
The Influence of Air Pollution on Non-Infectious Hospitalizations for Severe Acute Exacerbations of Chronic Obstructive Pulmonary Disease: A Time-Series from Serbia
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
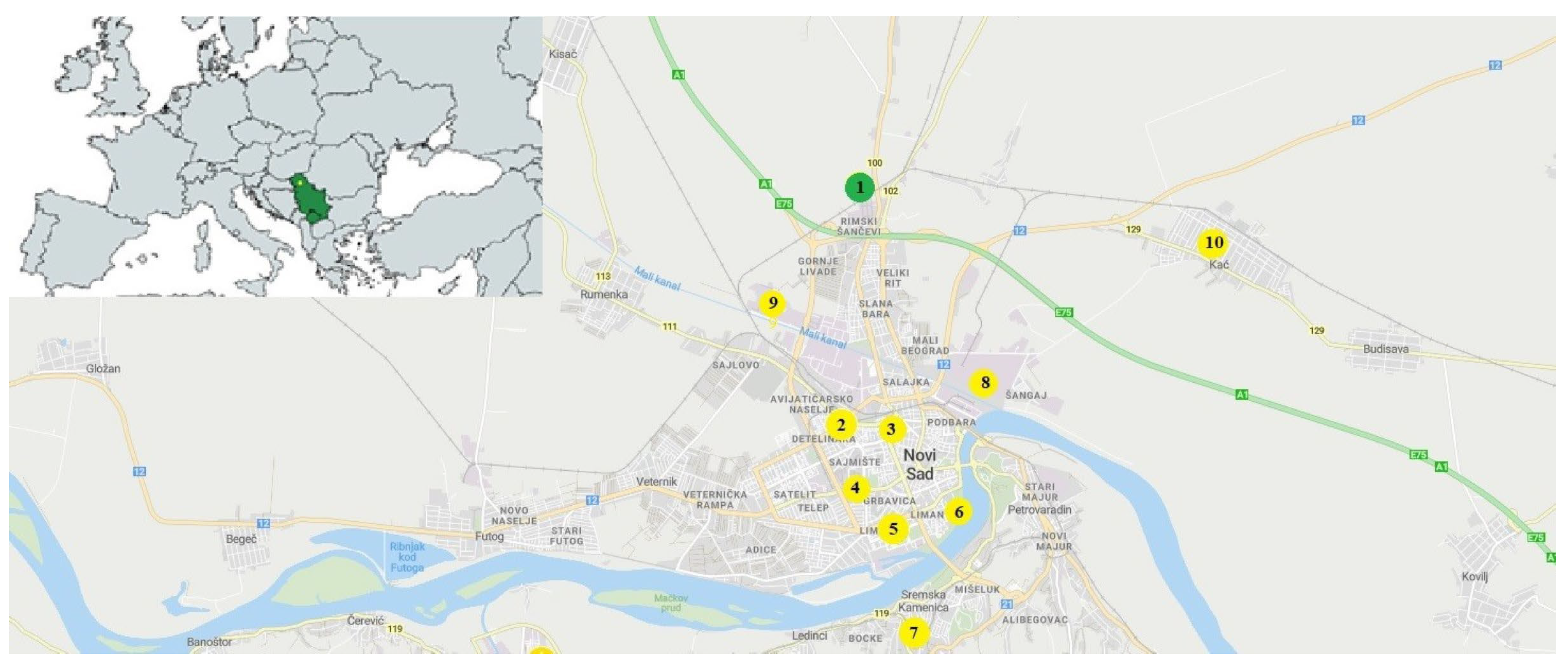
2.1. Study Design
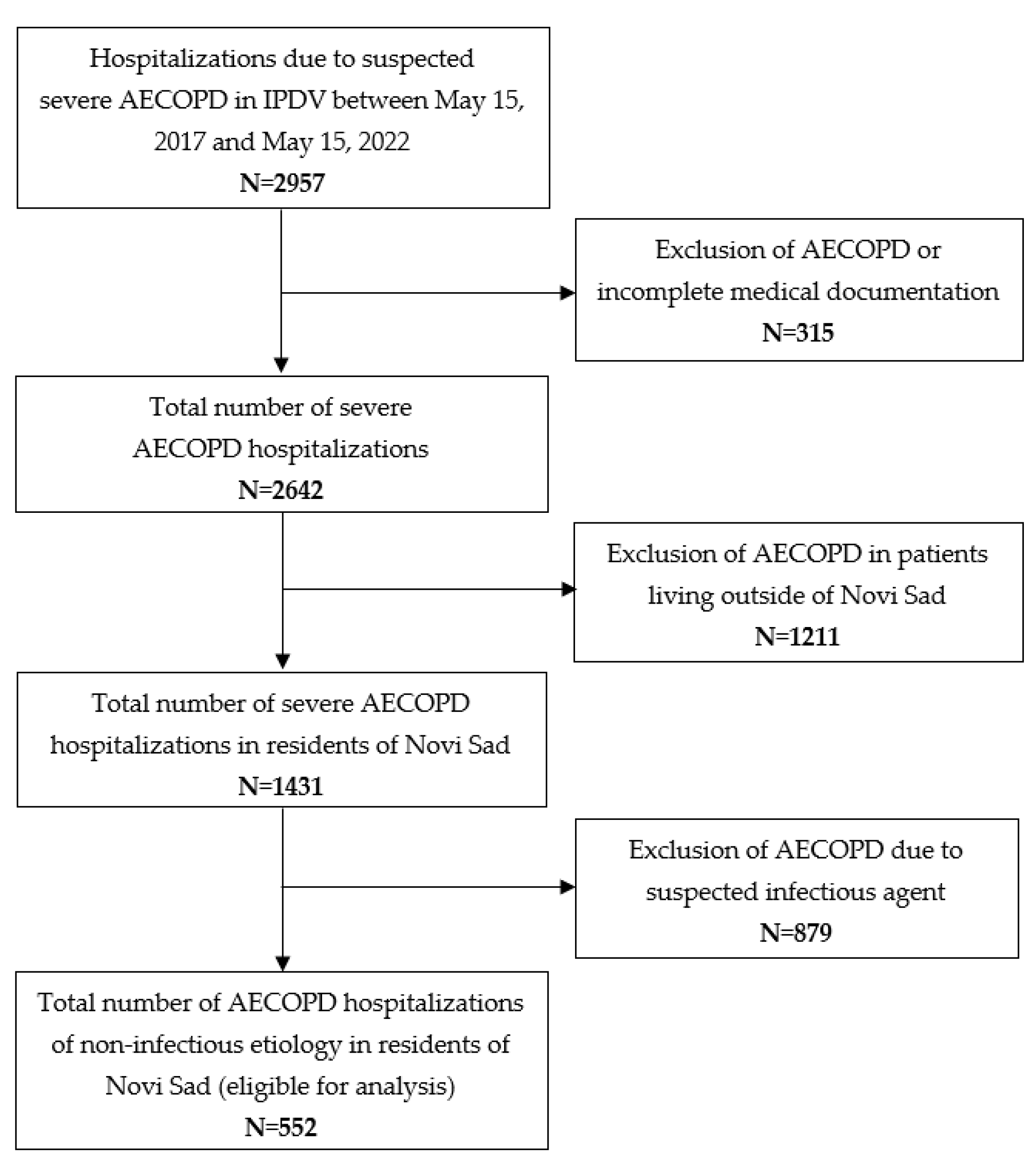
2.2. Study Population
2.3. Data on Air Pollution and Meteorological Factors
2.4. Statistical Analysis
+ ns(Date, df = 5),
3. Results
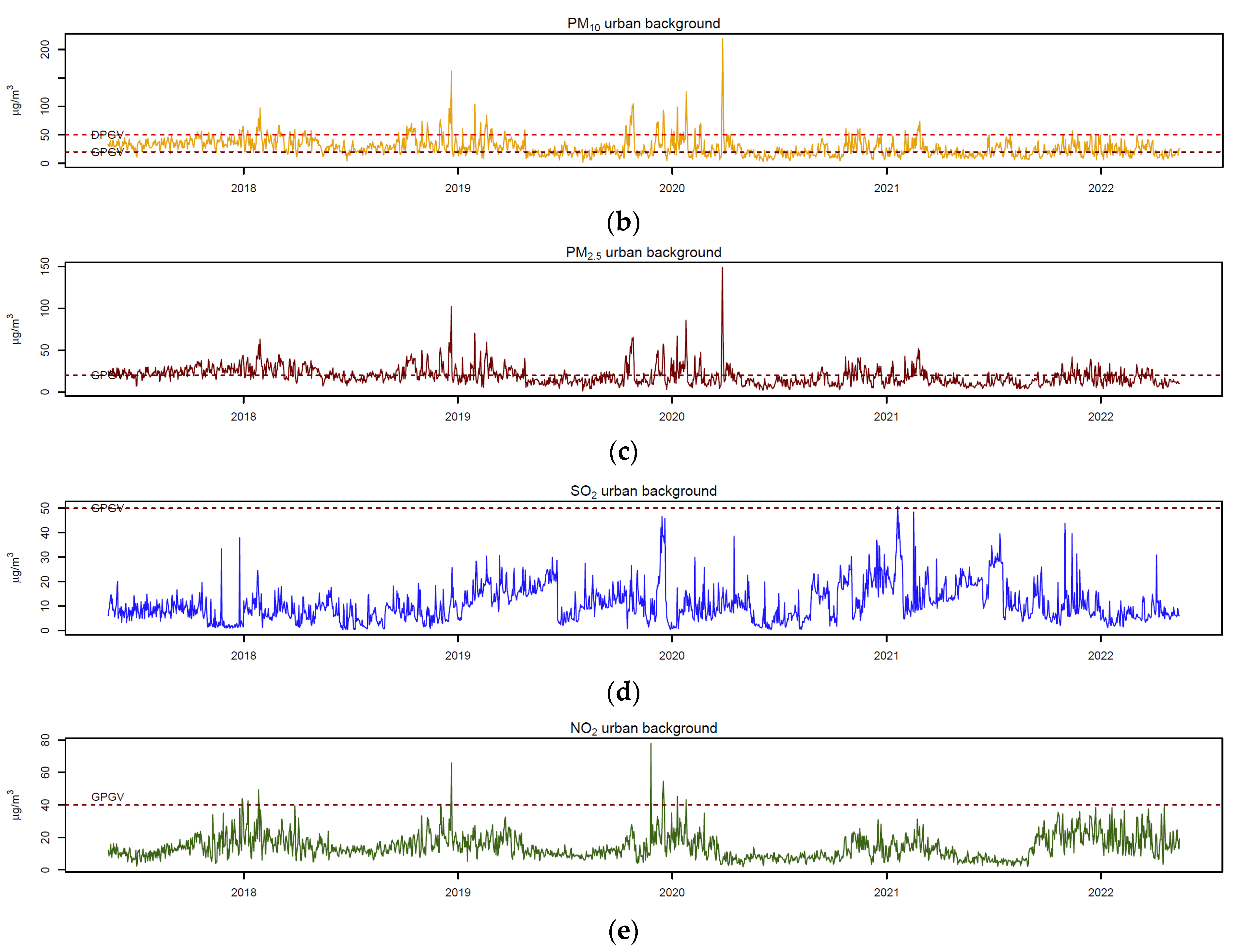
