
The Impact of Atmospheric Pollutants on Human Health and Economic Loss Assessment


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sampling Sites and Sample Collection
2.2. Sample Analysis
2.2.1. Statistical Descriptive Analysis
2.2.2. Time Series Analysis
2.2.3. Generalized Additive Model
2.3. Methodology of Economic Loss Assessment—Attributable Risk and Cost of Illness Approach
3. Results
3.1. Statistical Description of Admission Data for Respiratory Diseases and Air Pollution Concentrations
3.1.1. Characteristics of Numbers of Hospital Admissions for Respiratory Diseases
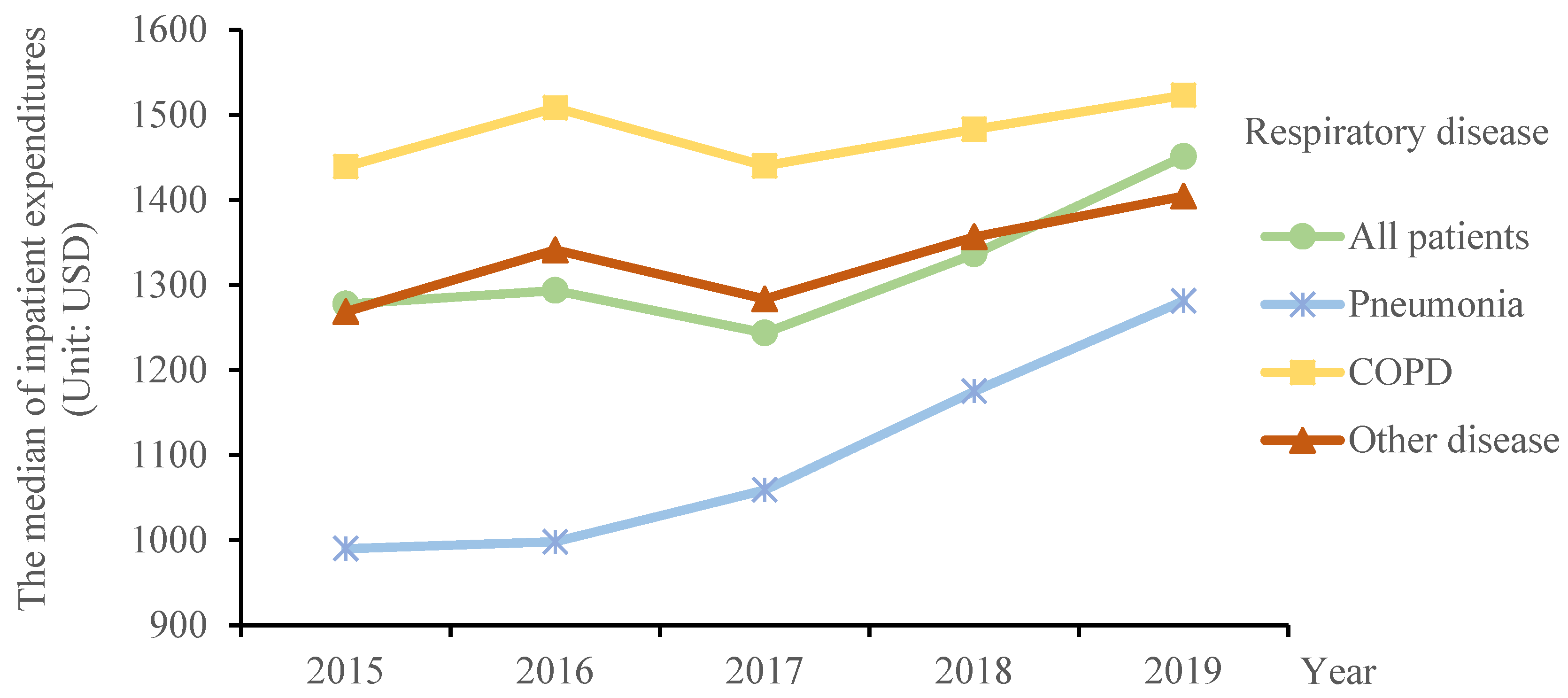
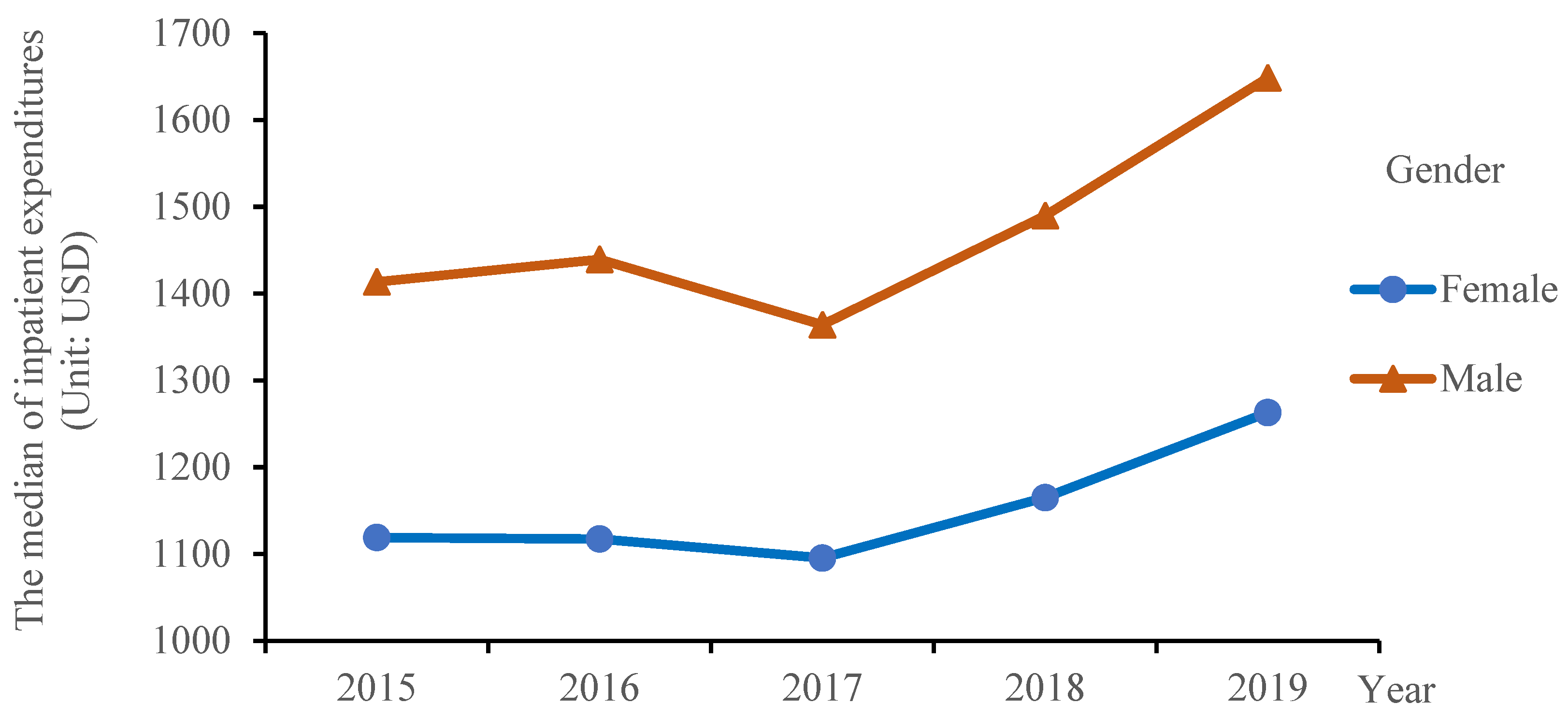
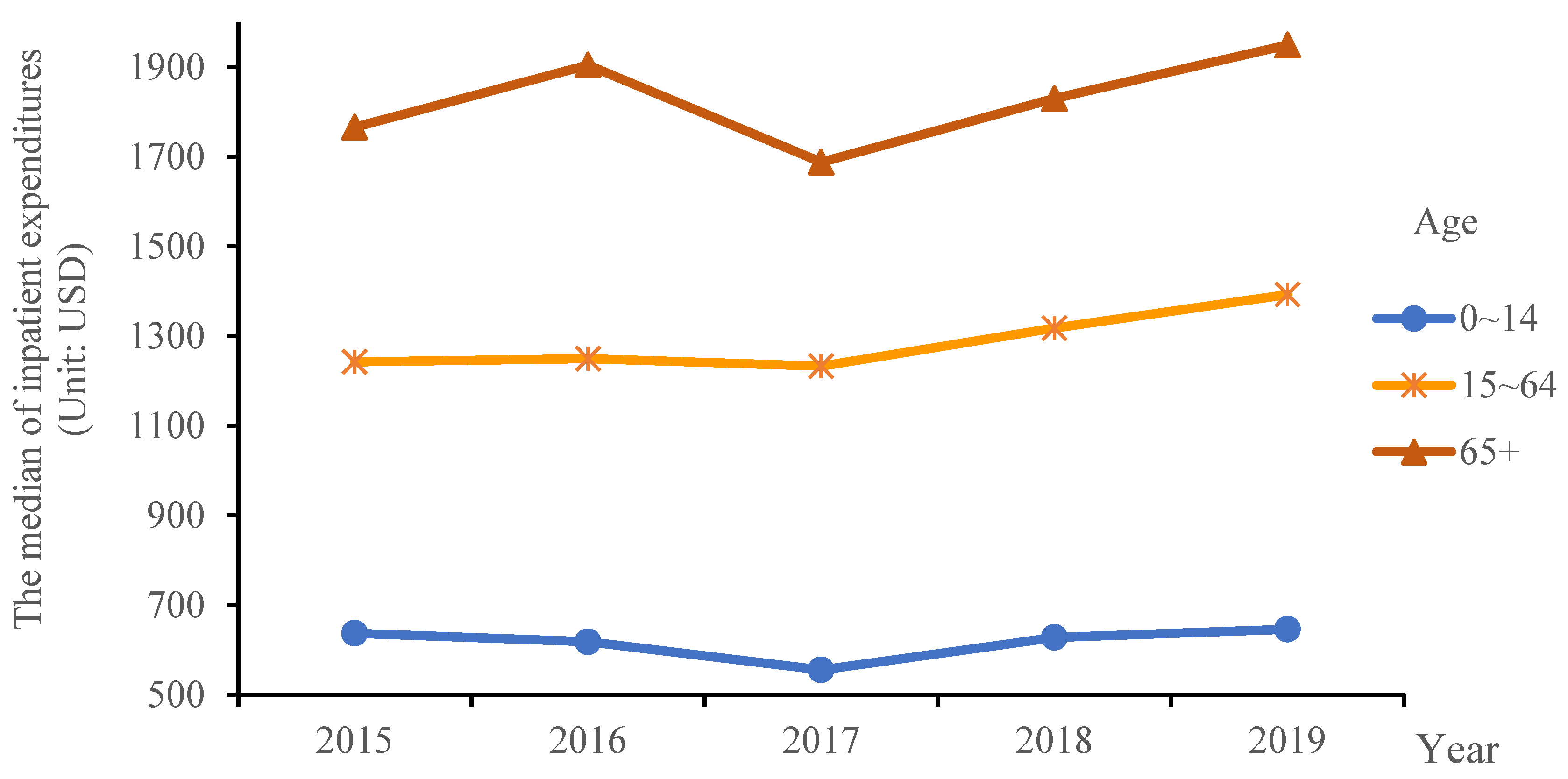
3.1.2. Characteristics of Inpatient Expenditure for Respiratory Diseases
3.1.3. Characteristics of Length of Stay for Respiratory Diseases
3.1.4. Characteristics of Changes in Air Pollutants
3.2. Quantitative Analysis of the Impact of Air Pollutants on Hospital Admissions for Respiratory Diseases
