
Relapse after Orthodontic-Surgical Treatment: A Retrospective Longitudinal Study
 , ,
, ,  , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Selection of Participants
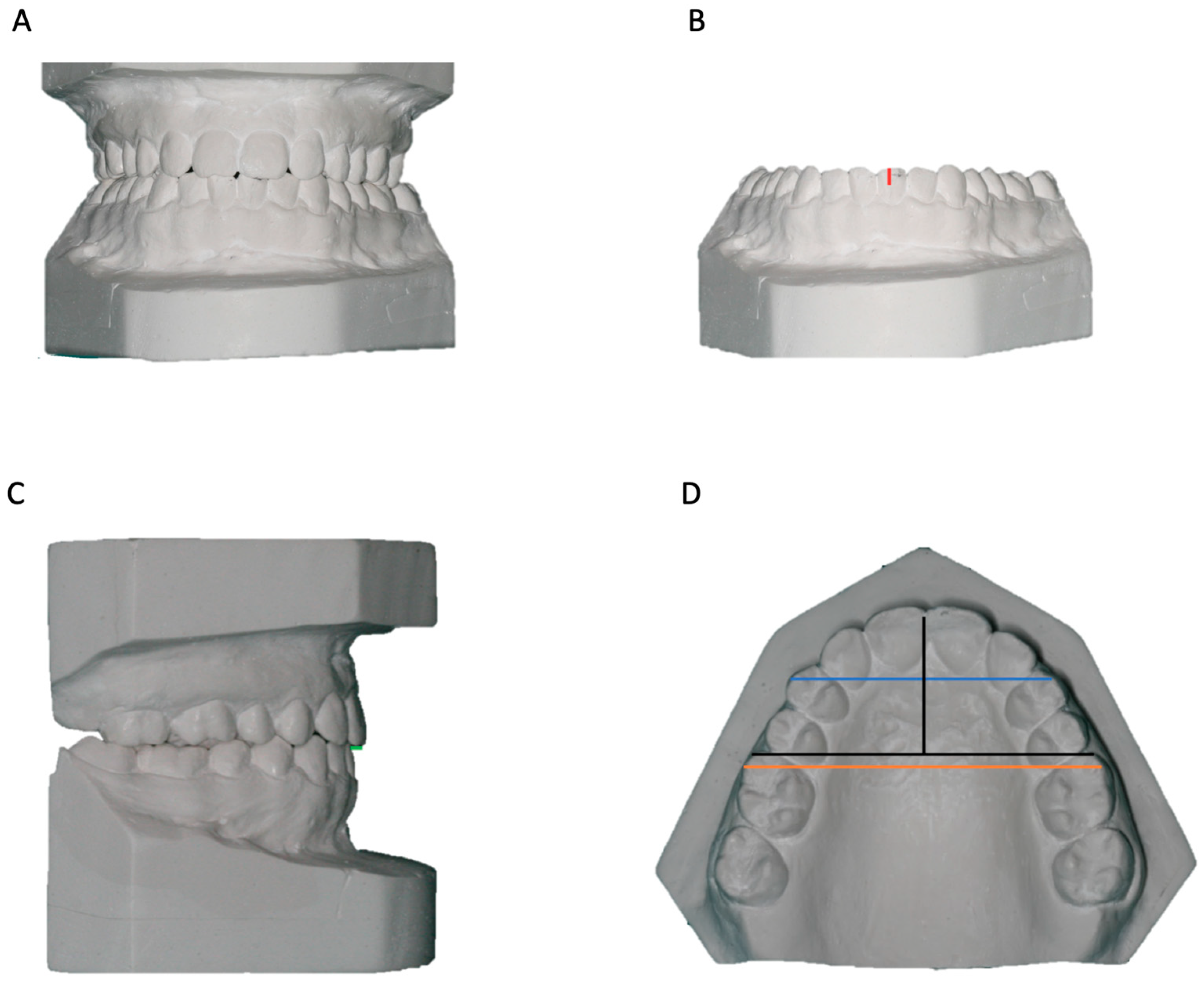
2.2. Evaluation of Dental Cast
2.3. Analysis of Lateral Cephalograms
2.4. Statistical Analysis
3. Results
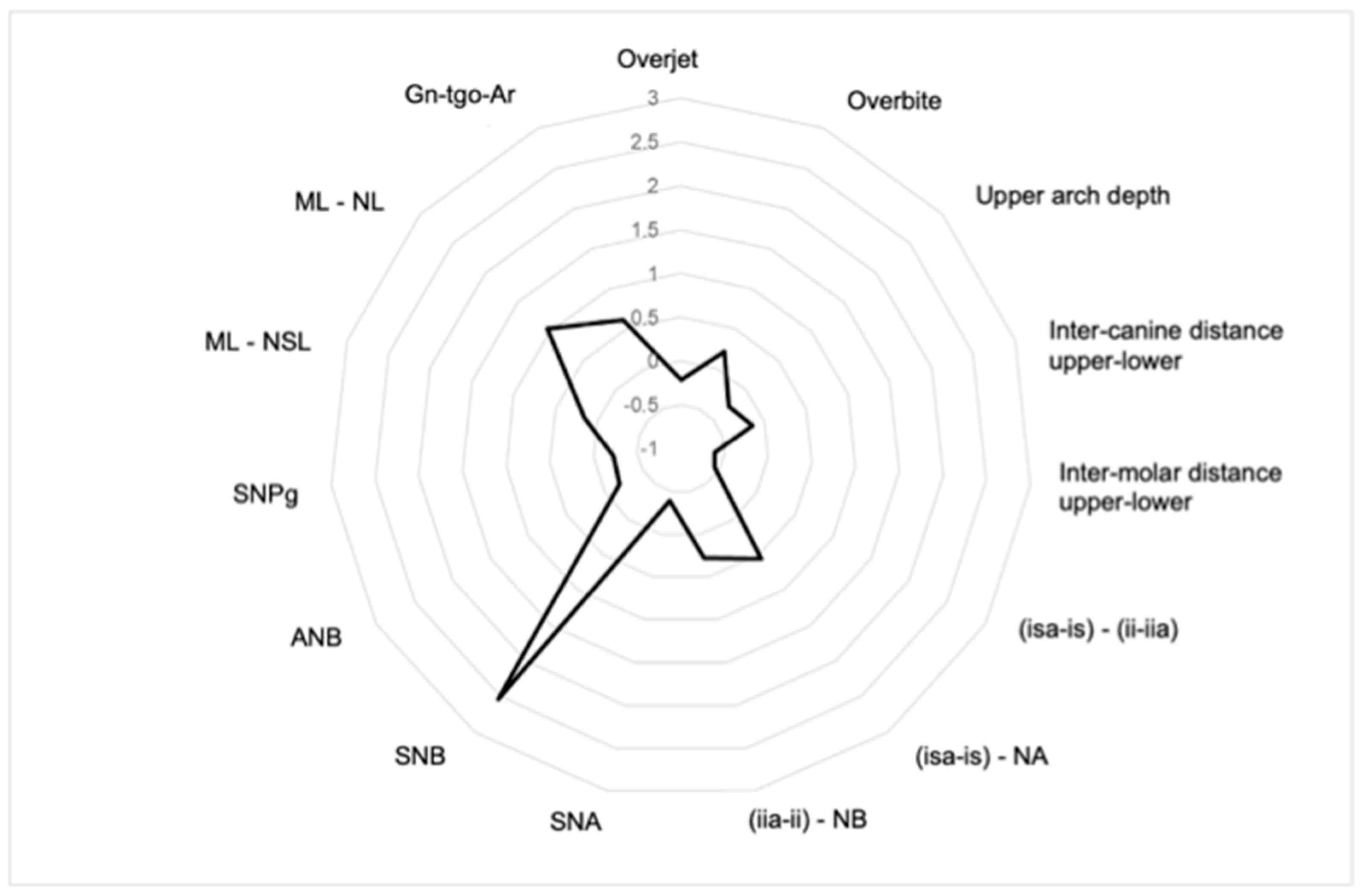
3.1. Dental and Skeletal Relapse
3.2. Influence of Malocclusion Type
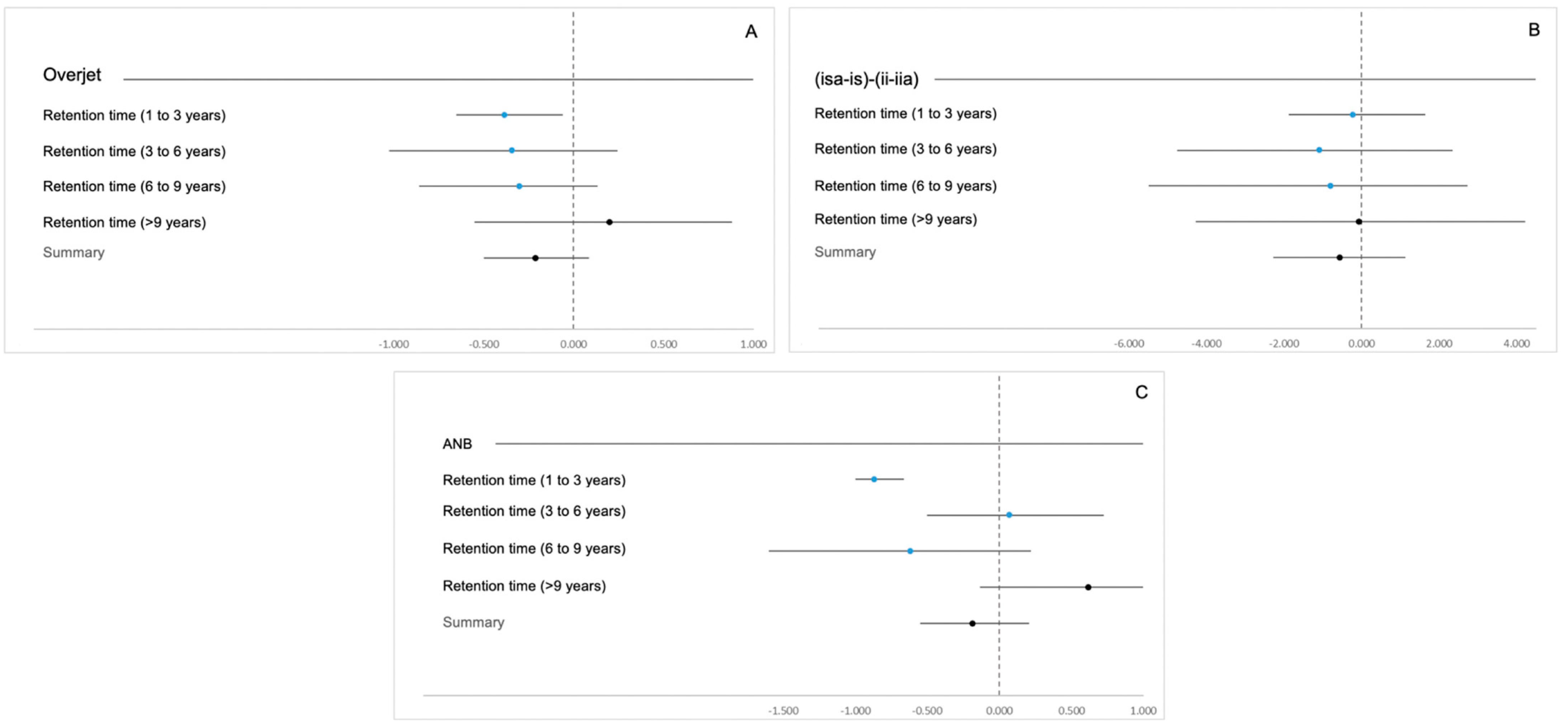
3.3. Influence of Retention Time
3.4. Influence of Sex and Age at the End of Treatment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cakirer, B.; Kucukkeles, N.; Nevzatoglu, S.; Koldas, T. Sagittal Airway Changes: Rapid Palatal Expansion versus Le Fort i Osteotomy during Maxillary Protraction. Eur. J. Orthod. 2012, 34, 381–389. [Google Scholar] [CrossRef]
- Yamada, T.; Sugiyama, G.; Mori, Y. Masticatory Muscle Function Affects the Pathological Conditions of Dentofacial Deformities. In Japanese Dental Science Review; Elsevier Ltd.: Amsterdam, The Netherlands, 2020; pp. 56–61. [Google Scholar] [CrossRef]
- Burgaz, M.A.; Eraydın, F.; Esener, S.D.; Ülkür, E. Patient with Severe Skeletal Class II Malocclusion: Double Jaw Surgery with Multipiece Le Fort I. Turk. J. Orthod. 2018, 31, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Proffit, W.R.; Fields, H.W.; Sarver, D.M. Contemporary Orthodontics, 5th ed.; Mosby: St. Louis, MO, USA, 2013. [Google Scholar]
- Choi, J.W.; Park, H.; Kwon, S.M.; Lee, J.Y. Surgery-First Orthognathic Approach for the Correction of Facial Asymmetry. J. Cranio-Maxillofac. Surg. 2021, 49, 435–442. [Google Scholar] [CrossRef]
- Jo, H.; Ohe, J.Y.; Lee, J.W.; Lee, B.S.; Jung, J. Posterior Bending Osteotomy: An Effective Measure to Secure Facial Symmetry in Orthognathic Surgery. J. Cranio-Maxillofac. Surg. 2021, 49, 538–544. [Google Scholar] [CrossRef]