3.1. Descriptive Statistics
3.2. Correlations between Air Pollutants and Meteorological Factors
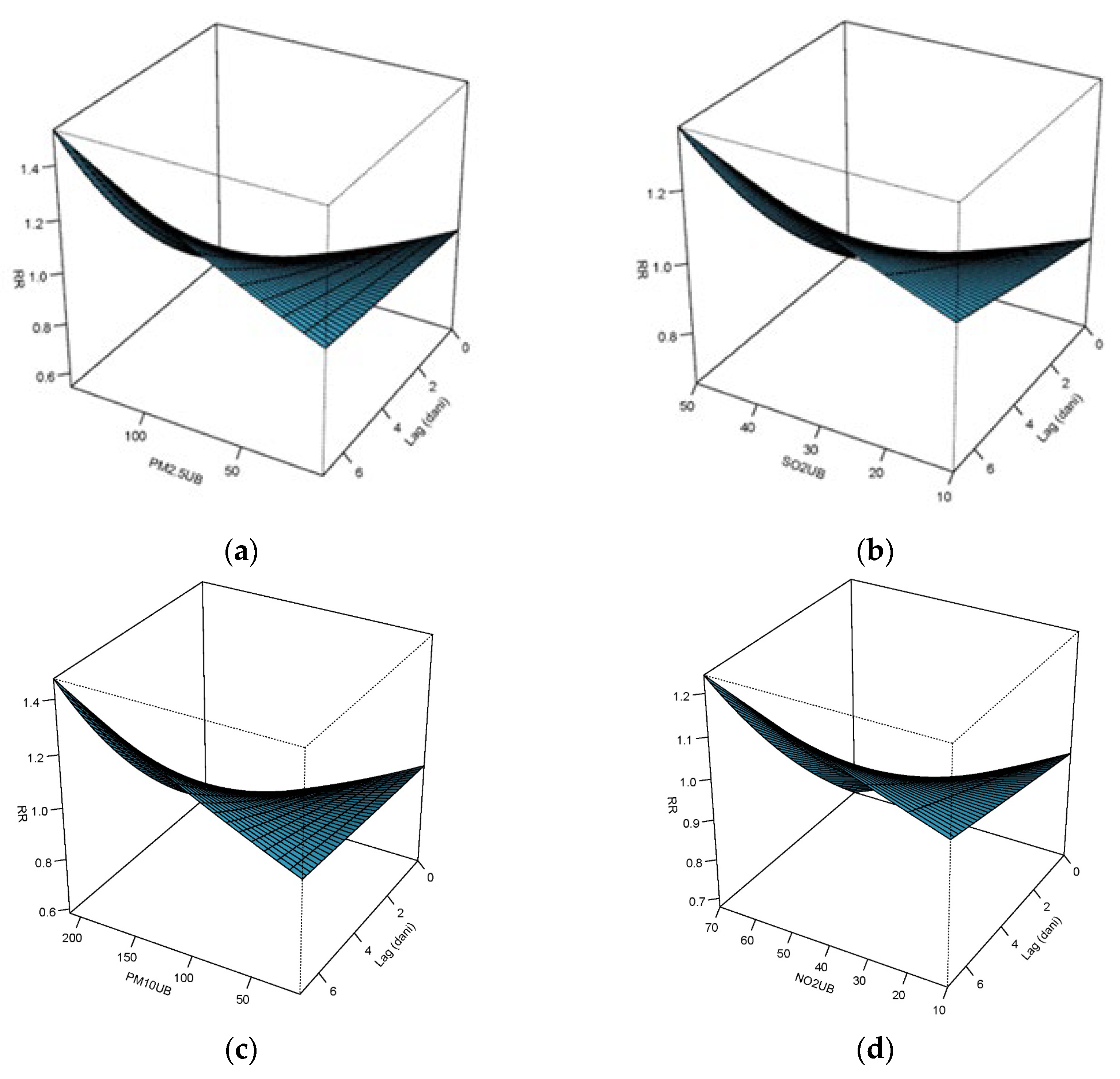
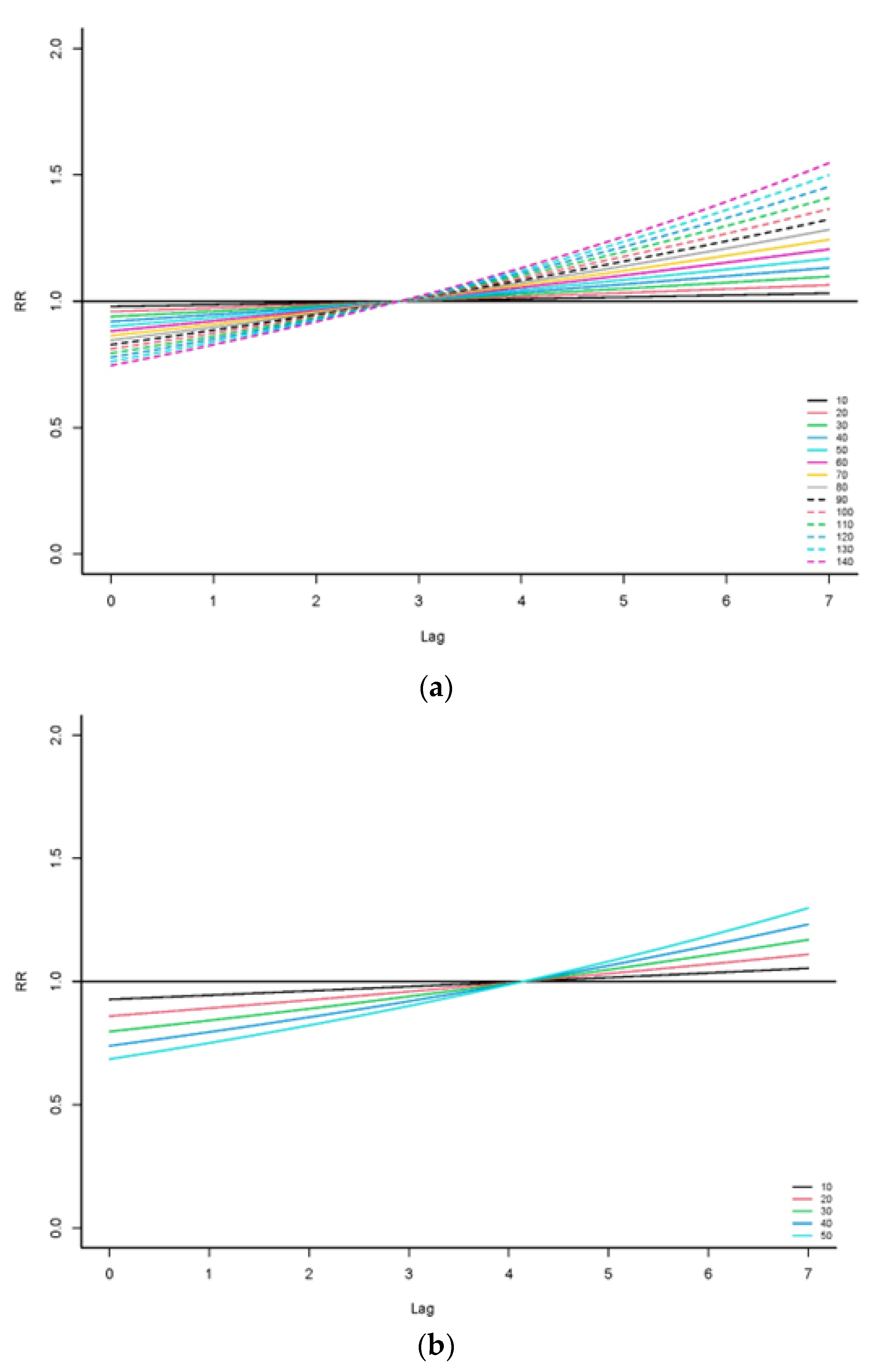
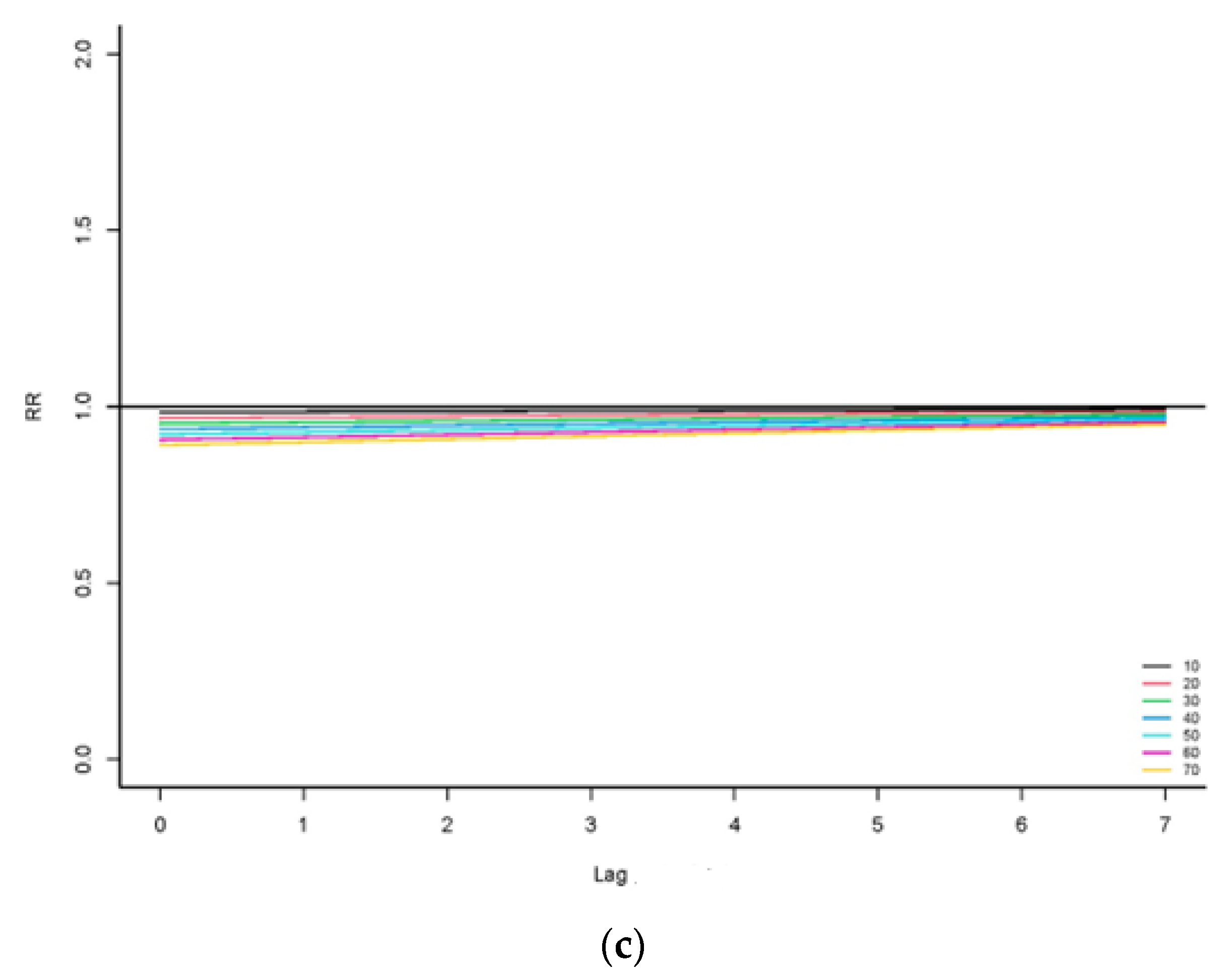
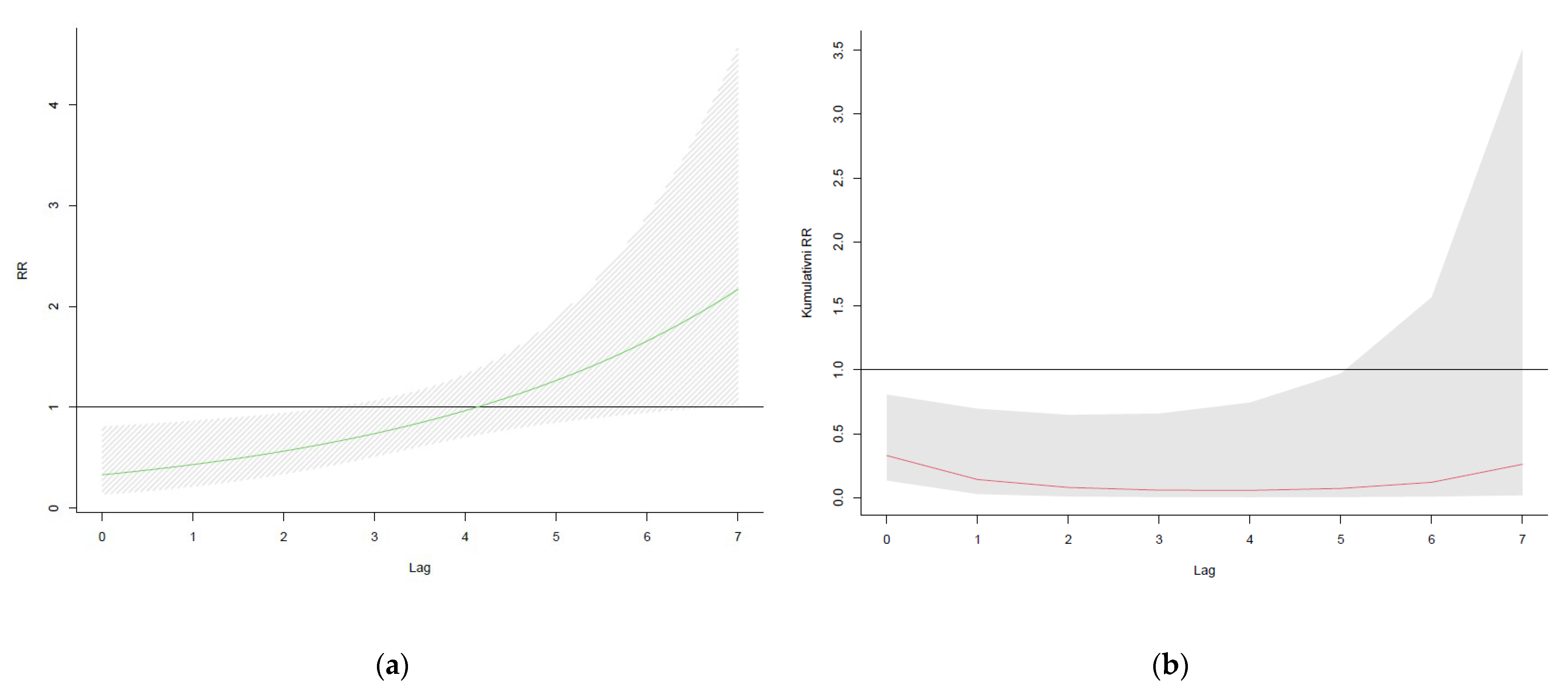
3.3. Influence of Air Pollution on AECOPD Hospitalizations (Single-Predictor and Multi-Predictor Models)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Javorac, J.; Jevtić, M.; Živanović, D.; Ilić, M.; Bijelović, S.; Dragić, N. What Are the Effects of Meteorological Factors on Exacerbations of Chronic Obstructive Pulmonary Disease? Atmosphere 2021, 12, 442. [Google Scholar] [CrossRef]
- Szalontai, K.; Gémes, N.; Furák, J.; Varga, T.; Neuperger, P.; Balog, J.Á.; Puskás, L.G.; Szebeni, G.J. Chronic Obstructive Pulmonary Disease: Epidemiology, Biomarkers, and Paving the Way to Lung Cancer. J. Clin. Med. 2021, 10, 2889. [Google Scholar] [CrossRef]
- Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease (2023 Report). Available online: https://goldcopd.org/2023-gold-report-2/ (accessed on 4 December 2022).
- National Heart, Lung and Blood Institute. Morbidity and Mortality Chartbook on Cardiovascular, Lung and Blood Diseases; US Department of Health and Human Services; Public Health Service; National Institute of Health: Bethesda, MD, USA, 2012. Available online: http://www.nhlbi.nih.gov/research/reports/2012-mortality-chart-book.html (accessed on 15 September 2022).