3.3. Assessment of Economic Losses
3.3.1. Analysis Results of Attributable Risk
3.3.2. Results of Economic Loss Assessment
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Technical Regulation on Ambient Air Quality Index (on Trial) (HJ 633—2012). Available online: https://www.mee.gov.cn/ywgz/fgbz/bz/bzwb/jcffbz/201203/t20120302_224166.shtml (accessed on 20 November 2021).
- Stanaway, J.D.; Afshin, A.; Gakidou, E.; Lim, S.S.; Abate, D.; Abate, K.H.; Abbafati, C.; Abbasi, H.; Abbastabar, H.; Abd-Allah, F.; et al. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1923–1994. [Google Scholar] [CrossRef] [Green Version]
- Lamichhane, D.K.; Kim, H.C.; Choi, C.M.; Shin, M.H.; Shim, Y.M.; Leem, J.H.; Ryu, J.S.; Nam, H.S.; Park, S.M. Lung Cancer Risk Resid. Expo. To air pollution: A Korean population-based case-control study. Yonsei Med. J. 2017, 58, 1111–1118. [Google Scholar] [CrossRef]
- Abdo, N.; Khader, Y.S.; Abdelrahman, M.; Graboski-Bauetr, A.; Malkawi, M.; Al-Sharif, M.; Elbetieha, A.M. Respiratory health outcomes and air pollution in the Eastern Mediterranean Region: A systematic review. Rev. Environ. Health 2016, 31, 259–280. [Google Scholar] [CrossRef] [PubMed]
- Soriano, J.B.; Kendrick, P.J.; Paulson, K.R.; Gupta, V.; Abrams, E.M.; Adedoyin, R.A.; Adhikari, T.B.; Advani, S.M.; Agrawal, A.; Ahmadian, E.; et al. Prevalence and attributable health burden of chronic respiratory diseases 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet Respir. Med. 2020, 8, 585–596. [Google Scholar] [CrossRef]
- Kyu, H.H.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national disability-adjusted life-years (DALYs) for 359 diseases and injuries and healthy life expectancy (HALE) for 195 countries and territories, 1990-2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1859–1922. [Google Scholar] [CrossRef] [Green Version]
- China Statistic Yearbook 2021. Available online: http://www.stats.gov.cn/tjsj/ndsj/2021/indexch.htm (accessed on 15 September 2021).
