
Cancer Therapy Assessment Accounting for Heterogeneity Using q-Rung Picture Fuzzy Dynamic Aggregation Approach



Abstract
:1. Introduction
Literature Review
2. Heterogeneity of Cancer Cells
2.1. Theory of Cancer Stem Cells and Differentiated Cancer Cells
2.2. Hypothesis: CSCs Are Responsible for Tumor Growth
3. Mathematical Modeling
3.1. Mathematical Modeling Using Stochastic Differential Equations
- An SDE model without treatment.
- An SDE model with chemotherapy.
- An SDDE model with chemotherapy and radiotherapy with delay.
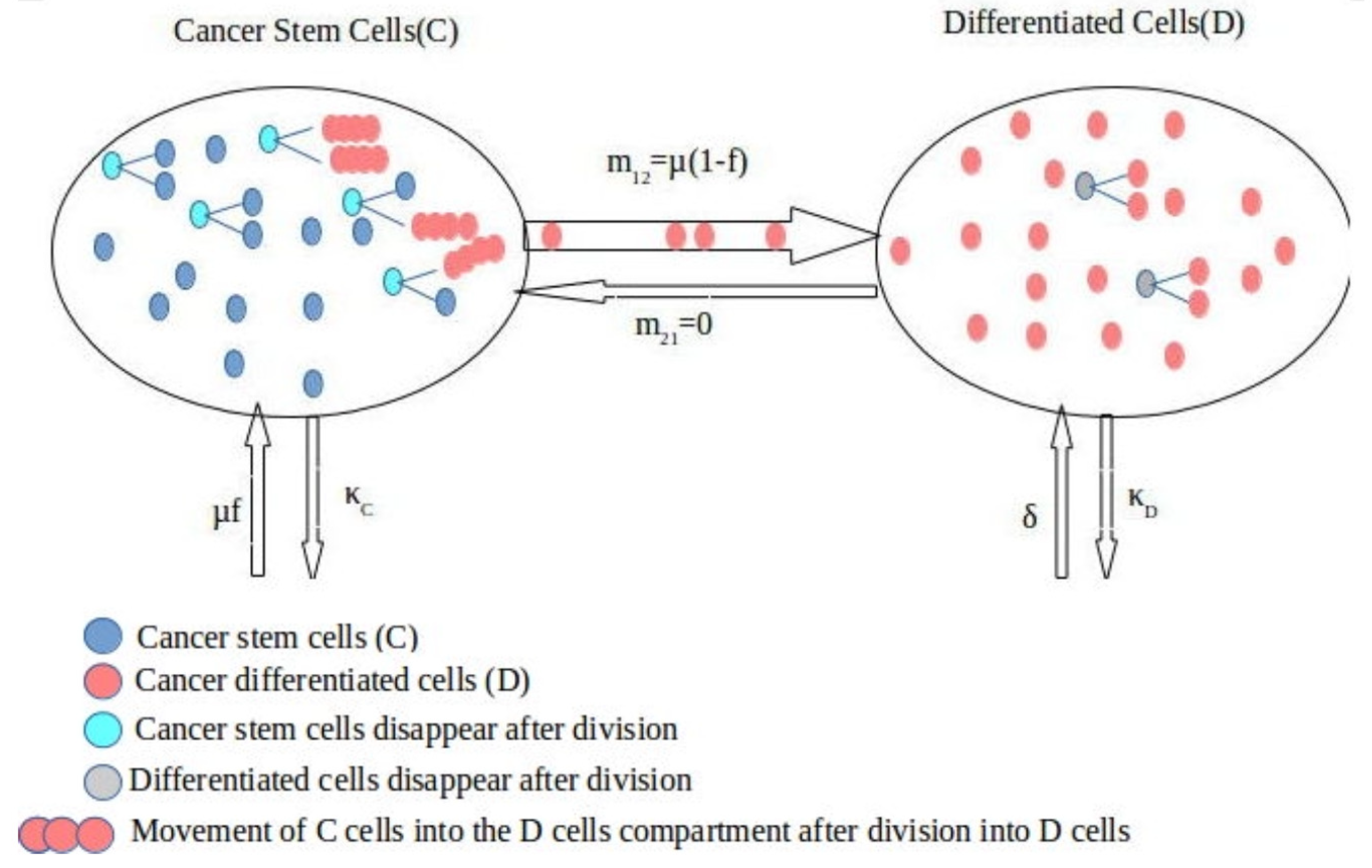
An SDE Model for Interaction between Cancer Stem Cells (C) and Differentiated Cells (D)
4. Preliminaries
- (i)
- (ii)
- (iii)
- (iv)
- (v)
- (vi)
- (vii)
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
5. q-Rung Picture Fuzzy Dynamic Einstein AOs
5.1. q-Rung Picture Fuzzy Dynamic Einstein-Weighted Averaging Operator
5.2. q-Rung Picture Fuzzy Dynamic Einstein-Weighted Geometric Operator
6. MCDM Method with Proposed AOs
| Algorithm 1 (MCDM Method) |
| Step 1: Obtain the decision matrices for the d different periods. |
| Step 2: Two kinds of criterion are discussed in the decision matrix: cost type indicators and benefit type indicators. There is no need for normalization if all indicators are of the same kind, but in MCDM, there may be two types of criteria. The matrix was updated to the transforming response matrix in this case using the normalization formula Equation (13). |
| Step 3: In this phase, we used one of the proposed AOs to aggregate all the normalized decision matrices into one cumulative q-RPF matrix . |
| Step 4: Define and as the q-RPF positive ideal solution (q-RPFPIS) and the q-RPF negative ideal solution (q-RPFNIS), respectively, where are the m largest q-RPFNs and are the m smallest q-RPFNs. Furthermore, we denote the alternatives by |
| Step 5: Calculate the distance between the alternative and the q-RPFPIS and the distance between the alternative and the q-RPFNIS respectively: |
| Step 6: Calculate the closeness coefficient of each alternative: |
| Step 7: Rank all the alternatives according to the closeness coefficients : the greater value , the better alternative . |
7. Case Study
- Moving to other areas of the body via the lymphatic system and bloodstream;
- Causing new blood vessels to grow, which creates blood delivery to the metastatic tumor that enables it to continue developing; the circulatory (blood) system is involved (hematogenous);
- Spreading into or infiltrating normal nearby tissue;
- Growing in this tissue until a tiny tumor forms;
- Stopping in small blood vessels farther away, invading the blood vessel walls, and proceeding into the surrounding tissue;
- Passing through the lymph glands or capillaries in the region.It is very much clear that cancer spreads due to the malignancy of the cells and it spreads as the malignancy travels into other cells. In the next section, we will start explaining different cancer treatments followed by the description of our technique to model the spread of cancer and our treatment strategy.
7.1. Different Treatment Strategies of Cancer
- (i)
- Curing cancer, which means that it is no longer present. It can take years to find out whether a person’s cancer has been cured.
- (ii)
- If a cure is unattainable, the goal may be to control the condition, such as shrinking the tumor or stopping the cancer from developing and spreading, or a combination of the two. This can improve the patient’s quality of life and help them live longer. In many situations, the cancer does not go away completely, but it is managed and controlled as a chronic disease, similarly to heart disease or diabetes. In other circumstances, the cancer may appear to have gone away for a time, but it may return.
- (iii)
- Chemotherapy medications may be used if the cancer has progressed to an advanced stage.
