

Burden of Natural-Cause and Cause-Specific Mortality Associated with Long-Term Exposure to PM2.5: A Case Study in Attica Region, Greece

Abstract
:1. Introduction
2. Materials and Methods
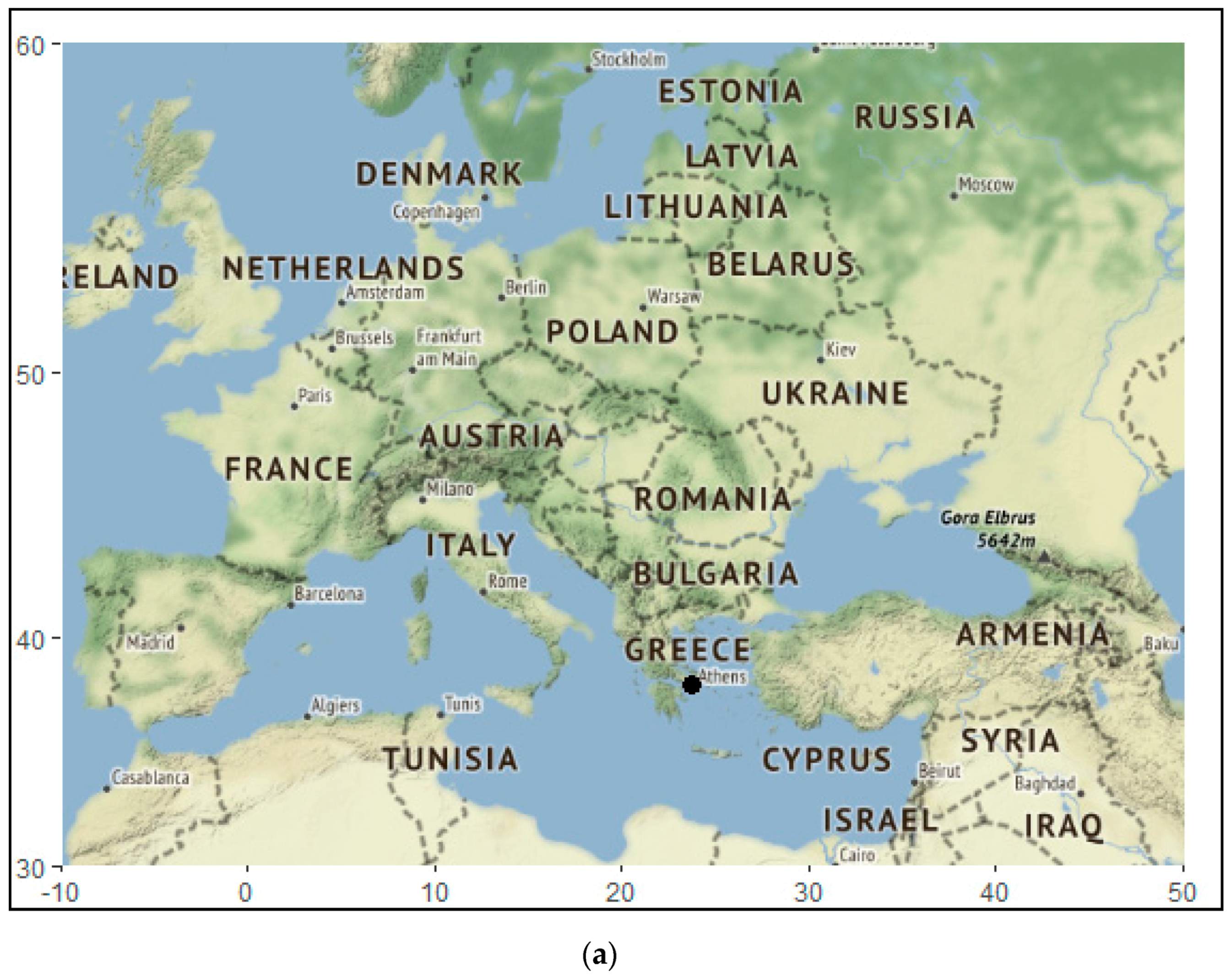
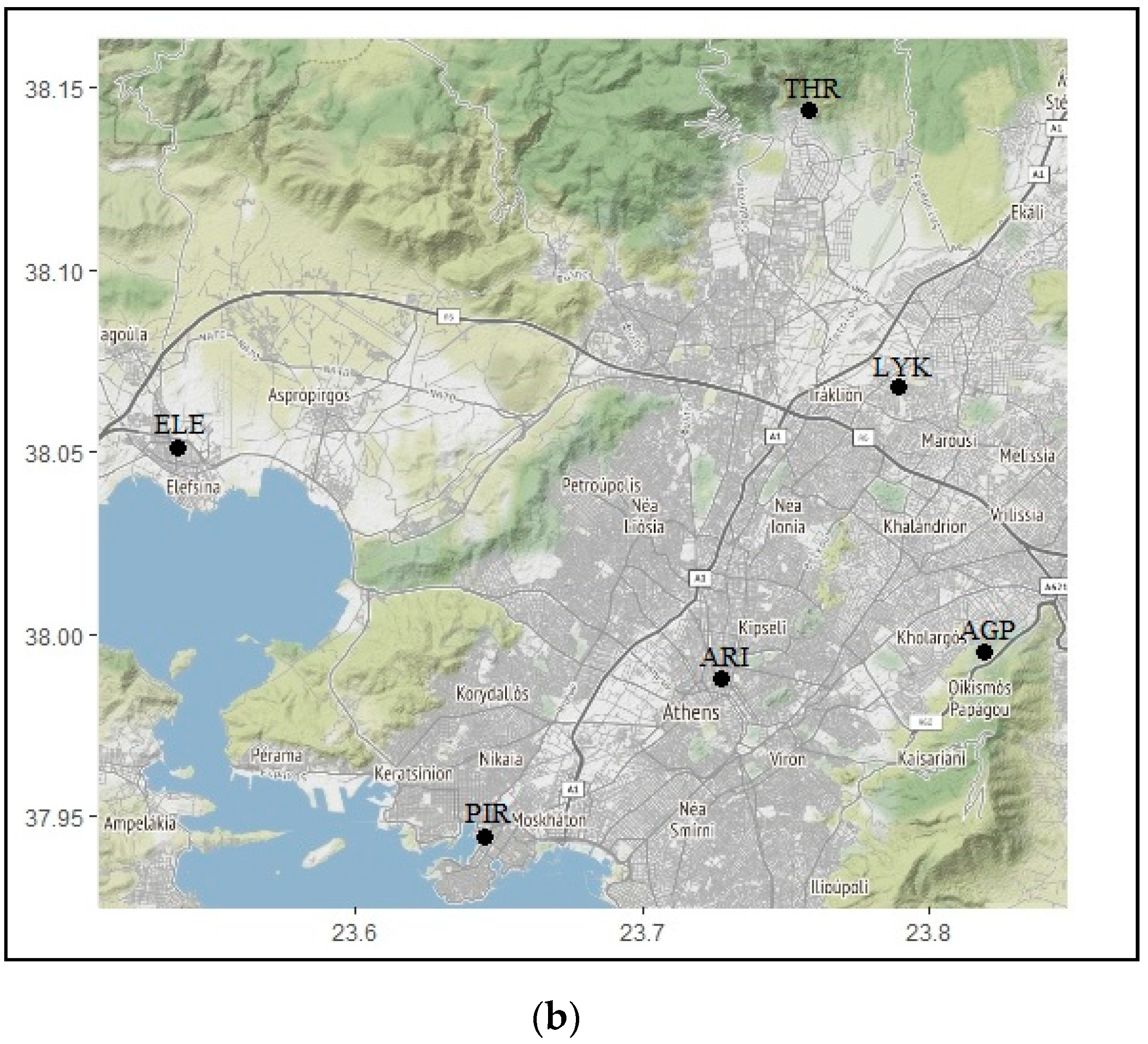
2.1. Study Area
2.2. Environmental Data
2.2.1. Data Collection
2.2.2. Data Calculation
2.3. Health Data
2.4. Health Impact Assessment in AirQ Software
3. Results and Discussion
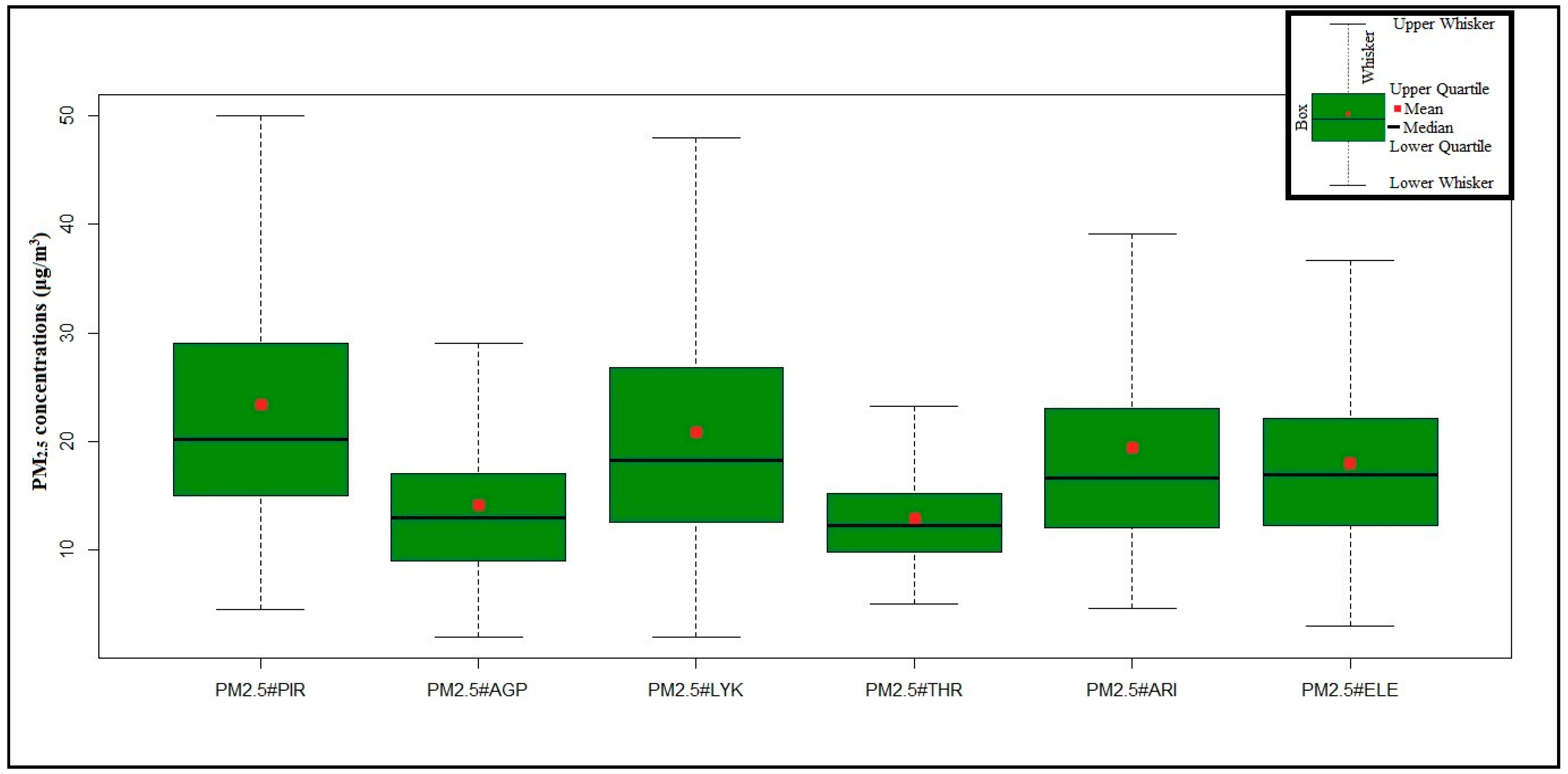
3.1. Temporal Variations of PM2.5 Concentrations
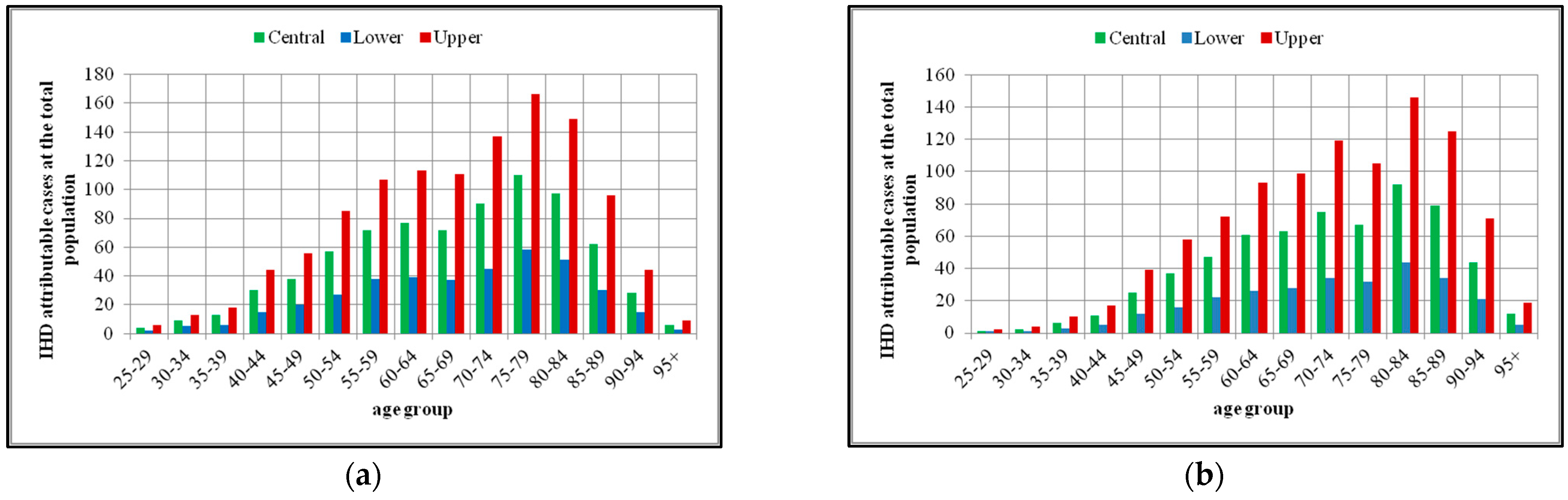
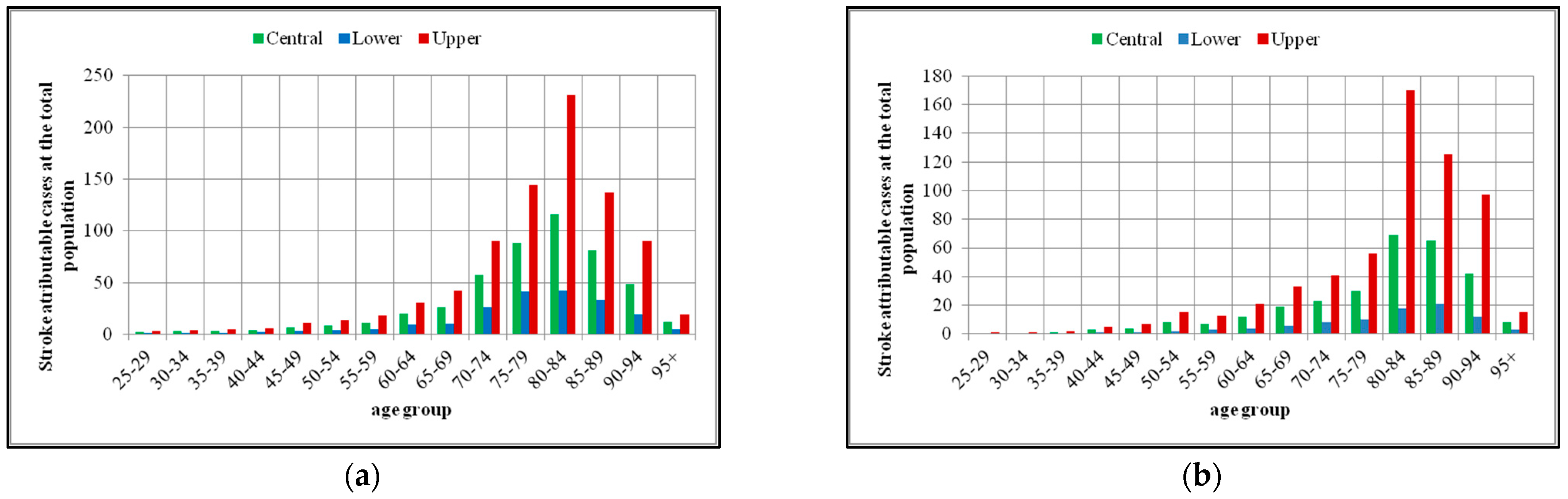
3.2. Mortality Attributed to the Exposure to PM2.5
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Manisalidis, I.; Stavropoulou, E.; Stavropoulos, A.; Bezirtzoglou, E. Environmental and Health Impacts of Air Pollution: A Review. Front. Public Health 2020, 8, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fuller, R.; Landrigan, P.J.; Balakrishnan, K.; Bathan, G.; Bose-O’Reilly, S.; Brauer, M.; Caravanos, J.; Chiles, T.; Cohen, A.; Corra, L.; et al. Pollution and health: A progress update. Lancet Planet. Health 2022, 6, e535–e547. [Google Scholar] [CrossRef] [PubMed]
- Rajagopalan, S.; Al-Kindi, S.G.; Brook, R.D. Air Pollution and Cardiovascular Disease: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2018, 72, 2054–2070. [Google Scholar] [CrossRef]
- Guevara, M. Emissions of Primary Particulate Matter. In Airborne Particulate Matter: Sources, Atmospheric Processes and Health; Royal Society of Chemsitry: London, UK, 2016; pp. 1–34. [Google Scholar] [CrossRef]
- Singh, K.; Tripathi, D. Particulate Matter and Human Health. In Environmental Health; IntechOpen: London, UK, 2021. [Google Scholar] [CrossRef]
- Miller, M.R.; Newby, D.E. Air pollution and cardiovascular disease: Car sick. Cardiovasc. Res. 2020, 116, 279–294. [Google Scholar] [CrossRef]