- Whittaker Brown, S.A.; Braman, S. Recent Advances in the Management of Acute Exacerbations of Chronic Obstructive Pulmonary Disease. Med. Clin. North Am. 2020, 104, 615–630. [Google Scholar] [CrossRef]
- DeVries, R.; Kriebel, D.; Sama, S. Outdoor Air Pollution and COPD-Related Emergency Department Visits, Hospital Admissions, and Mortality: A Meta-Analysis. COPD 2017, 14, 113–121. [Google Scholar] [CrossRef]
- Zhang, S.; Li, G.; Tian, L.; Guo, Q.; Pan, X. Short-term exposure to air pollution and morbidity of COPD and asthma in East Asian area: A systematic review and meta-analysis. Environ. Res. 2016, 148, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Song, B.; Zhang, H.; Jiao, L.; Jing, Z.; Li, H.; Wu, S. Effect of high-level fine particulate matter and its interaction with meteorological factors on AECOPD in Shijiazhuang, China. Sci. Rep. 2022, 12, 8711. [Google Scholar] [CrossRef] [PubMed]
- Dąbrowiecki, P.; Chciałowski, A.; Dąbrowiecka, A.; Piórkowska, A.; Badyda, A. Air pollution and long-term risk of hospital admission due to chronic obstructive pulmonary disease exacerbations in Poland: A time-stratified, case-crossover study. Pol. Arch. Intern. Med. 2023, 16444. [Google Scholar] [CrossRef]
- Zhou, X.; Li, C.; Gao, Y.; Zhou, C.; Huang, L.; Zhang, X. Ambient air pollutants relate to hospital admissions for chronic obstructive pulmonary disease in Ganzhou, China. Rev. Saude Publica 2022, 56, 46. [Google Scholar] [CrossRef] [PubMed]
- Gao, N.; Li, C.; Ji, J.; Yang, Y.; Wang, S.; Tian, X.; Xu, K.F. Short-term effects of ambient air pollution on chronic obstructive pulmonary disease admissions in Beijing, China (2013–2017). Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 297–309. [Google Scholar] [CrossRef]
- Sun, Q.; Liu, C.; Chen, R.; Wang, C.; Li, J.; Sun, J.; Kan, H.; Cao, J.; Bai, H. Association of fine particulate matter on acute exacerbation of chronic obstructive pulmonary disease in Yancheng, China. Sci. Total Environ. 2019, 650 Pt 2, 1665–1670. [Google Scholar] [CrossRef]
- Raji, H.; Riahi, A.; Borsi, S.H.; Masoumi, K.; Khanjani, N.; AhmadiAngali, K.; Goudarzi, G.; Dastoorpoor, M. Acute Effects of Air Pollution on Hospital Admissions for Asthma, COPD, and Bronchiectasis in Ahvaz, Iran. Int. J. Chron. Obstruct. Pulmon. Dis. 2020, 15, 501–514. [Google Scholar] [CrossRef]
- Jin, J.Q.; Han, D.; Tian, Q.; Chen, Z.Y.; Ye, Y.S.; Lin, Q.X.; Ou, C.Q.; Li, L. Individual exposure to ambient PM2.5 and hospital admissions for COPD in 110 hospitals: A case-crossover study in Guangzhou, China. Environ. Sci. Pollut. Res. Int. 2022, 29, 11699–11706. [Google Scholar] [CrossRef] [PubMed]
- Pini, L.; Giordani, J.; Gardini, G.; Concoreggi, C.; Pini, A.; Perger, E.; Vizzardi, E.; Di Bona, D.; Cappelli, C.; Ciarfaglia, M.; et al. Emergency department admission and hospitalization for COPD exacerbation and particulate matter short-term exposure in Brescia, a highly polluted town in northern Italy. Respir. Med. 2021, 179, 106334. [Google Scholar] [CrossRef]
- Mercan, Y.; Babaoglu, U.T.; Erturk, A. Short-term effect of particular matter and sulfur dioxide exposure on asthma and/or chronic obstructive pulmonary disease hospital admissions in Center of Anatolia. Environ. Monit. Assess. 2020, 192, 646. [Google Scholar] [CrossRef] [PubMed]
- Peng, W.; Li, H.; Peng, L.; Wang, Y.; Wang, W. Effects of particulate matter on hospital admissions for respiratory diseases: An ecological study based on 12.5 years of time series data in Shanghai. Environ. Health 2022, 21, 12. [Google Scholar] [CrossRef]
- Han, C.H.; Pak, H.; Chung, J.H. Short-term effects of exposure to particulate matter and air pollution on hospital admissions for asthma and chronic obstructive pulmonary disease in Gyeonggi-do, South Korea, 2007–2018. J. Environ. Health Sci. Eng. 2021, 19, 1535–1541. [Google Scholar] [CrossRef]
- Qiu, H.; Tan, K.; Long, F.; Wang, L.; Yu, H.; Deng, R.; Long, H.; Zhang, Y.; Pan, J. The burden of COPD morbidity attributable to the interaction between ambient air pollution and temperature in Chengdu, China. Int. J. Environ. Res. Public Health 2018, 15, 492. [Google Scholar] [CrossRef]
- Hoffmann, C.; Maglakelidze, M.; von Schneidemesser, E.; Witt, C.; Hoffmann, P.; Butler, T. Asthma and COPD exacerbation in relation to outdoor air pollution in the metropolitan area of Berlin, Germany. Respir. Res. 2022, 23, 64. [Google Scholar] [CrossRef]
- Gasparrini, A. Distributed Lag Linear and Non-Linear Models in R: The Package dlnm. J. Stat. Softw. 2011, 43, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Anderson, H.R.; Spix, C.; Medina, S.; Schouten, J.P.; Castellsague, J.; Rossi, G.; Zmirou, D.; Touloumi, G.; Wojtyniak, B.; Ponka, A.; et al. Air pollution and daily admissions for chronic obstructive pulmonary disease in 6 European cities: Results from the APHEA project. Eur. Respir. J. 1997, 10, 1064–1071. [Google Scholar] [CrossRef]
- Zhu, R.X.; Nie, X.H.; Chen, Y.H.; Chen, J.; Wu, S.W.; Zhao, L.H. Relationship Between Particulate Matter (PM2.5) and Hospitalizations and Mortality of Chronic Obstructive Pulmonary Disease Patients: A Meta-Analysis. Am. J. Med. Sci. 2020, 359, 354–364. [Google Scholar] [CrossRef]
- Wang, K.; Hao, Y.; Au, W.; Christiani, D.C.; Xia, Z.L. A Systematic Review and Meta-Analysis on Short-Term Particulate Matter Exposure and Chronic Obstructive Pulmonary Disease Hospitalizations in China. J. Occup. Environ. Med. 2019, 61, e112–e124. [Google Scholar] [CrossRef]