7.2. Chemotherapy
Cytotoxic and Cytostatic Agents
7.3. Radiotherapy and Common Radiobiological Models
7.3.1. Nominal Standard Dose (NSD)
7.3.2. Cumulative Radiation Effect (CRE)
7.3.3. Target Models
7.3.4. Linear Quadratic (LQ) Model
7.3.5. The LQ Model and Recolonization
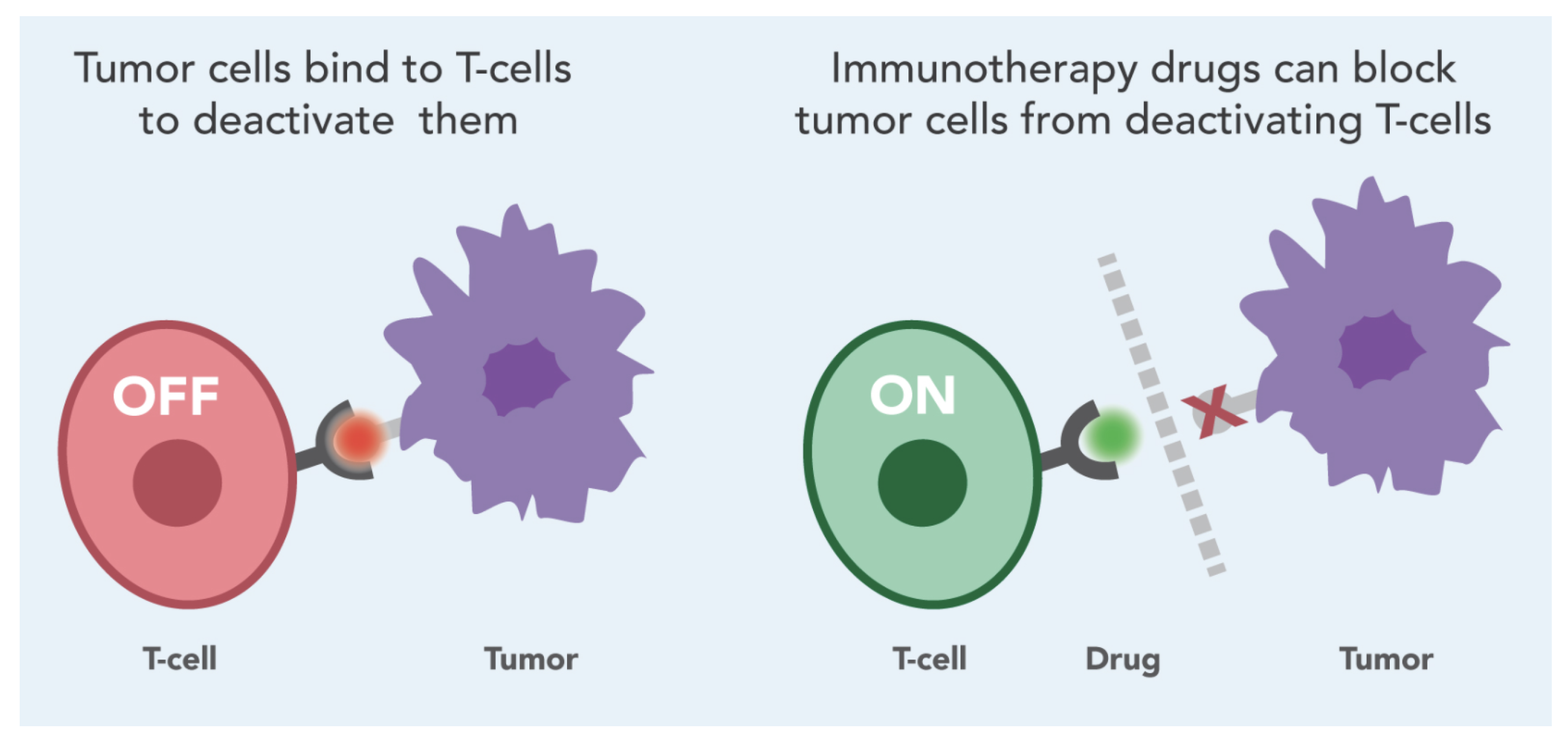
7.4. Immunotherapy
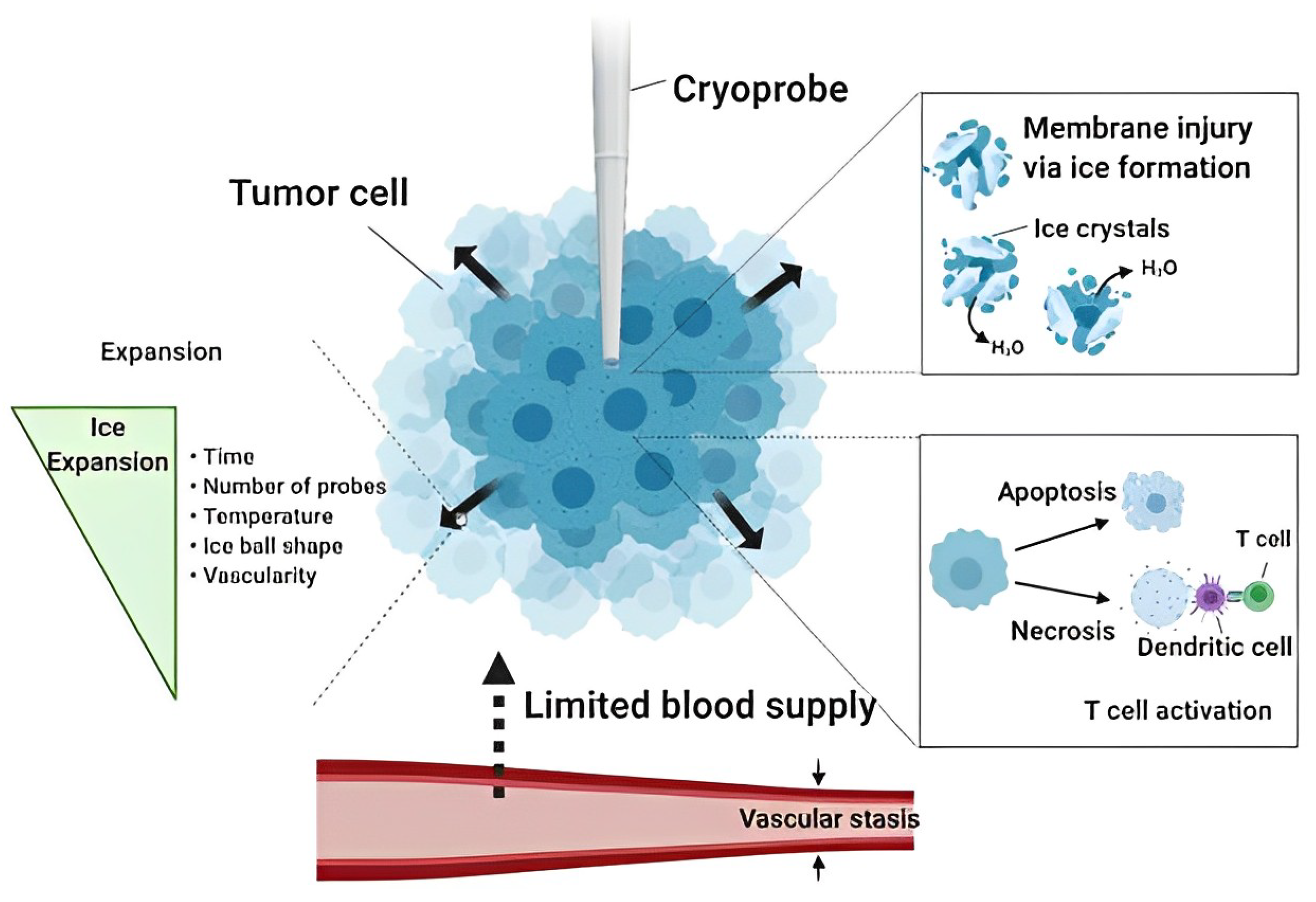
7.5. Cryoablation
7.6. Proposed Strategy
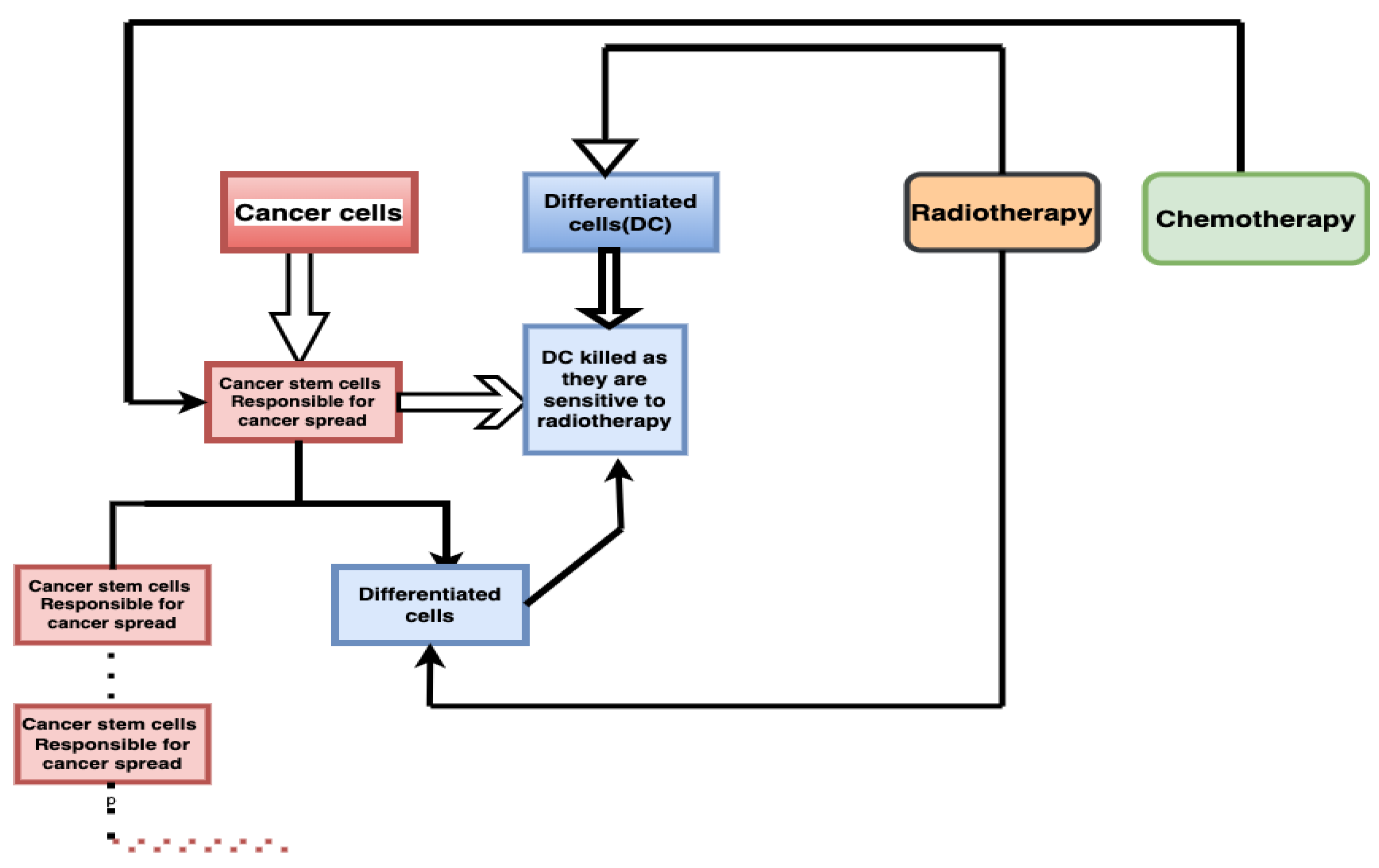
7.6.1. Treatment without Considering Heterogeneity of Cancer Cells
| Algorithm 2 (Treatment without considering Heterogeneity of Cancer Cells) |
| Step 1: First, the total cancer cells are considered. They are of two types: cancer stem cells (CSCs) and differentiated cells (DCs). Total cancer cells are: CSCs + DCs |
|
Step 2: Apply treatment of radio therapy on both CSCs and DCs. As DCs are sensitive to radiotherapy, they will be killed: CSC are resistant to radiotherapy and responsible for cancer cells. |
|
Step 3: CSCs will further continue to spread and divide into CSCs and DCs. This spread will continue. |