- Espitia-Pérez, L.; Jiménez-Vidal, L.; Espitia-Pérez, P. Particulate Matter Exposure: Genomic Instability, Disease, and Cancer Risk. In Environmental Health—Management and Prevention Practices; IntechOpen: London, UK, 2019. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.S.; Gordon, T.; Price, O.; Asgharian, B. Thoracic and respirable particle definitions for human health risk assessment. Part. Fibre Toxicol. 2013, 10, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pope, C.A., 3rd; Coleman, N.; Pond, Z.A.; Burnett, R.T. Fine particulate air pollution and human mortality: 25+ years of cohort studies. Environ. Res. 2020, 183, 108924. [Google Scholar] [CrossRef]
- Wu, X.; Zhu, B.; Zhou, J.; Bi, Y.; Xu, S.; Zhou, B. The epidemiological trends in the burden of lung cancer attributable to PM2.5 exposure in China. BMC Public Health 2021, 21, 737. [Google Scholar] [CrossRef]
- Strak, M.; Weinmayr, G.; Rodopoulou, S.; Chen, J.; de Hoogh, K.; Andersen, Z.J.; Atkinson, R.; Bauwelinck, M.; Bekkevold, T.; Bellander, T.; et al. Long term exposure to low level air pollution and mortality in eight European cohorts within the ELAPSE project: Pooled analysis. BMJ 2021, 374, n1904. [Google Scholar] [CrossRef]
- Dockery, D.W.; Pope, C.A., 3rd; Xu, X.; Spengler, J.D.; Ware, J.H.; Fay, M.E.; Ferris, B.G., Jr.; Speizer, F.E. An association between air pollution and mortality in six U.S. cities. New Engl. J. Med. 1993, 329, 1753–1759. [Google Scholar] [CrossRef] [Green Version]
- Pope, C.A., 3rd; Thun, M.J.; Namboodiri, M.M.; Dockery, D.W.; Evans, J.S.; Speizer, F.E.; Heath, C.W., Jr. Particulate air pollution as a predictor of mortality in a prospective study of U.S. adults. Am. J. Respir. Crit. Care Med. 1995, 151, 669–674. [Google Scholar] [CrossRef]