- Zhu, R.; Chen, Y.; Wu, S.; Deng, F.; Liu, Y.; Yao, W. The relationship between particulate matter (PM10) and hospitalizations and mortality of chronic obstructive pulmonary disease: A meta-analysis. COPD 2013, 10, 307–315. [Google Scholar] [CrossRef]
- Chen, Z.; Liu, N.; Tang, H.; Gao, X.; Zhang, Y.; Kan, H.; Deng, F.; Zhao, B.; Zeng, X.; Sun, Y. Health effects of exposure to sulfur dioxide, nitrogen dioxide, ozone, and carbon monoxide between 1980 and 2019: A systematic review and meta-analysis. Indoor Air 2022, 32, e13170. [Google Scholar] [CrossRef]
- Li, M.H.; Fan, L.C.; Mao, B.; Yang, J.W.; Choi, A.M.K.; Cao, W.J.; Xu, J.F. Short-term Exposure to Ambient Fine Particulate Matter Increases Hospitalizations and Mortality in COPD: A Systematic Review and Meta-analysis. Chest 2016, 149, 447–458. [Google Scholar] [CrossRef]
- Hwang, S.L.; Guo, S.E.; Chi, M.C.; Chou, C.T.; Lin, Y.C.; Lin, C.M.; Chou, Y.L. Association between Atmospheric Fine Particulate Matter and Hospital Admissions for Chronic Obstructive Pulmonary Disease in Southwestern Taiwan: A Population-Based Study. Int. J. Environ. Res. Public Health 2016, 13, 366. [Google Scholar] [CrossRef]
- Qian, Y.; Li, H.; Rosenberg, A.; Li, Q.; Sarnat, J.; Papatheodorou, S.; Schwartz, J.; Liang, D.; Liu, Y.; Liu, P.; et al. Long-term exposure to low-level NO2 and mortality among the elderly population in the southeastern United States. Environ. Health Perspect. 2021, 129, 127009. [Google Scholar] [CrossRef]
- DeVries, R.; Kriebel, D.; Sama, S. Low level air pollution and exacerbation of existing copd: A case crossover analysis. Environ. Health 2016, 15, 98. [Google Scholar] [CrossRef]
- Loaiza-Ceballos, M.C.; Marin-Palma, D.; Zapata, W.; Hernandez, J.C. Viral respiratory infections and air pollutants. Air Qual. Atmos. Health. 2022, 15, 105–114. [Google Scholar] [CrossRef]
- Choi, J.; Shim, J.J.; Lee, M.G.; Rhee, C.K.; Joo, H.; Lee, J.H.; Park, H.Y.; Kim, W.J.; Um, S.J.; Kim, D.K.; et al. Association Between Air Pollution and Viral Infection in Severe Acute Exacerbation of Chronic Obstructive Pulmonary Disease. J. Korean Med. Sci. 2023, 38, e68. [Google Scholar] [CrossRef]
- Belleudi, V.; Faustini, A.; Stafoggia, M.; Cattani, G.; Marconi, A.; Perucci, C.A.; Forastiere, F. Impact of fine and ultrafine particles on emergency hospital admissions for cardiac and respiratory diseases. Epidemiology 2010, 21, 414–423. [Google Scholar] [CrossRef] [PubMed]
- Anderson, H.R.; Bremner, S.A.; Atkinson, R.W.; Harrison, R.M.; Walters, S. Particulate matter and daily mortality and hospital admissions in the west midlands conurbation of the United Kingdom: Associations with fine and coarse particles, black smoke and sulphate. Occup. Environ. Med. 2001, 58, 504–510. [Google Scholar] [CrossRef]
- Faustini, A.; Stafoggia, M.; Colais, P.; Berti, G.; Bisanti, L.; Cadum, E.; Cernigliaro, A.; Mallone, S.; Scarnato, C.; Forastiere, F. Air pollution and multiple acute respiratory outcomes. Eur. Respir. J. 2013, 42, 304–313. [Google Scholar] [CrossRef] [PubMed]
- Schikowski, T.; Adam, M.; Marcon, A.; Cai, Y.; Vierkötter, A.; Carsin, A.E.; Jacquemin, B.; Al Kanani, Z.; Beelen, R.; Birk, M.; et al. Association of ambient air pollution with the prevalence and incidence of COPD. Eur. Respir. J. 2014, 44, 614–626. [Google Scholar] [CrossRef]
- Stieb, D.M.; Szyszkowicz, M.; Rowe, B.H.; Leech, J.A. Air pollution and emergency department visits for cardiac and respiratory conditions: A multi-city time-series analysis. Environ. Health 2009, 8, 25. [Google Scholar] [CrossRef]
- Slaughter, J.C.; Kim, E.; Sheppard, L.; Sullivan, J.H.; Larson, T.V.; Claiborn, C. Association between particulate matter and emergency room visits, hospital admissions and mortality in Spokane, Washington. J. Expo. Anal. Environ. Epidemiol. 2005, 15, 153–159. [Google Scholar] [CrossRef] [PubMed]
- Peel, J.L.; Tolbert, P.E.; Klein, M.; Metzger, K.B.; Flanders, W.D.; Todd, K.; Mulholland, J.A.; Ryan, P.B.; Frumkin, H. Ambient air pollution and respiratory emergency department visits. Epidemiology 2005, 16, 164–174. [Google Scholar] [CrossRef]
- Stevanović, I.; Jovasević-Stojanović, M.; Jović Stosić, J. Association between ambient air pollution, meteorological conditions and exacerbations of asthma and chronic obstructive pulmonary disease in adult citizens of the town of Smederevo. Vojnosanit. Pregl. 2016, 73, 152–158. [Google Scholar] [CrossRef]
- Jevtić, M.; Dragić, N.; Bijelović, S.; Popović, M. Air pollution and hospital admissions for chronic obstructive pulmonary disease in Novi Sad. Health Med. 2012, 6, 1207–1215. [Google Scholar]
- Milutinović, S.; Nikić, D.; Stošić, L.; Stanković, A.; Bogdanović, D. Short-term association between air pollution and emergency room admissions for chronic obstructive pulmonary disease in Nis, Serbia. Cent. Eur. J. Public Health 2009, 17, 8–13. [Google Scholar] [CrossRef] [PubMed]
- Stosic, L.; Dragic, N.; Stojanovic, D.; Lazarevic, K.; Bijelovic, S.; Apostolovic, M. Air pollution and hospital admissions for respiratory diseases in Nis, Serbia. Pol. J. Environ. Stud. 2021, 30, 4677–4686. [Google Scholar] [CrossRef]
- Institut za Javno Zdravlje Vojvodine. Prepoznavanje Faktora Rizika iz Životne Sredine Značajnih za Prevenciju Hronične Opstruktivne Bolesti Pluća među Stanovništvom Grada Novog Sada. (In Serbian). Available online: http://www.izjzv.org.rs/izjzv/uploads/ddbd4a24-356a-dab0-c031-e3e5b1102a0e/Prilog%20Izvestaju%20Projekta%20zdravstvo%20HOBP%202018.pdf (accessed on 25 March 2023).