- Antonarakis, G.S.; Herzog, G.; Kiliaridis, S. Vertical Relapse after Orthodontic and Orthognathic Surgical Treatment in a Patient with Myotonic Dystrophy. Eur. J. Paediatr. Dent. 2019, 20, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Halvorsen, E.T.; Beddari, I.Y.; Schilbred Eriksen, E.; Boe, O.E.; Wisth, P.J.; Loes, S.; Moen, K. Relapse and Stability after Mandibular Setback Surgery One Year Postoperatively: A Retrospective Study. J. Oral Maxillofac. Surg. 2014, 72, e1181. [Google Scholar] [CrossRef]
- Gaitán Romero, L.; Mulier, D.; Orhan, K.; Shujaat, S.; Shaheen, E.; Willems, G.; Politis, C.; Jacobs, R. Evaluation of Long-Term Hard Tissue Remodelling after Skeletal Class III Orthognathic Surgery: A Systematic Review. Int. J. Oral Maxillofac. Surg. 2020, 49, 51–61. [Google Scholar] [CrossRef]
- Depeursinge, A.; Racoceanu, D.; Iavindrasana, J.; Cohen, G.; Platon, A.; Poletti, P.-A.; Muller, H. Fusing Visual and Clinical Information for Lung Tissue Classification in HRCT Data. Artif. Intell. Med. 2010, 50, 13–21. [Google Scholar] [CrossRef]
- De Mol Van Otterloo, J.J.; Tuinzing, D.B.; Greebe, R.B.; Van Der Kwast, W.A.M. Intra-and Early Postoperative Complications of the Le Fort I Osteotomy A Retrospective Study on 410 Cases. J. Cranio-Maxillo-Facial Surg. 1991, 19, 217–222. [Google Scholar] [CrossRef]
- Bharti, D.; Mohindru, K.; Shetty, V.; Sunil Khanna, S.; Murugendrappa Gowdar, I.; Tiwari, R.V.; Tiwari, H. Evaluation Of Relapse In Orthognathic Surgery: An Original Research. Eur. J. Mol. Clin. Med. 2020, 7, 3210–3215. [Google Scholar]
- Joss, C.U.; Vassalli, I.M. Stability After Bilateral Sagittal Split Osteotomy Advancement Surgery With Rigid Internal Fixation: A Systematic Review. J. Oral Maxillofac. Surg. 2009, 67, 301–313. [Google Scholar] [CrossRef] [PubMed]