- Colonna, K.J.; Koutrakis, P.; Kinney, P.L.; Cooke, R.M.; Evans, J.S. Mortality Attributable to Long-Term Exposure to Ambient Fine Particulate Matter: Insights from the Epidemiologic Evidence for Understudied Locations. Environ. Sci. Technol. 2022, 56, 6799–6812. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Sun, Q.; Li, T.; Ren, X.; Lin, L.; Sun, M.; Duan, J.; Sun, Z. Adverse outcome pathway of fine particulate matter leading to increased cardiovascular morbidity and mortality: An integrated perspective from toxicology and epidemiology. J. Hazard. Mater. 2022, 430, 128368. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.; Lee, W.; Kim, D.; Kim, E.; Myung, W.; Kim, S.-Y.; Kim, H. Short-term PM2.5 exposure and emergency hospital admissions for mental disease. Environ. Res. 2019, 171, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Li, T.; Guo, Y.; Liu, Y.; Wang, J.; Wang, Q.; Sun, Z.; He, M.Z.; Shi, X. Estimating mortality burden attributable to short-term PM2.5 exposure: A national observational study in China. Environ. Int. 2019, 125, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Orellano, P.; Reynoso, J.; Quaranta, N.; Bardach, A.; Ciapponi, A. Short-term exposure to particulate matter (PM10 and PM2.5), nitrogen dioxide (NO2), and ozone (O3) and all-cause and cause-specific mortality: Systematic review and meta-analysis. Environ. Int. 2020, 142, 105876. [Google Scholar] [CrossRef] [PubMed]
- Sawada, N.; Nakaya, T.; Kashima, S.; Yorifuji, T.; Hanibuchi, T.; Charvat, H.; Yamaji, T.; Iwasaki, M.; Inoue, M.; Iso, H.; et al. Long-term exposure to fine particle matter and all-cause mortality and cause-specific mortality in Japan: The JPHC Study. BMC Public Health 2022, 22, 466. [Google Scholar] [CrossRef] [PubMed]
- Ciabattini, M.; Rizzello, E.; Lucaroni, F.; Palombi, L.; Boffetta, P. Systematic review and meta-analysis of recent high-quality studies on exposure to particulate matter and risk of lung cancer. Environ. Res. 2021, 196, 110440. [Google Scholar] [CrossRef]