- Ma, Y.; Xiao, B.; Liu, C.; Zhao, Y.; Zheng, X. Association between ambient air pollution and emergency room visits for respiratory diseases in spring dust storm season in Lanzhou, China. Int. J. Environ. Res. Public Health 2016, 13, 613. [Google Scholar] [CrossRef]
- Dong, J.; Liu, Y.; Bao, H. Revalue associations of short-term exposure to air pollution with respiratory hospital admissions in Lanzhou, China after the control and treatment of current pollution. Int. J. Hyg. Environ. Health 2021, 231, 113658. [Google Scholar] [CrossRef] [PubMed]
- Yao, M.; Wu, G.; Zhao, X.; Zhang, J. Estimating health burden and economic loss attributable to short-term exposure to multiple air pollutants in China. Environ. Res. 2020, 183, 109184. [Google Scholar] [CrossRef]
- Mamkhezri, J.; Bohara, A.K.; Camargo, A.I. Air pollution and daily mortality in Mexico city Metropolitan area. Atmosfera 2019, 33, 249–267. [Google Scholar] [CrossRef]
- Afghan, F.R.; Patidar, S.K. Health impacts assessment due to PM2.5, PM10 and NO2 exposure in National Capital Territory (NCT). Pollution 2020, 6, 115–126. [Google Scholar] [CrossRef]
- Hwang, J.; Kwon, J.; Yi, H.; Bae, H.-J.; Jang, M.; Kim, N. Association between long-term exposure to air pollutants and cardiopulmonary mortality rates in South Korea. BMC Public Health 2020, 20, 1402–1410. [Google Scholar] [CrossRef]
- Hansel, N.N.; Paulin, L.M.; Gassett, A.J.; Peng, R.D.; Alexis, N.; Fan, V.S.; Bleecker, E.; Bowler, R.; Comellas, A.P.; Dransfield, M.; et al. Design of the Subpopulations and Intermediate Outcome Measures in COPD (SPIROMICS) AIR Study. BMJ Open Respir. Res. 2017, 4, e186. [Google Scholar] [CrossRef]
- Li, G.; Huang, J.; Xu, G.; Pan, X.; Qian, X.; Xu, J.; Zhao, Y.; Zhang, T.; Liu, Q.; Guo, X.; et al. The short-term burden of ambient fine particulate matter on chronic obstructive pulmonary disease in Ningbo, China. Environ. Health 2017, 16, 54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Z.; Chai, P.; Wang, J.; Ye, Z.; Shen, P.; Lu, H.; Jin, M.; Gu, M.; Li, D.; Lin, H.; et al. Association of particulate matter air pollution and hospital visits for respiratory diseases: A time-series study from China. Environ. Sci. Pollut. Res. Int. 2019, 26, 12280–12287. [Google Scholar] [CrossRef]
- Luo, L.; Zhang, Y.; Jiang, J.; Luan, H.; Yu, C.; Nan, P.; Luo, B.; You, M. Short-Term effects of ambient air pollution on hospitalization for respiratory disease in Taiyuan, China: A time-series analysis. Int. J. Environ. Res. Public Health 2018, 15, 2160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Q.; Chen, Y.; Krewski, D.; Burnett, R.T.; Shi, Y.; McGrail, K.M. Effect of short-term exposure to low levels of gaseous pollutants on chronic obstructive pulmonary disease hospitalizations. Environ. Res. 2005, 99, 99–105. [Google Scholar] [CrossRef]
- Cadelis, G.; Tourres, R.; Molinie, J. Short-Term effects of the particulate pollutants contained in saharan dust on the visits of children to the emergency department due to asthmatic conditions in guadeloupe (French archipelago of the Caribbean). PLoS ONE 2014, 9, e91136. [Google Scholar] [CrossRef] [Green Version]
- Akpinar-Elci, M.; Martin, F.E.; Behr, J.G.; Diaz, R. Saharan dust, climate variability, and asthma in Grenada, the Caribbean. Int. J. Biometeorol. 2015, 59, 1667–1671. [Google Scholar] [CrossRef]
- Guarnieri, M.; Balmes, J.R. Outdoor air pollution and asthma. Lancet 2014, 383, 1581–1592. [Google Scholar] [CrossRef] [Green Version]
- Zhao, Y.; Hu, J.; Tan, Z.; Liu, T.; Zeng, W.; Li, X.; Huang, C.; Wang, S.; Huang, Z.; Ma, W. Ambient carbon monoxide and increased risk of daily hospital outpatient visits for respiratory diseases in Dongguan, China. Sci. Total Environ. 2019, 668, 254–260. [Google Scholar] [CrossRef]
- Moore, K.; Neugebauer, R.; Lurmann, F.; Hall, J.; Brajer, V.; Alcorn, S.; Tager, I. Ambient ozone concentrations cause increased hospitalizations for asthma in children: An 18-year study in southern California. Environ. Health Perspect. 2008, 116, 1063–1070. [Google Scholar] [CrossRef] [Green Version]
- Clark, N.A.; Demers, P.A.; Karr, C.J.; Koehoorn, M.; Lencar, C.; Tamburic, L.; Brauer, M. Effect of early life exposure to air pollution on development of childhood asthma. Environ. Health Perspect. 2010, 118, 284–290. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, H.; Gao, Z.; Ren, J.; Chang, L.T.-C.; Cheung, K.; Feng, Y.; Li, Y. An urban-rural and sex differences in cancer incidence and mortality and the relationship with PM2.5 exposure: An ecological study in the southeastern side of Hu line. Chemosphere 2019, 216, 766–773. [Google Scholar] [CrossRef] [PubMed]
- Katanoda, K.; Sobue, T.; Satoh, H.; Tajima, K.; Suzuki, T.; Nakatsuka, H.; Takezaki, T.; Nakayama, T.; Nitta, H.; Tanabe, K.; et al. An Association between long-term exposure to ambient air pollution and mortality from lung cancer and respiratory diseases in Japan. J. Epidemiol. 2011, 21, 132–143. [Google Scholar] [CrossRef] [Green Version]
- Nyberg, F.; Gustavsson, P.; Järup, L.; Bellander, T.; Berglind, N.; Jakobsson, R.; Pershagen, G. Urban air pollution and lung cancer in Stockholm. Epidemiology 2000, 11, 487–495. [Google Scholar] [CrossRef]
- Nsoh, M.; Mankollo, B.O.Y.; Ebongue, M.; Cyprien, K.N.; Likeng, J.L.N.; Islam, S.M.S.; Collier, A.; Tsoka-Gwegweni, J.M.; Cumber, S.N. Acute respiratory infection related to air pollution in Bamenda, North West Region of Cameroon. Pan. Afr. Med. J. 2019, 32, 1–8. [Google Scholar] [CrossRef]
- Zheng, P.W.; Wang, J.B.; Zhang, Z.Y.; Shen, P.; Chai, P.-F.; Li, D.; Jin, M.-J.; Tang, M.-L.; Lu, H.-C.; Lin, H.-B.; et al. Air pollution and hospital visits for acute upper and lower respiratory infections among children in Ningbo, China: A time-series analysis. Environ. Sci. Pollut. Res. 2017, 24 (Suppl. 4), 1–10. [Google Scholar] [CrossRef]
- Nhung, N.T.T.; Schindler, C.; Dien, T.M.; Probst-Hensch, N.; Künzli, N. Association of ambient air pollution with lengths of hospital stay for hanoi children with acute lower-respiratory infection, 2007–2016. Environ. Pollut. 2019, 247, 752–762. [Google Scholar] [CrossRef]
- Department of Ecology and Environment of Hubei Province. Available online: http://sthjt.hubei.gov.cn (accessed on 5 September 2021).