- Mobarak, K.A.; Espeland, L.; Krogstad, O.; Lyberg, T. Mandibular Advancement Surgery in High-Angle and Low-Angle Class II Patients: Different Long-Term Skeletal Responses. Am. J. Orthod. Dentofac. Orthop. 2001, 119, 368–381. [Google Scholar] [CrossRef] [PubMed]
- Gaitan Romero, L.; Shujaat, S.; Ma, H.; Orhan, K.; Shaheen, E.; Mulier, D.; Willems, G.; Politis, C.; Jacobs, R. Evaluation of long-term hard tissue relapse following surgical-orthodontic treatment in skeletal class II patients: A systematic review and meta-analysis. Int. J. Oral Maxillofac. Surg. 2021, 50, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Haas Junior, O.L.; Guijarro-Martínez, R.; de Sousa Gil, A.P.; da Silva Meirelles, L.; de Oliveira, R.B.; Hernández-Alfaro, F. Stability and Surgical Complications in Segmental Le Fort I Osteotomy: A Systematic Review. Int. J. Oral Maxillofac. Surg. 2017, 46, 1071–1087. [Google Scholar] [CrossRef]
- de Haan, I.F.; Ciesielski, R.; Nitsche, T.; Koos, B. Evaluation of relapse after orthodontic therapy combined with orthognathic surgery in the treatment of skeletal class III. J. Orofac. Orthop. 2013, 74, 362–369. [Google Scholar] [CrossRef] [PubMed]
- Mulier, D.; Gaitán Romero, L.; Führer, A.; Martin, C.; Shujaat, S.; Shaheen, E.; Politis, C.; Jacobs, R. Long-Term Dental Stability after Orthognathic Surgery: A Systematic Review. Eur. J. Orthod. 2021, 43, 104–112. [Google Scholar] [CrossRef]
- Kaklamanos, E.G.; Makrygiannakis, M.A.; Athanasiou, A.E. Could Medications and Biologic Factors Affect Post-Orthodontic Tooth Movement Changes? A Systematic Review of Animal Studies. In Orthodontics and Craniofacial Research; Blackwell Publishing Ltd.: Oxford, UK, 2021; pp. 39–51. [Google Scholar] [CrossRef]
- Proffit, W.R.; Turvey, T.A.; Phillips, C. The Hierarchy of Stability and Predictability in Orthognathic Surgery with Rigid Fixation: An Update and Extension. Head. Face Med. 2007, 3, 21. [Google Scholar] [CrossRef]