- Khosravipour, M.; Safari-Faramani, R.; Rajati, F.; Omidi, F. The long-term effect of exposure to respirable particulate matter on the incidence of myocardial infarction: A systematic review and meta-analysis study. Environ. Sci. Pollut. Res. 2022, 29, 42347–42371. [Google Scholar] [CrossRef]
- Adamkiewicz, Ł.; Maciejewska, K.; Rabczenko, D.; Drzeniecka-Osiadacz, A. Ambient Particulate Air Pollution and Daily Hospital Admissions in 31 Cities in Poland. Atmosphere 2022, 13, 345. [Google Scholar] [CrossRef]
- Stafoggia, M.; Oftedal, B.; Chen, J.; Rodopoulou, S.; Renzi, M.; Atkinson, R.W.; Bauwelinck, M.; Klompmaker, J.O.; Mehta, A.; Vienneau, D.; et al. Long-term exposure to low ambient air pollution concentrations and mortality among 28 million people: Results from seven large European cohorts within the ELAPSE project. Lancet Planet. Health 2022, 6, e9–e18. [Google Scholar] [CrossRef]
- Heinrich, J. Air pollutants and primary allergy prevention. Allergo J. Int. 2019, 28, 5–15. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Wu, W.; Wang, G.; Zhang, X.; Guo, Q.; Wang, B.; Cao, S.; Yan, M.; Pan, X.; Xue, T.; et al. Association between exposure to air pollution and risk of allergic rhinitis: A systematic review and meta-analysis. Environ. Res. 2022, 205, 112472. [Google Scholar] [CrossRef]
- Makri, A.; Stilianakis, N.I. Vulnerability to air pollution health effects. Int. J. Hyg. Environ. Health 2008, 211, 326–336. [Google Scholar] [CrossRef] [PubMed]
- Yazdi, M.D.; Wang, Y.; Di, Q.; Wei, Y.; Requia, W.J.; Shi, L.; Sabath, M.B.; Dominici, F.; Coull, B.A.; Evans, J.S.; et al. Long-Term Association of Air Pollution and Hospital Admissions Among Medicare Participants Using a Doubly Robust Additive Model. Circulation 2021, 143, 1584–1596. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.who.int/europe/tools-and-toolkits/airq---software-tool-for-health-risk-assessment-of-air-pollution (accessed on 1 March 2022).