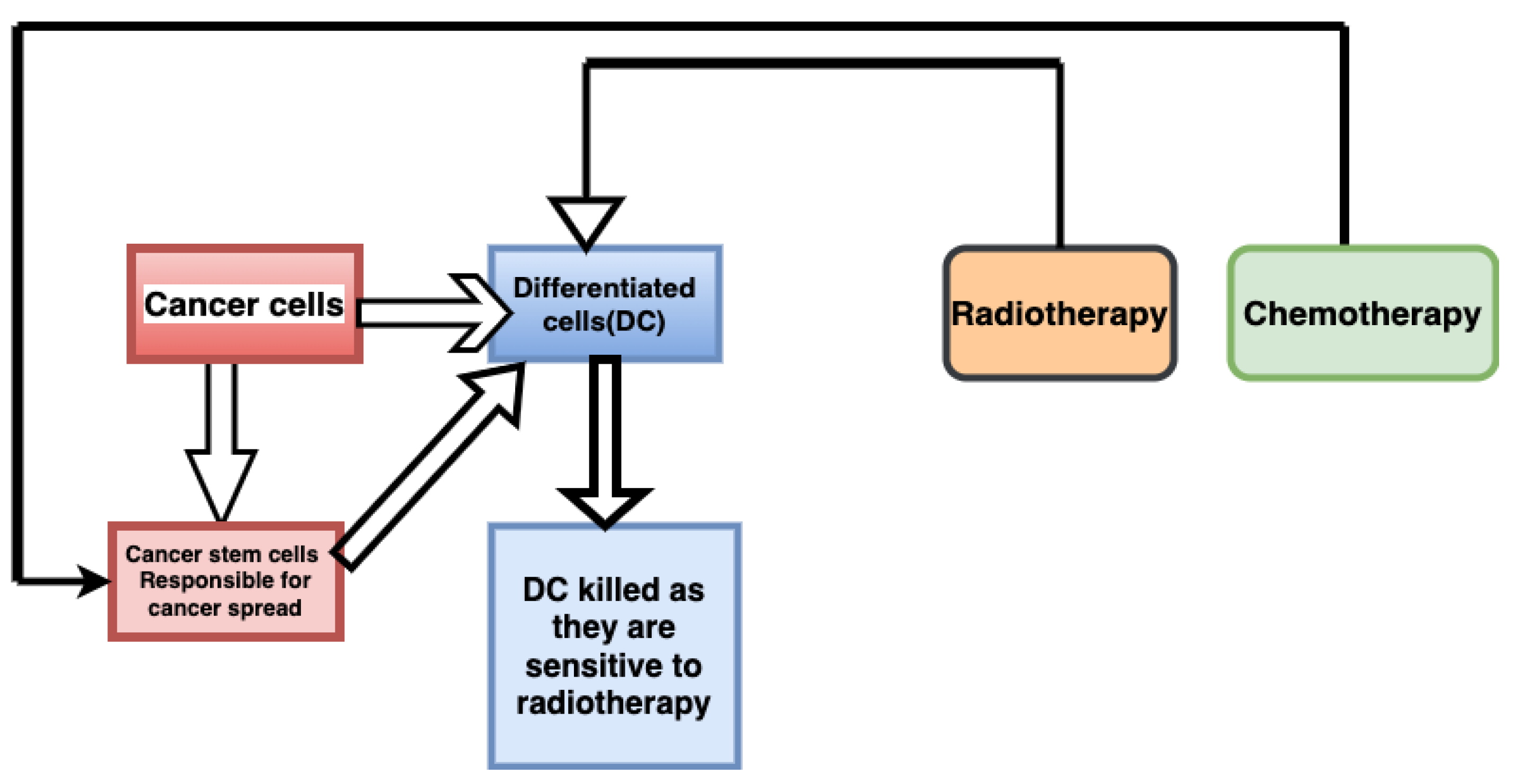
7.6.2. Suggested Treatment Strategy Accounting for Heterogeneity of Cells
| Algorithm 3 (Cancer treatment strategy accounting for Heterogeneity) |
| Step 1: First the total cancer cell are considered. They are of two types: cancer stem cells (CSCs) and differentiated cells (DCs). Total cancer cells are: CSCs + DCs |
| Step 2: First apply chemotherapy; this will convert CSCs into DCs. Meaning that it will convert radiotherapy-resistant cells (CSCs) into radiotherapy-sensitive cells (DCs). |
| Step 3: Now apply radiotherapy and maximum cells will be killed as chemotherapy application makes the process of conversion of CSC into DC fast enough. |

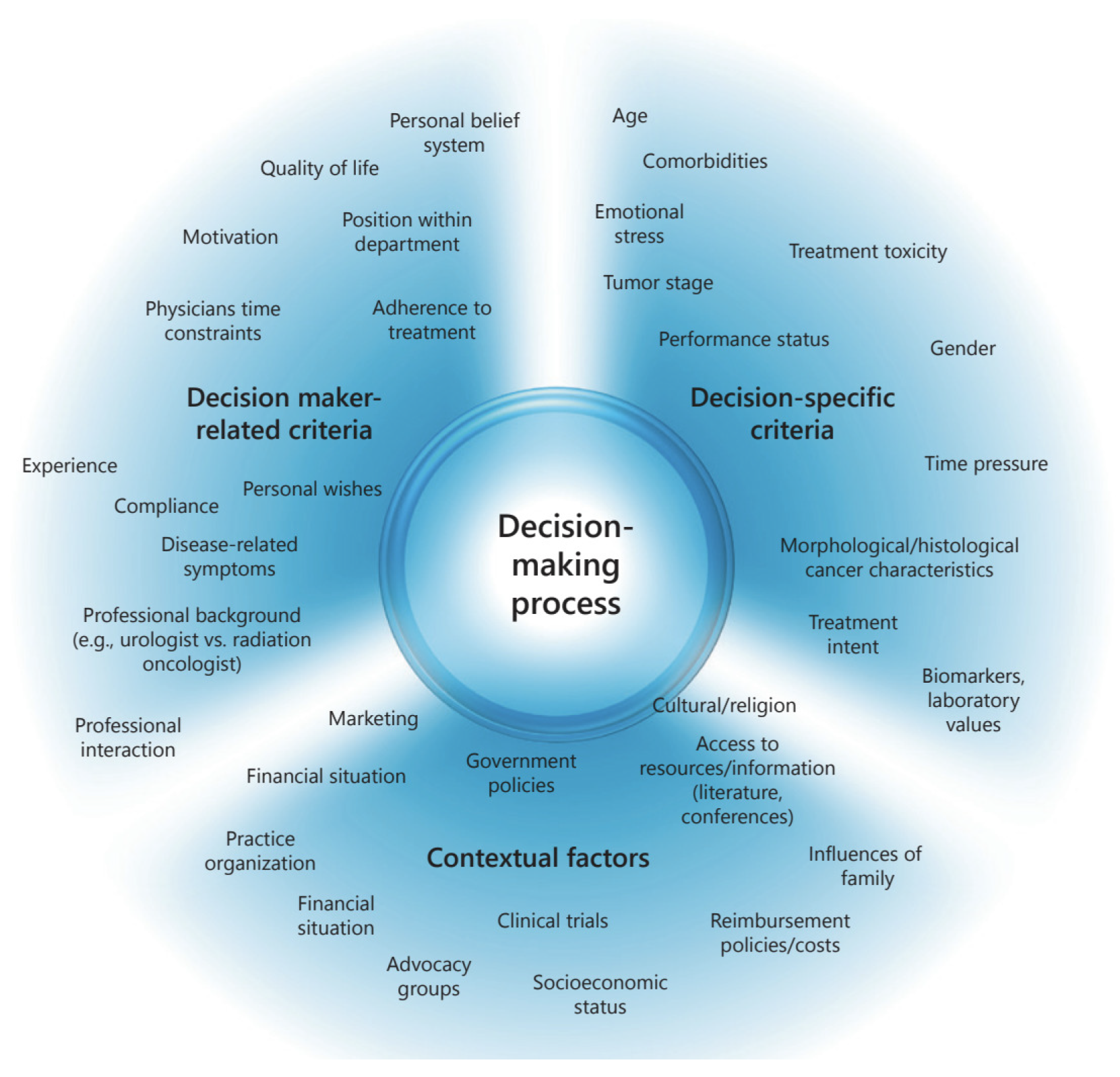
7.7. Decision-Making Criteria in Oncology
- (1)
- In oncology, age is a main criteria in choosing the treatment for cancer. The treatment choice changes with the age of the patient. For example, radiation therapy is highly related to age [69]. Patients over 65 years of age may not tolerate all treatments as well as their younger counterparts.
