
The Tip of the Iceberg: Genotype of Puerto Rican Pediatric Obesity



Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Clinical Assessment
2.3. Obesity Genetic Screening
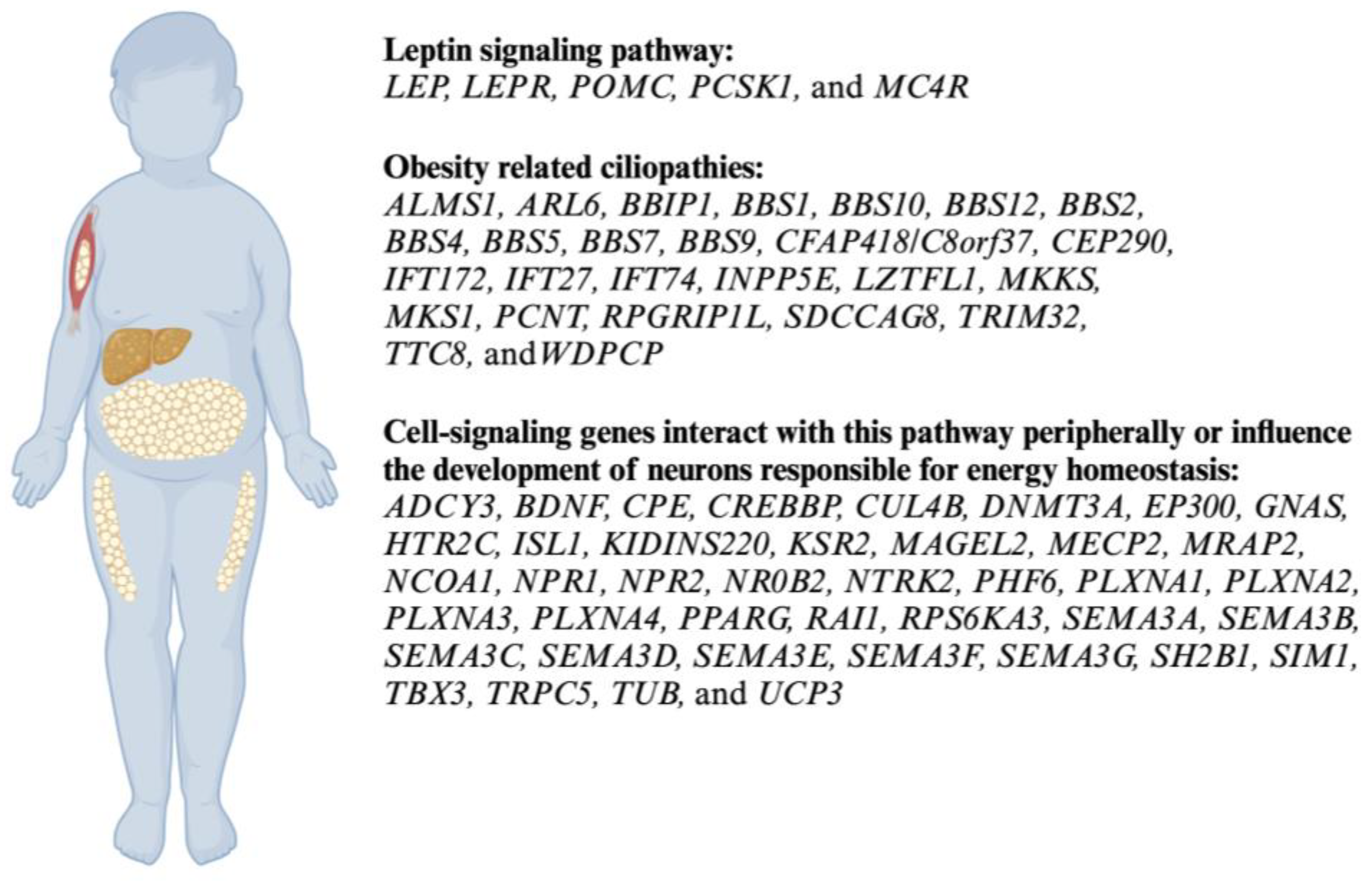
2.4. Genetic Panel and Analysis
2.5. Reports and Counseling
2.6. Statistical Analysis
3. Results
3.1. Demographics and Clinical Characteristics
3.2. Genetic Test Results
3.2.1. Overview of Obesity Genetic Variants
3.2.2. Pathogenic, Likely Pathogenic, or At-Risk Variants
3.2.3. Variants of Uncertain Significance (VUS)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lin, X.; Li, H. Obesity: Epidemiology, Pathophysiology, and Therapeutics. Front. Endocrinol. 2021, 12, 706978. [Google Scholar] [CrossRef]
- van Vliet-Ostaptchouk, J.V.; Snieder, H.; Lagou, V. Gene-Lifestyle Interactions in Obesity. Curr. Nutr. Rep. 2012, 1, 184–196. [Google Scholar] [CrossRef]
- Tiwari, A.; Balasundaram, P. Public Health Considerations Regarding Obesity. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Loos, R.J.F.; Yeo, G.S.H. The genetics of obesity: From discovery to biology. Nat. Rev. Genet. 2022, 23, 120–133. [Google Scholar] [CrossRef] [PubMed]
- Kumari, S.; Shukla, S.; Acharya, S. Childhood Obesity: Prevalence and Prevention in Modern Society. Cureus 2022, 14, e31640. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 28 February 2024).
