Type I | P | Type I | Yes | ||||
| 13 | 3 | MB | Type I | 3 | MB | Type V | Yes | No |
| DB | Type I | DB | Type I | Yes | ||||
| P | Type I | P | Type I | Yes | ||||
| 14 | 3 | MB | Type V | 3 | MB | Type IV | Yes | No |
| DB | Type I | DB | Type I | Yes | ||||
| P | Type I | P | Type I | Yes | ||||
| 15 | 3 | MB | Type I | 3 | MB | Type I | Yes | Yes |
| DB | Type I | DB | Type I | Yes | ||||
| P | Type I | P | Type I | Yes | ||||
| 16 | 3 | MB | Type I | 3 | MB | Type V | Yes | No |
| DB | Type I | DB | Type I | Yes | ||||
| P | Type I | P | Type I | Yes | ||||
| 17 | 3 | MB | Type I | 3 | MB | Type I | Yes | Yes |
| DB | Type I | DB | Type I | Yes | ||||
| P | Type I | P | Type I | Yes | ||||
| 18 | 3 | MB | Type IV | 3 | MB | Type I | Yes | No |
| DB | Type III | DB | Type I | No | ||||
| P | Type I | P | Type I | Yes | ||||
| Patient No. | MB | DB | B | P | ||||
|---|---|---|---|---|---|---|---|---|
| Right | Left | Right | Left | Right | Left | Right | Left | |
| 1 | 2 | 3 | 2 | 1 | 1 | 1 | ||
| 2 | 1 | 1 | 1 | 2 | 1 | 1 | ||
| 3 | 1 | 1 | 1 | 1 | 1 | 1 | ||
| 4 | 3 | 2 | 1 | 1 | 1 | 1 | ||
| 5 | 2 | 2 | 1 | 1 | 2 | 2 | ||
| 6 | 2 | 4 | 1 | 1 | ||||
| 7 | 2 | 1 | 2 | 1 | 2 | 1 | ||
| 8 | 6 | 4 | 1 | 1 | 1 | 1 | ||
| 9 | 1 | 1 | 1 | 1 | 1 | 1 | ||
| 10 | 2 | 1 | 3 | 1 | 1 | |||
| 11 | 1 | 1 | 1 | 1 | 1 | 1 | ||
| 12 | 3 | 2 | 1 | 1 | 1 | 1 | ||
| 13 | 2 | 1 | 1 | 1 | 1 | 1 | ||
| 14 | 2 | 1 | 1 | 1 | 1 | 1 | ||
| 15 | 1 | 1 | 1 | 1 | 1 | 1 | ||
| 16 | 2 | 2 | 1 | 1 | 1 | 1 | ||
| 17 | 1 | 4 | 1 | 1 | 1 | 1 | ||
| 18 | 4 | 3 | 1 | 1 | 1 | 1 | ||
| Patient No. | MB | DB | B | P | ||||
|---|---|---|---|---|---|---|---|---|
| Right | Left | Right | Left | Right | Left | Right | Left | |
| 1 | 1 | 1 | 0 | 0 | 1 | 0 | ||
| 2 | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 3 | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 4 | 1 | 0 | 0 | 0 | 0 | 0 | ||
| 5 | 0 | 1 | 0 | 0 | 1 | 2 | ||
| 6 | 1 | 0 | 0 | 1 | ||||
| 7 | 1 | 2 | 1 | 0 | 1 | 2 | ||
| 8 | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 9 | 0 | 1 | 0 | 0 | 1 | 1 | ||
| 10 | 0 | 0 | 2 | 0 | 0 | |||
| 11 | 1 | 2 | 0 | 0 | 0 | 0 | ||
| 12 | 1 | 2 | 0 | 0 | 0 | 1 | ||
| 13 | 1 | 0 | 0 | 0 | 0 | 0 | ||
| 14 | 0 | 3 | 0 | 0 | 0 | 0 | ||
| 15 | 0 | 0 | 0 | 0 | 0 | 0 | ||
| 16 | 2 | 1 | 0 | 0 | 1 | 0 | ||
| 17 | 0 | 0 | 0 | 0 | 0 | 1 | ||
| 18 | 0 | 0 | 0 | 0 | 0 | 0 | ||
| Lateral Canal Locations | MB | DB | B | P |
|---|---|---|---|---|
| Coronal_Buccal | 1 | 0 | 0 | 3 |
| Coronal_Palatal | 2 | 0 | 0 | 0 |
| Coronal_Mesial | 1 | 0 | 0 | 0 |
| Coronal_Distal | 2 | 0 | 0 | 0 |
| Middle_Buccal | 2 | 0 | 0 | 0 |
| Middle_Palatal | 3 | 0 | 1 | 0 |
| Middle_Mesial | 3 | 0 | 0 | 0 |
| Middle_Distal | 3 | 0 | 0 | 1 |
| Apical_Buccal | 1 | 0 | 0 | 6 |
| Apical_Palatal | 2 | 0 | 2 | 1 |
| Apical_Mesial | 0 | 1 | 0 | 0 |
| Apical_Distal | 1 | 0 | 0 | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dandache, G.; Aksoy, U.; Ozel, M.B.; Orhan, K. Anatomic Comparison of Contralateral Maxillary Second Molars Using High-Resolution Micro-CT. Symmetry 2023, 15, 420. https://doi.org/10.3390/sym15020420
Dandache G, Aksoy U, Ozel MB, Orhan K. Anatomic Comparison of Contralateral Maxillary Second Molars Using High-Resolution Micro-CT. Symmetry. 2023; 15(2):420. https://doi.org/10.3390/sym15020420
Chicago/Turabian StyleDandache, Ghassan, Umut Aksoy, Mehmet Birol Ozel, and Kaan Orhan. 2023. "Anatomic Comparison of Contralateral Maxillary Second Molars Using High-Resolution Micro-CT" Symmetry 15, no. 2: 420. https://doi.org/10.3390/sym15020420