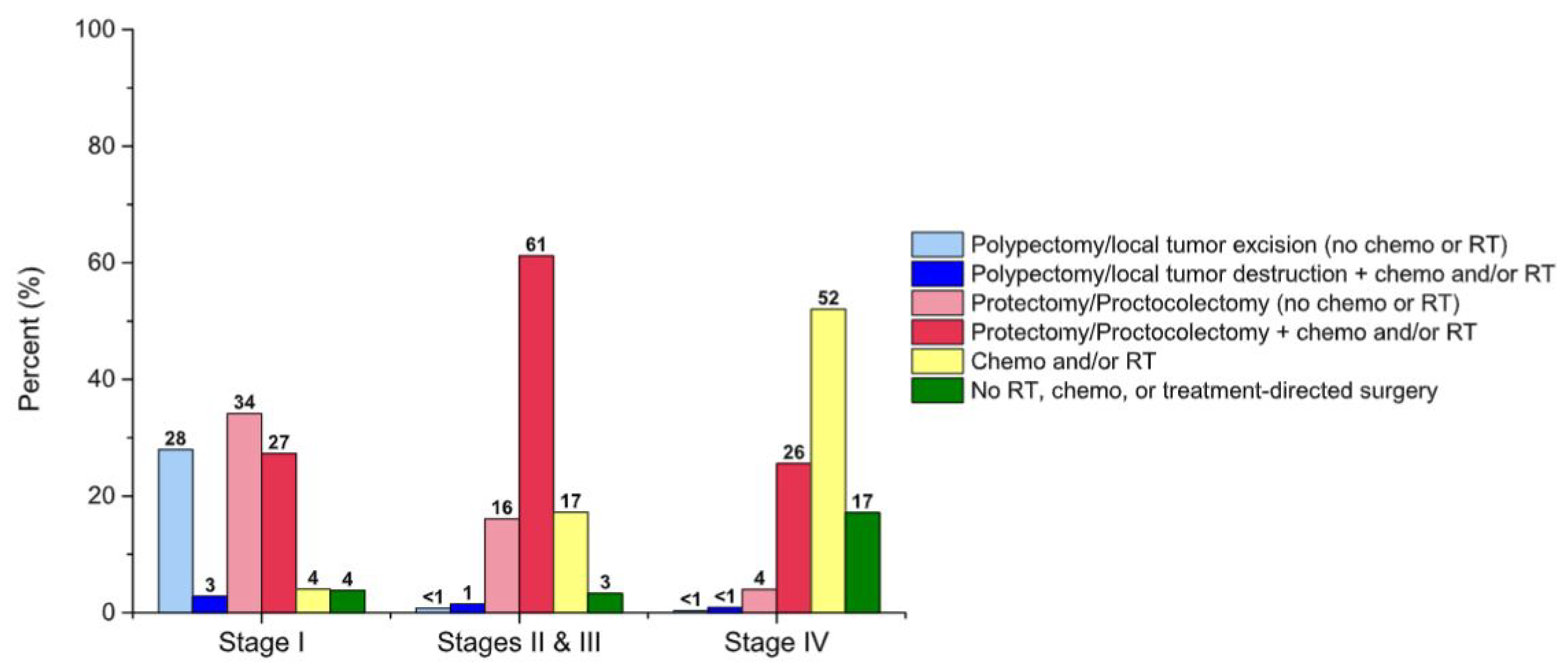
- (2)
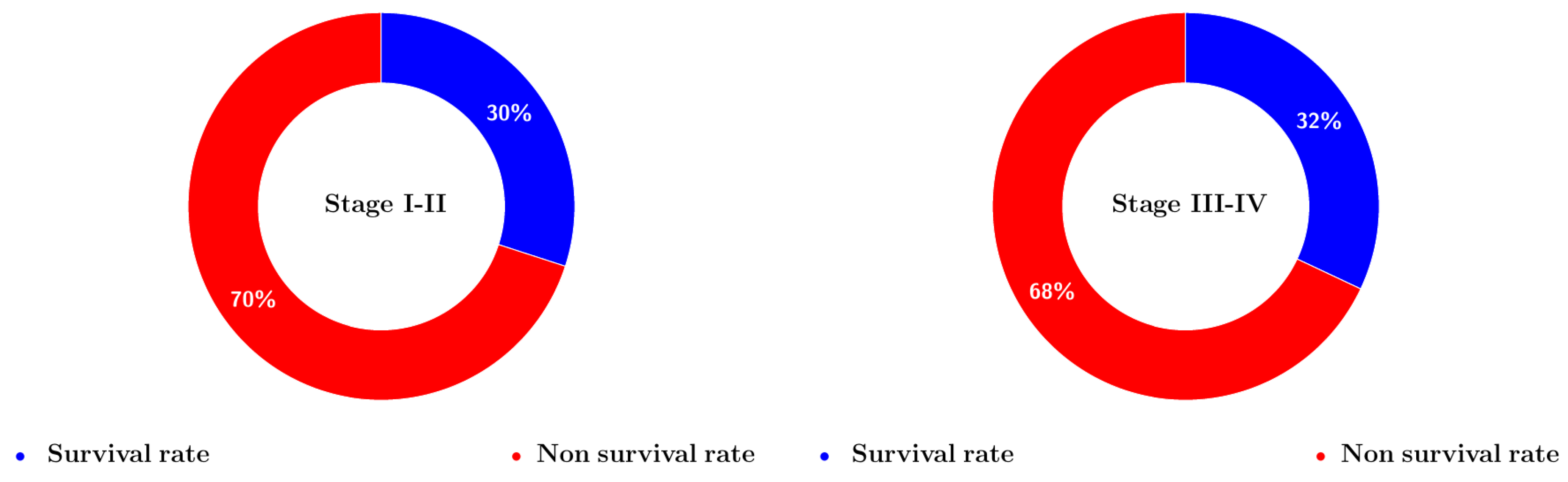
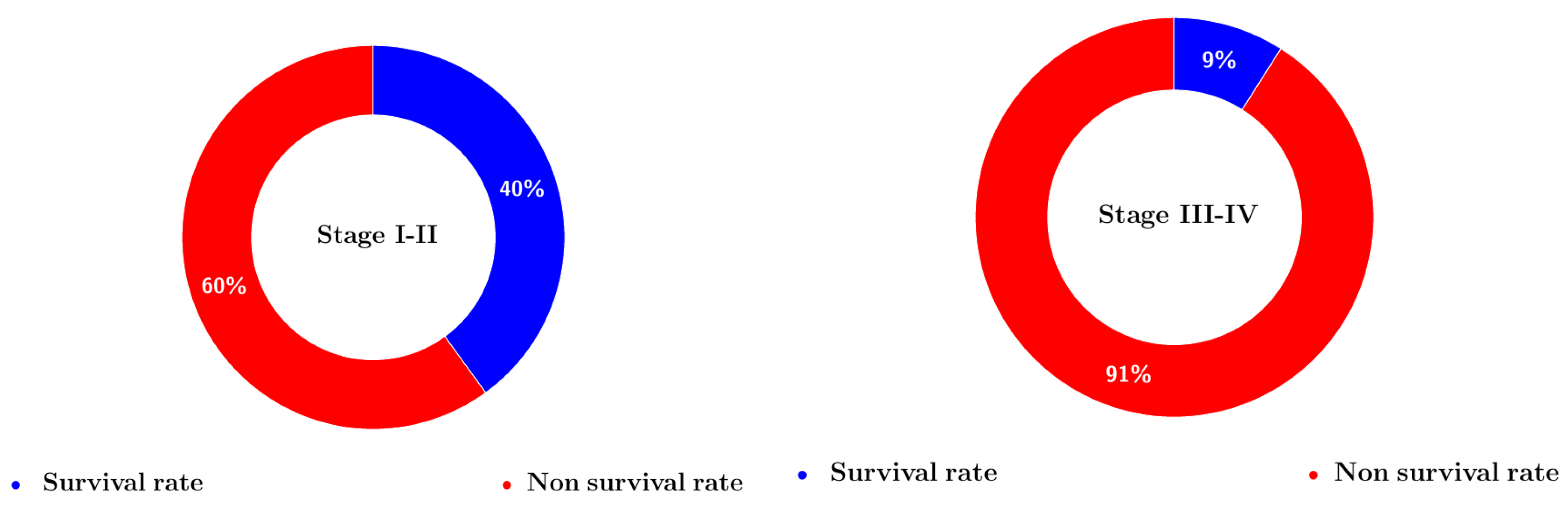
- The cancer entity and stage are key factors to consider throughout the decision-making process. Treatment is mostly determined by the stage and extent of the cancer. The treatment guidelines for regionally based tumors differ from those for advanced sickness or metastasized tumors. The Figure 11 shows the relationship between stage of cancer and survival with respect to the choice of treatment [70].
- (3)
- The choice between prioritizing the quantity or quality of life will influence the decision of whether or not to treat, the degree of data available to support the option, and perhaps the level of adverse effects the patient is prepared to risk. The purpose of a technique determines the selection of decision criteria [71,72].
- (4)
- Cost is also an important factor when choosing cancer treatments. The resources of every individual are limited, and since saving a life is someone’s top priority, it is important to choose a life-saving treatment strategy considering the limited resources.
- (5)
- Long-term side effects are also an important factor to consider when choosing cancer treatment strategy.
7.8. Decision-Making Process
7.9. Limitations of the Proposed Method
- Logical dependencies amongst the parameters were ignored in the preceding instances.
- In practice, it is not generally fair to suggest that each parameter in the MPDM is independent of the others. Any parameter in the MPDM may be reliant on or connected to other parameters.
- Evaluation of parameter dependencies should add to the objectivity of judgments in the suggested MPDM techniques. The consideration of dependence in the q-RPF MPDM may increase the decision-making framework’s quality.
7.10. Authenticity Analysis
- Test 1: If we replace the non-optimal alternate’s grade values with those of the worst choice, the ideal option should not change as long as the respective priority relationship remains unchanged.
- Test 2: The approach’s framework should be transitive.
- Test 3: Whenever a continuous dilemma is partitioned and the same MCDM algorithm is used, the accumulated rating of the alternatives must be comparable to the initial problem’s evaluation.