- Sahoo, K.; Sahoo, B.; Choudhury, A.K.; Sofi, N.Y.; Kumar, R.; Bhadoria, A.S. Childhood obesity: Causes and consequences. J. Fam. Med. Prim. Care 2015, 4, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Garver, W.S.; Newman, S.B.; Gonzales-Pacheco, D.M.; Castillo, J.J.; Jelinek, D.; Heidenreich, R.A.; Orlando, R.A. The genetics of childhood obesity and interaction with dietary macronutrients. Genes. Nutr. 2013, 8, 271–287. [Google Scholar] [CrossRef] [PubMed]
- Styne, D.M.; Arslanian, S.A.; Connor, E.L.; Farooqi, I.S.; Murad, M.H.; Silverstein, J.H.; Yanovski, J.A. Pediatric Obesity-Assessment, Treatment, and Prevention: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2017, 102, 709–757. [Google Scholar] [CrossRef] [PubMed]
- Lyon, H.N.; Hirschhorn, J.N. Genetics of common forms of obesity: A brief overview. Am. J. Clin. Nutr. 2005, 82, 215S–217S. [Google Scholar] [CrossRef] [PubMed]
- Mahmoud, R.; Kimonis, V.; Butler, M.G. Genetics of Obesity in Humans: A Clinical Review. Int. J. Mol. Sci. 2022, 23, 11005. [Google Scholar] [CrossRef] [PubMed]
- Duis, J.; Butler, M.G. Syndromic and Nonsyndromic Obesity: Underlying Genetic Causes in Humans. Adv. Biol. 2022, 6, e2101154. [Google Scholar] [CrossRef]
- Littleton, S.H.; Berkowitz, R.I.; Grant, S.F.A. Genetic Determinants of Childhood Obesity. Mol. Diagn. Ther. 2020, 24, 653–663. [Google Scholar] [CrossRef]
- O’Malley, M.A.; Stotz, K. Intervention, integration and translation in obesity research: Genetic, developmental and metaorganismal approaches. Philos. Ethics Humanit. Med. 2011, 6, 2. [Google Scholar] [CrossRef] [PubMed]
- Tirthani, E.; Said, M.S.; Rehman, A. Genetics and Obesity. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Thaker, V.V. Genetic and Epigenetic Causes of Obesity. Adolesc. Med. State Art Rev. 2017, 28, 379–405. [Google Scholar] [PubMed]
- Bouchard, C. Genetics of Obesity: What We Have Learned Over Decades of Research. Obesity 2021, 29, 802–820. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.Y.; Yin, R.X. Recent progress in epigenetics of obesity. Diabetol. Metab. Syndr. 2022, 14, 171. [Google Scholar] [CrossRef] [PubMed]
- Elias-Boneta, A.R.; Toro, M.J.; Garcia, O.; Torres, R.; Palacios, C. High prevalence of overweight and obesity among a representative sample of Puerto Rican children. BMC Public Health 2015, 15, 219. [Google Scholar] [CrossRef] [PubMed]
- Kannan, S.; Acosta, L.M.; Acevedo-Garcia, D.; Divjan, A.; Bracero, L.A.; Perzanowski, M.S.; Chew, G.L. Sociocultural characteristics, obesity and inflammatory biomarkers in Puerto Rican toddlers born in New York City. Pediatr. Allergy Immunol. 2013, 24, 487–492. [Google Scholar] [CrossRef] [PubMed]
- Hazrati, S.; Khan, F.; Huddleston, K.; De La Cruz, F.; Deeken, J.F.; Fuller, A.; Wong, W.S.W.; Niederhuber, J.E.; Hourigan, S.K. Clinical and social factors associated with excess weight in Hispanic and non-Hispanic White children. Pediatr. Res. 2019, 85, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Sohn, Y.B. Genetic obesity: An update with emerging therapeutic approaches. Ann. Pediatr. Endocrinol. Metab. 2022, 27, 169–175. [Google Scholar] [CrossRef]