- Al-Delayme, R.; Al-Khen, M.; Hamdoon, Z.; Jerjes, W. Skeletal and Dental Relapses after Skeletal Class III Deformity Correction Surgery: Single-Jaw versus Double-Jaw Procedures. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2013, 115, 466–472. [Google Scholar] [CrossRef]
- Choi, T.H.; Kim, S.H.; Yun, P.Y.; Kim, Y.K.; Lee, N.K. Factors Related to Relapse after Mandibular Setback Surgery with Minimal Presurgical Orthodontics. J. Oral Maxillofac. Surg. 2019, 77, e1072. [Google Scholar] [CrossRef]
- Fahradyan, A.; Wolfswinkel, E.M.; Clarke, N.; Park, S.; Tsuha, M.; Urata, M.M.; Hammoudeh, J.A.; Yamashita, D.D.R. Impact of the Distance of Maxillary Advancement on Horizontal Relapse after Orthognathic Surgery. Cleft Palate-Craniofacial J. 2018, 55, 546–553. [Google Scholar] [CrossRef]
- Willmar, K. On Le Fort I Osteotomy. A Follow-up Study of 106 Operated Patients with Maxillo-Facial Deformity. Scand. J. Plast. Reconstr. Surg. 1974, 12, 1–68. [Google Scholar] [CrossRef] [PubMed]
- Posnick, J.C.; Ewing, M.P. Skeletal stability after Le Fort I maxillary advancement in patients with unilateral cleft lip and palate. Plast. Reconstr. Surg. 1990, 85, 706–710. [Google Scholar] [CrossRef] [PubMed]
- Eskenazi, L.B.; Schendel, S.A. An analysis of Le Fort I maxillary advancement in cleft lip and palate patients. Plast. Reconstr. Surg. 1992, 90, 779–786. [Google Scholar] [CrossRef] [PubMed]
- Dowling, P.A.; Espeland, L.; Sandvik, L.; Mobarak, K.A.; Hogevold, H.E. LeFort I Maxillary Advancement: 3-Year Stability and Risk Factors for Relapse. Am. J. Orthod. Dentofac. Orthop. 2005, 128, 560–567. [Google Scholar] [CrossRef]
- Dolce, C.; Hatch, J.P.; Van Sickels, J.E.; Rugh, J.D. Rigid versus Wire Fixation for Mandibular Advancement: Skeletal and Dental Changes after 5 Years. Am. J. Orthod. Dentofac. Orthop. 2002, 121, 610–619. [Google Scholar] [CrossRef] [PubMed]