7.10.1. Authenticity Test 1
7.10.2. Authenticity Test 2 and Test 3
8. Conclusions and Discussion
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Appendix A
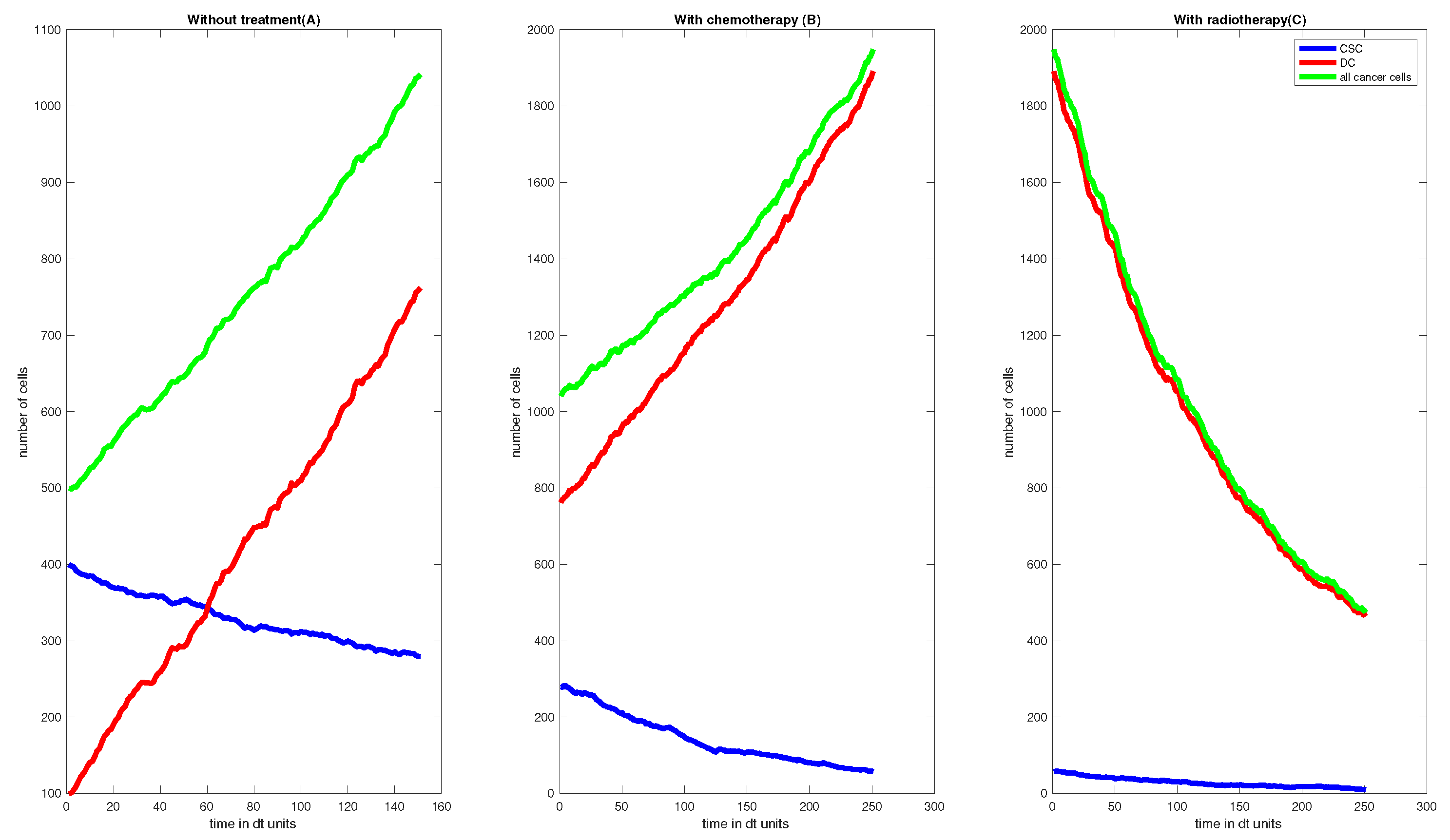
| Listing A1. Matlab code for the Figure 9. |
| 1 %clear all 2 clc 3 %First, do no treatment for X ticks 4 %Second, only chemotherapy for Y ticks 5 %Third, radiotherapy for Z ticks 6 % OBS, we do not do chemo- and radiotherapy together. Should we? 7 % C, number of of CSC (cancer stem cells) 8 % D, number of of DC (Differentiated cells) 9 counter=0; 10 counter1=0; 11 % Parameters 12 % Ratios 13 % dc_ratio = 3; % gamma/beta 14 %f, fraction with which CSC split into DC 15 %sigma, death rate of CSC, by chemo- and radiotherapy (radio very very 16 %small) 17 %gamma, death rate of DC, natural death and by chemo- and radiotherapy 18 % gamma = 0.7; % w/ treatment (both radio and chemo) 19 %beta, birth rate of DC 20 beta = 0.4; %from pdf 21 mu = 0.5; % what should this be????? 22 %%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%% 23 T_end = 10; 24 25 X = 100; %ticks without treatment 26 Y = 200; %ticks with chemotherapy 27 Z = 200; %ticks with radiotherapy 28 29 dt = T_end/(X+Y+Z); 30 31 C = zeros(X+Y+Z+1,1); % steam cancer 32 C(1) = 400; 33 D = zeros(X+Y+Z+1,1); 34 D(1) = 100; 35 cancer = zeros(X+Y+Z+1,1); 36 cancer(1) = C(1)+D(1); 37 38 39 N= zeros(X+Y+Z+1,1); % Normal cells initialization vector 40 dr=0.0003; 41 N(1)=2000; % Normal cell value at t=0 42 lambda1=0.2;%0.04 43 lambda2=0.003; 44 C_s=1500; % C_star 45 N_c=10000; % Normal cells carrying capacity 46 C_c=50000; % Cancer cells carrying capacity 47 48 49 %%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%% 50 %%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%%% 51 % Values for chemo 52 53 d = 10; % number of dose 54 alpha_ch =0.5; % alpha for cancer cells, increase sensitivity gives …complex values 55 alpha1_ch=0.3; % alpha for normal cells 56 beta1_ch=alpha1_ch/1.5; % beta for normal cells 57 beta_ch = alpha_ch/3; % beta for cancer cells 58 S_ch = exp(- alpha_ch*d - beta_ch*d^2); 59 60 R_ch = 1-S_ch;%cancer cells 61 62 S1_ch = exp(- alpha1_ch*d - beta1_ch*d^2); 63 R1_ch=1-S1_ch;% Normal cells 64 % Values for radio-therapy 65 d = 10; % number of dose 66 alpha_rt =0.5; % alpha for cancer cells 67 alpha1_rt=0.3; % alpha for normal cells 68 beta1_rt=alpha1_rt/3; % beta for normal cells 69 beta_rt = alpha_rt/10; % beta for cancer cells 70 S_rt = exp(- alpha_rt*d - beta_rt*d^2); 71 R_rt = 1-S_rt;%cancer cells 72 S1_rt = exp(- alpha1_rt*d - beta1_rt*d^2); 73 R1_rt=1-S1_rt;% Normal cells 74 % Before treatment 75 gamma = 0.2; % w/o treatment 76 sigma = 0; % w/o any treatment 77 f = 0.35; % w/o treatment 78 for t=1:X 79 tau = sqrt((mu+sigma)*C(t)*(4*mu*(1-f)*C(t)+(gamma+beta)*D(t))- … 80 4*mu^2*(1-f)^2*C(t)^2); 81 eta = sqrt(2*tau + (mu+sigma)*C(t)+4*mu*(1-f)*C(t)+(gamma+beta)*D(t)); 82 dW1 = sqrt(dt)*randn; 83 dW2 = sqrt(dt)*randn; 84 a = [2*mu*f*C(t)-mu*C(t)-sigma*C(t); 2*mu*(1-f)*C(t)-gamma*D(t)+beta*D(t)]; 85 b = 1/eta * [(mu+sigma)*C(t)+tau -2*mu*(1-f)*C(t); … 86 -2*mu*(1-f)*C(t) 4*mu*(1-f)*C(t)+(gamma+beta)*D(t)+tau]; 87 A = [C(t) D(t)]’ + a*dt+ b*[dW1; dW2]; 88 C(t+1) = A(1); 89 D(t+1) = A(2); 90 cancer(t+1) = C(t+1)+D(t+1); 91 92 d1=dr*C_s*cancer(t+1); 93 d2=0; 94 b2=(1-(N(t)/N_c)-(cancer(t+1)/C_c)); 95 96 tau1 = sqrt((d1*lambda1^1^2*(d2+b2)*lambda2^2)); 97 eta1=sqrt((d1*lambda1^2)+((d2+b2)*lambda2^2)+(2*tau1)); 98 99 a1= [-lambda1*d1; lambda2*(b2-d2)]; 100 b1= (1/eta1)*[(d1*lambda1^2)+tau1 0; 0 ((d2+b2)*lambda2^2)+tau1]; 101 A1= [N(t) cancer(t+1)]’ + a1*dt+b1*[dW1; dW2]; 102 N(t+1)=A1(1); 103 cancer(t+1) = A1(2); 104 105 if cancer(t+1)≥2*cancer(1)&& counter==0 106 time_double= t; 107 counter=1; 108 sprintf(‘The doubling time is %d ticks’,time_double) 109 end 110 111 end 112 figure() 113 subplot(131) 114 plot(1:X+1,N(1:X+1),‘-k’);hold on 115 plot(1:X+1,C(1:X+1),‘-b’); 116 plot(1:X+1,D(1:X+1),‘-r’) 117 plot(1:X+1,cancer(1:X+1),‘-g’) 118 % legend(’N’,’CSC’,’DC’, ’all cancer cells’) 119 title(‘Without treatment’) 120 xlabel(‘time in dt units’) 121 ylabel(‘number of cells’) 122 pause(1.5) 123 124 125 %---------------------------------------------------------------------- 126 % With chemotherapy 127 f = 0.6; % w/ chemo (radio same?) % f---rate of conversion of c to d (more…f) (as per simulation results as the f increases the rate of…conversion and total number falls down ) 128 %gamma hardly changes 129 sigma = 0.5; % w/ chemo (and radio) chemo effect on cancer cell 130 % sigma1 ---> add chemo on normanl 0.0001 131 % sigma1=0.0001; 132 N_d=1; % no. of integer delays 133 t_d=N_d; %delay 134 for t=1:Y 135 tau = sqrt((mu+sigma)*C(X+t-t_d)*(4*mu*(1-f)*C(X+t-t_d) 136 +(gamma+beta)*D(X+t-t_d))-4*mu^2*(1-f)^2*C(X+t-t_d)^2); 137 eta = sqrt(2*tau + … (mu+sigma)*C(X+t-t_d)+4*mu*(1-f)*C(X+t-t_d)+(gamma+beta)*D(X+t-t_d)); 138 a = [2*mu*f*C(X+t-t_d)-mu*C(X+t-t_d)-sigma*C(X+t-t_d); … 2*mu*(1-f)*C(X+t-t_d)- 139 gamma*D(X+t-t_d)+beta*D(X+t-t_d)]; 140 b = 1/eta * [(mu+sigma)*C(X+t-t_d)+tau -2*mu*(1-f)*C(X+t-t_d); … 141 -2*mu*(1-f)*C(X+t-t_d) … 4*mu*(1-f)*C(X+t-t_d)+(gamma+beta)*D(X+t-t_d)+tau]; 142 dW1 = sqrt(dt)*randn; 143 dW2 = sqrt(dt)*randn; 144 A = [C(X+t) D(X+t)]’ + dt*a+ b*[dW1; dW2]; 145 C(X+t+1) = A(1); 146 D(X+t+1) = A(2); 147 cancer(X+t+1) = C(X+t+1)+D(X+t+1); 148 149 d1=dr*C_s*cancer(X+t+1)+R1_ch; 150 d2=-R_ch*cancer(X+t+1); 151 b2=(1-(N(X+t)/N_c)-(cancer(X+t+1)/C_c)); 152 tau1 = sqrt((d1*lambda1^1^2*(d2+b2)*lambda2^2)); 153 eta1=sqrt((d1*lambda1^2)+((d2+b2)*lambda2^2)+(2*tau1)); 154 155 a1= [-lambda1*d1; lambda2*(b2-d2)]; 156 b1= (1/eta1)*[(d1*lambda1^2)+tau1 0; 0 ((d2+b2)*lambda2^2)+tau1]; 157 A1= [N(X+t) cancer(X+t+1)]’ + a1*dt+b1*[dW1; dW2]; 158 N(X+t+1)=A1(1); 159 cancer(X+t+1) = A1(2); 160 161 if cancer(X+t+1)≥2*cancer(1)&& counter==0 162 time_double= t; 163 counter=1; 164 sprintf(‘The doubling time is %d ticks’,time_double) 165 end 166 end 167 168 % figure() 169 subplot(132) 170 plot(1:Y+1,N(X+1:X+Y+1),‘-k’);hold on 171 plot(1:Y+1,C(X+1:X+Y+1),‘-b’) 172 plot(1:Y+1,D(X+1:X+Y+1),‘-r’) 173 plot(1:Y+1,cancer(X+1:X+Y+1),‘-g’) 174 % legend(’N’,’CSC’,’DC’, ’all cancer cells’) 175 title(‘With chemotherapy’) 176 xlabel(‘time in dt units’) 177 ylabel(‘number of cells’) 178 pause(1.5) 179 % With radiotherapy 180 % f = 0.3; % w/ chemo (radio same?) 181 %Y=0; 182 gamma = 0.8; 183 % sigma = 0.5; % w/ chemo (and radio) 184 185 for t=1:Z 186 tau=sqrt((mu+sigma)*C(X+Y+t)*(4*mu*(1-f)*C(X+Y+t)+(gamma+beta)*D(X+Y+t))- 187 4*mu^2*(1-f)^2*C(X+Y+t)^2); 188 eta = sqrt(2*tau + (mu+sigma)*C(X+Y+t)+4*mu*(1-f)*C(X+Y+t)+(gamma+beta)*D(X+Y+t)); 189 a = [2*mu*f*C(X+Y+t)-mu*C(X+Y+t)-sigma*C(X+Y+t); 2*mu*(1-f)*C(X+Y+t) 190 -gamma*D(X+Y+t)+beta*D(X+Y+t)]; 191 b = 1/eta * [(mu+sigma)*C(X+Y+t)+tau -2*mu*(1-f)*C(X+Y+t); … 192 -2*mu*(1-f)*C(X+Y+t) 4*mu*(1-f)*C(X+Y+t)+(gamma+beta)*D(X+Y+t)+tau]; 193 dW1 = sqrt(dt)*randn; 194 dW2 = sqrt(dt)*randn; 195 A = [C(X+Y+t) D(X+Y+t)]’ + dt*a+ b*[dW1; dW2]; 196 C(X+Y+t+1) = A(1); 197 D(X+Y+t+1) = A(2); 198 