- Samek, L. Overall human mortality and morbidity due to exposure to air pollution. Int. J. Occup. Med. Environ. Health 2016, 29, 417–426. [Google Scholar] [CrossRef]
- De Marco, A.; Amoatey, P.; Khaniabadi, Y.O.; Sicard, P.; Hopke, P.K. Mortality and morbidity for cardiopulmonary diseases attributed to PM2.5 exposure in the metropolis of Rome, Italy. Eur. J. Intern. Med. 2018, 57, 49–57. [Google Scholar] [CrossRef]
- Pala, K.; Aykac, N.; Yasin, Y. Premature deaths attributable to long-term exposure to PM2.5 in Turkey. Environ. Sci. Pollut. Res. 2021, 28, 51940–51947. [Google Scholar] [CrossRef]
- Brito, J.; Bernardo, A.; Gonçalves, L.L. Atmospheric pollution and mortality in Portugal: Quantitative assessment of the environmental burden of disease using the AirQ+ model. Sci. Total Environ. 2022, 815, 152964. [Google Scholar] [CrossRef] [PubMed]
- Ravindra, K.; Singh, T.; Mor, S. Preventable mortality attributable to exposure to air pollution at the rural district of Punjab, India. Environ. Sci. Pollut. Res. 2022, 29, 32271–32278. [Google Scholar] [CrossRef] [PubMed]
- Orru, H.; Olstrup, H.; Kukkonen, J.; López-Aparicio, S.; Segersson, D.; Geels, C.; Tamm, T.; Riikonen, K.; Maragkidou, A.; Sigsgaard, T.; et al. Health impacts of PM2.5 originating from residential wood combustion in four nordic cities. BMC Public Health 2022, 22, 1286. [Google Scholar] [CrossRef]
- Soleimani, M.; Akbari, N.; Saffari, B.; Haghshenas, H. Health effect assessment of PM2.5 pollution due to vehicular traffic (case study: Isfahan). J. Transp. Health 2022, 24, 101329. [Google Scholar] [CrossRef]
- Moustris, K.P.; Proias, G.T.; Larissi, I.K.; Nastos, P.T.; Koukouletsos, K.V.; Paliatsos, A.G. Health impacts due to particulate air pollution in Volos City, Greece. J. Environ. Sci. Health. Part A Toxic/Hazard. Subst. Environ. Eng. 2016, 51, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Ntourou, K.; Moustris, K.P.; Giannouli, M.; Nastos, P.T.; Paliatsos, A.G. Estimation of Hospital Admissions Respiratory Disease Attributed to PM10 Exposure Using the AirQ Model Within the Greater Athens Area. In Perspectives on Atmospheric Sciences. Springer Atmospheric Sciences; Karacostas, T., Bais, A., Nastos, P., Eds.; Springer: Cham, Switzerland, 2017. [Google Scholar] [CrossRef]
- Moustris, K.P.; Ntourou, K.; Nastos, P.T. Estimation of Particulate Matter Impact on Human Health within the Urban Environment of Athens City, Greece. Urban Sci. 2017, 1, 6. [Google Scholar] [CrossRef] [Green Version]
- Touloumi, G.; Samoli, E.; Katsouyanni, K. Daily mortality and "winter type" air pollution in Athens, Greece--a time series analysis within the APHEA project. J. Epidemiology Community Health 1996, 50 (Suppl. 1), s47–s51. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Economopoulou, A.A.; Economopoulos, A.P. Air pollution in Athens basin and health risk assessment. Environ. Monit. Assess. 2002, 80, 277–299. [Google Scholar] [CrossRef]
- Tzima, K.; Analitis, A.; Katsouyanni, K.; Samoli, E. Has the risk of mortality related to short-term exposure to particles changed over the past years in Athens, Greece? Environ. Int. 2018, 113, 306–312. [Google Scholar] [CrossRef]
- Kasdagli, M.-I.; Katsouyanni, K.; de Hoogh, K.; Lagiou, P.; Samoli, E. Associations of air pollution and greenness with mortality in Greece: An ecological study. Environ. Res. 2021, 196, 110348. [Google Scholar] [CrossRef]
- Kasdagli, M.-I.; Katsouyanni, K.; de Hoogh, K.; Lagiou, P.; Samoli, E. Investigating the association between long-term exposure to air pollution and greenness with mortality from neurological, cardio-metabolic and chronic obstructive pulmonary diseases in Greece. Environ. Pollut. 2022, 292, 118372. [Google Scholar] [CrossRef]
- Paliatsos, A.G.; Nastos, T.P. Relation between air pollution episodes and discomfort index in the greater Athens area, Greece. Glob. Nest J. 1999, 1, 91–97. [Google Scholar] [CrossRef]
- Larissi, I.K.; Koukouletsos, K.V.; Moustris, K.P.; Antoniou, A.; Paliatsos, A.G. PM10 concentration levels in the Greater Athens area, Greece. Fresenius Environ. Bull. 2010, 19, 226–231. [Google Scholar]
- Sindosi, O.A.; Katsoulis, B.D.; Bartzokas, A. An objective definition of air mass types affecting athens, greece; The corresponding atmospheric pressure patterns and air pollution levels. Environ. Technol. 2003, 24, 947–962. [Google Scholar] [CrossRef] [PubMed]
- Valavanidis, A.; Vlachogianni, T.L.S.; Fiotakis, C. Atmospheric Pollution in Urban Areas of Greece and Economic Crisis. Trends in Air Quality and Atmospheric Pollution Data, Research and Adverse Health Effects; Department of Chemistry, University of Athens: Athens, Greece, 2015; Volume 1, pp. 1–27. Available online: www.chem.uoa.gr (accessed on 1 March 2022).