- Brandtner, C.; Hachleitner, J.; Rippel, C.; Krenkel, C.; Gaggl, A. Long-Term Skeletal and Dental Stability after Orthognathic Surgery of the Maxillo-Mandibular Complex in Class II Patients with Transverse Discrepancies. J. Cranio-Maxillofac. Surg. 2015, 43, 1516–1521. [Google Scholar] [CrossRef]
- Proffit, W.R.; Phillips, C.; Turvey, T.A. Long-Term Stability of Adolescent versus Adult Surgery for Treatment of Mandibular Deficiency. Int. J. Oral Maxillofac. Surg. 2010, 39, 327–332. [Google Scholar] [CrossRef]
- De Lir, A.D.L.S.; De Moura, W.L.; Oliveira Ruellas, A.C.; Gomes Souza, M.M.; Nojima, L.I. Long-Term Skeletal and Profile Stability after Surgical-Orthodontic Treatment of Class II and Class III Malocclusion. J. Cranio-Maxillofac. Surg. 2013, 41, 296–302. [Google Scholar] [CrossRef]
- Janson, H.; Olsson, U. A Measure of Agreement for Interval or Nominal Multivariate Observations by Different Sets of Judges. Educ. Psychol. Meas. 2004, 64, 62–70. [Google Scholar] [CrossRef]
- Gallego-Romero, D.; José-Llamas-Carrera, M.; Torres-Lagares, D.; Paredes, V.; Espinar, E.; Guevara, E.; Gutiérrez-Pérez, J.L. Long-Term Stability of Surgical-Orthodontic Correction of Class III Malocclusions with Long-Face Syndrome. Med. Oral Patol. Oral Cir. Bucal 2012, 17. [Google Scholar] [CrossRef]
- Eggensperger, N.; Smolka, K.; Luder, J.; Iizuka, T. Short- and Long-Term Skeletal Relapse after Mandibular Advancement Surgery. Int. J. Oral Maxillofac. Surg. 2006, 35, 36–42. [Google Scholar] [CrossRef] [PubMed]
- Joss, C.U.; Thüer, U.W. Stability of the Hard and Soft Tissue Profile after Mandibular Advancement in Sagittal Split Osteotomies: A Longitudinal and Long-Term Follow-up Study. Eur. J. Orthod. 2008, 30, 16–23. [Google Scholar] [CrossRef]
- Moen, K.; Wisth, P.J.; Skaale, S.; Bøe, O.E.; Tornes, K. Dental or Skeletal Relapse after Sagittal Split Osteotomy Advancement Surgery? Long-Term Follow-Up. J. Oral Maxillofac. Surg. 2011, 69, e461–e468. [Google Scholar] [CrossRef] [PubMed]