- China Meteorological Data Sharing Service System. Available online: http://data.cma.cn (accessed on 8 September 2021).
- Wu, Z.; Chen, X.; Li, G.; Tian, L.; Wang, Z.; Xiong, X.; Yang, C.; Zhou, Z.; Pan, X. Attributable risk and economic cost of hospital admissions for mental disorders due to PM2.5 in Beijing. Sci. Total Environ. 2020, 718, 137274. [Google Scholar] [CrossRef]
- Kennelly, B. How should cost-of-illness studies be interpreted? Lancet Psychiatry 2017, 4, 735–736. [Google Scholar] [CrossRef] [Green Version]
- Zhang, P.; Zhou, X. Health and economic impacts of particulate matter pollution on hospital admissions for mental disorders in Chengdu, Southwestern China. Sci. Total Environ. 2020, 733, 139114. [Google Scholar] [CrossRef] [PubMed]
- National Bureau of Statistics. Available online: http://www.stats.gov.cn/ (accessed on 10 September 2021).




{kind=link}
{kind=link}
{kind=link}
| Year | GDP Indicator (1978 = 100) | GDP Deflator * |
|---|---|---|
| 2015 | 3035.9 | 1.294 |
| 2016 | 3243.5 | 1.211 |
| 2017 | 3468.8 | 1.133 |
| 2018 | 3703.0 | 1.061 |
| 2019 | 3929.2 | 1.000 |
| Variable | n (%) |
|---|---|
| Gender | |
| Male | 27,725 (60.67) |
| Female | 17,974 (39.33) |
| Age (years) | |
| 0~14 | 8340 (18.26) |
| 15~64 | 17,074 (37.39) |
| 65+ | 20,285 (44.42) |
| Disease subgroups | |
| Pneumonia | 10,724 (23.47) |
| COPD | 11,517 (25.20) |
| Other diseases | 23,458 (51.33) |
| Variable | Pneumonia (n = 10,724) | COPD (n = 11,517) | Others (n = 23,458) | |||
|---|---|---|---|---|---|---|
| Cases | Percentage (%) | Cases | Percentage (%) | Cases | Percentage (%) | |
| Gender | ||||||
| Male | 6019 | 56.13 | 8154 | 70.80 | 13,552 | 57.77 |
| Female | 4705 | 43.87 | 3363 | 29.20 | 9906 | 42.23 |
| Age (years) | ||||||
| 0~14 | 3532 | 32.94 | 0 | 0.00 | 4808 | 20.50 |
| 15~64 | 3001 | 27.98 | 3138 | 27.25 | 10,935 | 46.62 |
| 65+ | 4191 | 39.08 | 8379 | 72.75 | 7715 | 32.89 |
| Variable | Min 1 | P25 2 | P50 3 | P75 4 | Max 5 | |
|---|---|---|---|---|---|---|
| All inpatients | 25.05 ± 12.07 | 0 | 16 | 24 | 33 | 77 |
| Disease subgroups | ||||||
| Pneumonia | 5.87 ± 3.87 | 0 | 3 | 5 | 8 | 23 |
| COPD | 6.31 ± 3.57 | 0 | 4 | 6 | 8 | 30 |
| Gender | ||||||
| Male | 15.18 ± 7.84 | 0 | 10 | 15 | 20 | 49 |
| Female | 9.84 ± 5.29 | 0 | 6 | 9 | 13 | 36 |
| Age (years) | ||||||
| 0~14 | 4.62 ± 3.13 | 0 | 2 | 4 | 6 | 20 |
| 15~64 | 9.41 ± 5.34 | 0 | 5 | 8 | 13 | 32 |
| 65+ | 11.11 ± 6.08 | 0 | 7 | 10 | 15 | 53 |
| Season | ||||||
| Cold season | 24.52 ± 13.28 | 0 | 15 | 24 | 33 | 77 |
| Warm season | 25.58 ± 10.74 | 0 | 18 | 25 | 32 | 67 |
| Variable | Min 1 | P25 2 | P50 3 | P75 4 | Max 5 | |
|---|---|---|---|---|---|---|
| All inpatients | 2370.76 ± 967.37 | 1.29 | 774.49 | 1334.18 | 2489.42 | 142,717.11 |
| Disease subgroups | ||||||
| Pneumonia | 2286 ± 2230.45 | 12.04 | 705.73 | 1131.18 | 2258.07 | 98,337.68 |