- Manalis, N.; Grivas, G.; Protonotarios, V.; Moutsatsou, A.; Samara, C.; Chaloulakou, A. Toxic metal content of particulate matter (PM10), within the Greater Area of Athens. Chemosphere 2005, 60, 557–566. [Google Scholar] [CrossRef] [PubMed]
- ACEA Report. Vehicles in use Europe 2022. Available online: https://www.acea.auto/files/ACEA-report-vehicles-in-use-europe-2022.pdf (accessed on 1 October 2022).
- Directive 2008/50/EC of the European Parliament and of the Council of 21 May 2008 on Ambient Air Quality and Cleaner Air for Europe. Available online: https://eur-lex.europa.eu/eli/dir/2008/50/oj?locale=en (accessed on 9 October 2022).
- Krzyzanowski, M.; Apte, J.; Bonjour, S.P.; Brauer, M.; Cohen, A.J.; Prüss-Ustun, A.M. Air Pollution in the Mega-cities. Curr. Environ. Health Rep. 2014, 1, 185–191. [Google Scholar] [CrossRef] [Green Version]
- Conti, G.O.; Heibati, B.; Kloog, I.; Fiore, M.; Ferrante, M. A review of AirQ Models and their applications for forecasting the air pollution health outcomes. Environ. Sci. Pollut. Res. 2017, 24, 6426–6445. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO Global Air Quality Guidelines: Particulate Matter (PM2.5 and PM10), Ozone, Nitrogen Dioxide, Sulfur Dioxide and Carbon Monoxide; World Health Organization: Geneva, Switzerland, 2021; Available online: https://apps.who.int/iris/handle/10665/345329 (accessed on 1 October 2022).
- Moustris, K.P.; Petraki, E.; Ntourou, K.; Priniotakis, G.; Nikolopoulos, D. Spatiotemporal Evaluation of PM10 Concentrations within the Greater Athens Area, Greece. Trends, Variability and Analysis of a 19 Years Data Series. Environments 2020, 7, 85. [Google Scholar] [CrossRef]
- Gratsea, M.; Liakakou, E.; Mihalopoulos, N.; Adamopoulos, A.; Tsilibari, E.; Gerasopoulos, E. The combined effect of reduced fossil fuel consumption and increasing biomass combustion on Athens’ air quality, as inferred from long term CO measurements. Sci. Total. Environ. 2017, 592, 115–123. [Google Scholar] [CrossRef]
- Saffari, A.; Daher, N.; Samara, C.; Voutsa, D.; Kouras, A.; Manoli, E.; Karagkiozidou, O.; Vlachokostas, C.; Moussiopoulos, N.; Shafer, M.M.; et al. Increased Biomass Burning Due to the Economic Crisis in Greece and Its Adverse Impact on Wintertime Air Quality in Thessaloniki. Environ. Sci. Technol. 2013, 47, 13313–13320. [Google Scholar] [CrossRef]
- Santamouris, M.; Paravantis, J.A.; Founda, D.; Kolokotsa, D.; Michalakakou, P.; Papadopoulos, A.M.; Kontoulis, N.; Tzavali, A.; Stigka, E.K.; Ioannidis, Z.; et al. Financial crisis and energy consumption: A household survey in Greece. Energy Build. 2013, 65, 477–487. [Google Scholar] [CrossRef]
- Vrekoussis, M.; Richter, A.; Hilboll, A.; Burrows, J.P.; Gerasopoulos, E.; Lelieveld, J.; Barrie, L.; Zerefos, C.; Mihalopoulos, N. Economic crisis detected from space: Air quality observations over Athens/Greece. Geophys. Res. Lett. 2013, 40, 458–463. [Google Scholar] [CrossRef]
- Liakakou, E.; Panopoulou, A.; Grivas, G.; Kritikou, T.; Panagopoulos, P.; Maggos, T.; Gerasopoulos, E.; Sauvage, S.; Mihalopoulos, N. Variability and sources of NMHCs at a coastal urban location in the Piraeus Port, Greece. Atmospheric Pollut. Res. 2022, 13, 101386. [Google Scholar] [CrossRef]
- Requia, W.J.; Higgins, C.; Adams, M.D.; Mohamed, M.; Koutrakis, P. The health impacts of weekday traffic: A health risk assessment of PM2.5 emissions during congested periods. Environ. Int. 2018, 111, 164–176. [Google Scholar] [CrossRef] [PubMed]
- Theodosi, C.; Grivas, G.; Zarmpas, P.; Chaloulakou, A.; Mihalopoulos, N. Mass and chemical composition of size-segregated aerosols (PM1, PM2.5, PM10) over Athens, Greece: Local versus regional sources. Atmospheric Chem. Phys. 2011, 11, 11895–11911. [Google Scholar] [CrossRef] [Green Version]
- Pateraki, S.; Asimakopoulos, D.; Maggos, T.; Vasilakos, C. Particulate matter levels in a suburban Mediterranean area: Analysis of a 53-month long experimental campaign. J. Hazard. Mater. 2010, 182, 801–811. [Google Scholar] [CrossRef]
- Mavrakis, A.; Lykoudis, S.; Christides, A.; Dasaklis, S.; Tasopoulos, A.; Theoharatos, G.; Kyvelou, S.; Verouti, E. Air quality levels in a closed industrialized basin (Thriassion Plain, Greece). Fresenius Environ. Bull. 2008, 17, 443–454. [Google Scholar]