- Schilbred Eriksen, E.; Wisth, P.J.; Løes, S.; Moen, K. Skeletal and Dental Stability after Intraoral Vertical Ramus Osteotomy: A Long-Term Follow-Up. Int. J. Oral Maxillofac. Surg. 2017, 46, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Kerstens, H.C.J.; Tuinzing, D.B.; Golding, R.P.; Van Der Kwast, W.A.M. Condylar Atrophy and Osteoarthrosis after Bimaxillary Surgery. Oral Surg. Oral Med. Oral Pathol. 1990, 69, 274–280. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, N.K.; Agarwal, S.S.; Datana, S.; Bhandari, S.K. Long-Term Study of Relapse After Mandibular Orthognathic Surgery: Advancement Versus Setback. J. Maxillofac. Oral Surg. 2022, 21, 469–480. [Google Scholar] [CrossRef]
- Eckmüller, S.; Paddenberg, E.; Hiller, K.A.; Proff, P.; Knüttel, H.; Kirschneck, C. Relapse in Class II Orthognathic Surgery: A Systematic Review. BMC Oral Health 2022, 22, 605. [Google Scholar] [CrossRef]
- Quast, A.; Santander, P.; Leding, J.; Klenke, D.; Moser, N.; Schliephake, H.; Meyer-Marcotty, P. Orthodontic Incisor Decompensation in Orthognathic Therapy—Success and Efficiency in Three Dimensions. Clin. Oral Investig. 2021, 25, 4001–4010. [Google Scholar] [CrossRef]
- Miao, M.Z.; Wang, B.; Wu, D.; Zhang, S.; Wong, S.; Shi, O.; Hu, A.; Mao, L.; Fang, B. Temporomandibular Joint Positional Change Accompanies Post-Surgical Mandibular Relapse—A Long-Term Retrospective Study among Patients Who Underwent Mandibular Advancement. Orthod. Craniofac Res. 2018, 21, 33–40. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Cephalometric Variables | Description |
|---|---|
| Skeletal | |
| Sagittal relationship SNA | Maxilla position in relation to the anterior portion of the skull base |
| SNB | Mandible position in relation to the anterior portion of the skull base |
| ANB SNPg | Intermaxillary basal relationship Chin position in relation to the anterior portion of the skull base |