cancer(X+Y+t+1) = C(X+Y+t+1)+D(X+Y+t+1); 199 d1=dr*C_s*cancer(X+Y+t+1)+R1_rt; 200 d2=-R_rt*cancer(X+Y+t+1); 201 b2=(1-(N(X+Y+t)/N_c)-(cancer(X+Y+t+1)/C_c)); 202 tau1 = sqrt((d1*lambda1^1^2*(d2+b2)*lambda2^2)); 203 eta1=sqrt((d1*lambda1^2)+((d2+b2)*lambda2^2)+(2*tau1)); 204 205 a1= [-lambda1*d1; lambda2*(b2-d2)]; 206 b1= (1/eta1)*[(d1*lambda1^2)+tau1 0; 0 ((d2+b2)*lambda2^2)+tau1]; 207 A1= [N(X+Y+t) cancer(X+Y+t+1)]’ + a1*dt+b1*[dW1; dW2]; 208 N(X+Y+t+1)=A1(1); 209 cancer(X+Y+t+1) = A1(2); 210 211 if cancer(X+Y+t+1)≥2*cancer(1)&& counter==0 212 time_double= t; 213 counter=1; 214 sprintf(‘The doubling time is %d ticks’,time_double) 215 end 216 217 if cancer(X+Y+t+1)≤ 900 && counter1==0 218 time_exit= t; 219 counter1=1; 220 hold on 221 sprintf(‘The exit time is %d ticks’,time_exit) 222 end 223 224 end 225 226 % figure() 227 subplot(133) 228 plot(1:Z+1,N(X+Y+1:X+Y+Z+1),‘-k’);hold on 229 plot(1:Z+1,C(X+Y+1:X+Y+Z+1),‘-b’); 230 plot(1:Z+1,D(X+Y+1:X+Y+Z+1),‘-r’); 231 plot(1:Z+1,cancer(X+Y+1:X+Y+Z+1),‘-g’); 232 legend(‘N’,‘CSC’,‘DC’, ‘all cancer cells’); 233 xlabel(‘time in dt units’) 234 ylabel(‘number of cells’) 235 title(‘With radiotherapy’) |
References
- Fedorov, A.; Clunie, D.; Ulrich, E.; Bauer, C.; Wahle, A.; Brown, B.B. DICOM for quantitative imaging biomarker development: A standards based approach to sharing clinical data and structured PET/CT analysis results in head and neck cancer research. PeerJ 2016, 4, e2057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sheergojri, A.R.; Iqbal, P.; Agarwal, P.; Ozdemir, N. Uncertainty-based Gompertz growth model for tumor population and its numerical analysis. Int. J. Optim. Control Theor. Appl. IJOCTA 2022, 12, 137–150. [Google Scholar] [CrossRef]
- Nopour, R.; Shanbehzadeh, M.; Kazemi-Arpanahi, H. Developing a clinical decision support system based on the fuzzy logic and decision tree to predict colorectal cancer. Med. J. Islam. Repub. Iran 2021, 35, 44. [Google Scholar] [CrossRef] [PubMed]
- Balis, F.M. The goal of cancer treatment. Oncologist 1998, 3. [Google Scholar] [CrossRef] [Green Version]
- Zadeh, L.A. Fuzzy sets. Inf. Control 1965, 8, 338–353. [Google Scholar] [CrossRef] [Green Version]
- Atanassov, K.T. Intuitionistic fuzzy sets. Fuzzy Sets Syst. 1986, 20, 87–96. [Google Scholar] [CrossRef]
- Cuong, B.C.; Kreinovich, V. Picture fuzzy sets—A new concept for computational intelligence problems. In Proceedings of the 2013 Third World Congress on Information and Communication Technologies (WICT 2013), Hanoi, Vietnam, 15–18 December 2013; IEEE: Hanoi, Vietnam, 2013; pp. 1–6. [Google Scholar]
- Cuong, B.C. Picture fuzzy sets. J. Comput. Sci. Technol. 2014, 30, 409–420. [Google Scholar]
- Wei, G.; Alsaadi, F.E.; Hayat, T.; Alsaedi, A. Projection models for multiple attribute decision making with picture fuzzy information. Int. J. Mach. Learn. Cybern. 2018, 9, 713–719. [Google Scholar] [CrossRef]
- Wei, G.; Gao, H. The generalized Dice similarity measures for picture fuzzy sets and their applications. Informatica 2018, 29, 107–124. [Google Scholar] [CrossRef] [Green Version]
- Wei, G. Some similarity measures for picture fuzzy sets and their applications. Iran. J. Fuzzy Syst. 2018, 15, 77–89. [Google Scholar]
- Cuong, H.B.C.; Pham, V.H. Some fuzzy logic operators for picture fuzzy sets. In Proceedings of the Seventh International Conference on Knowledge and Systems Engineering, Yokohama, Japan, 10–12 June 2015; pp. 132–137. [Google Scholar]
- Phong, P.H.; Hieu, D.T.; Ngan, R.T.H.; Them, P.T. Some compositions of picture fuzzy relations. In Proceedings of the 7th National Conference on Fundamental and Applied Information Technology Research, FAIR’7, Thai Nguyen, Vietnam, 19–20 June 2014; pp. 19–20. [Google Scholar]
- Riaz, M.; Hashmi, M.R.; Pamucar, D.; Chu, Y.M. Spherical linear Diophantine fuzzy sets with modeling uncertainties in MCDM. Comput. Model. Eng. Sci. 2021, 126, 1125–1164. [Google Scholar] [CrossRef]
- Wang, R.; Wang, J.; Gao, H.; Wei, G. Methods for MADM with picture fuzzy muirhead mean operators and their application for evaluating the financial investment risk. Symmetry 2018, 11, 6. [Google Scholar] [CrossRef]
- Garg, H. Some picture fuzzy aggregation operators and their applications to multicriteria decision-making. Arab. J. Sci. Eng. 2017, 42, 5275–5290. [Google Scholar] [CrossRef]
- Tian, C.; Peng, J.J.; Zhang, S.; Zhang, W.Y.; Wang, J.Q. Weighted picture fuzzy aggregation operators and their applications to multi-criteria decision-making problems. Comput. Ind. Eng. 2019, 137, 106037. [Google Scholar] [CrossRef]
- Wei, G.W. Picture fuzzy hamacher aggregation operators and their application to multiple attribute decision making. Fundam. Informaticae 2018, 157, 271–320. [Google Scholar] [CrossRef]
- Jana, C.; Senapati, T.; Pal, M.; Yager, R.R. Picture fuzzy Dombi aggregation operators: Application to MADM process. Appl. Soft Comput. 2019, 74, 99–109. [Google Scholar] [CrossRef]
- Wang, L.; Zhang, H.Y.; Wang, J.Q.; Wu, G.F. Picture fuzzy multi-criteria group decision-making method to hotel building energy efficiency retrofit project selection. RAIRO-Oper. Res. 2020, 54, 211–229. [Google Scholar] [CrossRef] [Green Version]
- Riaz, M.; Farid, H.M.A. Hierarchical medical diagnosis approach for COVID-19 based on picture fuzzy fairly aggregation operators. Int. J. Biomath. 2022, 16, 2250075. [Google Scholar] [CrossRef]
- Naeem, M.; Khan, Y.; Ashraf, S.; Weera, W.; Batool, B. A novel picture fuzzy Aczel-Alsina geometric aggregation information: Application to determining the factors affecting mango crops. AIMS Math. 2022, 7, 12264–12288. [Google Scholar] [CrossRef]
- Farid, H.M.A.; Riaz, M. Some generalized q-rung orthopair fuzzy Einstein interactive geometric aggregation operators with improved operational laws. Int. J. Intell. Syst. 2021, 36, 7239–7273. [Google Scholar] [CrossRef]
- Saha, A.; Dutta, D.; Kar, S. Some new hybrid hesitant fuzzy weighted aggregation operators based on Archimedean and Dombi operations for multi-attribute decision making. Neural Comput. Appl. 2021, 33, 8753–8776. [Google Scholar] [CrossRef]
- Saha, A.; Majumder, P.; Dutta, D.; Debnath, B.K. Multi-attribute decision making using q-rung orthopair fuzzy weighted fairly aggregation operators. J. Ambient. Intell. Humaniz. Comput. 2011, 12, 8149–8171. [Google Scholar] [CrossRef]
- Akram, M.; Sattar, A.; Karaaslan, F.; Samanta, S. Extension of competition graphs under complex fuzzy environment. Complex Intell. Syst. 2021, 7, 539–558. [Google Scholar] [CrossRef]
- Karaaslan, F.; Ozlu, S. Correlation coefficients of dual type-2 hesitant fuzzy sets and their applications in clustering analysis. Int. J. Intell. Syst. 2020, 35, 1200–1229. [Google Scholar] [CrossRef]
- Alcantud, J.C.R. The relationship between fuzzy soft and soft topologies. J. Intell. Fuzzy Syst. 2022, 24, 1653–1668. [Google Scholar] [CrossRef]
- Kirişci, M.; Demir, I.; Şimşek, N. Fermatean fuzzy ELECTRE multi-criteria group decision-making and most suitable biomedical material selection. Artif. Intell. Med. 2022, 127, 102278. [Google Scholar] [CrossRef]