- GBD 2016 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1345–1422. [Google Scholar] [CrossRef] [Green Version]
- Kotsiou, O.S.; Zouridis, S.; Kosmopoulos, M.; Gourgoulianis, K.I. Impact of the financial crisis on COPD burden: Greece as a case study. Eur. Respir. Rev. 2018, 27, 170106. [Google Scholar] [CrossRef] [Green Version]
- Syrigos, K.N.; Georgoulias, V.; Zarogoulidis, K.; Makrantonakis, P.; Charpidou, A.; Christodoulou, C. Epidemiological Characteristics,EGFRStatus and Management Patterns of Advanced Non-small Cell Lung Cancer Patients: The Greek REASON Observational Registry Study. Anticancer Res. 2018, 38, 3735–3744. [Google Scholar] [CrossRef]
- Katsouyanni, K.; Trichopoulos, D.; Kalandidi, A.; Tomos, P.; Riboli, E. A case-control study of air pollution and tobacco smoking in lung cancer among women in Athens. Prev. Med. 1991, 20, 271–278. [Google Scholar] [CrossRef]
- Michas, G.; Karvelas, G.; Trikas, A. Cardiovascular disease in Greece; the latest evidence on risk factors. Hell. J. Cardiol. HJC = Hell. Kardiol. Ep. 2019, 60, 271–275. [Google Scholar] [CrossRef]
- Lackland, D.T.; Roccella, E.J.; Deutsch, A.; Fornage, M.; George, M.G.; Howard, G.; Kissela, B.M.; Kittner, S.J.; Lichtman, J.H.; Lisabeth, L.D.; et al. Factors influencing the decline in stroke mortality: A statement from the American Heart Association/American Stroke Association. Stroke 2014, 45, 315–353. [Google Scholar] [CrossRef] [Green Version]
- Karantali, E.; Vemmos, K.; Tsampalas, E.; Xynos, K.; Karachalia, P.; Lambrou, D.; Angeloglou, S.; Kazakou, M.; Karagianni, A.; Aravantinou-Fatorou, K.; et al. Temporal trends in stroke incidence and case-fatality rates in Arcadia, Greece: A sequential, prospective, population-based study. Int. J. Stroke 2022, 17, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Amoatey, P.; Sicard, P.; De Marco, A.; Khaniabadi, Y.O. Long-term exposure to ambient PM2.5 and impacts on health in Rome, Italy. Clin. Epidemiology Glob. Health 2010, 8, 531–535. [Google Scholar] [CrossRef] [Green Version]
- Todorović, M.N.; Radenković, M.B.; Rajšić, S.F.; Ignjatović, L.M. Evaluation of mortality attributed to air pollution in the three most populated cities in Serbia. Int. J. Environ. Sci. Technol. 2019, 16, 7059–7070. [Google Scholar] [CrossRef]
- Rovira, J.; Domingo, J.L.; Schuhmacher, M. Air quality, health impacts and burden of disease due to air pollution (PM10, PM2.5, NO2 and O3): Application of AirQ+ model to the Camp de Tarragona County (Catalonia, Spain). Sci. Total. Environ. 2020, 703, 135538. [Google Scholar] [CrossRef] [PubMed]
- Prabhu, V.; Singh, P.; Kulkarni, P.; Sreekanth, V. Characteristics and health risk assessment of fine particulate matter and surface ozone: Results from Bengaluru, India. Environ. Monit. Assess. 2022, 194, 211. [Google Scholar] [CrossRef] [PubMed]
- Hopke, P.K.; Nazari, S.S.H.; Hadei, M.; Yarahmadi, M.; Kermani, M.; Yarahmadi, E.; Shahsavani, A. Spatial and Temporal Trends of Short-Term Health Impacts of PM2.5 in Iranian Cities—A Modelling Approach (2013–2016). Aerosol Air Qual. Res. 2018, 18, 497–504. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| AQMS Name | Geographical Coordinates | Height (m a.s.l.) * | Zone/Station Type |
|---|---|---|---|
| ARI (Aristotelous) | 37,988066 | 75 | Urban-Traffic |
| 23,727617 | |||
| LYK (Lykovrisi) | 38,067793 | 234 | Suburban-Background |
| 23,788986 | |||
| PIR (Piraeus) | 37,944656 | 4 | Urban-Traffic |
| 23,645230 | |||
| AGP (Agia Paraskevi) | 37,995110 | 290 | Suburban-Background |
| 23,819421 | |||
| ELE (Elefsina) | 38,051322 | 20 | Suburban-Industrial |
| 23,538432 | |||
| THR (Thrakomakedones) | 38,143521 | 550 | Suburban-Background |
| 23,758195 |
| Health Outcome Definition | ICD-10 Classification Codes Included |
|---|---|
| Mortality, all (natural) causes (adults 30+) | A00-R99 |
| Mortality, Chronic Obstructive Pulmonary Disease (COPD) (adults 30+) | J40-J47 |
| Mortality, Ischemic Heart Disease (IHD) (adults 25+) | I20-I25 |
| Mortality, Lung Cancer (LC) (adults 25+) | C33-C34 |
| Mortality, Stroke (adults 25+) | I60-I69 |
| Year | PM2.5-PIR | PM2.5-AGP | PM2.5-LYK | PM2.5-THR | PM2.5-ARI | PM2.5-ELE |