| COPD | 2390.32 ± 1492.43 | 1.86 | 1045.09 | 1486.65 | 2538.34 | 79,745.31 |
| Gender | ||||||
| Male | 2655.08 ± 1374.98 | 1.29 | 825.82 | 1488.00 | 2818.49 | 142,717.11 |
| Female | 1930.95 ± 1261.26 | 1.29 | 723.32 | 1162.77 | 2019.55 | 93,152.57 |
| Age (years) | ||||||
| 0~14 | 680.03 ± 417.34 | 11.19 | 514.12 | 622.33 | 789.19 | 10,817.72 |
| 15~64 | 2121.07 ± 1560.15 | 1.86 | 830.85 | 1296.84 | 2173.50 | 92,695.38 |
| 65+ | 3234.6 ± 1912.49 | 1.29 | 1163.24 | 1843.32 | 3715.42 | 142,717.11 |
| Season | ||||||
| Cold season | 2364.84 ± 1024.72 | 2.48 | 1719.98 | 2200.55 | 2786.48 | 98,337.68 |
| Warm season | 1711.03 ± 929.33 | 1.29 | 1043.22 | 1613.34 | 2248.95 | 142,717.11 |
| Variable | Min 1 | P25 2 | P50 3 | P75 4 | Max 5 | |
|---|---|---|---|---|---|---|
| All inpatients | 9.31 ± 2.27 | 1 | 8 | 9 | 10 | 350 |
| Disease subgroups | ||||||
| Pneumonia | 8.68 ± 4.99 | 1 | 7 | 8 | 10 | 180 |
| COPD | 10.17 ± 3.57 | 1 | 8 | 10 | 12 | 130 |
| Gender | ||||||
| Male | 9.79 ± 3.17 | 1 | 8 | 9 | 11 | 76 |
| Female | 8.52 ± 2.73 | 1 | 7 | 8 | 10 | 39 |
| Age (years) | ||||||
| 0~14 | 4.63 ± 2.08 | 1 | 4 | 5 | 6 | 39 |
| 15~64 | 8.50 ± 4.63 | 1 | 7 | 8 | 9 | 350 |
| 65+ | 11.53 ± 3.39 | 1 | 10 | 11 | 13 | 197 |
| Season | ||||||
| Cold season | 9.38 ± 2.54 | 1 | 8 | 9 | 10 | 350 |
| Warm season | 9.26 ± 1.93 | 1 | 8 | 9 | 10 | 191 |
| Air Pollutants | Min 1 | P25 2 | P50 3 | P75 4 | Max 5 | |
|---|---|---|---|---|---|---|
| PM2.5 (μg/m3) | 54.07 ± 34.99 | 4 | 30 | 46 | 67 | 281 |
| PM10 (μg/m3) | 87.32 ± 47.75 | 3 | 53 | 81 | 112 | 618 |
| SO2 (μg/m3) | 11.24 ± 7.66 | 2 | 6 | 9 | 14 | 74 |
| NO2 (μg/m3) | 44.97 ± 18.94 | 11 | 30 | 42 | 56 | 119 |
| O3 (μg/m3) | 92.83 ± 53.51 | 4 | 53 | 85 | 122 | 281 |
| CO (mg/m3) | 1.020 ± 0.301 | 0.416 | 0.810 | 0.990 | 1.170 | 2.672 |
| Pollutants | Average Time | Concentration Value | Concentration Unit | |
|---|---|---|---|---|
| Level One | Level Two | |||
| PM2.5 | Annual average | 15 | 35 | μg/m3 |
| Daily average | 35 | 75 | ||
| PM10 | Annual average | 40 | 70 | |
| Daily average | 50 | 150 | ||
| SO2 | Annual average | 20 | 60 | |
| Daily average | 50 | 150 | ||
| NO2 | Annual average | 40 | 40 | |
| Daily average | 80 | 80 | ||
| O3 | Eight hour average | 100 | 160 | |
| CO | Daily average | 4 | 4 | mg/m3 |
| Variable | PM2.5 | PM10 | SO2 | NO2 | O3 | CO |
|---|---|---|---|---|---|---|
| All inpatients | Lag7 (0.0017) | Lag7 (0.0007) | Lag7 (0.0080) | Lag6 (0.0008) | - | Lag7 (0.0001) |
| Disease Subgroups | ||||||
| Pneumonia | Lag7 (0.0021) | Lag7 (0.0008) | Lag7 (0.0125) | Lag6 (0.0020) | Lag1 (0.0008) | - |
| COPD | Lag7 (0.0019) | - | Lag1 (0.0063) | - | - | Lag7 (0.0002) |
| Gender | ||||||
| Male | Lag7 (0.0020) | Lag7 (0.0009) | Lag7 (0.0100) | Lag7 (0.0011) | Lag6 (0.0005) | Lag7 (0.0001) |
| Female | Lag7 (0.0013) | Lag7 (0.0005) | Lag2 (0.0069) | - | - | Lag7 (0.0001) |
| Age (years) | ||||||