| Vertical relationship | |
| ML–SN | Angle of the mandibular plane in relation to the anterior portion of skull base |
| ML–NL Gn-tgo-Ar | Intermaxillary angle Gonial angle |
| Dental | |
| (isa-is)–(ii-iia) (isa-is)–NA | Inter-incisal angle Inclination of the upper incisor in relation to NA |
| (iia-ii)–NB | Inclination of the lower incisor in relation to NB |
| Variables | TO | T1 | T2 | T2 − T1 | p † | padj ‡ |
|---|---|---|---|---|---|---|
| Overjet (mm) | 3.71 (5.90) | 1.68 (0.79) | 1.46 (0.83) | −0.21 (0.74) | 0.175 | 0.525 |
| −6.70/17.80 | 0.40/3.10 | 0.30/3.10 | −1.70/1.30 | |||
| Overbite(mm) | 1.47 (4.48) | 1.77 (0.59) | 1.98 (0.67) | 0.21 (0.52) | 0.070 | 0.390 |
| −14.50/7.80 | 0.50/2.90 | 1.10/3.70 | −0.60/1.20 | |||
| Upper arch depth (mm) | 27.04 (3.74) | 24.77 (4.06) | 24.50 (3.84) | −0.27 (0.95) | 0.118 | 0.443 |
| 19.80/33.50 | 19.30/31.90 | 19.50/32.40 | −2.60/2.10 | |||
| Inter-canine distance upper-lower (mm) | 6.35 (2.68) | 7.83 (2.57) | 7.69 (2.74) | −0.14 (1.77) | 0.932 | 0.932 |
| 0.20/10.60 | −2.50/10.40 | −0.90/11.20 | −5.80/3.20 | |||
| Inter-molar distance Upper-lower (mm) | 6.27 (8.99) | 7.16 (8.56) | 6.55 (9.25) | −0.61 (1.68) | 0.053 | 0.390 |
| −3.90/45.80 | −1.80/44.90 | −7.00/45.90 | −7.10/2.20 | |||
| (isa-is)–(ii-iia) (°) | 26.42 (14.68) | 127.78 (7.03) | 127.22 (6.40) | −0.56 (4.40) | 0.840 | 0.932 |
| 102.60/160.00 | 115.70/142.70 | 116.20/138.50 | −10.40/5.60 | |||
| (isa-is)–NA (°) | 25.86 (9.12) | 22.71 (8.46) | 23.27 (8.72) | 0.56 (3.23) | 0.493 | 0.740 |
| 5.70/42.80 | 7.70/39.60 | 9.40/37.60 | −6.10/7.60 | |||
| (isa-is)–NB (°) | 26.42 (8.15) | 26.60 (6.37) | 26.87 (6.51) | 0.28 (3.11) | 0.778 | 0.932 |
| 7.40/42.00 | 14.70/36.90 | 14.50/38.70 | −5.60/6.60 | |||
| SNA (°) | 80.75 (4.81) | 83.06 (4.61) | 82.68 (4.27) | −0.39 (1.13) | 0.078 | 0.390 |