|---|---|---|---|---|---|---|
| 2007 | 37.26 ± 15.27 | 19.69 ± 9.69 | 32.80 ± 16.64 | - | - | - |
| 2008 | 28.52 ± 12.82 | 19.10 ± 7.72 | 29.54 ± 12.15 | - | - | - |
| 2009 | 27.56 ± 11.42 | 15.95 ± 7.87 | 24.09 ± 10.01 | - | - | - |
| 2010 | 22.21 ± 8.22 | 14.56 ± 7.81 * | 22.59 ± 9.63 | - | - | - |
| 2011 | 26.59 ± 11.31 * | 17.02 ± 5.71 | 20.41 ± 8.79 | - | - | - |
| 2012 | 23.42 ± 10.66 * | 14.61 ± 4.60 | 22.11 ± 10.03 | - | - | - |
| 2013 | 24.89 ± 7.76 * | 10.02 ± 3.79 | 11.79 ± 7.59 * | - | - | - |
| 2014 | 19.83 ± 8.78 | 11.18 ± 5.55 * | 15.73 ± 7.28 * | - | - | - |
| 2015 | 21.23 ± 14.50 | 10.35 ± 4.60 | 16.49 ± 13.96 | 12.80 ± 4.05 | 19.64 ± 15.20 | 16.06 ± 7.89 |
| 2016 | 20.07 ± 10.64 | 12.23 ± 5.99 | 17.24 ± 9.86 | 12.91 ± 6.09 | 19.98 ± 11.49 | 21.24 ± 8.76 |
| 2017 | 17.96 ± 9.79 | 10.72 ± 3.92 | 16.42 ± 9.20 | 12.73 ± 4.46 | 19.49 ± 10.41 | 16.32 ± 6.23 |
| 2018 | 18.03 ± 8.97 | 11.58 ± 5.30 | 15.28 ± 7.81 | 13.44 ± 5.19 | 19.03 ± 9.91 | 17.84 ± 7.28 |
| Mortality, All-Natural Causes (30+ Years Old) | Study Year | |
|---|---|---|
| 2007 | 2018 | |
| Population at risk | 2,716,931 | 2,562,652 |
| Baseline incidence | 34,164 | 38,194 |
| Estimated attributable proportion (at the total population) | 13.91% [9.30–18.01%] | 6.35% [4.18–8.32%] |
| Estimated number of attributable cases (at the total population) | 4752 [3179–6152] | 2424 [1598–3179] |
| Estimated number of attributable cases (per 100,000 population at risk) | 174.92 [117.00–226.43] | 94.59 [62.37–124.06] |
| Mortality, Chronic Obstructive Pulmonary Disease (COPD) (25+ years old) | Study year | |
| 2007 | 2018 | |
| Population at risk | 3,004,475 | 2,833,868 |
| Baseline incidence | 630 | 916 |
| Estimated attributable proportion | 23.22% [12.60–34.93%] | 16.07% [6.92–26.62%] |
| Estimated number of attributable cases (at the total population) | 146 [79–220] | 147 [63–244] |
| Estimated number of attributable cases (per 100,000 population at risk) | 4.87 [2.64–7.33] | 5.20 [2.24–8.60] |
| Mortality, Lung Cancer (LC) (25+ years old) | Study year | |
| 2007 | 2018 | |
| Population at risk | 3,004,475 | 2,833,868 |
| Baseline incidence | 2010 | 2472 |
| Estimated attributable proportion | 16.28% [9.39–23.71%] | 9.63% [4.91–15.4%] |
| Estimated number of attributable cases (at the total population) | 327 [189–477] | 238 [121–381] |
| Estimated number of attributable cases (per 100,000 population at risk) | 10.89 [6.28–15.86] | 8.40 [4.28–13.43] |
| Mortality, Ischemic Heart Disease (IHD) (25+ years old) | Study year | |
| 2007 | 2018 | |
| Population at risk | 3,004,475 | 2,833,868 |
| Baseline incidence | 4573 | 5062 |
| Estimated attributable proportion | 20.89% [10.71–30.90] | 16.93% [7.66–25.95] |
| Estimated number of attributable cases (at the total population) | 765 [391–1154] | 622 [284–979] |
| Estimated number of attributable cases (per 100,000 population at risk) | 25.46 [13.01–38.41] | 21.95 [10.02–34.55] |
| Mortality, Stroke (25+ years old) | Study year | |
| 2007 | 2018 | |
| Population at risk | 3,004,475 | 2,833,868 |
| Baseline incidence | 4425 | 3560 |
| Estimated attributable proportion | 16.53% [7.19–26.56] | 15.07% [4.17–23.17] |
| Estimated number of attributable cases (at the total population) | 486 [202–845] | 291 [89–602] |
| Estimated number of attributable cases (per 100,000 population at risk) | 16.18 [6.72–28.12] | 10.27 [3.14–21.24] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Begou, P.; Kassomenos, P. Burden of Natural-Cause and Cause-Specific Mortality Associated with Long-Term Exposure to PM2.5: A Case Study in Attica Region, Greece. Atmosphere 2022, 13, 2026. https://doi.org/10.3390/atmos13122026
Begou P, Kassomenos P. Burden of Natural-Cause and Cause-Specific Mortality Associated with Long-Term Exposure to PM2.5: A Case Study in Attica Region, Greece. Atmosphere. 2022; 13(12):2026. https://doi.org/10.3390/atmos13122026
Chicago/Turabian StyleBegou, Paraskevi, and Pavlos Kassomenos. 2022. "Burden of Natural-Cause and Cause-Specific Mortality Associated with Long-Term Exposure to PM2.5: A Case Study in Attica Region, Greece" Atmosphere 13, no. 12: 2026. https://doi.org/10.3390/atmos13122026