| 0~14 | Lag7 (0.0026) | Lag7 (0.0009) | Lag7 (0.0163) | Lag6 (0.0018) | - | - |
| 15~64 | Lag7 (0.0015) | Lag7 (0.0006) | Lag3 (0.0086) | - | - | Lag7 (0.0001) |
| 65+ | Lag7 (0.0014) | Lag7 (0.0008) | Lag7 (0.0074) | Lag7 (0.0011) | Lag4 (0.0006) | Lag7 (0.0002) |
| Variable | PM2.5 | PM10 | SO2 | NO2 | O3 | CO |
|---|---|---|---|---|---|---|
| Attributable Fraction (%, 95% CI) | ||||||
| All inpatients | 8.50 (6.54, 10.40) | 5.81 (3.73, 7.82) | 8.80 (5.80, 10.27) | 3.33 (0.57, 6.00) | - | 11.73 (3.42, 19.27) |
| Disease Subgroups | ||||||
| Pneumonia | 10.19 (6.18, 13.97) | 6.60 (2.47, 10.51) | 11.84 (7.35, 16.04) | 8.35 (3.01, 13.34) | 6.29 (0.34, 11.76) | - |
| COPD | 9.91 (6.05, 13.55) | - | 6.81 (2.15, 11.15) | - | - | 16.05 (8.01, 23.33) |
| Gender | ||||||
| Male | 9.70 (7.24, 12.07) | 7.10 (4.51, 9.60) | 9.95 (7.13, 12.66) | 4.83 (1.32, 8.20) | 4.29 (0.59, 7.80) | 12.76 (7.40, 17.79) |
| Female | 6.50 (3.22, 9.62) | 4.05 (0.59, 7.36) | 7.10 (3.36, 10.63) | - | - | 8.78 (1.68, 15.32) |
| Age (years) | ||||||
| 0~14 | 12.11 (7.79, 16.16) | 6.98 (2.34, 11.34) | 15.18 (10.22, 19.77) | 7.64 (1.47, 13.36) | - | - |
| 15~64 | 7.53 (4.21, 10.70) | 4.55 (0.99, 7.95) | 8.74 (4.94, 12.34) | - | - | 12.99 (6.05, 19.38) |
| 65+ | 7.42 (4.40, 10.32) | 6.40 (3.27, 9.41) | 7.75 (4.32, 11.01) | 4.82 (0.68, 8.76) | 4.95 (0.71, 8.94) | 9.79 (3.28, 15.83) |
| Attributable Number (1000 cases, 95% CI) | ||||||
| All inpatients | 37.6 (28.9, 46.) | 25.7 (16.5, 34.6) | 35.7 (25.7, 45.4) | 14.7 (2.5, 26.5) | - | 51.8 (15.1, 85.2) |
| Disease Subgroups | ||||||
| Pneumonia | 8.8 (6.4, 14.5) | 6.8 (2.6, 10.9) | 12.3 (7.6, 16.6) | 8.7 (3.1, 13.8) | 6.5 (0.4, 12.2) | - |
| COPD | 9.5 (6.7, 15.1) | - | 7.6 (2.4, 12.4) | - | - | 17.9 (8.9, 26.0) |
| Gender | ||||||
| Male | 22.8 (19.4, 32.4) | 19.0 (12.1, 25.8) | 26.7 (19.1, 33.9) | 13.0 (3.5, 22.) | 11.5 (1.6, 20.9) | 34.2 (19.8, 47.7) |
| Female | 14.8 (5.6, 16.7) | 7.0 (1, 12.8) | 12.3 (5.8, 18.5) | - | - | 15.3 (2.9, 26.6) |
| Age (years) | ||||||
| 0~14 | 6.9 (6.4, 13.2) | 5.7 (1.9, 9.2) | 12.4 (8.3, 16.1) | 6.2 (1.2, 10.9) | - | - |
| 15~64 | 14.0 (6.9, 17.6) | 7.5 (1.6, 13.1) | 14.4 (8.1, 20.2) | - | - | 21.3 (9.9, 31.8) |
| 65+ | 16.7 (8.6, 20.2) | 12.6 (6.4, 18.5) | 15.2 (8.5, 21.6) | 9.5 (1.3, 17.2) | 9.7 (1.4, 17.5) | 19.2 (6.4, 31.1) |
| Variable | PM2.5 | PM10 | SO2 | NO2 | O3 | CO |
|---|---|---|---|---|---|---|
| All inpatients | 103 (79, 126) | 71 (45, 95) | 98 (70, 125) | 40 (7, 73) | - | 142 (41, 234) |
| Disease subgroups | ||||||
| Pneumonia | 24 (18, 40) | 19 (7, 30) | 34 (21, 46) | 24 (9, 38) | 17 (1, 32) | - |
| COPD | 26 (18, 41) | - | 21 (7, 34) | - | - | 50 (25, 73) |
| Gender | ||||||
| Male | 63 (53, 89) | 52 (33, 71) | 73 (53, 93) | 36 (10, 60) | 35 (5, 64) | 104 (60, 145) |
| Female | 41 (15, 46) | 19 (3, 35) | 34 (16, 51) | - | - | 35 (7, 61) |
| Age (years) | ||||||
| 0~14 | 19 (17, 36) | 16 (5, 25) | 34 (23, 44) | 17 (3, 30) | - | - |