- Llewellyn, C.H.; Trzaskowski, M.; van Jaarsveld, C.H.M.; Plomin, R.; Wardle, J. Satiety mechanisms in genetic risk of obesity. JAMA Pediatr. 2014, 168, 338–344. [Google Scholar] [CrossRef]
- Vaisse, C.; Reiter, J.F.; Berbari, N.F. Cilia and Obesity. Cold Spring Harb. Perspect. Biol. 2017, 9, a028217. [Google Scholar] [CrossRef]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: A joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–424. [Google Scholar] [CrossRef]
- Roberts, K.J.; Ariza, A.J.; Selvaraj, K.; Quadri, M.; Mangarelli, C.; Neault, S.; Davis, E.E.; Binns, H.J. Testing for rare genetic causes of obesity: Findings and experiences from a pediatric weight management program. Int. J. Obes. 2022, 46, 1493–1501. [Google Scholar] [CrossRef]
- Butte, N.F.; Cai, G.; Cole, S.A.; Comuzzie, A.G. Viva la Familia Study: Genetic and environmental contributions to childhood obesity and its comorbidities in the Hispanic population. Am. J. Clin. Nutr. 2006, 84, 646–654. [Google Scholar] [CrossRef]
- Young, K.L.; Graff, M.; Fernandez-Rhodes, L.; North, K.E. Genetics of Obesity in Diverse Populations. Curr. Diabetes Rep. 2018, 18, 145. [Google Scholar] [CrossRef]
- Tamaroff, J.; Williamson, D.; Slaughter, J.C.; Xu, M.; Srivastava, G.; Shoemaker, A.H. Prevalence of genetic causes of obesity in clinical practice. Obes. Sci. Pract. 2023, 9, 508–515. [Google Scholar] [CrossRef]
- Arnouk, L.; Chantereau, H.; Courbage, S.; Tounian, P.; Clement, K.; Poitou, C.; Dubern, B. Hyperphagia and impulsivity: Use of self-administered Dykens’ and in-house impulsivity questionnaires to characterize eating behaviors in children with severe and early-onset obesity. Orphanet J. Rare Dis. 2024, 19, 84. [Google Scholar] [CrossRef]
- Malhotra, S.; Sivasubramanian, R.; Srivastava, G. Evaluation and Management of Early Onset Genetic Obesity in Childhood. J. Pediatr. Genet. 2021, 10, 194–204. [Google Scholar] [CrossRef]
- Clément, K.; Mosbah, H.; Poitou, C. Rare genetic forms of obesity: From gene to therapy. Physiol. Behav. 2020, 227, 113134. [Google Scholar] [CrossRef]
- Dubern, B.; Mosbah, H.; Pigeyre, M.; Clement, K.; Poitou, C. Rare genetic causes of obesity: Diagnosis and management in clinical care. Ann. Endocrinol. 2022, 83, 63–72. [Google Scholar] [CrossRef]
- Loid, P.; Mustila, T.; Makitie, R.E.; Viljakainen, H.; Kampe, A.; Tossavainen, P.; Lipsanen-Nyman, M.; Pekkinen, M.; Makitie, O. Rare Variants in Genes Linked to Appetite Control and Hypothalamic Development in Early-Onset Severe Obesity. Front. Endocrinol. 2020, 11, 81. [Google Scholar] [CrossRef] [PubMed]
- Pomeroy, J.; Krentz, A.D.; Richardson, J.G.; Berg, R.L.; VanWormer, J.J.; Haws, R.M. Bardet-Biedl syndrome: Weight patterns and genetics in a rare obesity syndrome. Pediatr. Obes. 2021, 16, e12703. [Google Scholar] [CrossRef] [PubMed]