- Feng, F.; Fujita, H.; Ali, M.I.; Yager, R.R.; Liu, X. Another view on generalized intuitionistic fuzzy soft sets and related multiattribute decision making methods. IEEE Trans. Fuzzy Syst. 2018, 27, 474–488. [Google Scholar] [CrossRef]
- Mahmood, T.; Ullah, K.; Khan, Q.; Jan, N. An approach toward decision-making and medical diagnosis problems using the concept of spherical fuzzy sets. Neural Comput. Appl. 2019, 31, 7041–7053. [Google Scholar] [CrossRef]
- Ashraf, T.; Abdullah, S.T.; Mahmood, F.; Ghani, T.M. Spherical fuzzy sets and their applications in multi-attribute decision making problems. Int. J. Intell. Syst. 2019, 36, 2829–2844. [Google Scholar] [CrossRef]
- Gündoğdu, F.K.; Kahraman, C. A novel fuzzy TOPSIS method using emerging interval-valued spherical fuzzy sets. Eng. Appl. Artif. Intell. 2019, 85, 307–323. [Google Scholar] [CrossRef]
- Parimala, M.; Broumi, S.; Prakash, K.; Topal, S. Bellman–ford algorithm for solving shortest path problem of a network under picture fuzzy environment. Complex Intell. Syst. 2011, 7, 2373–2381. [Google Scholar] [CrossRef]
- Li, L.; Zhang, R.; Wang, J.; Shang, X.; Bai, K. A novel approach to multi-attribute group decision-making with q-rung picture linguistic information. Symmetry 2018, 10, 172. [Google Scholar] [CrossRef]
- Akram, M.; Shahzadi, G.; Alcantud, J.C.R. Multi-attribute decision-making with q-rung picture fuzzy information. Granul. Comput. 2022, 7, 197–215. [Google Scholar] [CrossRef]
- Pinar, A.; Boran, F.E. A novel distance measure on q-rung picture fuzzy sets and its application to decision making and classification problems. Artif. Intell. Rev. 2022, 55, 1317–1350. [Google Scholar] [CrossRef]
- He, J.; Wang, X.; Zhang, R.; Li, L. Some q-rung picture fuzzy Dombi Hamy Mean operators with their application to project assessment. Mathematics 2019, 7, 468. [Google Scholar] [CrossRef] [Green Version]
- Liu, P.; Shahzadi, G.; Akram, M. Specific types of q-rung picture fuzzy Yager aggregation operators for decision making. Int. J. Comput. Intell. Syst. 2020, 13, 1072–1091. [Google Scholar] [CrossRef]
- Kamacı, H.; Petchimuthu, S.; Akçetin, E. Dynamic aggregation operators and Einstein operations based on interval-valued picture hesitant fuzzy information and their applications in multi-period decision making. Comput. Appl. Math. 2021, 40, 1–52. [Google Scholar] [CrossRef]
- Yang, Z.; Li, J.; Huang, L.; Shi, Y. Developing dynamic intuitionistic normal fuzzy aggregation operators for multi-attribute decision-making with time sequence preference. Expert Syst. Appl. 2017, 82, 344–356. [Google Scholar] [CrossRef]
- Jana, C.; Pal, M.; Liu, P. Multiple attribute dynamic decision making method based on some complex aggregation functions in CQROF setting. Comput. Appl. Math. 2022, 41, 103. [Google Scholar] [CrossRef]
- Peng, D.H.; Wang, H. Dynamic hesitant fuzzy aggregation operators in multi-period decision making. Kybernetes 2014, 43, 715–736. [Google Scholar] [CrossRef]
- Gumus, S.; Bali, Q. Dynamic aggregation operators based on intuitionistic fuzzy tools and einstein operations. Fuzzy Inf. Eng. 2017, 9, 45–65. [Google Scholar] [CrossRef]
- Riaz, M.; Farid, H.M.A. Picture fuzzy aggregation approach with application to third-party logistic provider selection process. Rep. Mech. Eng. 2022, 3, 318–327. [Google Scholar] [CrossRef]
- Sahu, R.; Dash, S.R.; Das, S. Career selection of students using hybridized distance measure based on picture fuzzy set and rough set theory. Decis. Mak. Appl. Manag. Eng. 2021, 4, 104–126. [Google Scholar] [CrossRef]
- Vojinovic, N.; Stevic, Z.; Tanackov, I. A Novel IMF SWARA-FDWGA-PESTEL Analysis For Assessment Of Healthcare System. Oper. Res. Eng. Sci. Theory Appl. 2022, 5, 139–151. [Google Scholar] [CrossRef]
- Peng, X.D.; Yang, Y. Some results for Pythagorean fuzzy sets. Int. J. Intell. Syst. 2015, 30, 1133–1160. [Google Scholar] [CrossRef]
- Jana, C.; Pal, M.; Wang, J.Q. Bipolar fuzzy Dombi aggregation operators and its application in multiple-attribute decision-making process. J. Ambient. Intell. Humaniz. Comput. 2019, 10, 3533–3549. [Google Scholar] [CrossRef]
- Feng, F.; Zheng, Y.; Sun, B.; Akram, M. Novel score functions of generalized orthopair fuzzy membership grades with application to multiple attribute decision making. Granul. Comput. 2022, 7, 95–111. [Google Scholar] [CrossRef]
- Yager, R.R.; Abbasov, A.M. Pythagorean membership grades, complex numbers, and decision making. Int. J. Intell. Syst. 2013, 28, 436–452. [Google Scholar] [CrossRef]
- Yager, R.R. Generalized orthopair fuzzy sets. IEEE Trans. Fuzzy Syst. 2016, 25, 1222–1230. [Google Scholar] [CrossRef]
- Xu, Z.S. Intuitionistic fuzzy aggregation operators. IEEE Trans. Fuzzy Syst. 2007, 15, 1179–1187. [Google Scholar]
- Wei, G. Picture fuzzy aggregation operators and their application to multiple attribute decision making. J. Intell. Fuzzy Syst. 2017, 33, 713–724. [Google Scholar] [CrossRef]
- Liu, P.; Wang, P. Some q-rung orthopair fuzzy aggregation operators and their applications to multiple-attribute decision making. Int. J. Intell. Syst. 2018, 33, 259–280. [Google Scholar] [CrossRef]
- Magee, J.A.; Piskounova, E.; Morrison, S.J. Cancer stem cells: Impact, heterogeneity, and uncertainty. Cancer Cell 2012, 21, 283–296. [Google Scholar] [CrossRef] [PubMed]
- Lopez Alfonso, J.C.; Jagiella, N.; Nunez, L.; Herrero, M.A.; Drasdo, D. Estimating dose painting effects in radiotherapy: A mathematical model. PLoS ONE 2014, 9, e89380. [Google Scholar] [CrossRef]
- Jordan, C.T.; Guzman, M.L.; Noble, M. Cancer stem cells. N. Engl. J. Med. 2016, 355, 1253–1261. [Google Scholar] [CrossRef] [PubMed]
- Lobo, N.A.; Shimono, Y.; Qian, D.; Clarke, M.F. The biology of cancer stem cells. Annu. Rev. Cell Dev. Biol. 2007, 23, 675–699. [Google Scholar] [CrossRef] [Green Version]
- Blevins-Knabe, B. Early mathematical development: How the home environment matters. In Early Childhood Mathematics Skill Development in the Home Environment; Springer: Berlin/Heidelberg, Germany, 2016; pp. 7–28. [Google Scholar]
- Dawson, A.; Hillen, T. Derivation of the tumour control probability (TCP) from a cell cycle model. Comput. Math. Methods Med. 2006, 7, 121–141. [Google Scholar] [CrossRef] [Green Version]
- Gong, J. Tumor Control Probability Models. Ph.D. Thesis, University of Alberta, Edmonton, AB, USA, 2013. [Google Scholar]
- Ruddon, R.W. Cancer Biology; Oxford University Press: Oxford, UK, 2007. [Google Scholar]
- Rozek, L. S NPG services. Nat. Rev. Cancer 2005, 5, 588. [Google Scholar]
- Serkova, N.J.; Eckhardt, S.G. Metabolic imaging to assess treatment response to cytotoxic and cytostatic agents. Front. Oncol. 2016, 6, 152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gazda, M.J.; Coia, L.R. Principles of radiation therapy. In Cancer Management: A Multidisciplinary Approach; Oncology Group: Melville, NY, USA, 2001; Available online: http://thymic.org/uploads/reference_sub/02radtherapy.pdf (accessed on 15 June 2022).