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Number of Patients (%) | ||
|---|---|---|
| Gender | Male | 228 (41.3) |
| Female | 324 (58.7) | |
| Age | Under 65 | 176 (31.88) |
| 65 or older | 376 (68.12) | |
| Smoking status | Active smokers | 239 (44%) |
| Former smokers | 228 (41.9%) | |
| Non-smokers | 76 (14%) | |
| Comorbidities | Cardiovascular diseases | 446 (80.8) |
| Other respiratory diseases | 50 (9.06) | |
| Diabetes mellitus | 71 (12.86) | |
| Other endocrinological diseases | 94 (17.03) | |
| Depression | 68 (12.32%) | |
| Other psychiatric diseases | 21 (3.8%) | |
| Neurological diseases | 69 (12.5) | |
| Gastrointestinal diseases | 87 (15.76) | |
| Malignancy | 89 (16.12%) | |
| Urogenital diseases | 45 (8.15) | |
| Other | 66 (11.96%) | |
| COPD history | Mean years since COPD diagnosis | 9.33 (±7.31, range 0–45) |
| Previous hospitalizations due to AECOPD | 3.4 (±5.78, range 0–41) |
| PM10 | PM2.5 | SO2 | NO2 | AP | Temp. | Hum. | WS | |
|---|---|---|---|---|---|---|---|---|
| PM10 | 0.97 ** | 0.02 | 0.49 ** | 0.22 ** | −0.16 ** | 0.03 | −0.21 ** | |
| PM2.5 | 0.97 ** | 0.00 | 0.52 ** | 0.23 ** | −0.22 ** | 0.07 | −0.20 ** | |
| SO2 | 0.02 | 0.00 | −0.07 | −0.18 ** | 0.03 | −0.13 ** | −0.02 | |
| NO2 | 0.49 ** | 0.52 ** | −0.07 ** | 0.33 ** | −0.52 ** | 0.34 ** | −0.16 ** | |
| AP | 0.22 ** | 0,23 ** | −0.18 ** | 0.33 ** | −0.33 ** | −0.01 | −0.13 ** | |
| Temp. | −0.16 ** | −0.22 ** | 0.03 | −0.52 ** | −0.33 ** | −0.58 ** | −0.17 ** | |
| Hum. | 0.03 | 0.07 ** | −0.13 ** | 0.34 ** | −0.01 | −0.58 ** | −0.03 | |
| WS | −0.21 ** | −0.20 ** | −0.02 | −0.16 ** | −0.13 ** | −0.17 ** | −0.03 |
| Concentration (in μg/m3) | RR (95% CI RR) | |||
|---|---|---|---|---|
| PM10 UB | PM2.5 UB | SO2 UB | NO2 UB | |
| 10 | 0.97 (0.89–1.06) | 0.95 (0.84–1.07) | 0.91 (0.76–1.09) | 0.91 (0.76–1.08) |
| 20 | 0.94 (0.80–1.12) | 0.90 (0.70–1.16) | 0.83 (0.57–1.19) | 0.82 (0.57–1.17) |
| 30 | 0.92 (0.71–1.18) | 0.85 (0.59–1.24) | 0.75 (0.43–1.31) | 0.74 (0.44–1.27) |
| 40 | 0.89 (0.64–1.25) | 0.81 (0.49–1.33) | 0.68 (0.33–1.43) | 0.67 (0.33–1.37) |
| 50 | 0.86 (0.57–1.32) | 0.77 (0.41–1.43) | 0.62 (0.25–1.56) | 0.61 (0.25–1.48) |
| 60 | 0.84 (0.51–1.39) | 0.73 (0.34–1.54) | 0.55 (0.19–1.60) | |
| 70 | 0.82 (0.45–1.47) | 0.69 (0.29–1.66) | 0.50 (0.14–1.74) | |
| 80 | 0.79 (0.40–1.55) | 0.66 (0.24–1.78) | ||
| 90 | 0.77 (0.36–1.64) | 0.62 (0.20–1.92) | ||
| 100 | 0.75 (0.32–1.73) | 0.59 (0.17–2.06) | ||
| 110 | 0.73 (0.29–1.83) | 0.56 (0.14–2.21) | ||
| 120 | 0.71 (0.26–1.93) | 0.53 (0.12–2.38) | ||
| 130 | 0.68 (0.23–2.04) | 0.50 (0.10–2.56) | ||
| 140 | 0.67 (0.20–2.16) | 0.48 (0.08–2.75) | ||
| 150 | 0.65 (0.18–2.28) | |||
| 160 | 0.63 (0.16–2.41) | |||
| 170 | 0.61 (0.15–2.55) | |||
| 180 | 0.59 (0.13–2.69) | |||
| 190 | 0.57 (0.12–2.84) | |||
| 200 | 0.56 (0.10–3.00) | |||
| 210 | 0.54 (0.09–3.17) | |||
| Variable | PM10 | PM2.5 | SO2 | NO2 | |
|---|---|---|---|---|---|
| Smoking status | Single-predictor models | ||||
| Smokers | 0.52 (0.13–2.07) | 0.49 (0.12–1.96) | 1.02 (0.46–2.24) | 0.47 (0.16–1.37) | |
| Non-smokers | 0.87 (0.26–2.94) | 0.79 (0.23–2.72) | 0.59 (0.28–1.24) | 0.83 (0.33–2.11) | |
| Multi-predictor models | |||||
| Smokers | - | 1.55 (0.23–10.41) | 1.04 (0.46–2.34) | 0.63 (0.11–3.59) | |
| Non-smokers | - | 1.02 (0.17–6.13) | 0.58 (0.27–1.26) | 0.86 (0.18–4.15) | |
| Study/ Country | No. of AECOPD | Time Period | Study Design | Lag Days a | Air Pollutant | OR/RR/PC (95% CI) b | Confounding Factors |
|---|---|---|---|---|---|---|---|
| Song et al., [8] 2022; China | 4766 | January 2015–December 2018 | Time-series | 0–7 | PM2.5 | OR 1.114 (1.055 to 1.176) | Temperature, humidity, other air pollutants, time, holiday, day of the week |
| Dąbrowiecki et al., [9] 2023; Poland | 26,948 | 1 January 2011 – 31 December 2018 | Case-crossover | 0–21 | PM10 | RR 1.028 (1.008 to 1.049) | Temperature, humidity, atmospheric pressure, time, city, day of the week |
| PM2.5 | RR 1.030 (1.006 to 1.055) | ||||||
| SO2 | RR 1.145 (1.038 to 1.262) | ||||||
| NO2 | RR 1.032 (0.988 to 1.078) d | ||||||
| Zhou et al., [10] 2021; China | 4980 | 1 January 2016–31 December 2020 | Time-series | 6 | PM10 | PC 1.3% (0.3 to 2.4) | Seasonal and long-term trends, air pollutants |
| 6 | PM2.5 | PC 2.8% (1.0 to 4.7) | |||||
| 6 | SO2 | PC ~3.2% (−0.7 to 7.1) d | |||||
| 9 | NO2 | PC 3.6% (1.2 to 6.2) | |||||
| Gao et al., [11] 2019; China | 73,076 | 1 January 2013–28 February 2017 | Time-series | 0–7 | PM10 | PC 0.92% (0.55 to 1.30) | Temperature, humidity, seasonal and long-term trends |
| 0–6 | PM2.5 | PC 0.82% (0.38 to 1.26) | |||||
| 0–1 | SO2 | PC 2.07% (1.0 to 3.15) | |||||
| 0–6 | NO2 | PC 3.03% (1.82 to 4.26) | |||||
| Sun et al., [12] 2019; China | 4761 | 1 January 2015–31 December 2017 | Time-series | 0 | PM2.5 | PC 1.05% (0.14 to 1.96) | Temperature, humidity, other air pollutants, time, holiday, day of the week |