- Guardiola, G.A.; Ramos, F.; Izquierdo, N.J.; Oliver, A.L. A Genotype-Phenotype Analysis of the Bardet-Biedl Syndrome in Puerto Rico. Clin. Ophthalmol. 2021, 15, 3757–3764. [Google Scholar] [CrossRef] [PubMed]
- Meier, D.T.; Rachid, L.; Wiedemann, S.J.; Traub, S.; Trimigliozzi, K.; Stawiski, M.; Sauteur, L.; Winter, D.V.; Le Foll, C.; Bregere, C.; et al. Prohormone convertase 1/3 deficiency causes obesity due to impaired proinsulin processing. Nat. Commun. 2022, 13, 4761. [Google Scholar] [CrossRef]
- Nies, V.J.M.; Struik, D.; Wolfs, M.G.M.; Rensen, S.S.; Szalowska, E.; Unmehopa, U.A.; Fluiter, K.; van der Meer, T.P.; Hajmousa, G.; Buurman, W.A.; et al. TUB gene expression in hypothalamus and adipose tissue and its association with obesity in humans. Int. J. Obes. 2018, 42, 376–383. [Google Scholar] [CrossRef]
- Lee, C.H.; Kang, G.M.; Kim, M.S. Mechanisms of Weight Control by Primary Cilia. Mol. Cells 2022, 45, 169–176. [Google Scholar] [CrossRef]


{kind=link}
| Characteristics | Value (n = 103) |
|---|---|
| Gender (F/M) | 36/67 |
| Age, median (IQR), (years) | 9 (6) |
| Ethnicity, n (%), Hispanics, Puerto Ricans | 103 (100) |
| BMI females, median (IQR), (kg/m2) | 31.7 (12.8) |
| BMI males, median (IQR), (kg/m2) | 29.4 (7.5) |
| Hyperphagia | 87 (84) |
| Age onset of hyperphagia females, median (IQR), (years) | 4 (2) |
| Age of onset of hyperphagia males, median (IQR), (years) | 5 (2.5) |
| Family history of obesity, n (%) | 93 (90) |
| Population | Frequency (n = 138) |
|---|---|
| Latino (n, %) | (48, 34.8) |
| European (non-Finnish) | (34, 24.6) |
| African | (30, 21.7) |
| South Asian | (12, 8.7) |
| Ashkenazi Jewish | (10, 7.2) |
| East Asian | (2, 1.4) |
| European (Finnish) | (2, 1.4) |
| Gene | Variant | Frequency | Classification |
|---|---|---|---|
| PCSK1 | c.661A>G | 5 | Pathogenic |
| BBS1 | c.1169T>G | 4 | Pathogenic |
| BBS1 | c.1645G>T | 3 | Pathogenic |
| TUB | c.1421C>T | 2 | Risk |
| BBS9 | c.396G>C | 4 | VUS |
| SH2B1 | c.1028C>T | 3 | VUS |
| PCSK1 | c.1918A>G | 3 | VUS |
| SEMA3F | c.1963C>A | 3 | VUS |
| RPGRIP1L | c.251G>A | 3 | VUS |
| VPS13B | c.5528A>T | 3 | VUS |
| SDCCAG8 | c.833G>A | 3 | VUS |
| MKS1 | c.83T>C | 3 | VUS |
| MKS1 | c.857A>G | 3 | VUS |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melendez-Montañez, J.M.; De Jesus-Rojas, W. The Tip of the Iceberg: Genotype of Puerto Rican Pediatric Obesity. Genes 2024, 15, 394. https://doi.org/10.3390/genes15040394
Melendez-Montañez JM, De Jesus-Rojas W. The Tip of the Iceberg: Genotype of Puerto Rican Pediatric Obesity. Genes. 2024; 15(4):394. https://doi.org/10.3390/genes15040394
Chicago/Turabian StyleMelendez-Montañez, Jesus M., and Wilfredo De Jesus-Rojas. 2024. "The Tip of the Iceberg: Genotype of Puerto Rican Pediatric Obesity" Genes 15, no. 4: 394. https://doi.org/10.3390/genes15040394