| 15~64 | 38 (19, 48) | 21 (4, 36) | 39 (22, 56) | - | - | 59 (27, 87) |
| 65+ | 46 (24, 56) | 34 (18, 51) | 42 (23, 59) | 26 (4, 47) | 36 (5, 65) | 53 (18, 85) |
| Air Pollutants | Annual Average Concentrations of Pollutants in the Air under Four Scenarios | Evitable Economic Losses under Different Scenarios of Decreasing Air Pollutant Concentrations (Million USD) | |||||||
|---|---|---|---|---|---|---|---|---|---|
| All Inpatients | Disease Subgroups | Gender Groups | Age Groups | ||||||
| Pneumonia | COPD | Male | Female | 0~14 | 15~64 | 65+ | |||
| PM2.5 | 10 μg/m3 | 16.88 | 4.72 | 5.01 | 11.73 | 5.01 | 4.44 | 5.58 | 6.58 |
| 20 μg/m3 | 13.02 | 3.58 | 4.01 | 9.01 | 3.86 | 3.29 | 4.29 | 5.15 | |
| 30 μg/m3 | 9.01 | 2.58 | 2.86 | 6.30 | 2.72 | 2.15 | 3.00 | 3.72 | |
| 40 μg/m3 | 5.01 | 1.29 | 1.72 | 3.43 | 1.57 | 1.14 | 1.72 | 2.15 | |
| PM10 | 20 μg/m3 | 10.88 | 2.86 | - | 8.01 | 3.00 | 2.43 | 3.15 | 5.29 |
| 40 μg/m3 | 7.58 | 2 | - | 5.58 | 2.00 | 1.57 | 2.15 | 3.72 | |
| 60 μg/m3 | 4.15 | 1 | - | 3.15 | 1.14 | 0.86 | 1.29 | 2.15 | |
| 80 μg/m3 | 0.86 | 0.14 | - | 0.57 | 0.29 | 0.14 | 0.29 | 0.57 | |
| SO2 | 4 μg/m3 | 12.45 | 4.15 | 2.72 | 9.30 | 4.29 | 4.29 | 5.01 | 5.29 |
| 6 μg/m3 | 8.73 | 2.86 | 2 | 6.44 | 3.00 | 2.86 | 3.58 | 3.86 | |
| 8 μg/m3 | 5.01 | 1.43 | 1.29 | 3.72 | 1.72 | 1.43 | 2.00 | 2.29 | |
| 10 μg/m3 | 1.14 | 0.43 | 0.72 | 0.43 | 0.00 | 0.43 | 0.72 | ||
| NO2 | 10 μg/m3 | 6.3 | 3.72 | - | 5.58 | - | 2.72 | - | 4.01 |
| 20 μg/m3 | 4.44 | 2.58 | - | 4.01 | - | 1.86 | - | 2.86 | |
| 30 μg/m3 | 2.72 | 1.57 | - | 2.29 | - | 1.14 | - | 1.72 | |
| 40 μg/m3 | 0.86 | 0.43 | - | 0.72 | - | 0.29 | - | 0.57 | |
| O3 | 20 μg/m3 | 4.87 | 2.72 | - | 4.87 | - | - | - | 4.15 |
| 40 μg/m3 | 3.43 | 1.86 | - | 3.43 | - | - | - | 2.86 | |
| 60 μg/m3 | 2.00 | 1 | - | 2.00 | - | - | - | 1.57 | |
| 80 μg/m3 | 0.57 | 0.14 | - | 0.57 | - | - | - | 0.43 | |
| CO | 0.25 mg/m3 | 21.75 | - | 7.58 | 14.31 | 6.44 | - | 9.01 | 8.01 |
| 0.50 mg/m3 | 14.74 | - | 5.29 | 9.73 | 4.29 | - | 6.01 | 5.58 | |
| 0.75 mg/m3 | 7.58 | - | 2.86 | 5.01 | 2.29 | - | 3.15 | 2.86 | |
| 1.00 mg/m3 | 0.14 | - | 0.29 | 0.14 | 0.14 | - | 0 | 0.14 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, H.; You, S.; Zhang, M.; Liu, D.; Wang, X.; Ren, J.; Yu, C. The Impact of Atmospheric Pollutants on Human Health and Economic Loss Assessment. Atmosphere 2021, 12, 1628. https://doi.org/10.3390/atmos12121628
Zhang H, You S, Zhang M, Liu D, Wang X, Ren J, Yu C. The Impact of Atmospheric Pollutants on Human Health and Economic Loss Assessment. Atmosphere. 2021; 12(12):1628. https://doi.org/10.3390/atmos12121628
Chicago/Turabian StyleZhang, Houli, Shibing You, Miao Zhang, Difei Liu, Xuyan Wang, Jingru Ren, and Chuanhua Yu. 2021. "The Impact of Atmospheric Pollutants on Human Health and Economic Loss Assessment" Atmosphere 12, no. 12: 1628. https://doi.org/10.3390/atmos12121628