| Raji et al., [13] 2020; Iran | 4534 | March 2008–March 2018 | Time-series | 2 | PM2.5 | RR 1.003 (1.001 to 1.005) | Temperature, humidity, trend, seasonality, weekdays, holidays |
| 4 | NO2 | RR 1.049 (1.017 to 1.124) (only in females) | |||||
| Jin et al., [14] 2022; China | 40,002 | 2014—2015 | Case-crossover | 0–5 | PM2.5 | OR 1.016 (1.006 to 1.027) | Temperature, humidity, holiday |
| Pini et al., [15] 2021; Italy | 431 | January 2014–January 2016 | Time-series | 0–5 | PM10 | RR 1.07 (1.01 to 1.14) | Medium and long-term temporal trends, holidays, influenza, humidity, temperature |
| 0–5 | PM2.5 | RR 1.11 (1.04 to 1.18) | |||||
| Mercan et al., [16] 2020; Turkey | 23,830 | 1 August 2016–1 August 2019 | Time-series | 0 | PM10 | RR 1.029 (1.022 to 1.035) | Temperature, humidity, atmospheric pressure, holiday, day of the week, |
| 0 | SO2 | RR 1.065 (1.056 to 1.075) | |||||
| Peng et al., [17] 2022; China | 665,541 | 1 January 2008–31 July 2020 | Time-series | 1 | PM10 | PC 0.361% (0.151 to 0.572) | Temperature, humidity, seasonality, weekdays, holidays |
| PM2.5 | PC 1.167% (0.820 to 1.515) | ||||||
| Han et al., [18] 2021; China | 85,301 | January 2007–February 2018 | Case-crossover | 6 | PM10 | OR 1.01 (1.00 to 1.01) c | Temperature, humidity, atmospheric pressure |
| 0–7 | PM2.5 | OR 1.11 (1.10 to 1.13) c | |||||
| 0–4 | SO2 | OR 1.65 (1.53 to 1.79) c | |||||
| 5 | NO2 | OR 1.05 (1.04 to 1.05) c |
| Study/ Country | No. of AECOPD | Time Period | Study Design | Lag Days a | Air Pollutant | OR/RR/PC (95% CI) | Confounding Factors |
|---|---|---|---|---|---|---|---|
| Hoffmann et al., [20] 2022; Germany | 8645 | 1 January 2005–31 December 2015 | Time-series | 0 | PM10 | N/A (0.988 to 1.032) b | Seasonal and long-term trends, temperature, humidity, wind speed |
| PM2.5 | N/A (0.966 to 1.019) b | ||||||
| NO2 | RR 1.123 (1.081 to 1.168) b,* | ||||||
| Stieb et al., [37] 2009; Canada | 40,491 (ED visits) | 1990s–early 2000s | Time-series | 0 | PM10 | PC −0.6 (−3.3 to 2.2) per 20.6 μg/m3 increase | Temporal cycles, temperature, humidity, day of the week, holidays |
| PM2.5 | PC −1.8 (−6.1 to 2.7) per 8.2 μg/m3 increase | ||||||
| SO2 | PC −1.9 (−4.3 to 0.6) per 5.1 ppb increase | ||||||
| NO2 | PC 0.1 (−5.6 to 6.2) per 18.4 ppb increase | ||||||
| Slaughter et al., [38] 2005; USA | 1.1 cases/day | January 1995–December 2000 | Time-series | 1 | PM10 | RR 0.99 (0.91 to 1.08) b | Seasonal and long-term trends, time, temperature, humidity, day of the week |
| PM2.5 | RR 0.98 (0.90 to 1.07) b | ||||||
| Peel et al., [39] 2005; USA | 7.42 cases/day (ED visits) | 1 January 1993–31 August 2000 | Time-series | 0–3 | PM10 | RR 1.018 (0.994 to 1.043) b | Seasonal and long-term trends, time, temperature, dew point, day of the week, holiday, hospital entry and exit |
| NO2 | RR 1.035 (1.006 to 1.065) * per 20 ppb increase | ||||||
| SO2 | RR 1.016 (0.985 to 1.049) per 20 ppb increase | ||||||
| Faustini et al., [35] 2005; Italy | 38,577 | 1 January 2001–31 December 2005 | Case-crossover | 0 | PM10 | PC 0.67 (−0.02 to 1.35) b | Temperature, atmospheric pressure, seasonal and long-term trends, holidays, influenza epidemics |
| NO2 | PC 1.20 (0.17 to 2.23) b,* | ||||||
| Belleudi et al., [33] 2010; Italy | 15,087 | 10 April 2001–31 December 2005 | Case-crossover | 0 | PM10 | PC 0.40 (−1.41 to 2.25) for 14 μg/m3 | Seasonal trends, temperature, barometric pressure, holidays |
| PM2.5 | PC 1.88 (−0.27 to 4.09) for 10 μg/m3 | ||||||
| Anderson et al., [34] 2001; UK | N/A | October 1994–December 1996 | Time-series | 0 | PM10 | PC −1.8 (−6.9 to 3.5) c | Long-term time trends, seasonal patterns, influenza epidemic, day of the week, temperature, humidity |
| PM2.5 | PC −3.9 (−9.0 to 1.6) c | ||||||
| SO2 | PC −4.2 (−8.9 to 0.8) c | ||||||
| NO2 | PC 2.5 (2.1 to 7.3) c |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Javorac, J.; Živanović, D.; Ilić, M.; Kašiković Lečić, S.; Milenković, A.; Dragić, N.; Bijelović, S.; Savić, N.; Tot Vereš, K.; Smuđa, M.; et al. The Influence of Air Pollution on Non-Infectious Hospitalizations for Severe Acute Exacerbations of Chronic Obstructive Pulmonary Disease: A Time-Series from Serbia. Atmosphere 2023, 14, 730. https://doi.org/10.3390/atmos14040730
Javorac J, Živanović D, Ilić M, Kašiković Lečić S, Milenković A, Dragić N, Bijelović S, Savić N, Tot Vereš K, Smuđa M, et al. The Influence of Air Pollution on Non-Infectious Hospitalizations for Severe Acute Exacerbations of Chronic Obstructive Pulmonary Disease: A Time-Series from Serbia. Atmosphere. 2023; 14(4):730. https://doi.org/10.3390/atmos14040730
Chicago/Turabian StyleJavorac, Jovan, Dejan Živanović, Miroslav Ilić, Svetlana Kašiković Lečić, Ana Milenković, Nataša Dragić, Sanja Bijelović, Nevena Savić, Kristina Tot Vereš, Mirjana Smuđa, and et al. 2023. "The Influence of Air Pollution on Non-Infectious Hospitalizations for Severe Acute Exacerbations of Chronic Obstructive Pulmonary Disease: A Time-Series from Serbia" Atmosphere 14, no. 4: 730. https://doi.org/10.3390/atmos14040730