- Nie, D. Cancer stem cell and niche. Front. Biosci. Sch. Ed. 2009, 2, 184–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Panje, C.M.; Glatzer, M.; Sirén, C.; Plasswilm, L. Putora PM: Treatment options in oncology. JCO Clin. Cancer Inform. 2018, 2, 1–10. [Google Scholar] [CrossRef]
- Martin, A.M.; Raabe, E.; Eberhart, C.; Cohen, K.J. Management of pediatric and adult patients with medulloblastoma. Curr. Treat. Options Oncol. 2014, 15, 581–594. [Google Scholar] [CrossRef]
- Miller, K.D.; Nogueira, L.; Mariotto, A.B.; Rowl, J.H.; Yabroff, K.R.; Alfano, C.M.; Siegel, R.L. Cancer treatment and survivorship statistics. CA Cancer J. Clin. 2019, 69, 363–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Decaestecker, K.; De Meerleer, G.; Ameye, F.; Fonteyne, V.; Lambert, B.; Joniau, S.; Ost, P. Surveillance or metastasis-directed Therapy for OligoMetastatic Prostate cancer recurrence (STOMP): Study protocol for a randomized phase II trial. BMC Cancer 2014, 14, 671. [Google Scholar] [CrossRef]
- Zappa, C.; Shaker, A.M. Non-small cell lung cancer: Current treatment and future advances. Transl. Lung Cancer Res. 2016, 5, 288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.; Triantaphyllou, E. Ranking irregularities when evaluating alternatives by using some ELECTRE methods. Omega 2008, 36, 45–63. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Corresponding Probability of Each Change () | |
|---|---|
| , | |
| (all other cases) |
| Criteria | |
|---|---|
| Age | |
| Type of cancer | |
| Stage of the cancer | |
| Cost of treatment | |
| Chance of a cure |
| (0.367,0.142,0.372) | (0.364,0.155,0.283) | (0.285,0.165,0.152) | (0.145,0.154,0.253) | (0.385,0.132,0.473) | |
| (0.167,0.384,0.236) | (0.140,0.150,0.168) | (0.165,0.135,0.374) | (0.144,0.363,0.396) | (0.145,0.475,0.337) | |
| (0.142,0.131,0.136) | (0.144,0.265,0.572) | (0.475,0.165,0.249) | (0.473,0.166,0.138) | (0.375,0.142,0.399) | |
| (0.464,0.163,0.172) | (0.485,0.175,0.152) | (0.175,0.253,0.299) | (0.155,0.242,0.393) | (0.455,0.353,0.248) | |
| (0.353,0.266,0.239) | (0.133,0.175,0.131) | (0.175,0.125,0.493) | (0.384,0.155,0.493) | (0.142,0.363,0.395) |
| (0.384,0.155,0.142) | (0.245,0.133,0.231) | (0.465,0.155,0.375) | (0.167,0.165,0.172) | (0.235,0.155,0.188) | |
| (0.165,0.125,0.285) | (0.350,0.245,0.147) | (0.155,0.280,0.134) | (0.455,0.345,0.124) | (0.152,0.140,0.182) | |
| (0.353,0.170,0.395) | (0.175,0.145,0.153) | (0.145,0.255,0.166) | (0.163,0.282,0.171) | (0.442,0.135,0.227) | |
| (0.277,0.464,0.173) | (0.165,0.166,0.132) | (0.125,0.140,0.157) | (0.280,0.272,0.237) | (0.489,0.135,0.382) | |
| (0.151,0.136,0.182) | (0.280,0.494,0.131) | (0.175,0.242,0.182) | (0.384,0.182,0.182) | (0.153,0.246,0.151) |
| (0.134,0.274,0.162) | (0.135,0.175,0.153) | (0.285,0.253,0.253) | (0.253,0.145,0.153) | (0.162,0.253,0.156) | |
| (0.242,0.166,0.374) | (0.155,0.145,0.192) | (0.144,0.165,0.137) | (0.463,0.130,0.148) | (0.134,0.134,0.145) | |
| (0.134,0.155,0.142) | (0.131,0.165,0.153) | (0.135,0.490,0.264) | (0.263,0.145,0.489) | (0.242,0.253,0.375) | |
| (0.166,0.384,0.373) | (0.353,0.275,0.153) | (0.165,0.155,0.197) | (0.255,0.155,0.264) | (0.135,0.164,0.153) | |
| (0.145,0.266,0.133) | (0.285,0.195,0.486) | (0.310,0.155,0.174) | (0.145,0.155,0.247) | (0.283,0.245,0.486) |
| (0.467,0.242,0.472) | (0.464,0.255,0.383) | (0.385,0.265,0.252) | (0.254,0.353,0.245) | (0.485,0.232,0.573) | |
| (0.267,0.484,0.336) | (0.240,0.250,0.268) | (0.265,0.235,0.474) | (0.463,0.496,0.244) | (0.245,0.575,0.437) | |
| (0.242,0.231,0.236) | (0.244,0.365,0.672) | (0.575,0.265,0.349) | (0.266,0.238,0.573) | (0.475,0.242,0.499) | |
| (0.564,0.263,0.272) | (0.585,0.275,0.252) | (0.275,0.353,0.399) | (0.342,0.493,0.255) | (0.555,0.453,0.348) | |
| (0.453,0.366,0.339) | (0.233,0.275,0.231) | (0.275,0.225,0.593) | (0.255,0.593,0.484) | (0.242,0.463,0.495) |
| (0.484,0.255,0.242) | (0.345,0.233,0.331) | (0.565,0.255,0.475) | (0.265,0.272,0.267) | (0.335,0.255,0.288) | |
| (0.265,0.225,0.385) | (0.450,0.345,0.247) | (0.255,0.380,0.234) | (0.445,0.224,0.555) | (0.252,0.240,0.282) | |
| (0.453,0.270,0.495) | (0.275,0.245,0.253) | (0.245,0.355,0.266) | (0.382,0.271,0.263) | (0.542,0.235,0.327) | |
| (0.377,0.564,0.273) | (0.265,0.266,0.232) | (0.225,0.240,0.257) | (0.372,0.337,0.380) | (0.589,0.235,0.482) | |
| (0.251,0.236,0.282) | (0.380,0.594,0.231) | (0.275,0.342,0.282) | (0.282,0.282,0.484) | (0.253,0.346,0.251) |
| (0.234,0.374,0.262) | (0.235,0.275,0.253) | (0.385,0.353,0.353) | (0.245,0.253,0.353) | (0.262,0.353,0.256) | |
| (0.342,0.266,0.474) | (0.255,0.245,0.292) | (0.244,0.265,0.237) | (0.230,0.248,0.563) | (0.234,0.234,0.245) | |
| (0.234,0.255,0.242) | (0.231,0.265,0.253) | (0.235,0.590,0.364) | (0.245,0.589,0.363) | (0.342,0.353,0.475) | |
| (0.266,0.484,0.473) | (0.453,0.375,0.253) | (0.265,0.255,0.297) | (0.255,0.364,0.355) | (0.235,0.264,0.253) | |
| (0.245,0.366,0.233) | (0.385,0.295,0.586) | (0.410,0.255,0.274) | (0.255,0.347,0.245) | (0.383,0.345,0.586) |
| (0.445253, 0.281624, 0.301029) | (0.386485, 0.251598, 0.319061) | (0.48957, 0.284412, 0.359481) | |
| (0.297577, 0.297896, 0.393483) | (0.380198, 0.282677, 0.266157) | (0.255217, 0.295307, 0.290462) | |
| (0.381590, 0.253276, 0.316056) | (0.255363, 0.282726, 0.288560) | (0.454748, 0.379352, 0.317078) | |
| (0.459936, 0.429227, 0.321736) | (0.484967, 0.271364, 0.244091) | (0.255768, 0.274417, 0.306307) | |
| (0.363962, 0.279072, 0.281441) | (0.358396, 0.383055, 0.305997) | (0.340495, 0.276223, 0.350056) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kausar, R.; Farid, H.M.A.; Riaz, M.; Božanić, D. Cancer Therapy Assessment Accounting for Heterogeneity Using q-Rung Picture Fuzzy Dynamic Aggregation Approach. Symmetry 2022, 14, 2538. https://doi.org/10.3390/sym14122538
Kausar R, Farid HMA, Riaz M, Božanić D. Cancer Therapy Assessment Accounting for Heterogeneity Using q-Rung Picture Fuzzy Dynamic Aggregation Approach. Symmetry. 2022; 14(12):2538. https://doi.org/10.3390/sym14122538
Chicago/Turabian StyleKausar, Rukhsana, Hafiz Muhammad Athar Farid, Muhammad Riaz, and Darko Božanić. 2022. "Cancer Therapy Assessment Accounting for Heterogeneity Using q-Rung Picture Fuzzy Dynamic Aggregation Approach" Symmetry 14, no. 12: 2538. https://doi.org/10.3390/sym14122538