| 72.00/88.70 | 74.60/94.80 | 76.30/92.80 | −2.00/2.10 | |||
| SNB (°) | 79.30 (8.07) | 77.55 (15.29) | 80.10 (5.50) | 2.54 (14.10) | 0.399 | 0.665 |
| 63.20/95.10 | 9.20/96.60 | 70.20/95.60 | −2.80/69.90 | |||
| ANB (°) | 1.44 (6.57) | 2.72 (3.72) | 2.54 (3.23) | −0.19 (1.00) | 0.377 | 0.665 |
| −8.00/12.40 | −3.00/9.80 | −2.80/9.80 | −2.80/1.80 | |||
| SNPg (°) | 79.82 (8.18) | 81.36 (5.76) | 81.13 (5.78) | −0.23 (1.26) | 0.211 | 0.528 |
| 63.00/94.50 | 70.50/97.60 | 70.30/96.40 | −3.00/2.70 | |||
| ML–NSL (°) | 38.29 (8.09) | 37.44 (6.31) | 37.59 (6.49) | 0.15 (1.79) | 0.891 | 0.932 |
| 18.00/58.90 | 27.30/55.80 | 26.60/57.90 | −3.20/3.90 | |||
| ML–NL (°) | 24.91 (8.34) | 23.35 (6.81) | 24.40 (6.48) | 1.05 (4.24) | 0.319 | 0.665 |
| 10.00/46.80 | 9.10/34.10 | 10.20/39.50 | −6.10/13.60 | |||
| Gn-tgo-Ar (°) | 131.72 (6.53) | 130.68 (6.31) | 131.28 (6.69) | 0.61 (4.72) | 0.840 | 0.932 |
| 115.00/145.00 | 114.50/143.60 | 121.00/153.90 | −5.20/14.80 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matos, J.; Travassos, R.; Caramelo, F.; Ribeiro, M.P.; Marques, F.; Marto, C.M.; Paula, A.B.; Nunes, C.; Francisco, I.; Vale, F. Relapse after Orthodontic-Surgical Treatment: A Retrospective Longitudinal Study. Symmetry 2023, 15, 1083. https://doi.org/10.3390/sym15051083
Matos J, Travassos R, Caramelo F, Ribeiro MP, Marques F, Marto CM, Paula AB, Nunes C, Francisco I, Vale F. Relapse after Orthodontic-Surgical Treatment: A Retrospective Longitudinal Study. Symmetry. 2023; 15(5):1083. https://doi.org/10.3390/sym15051083
Chicago/Turabian StyleMatos, João, Raquel Travassos, Francisco Caramelo, Madalena Prata Ribeiro, Filipa Marques, Carlos Miguel Marto, Anabela Baptista Paula, Catarina Nunes, Inês Francisco, and Francisco Vale. 2023. "Relapse after Orthodontic-Surgical Treatment: A Retrospective Longitudinal Study" Symmetry 15, no. 5: 1083. https://doi.org/10.3390/sym15051083