
A Three-Way Interaction of Sex, PER2 rs56013859 Polymorphism, and Family Maltreatment in Depressive Symptoms in Adolescents
 ,
,
Abstract
:
1. Introduction
1.1. Depression
1.2. Thoughts of Death and Suicide in Depression
1.3. Sleep Complaints in Depression
1.4. Family Maltreatment
1.5. Circadian Rhythms and PER2
1.6. Aim
- Is there an interaction between rs56013859 polymorphism and sex in combination with family maltreatment in adolescents as predictor of: (a) core depressive symptoms, (b) sleep complaints, and (c) thoughts of death and suicide?
- If an interaction effect is present, for whom and at which level of family maltreatment is it present?
- Does the effect of this interaction remain over time?
2. Materials and Methods
2.1. Sample
2.2. Procedures
2.2.1. Assessment of Depressive Symptoms
- Have you felt down, sad, or empty, almost all the time, almost every day?
- Have you felt annoyed, angry, or upset almost all the time, almost every day?
- Almost every day, have you felt disinterested in most things or found it difficult to enjoy the things you normally enjoy?
- Have you been feeling weak, tired, or low on energy?
- Has your self-confidence been worse than usual?
- Have you felt guilty or worthless?
- Have you had difficulty thinking or concentrating?
- Have you had thoughts about death, or have you thought that it would be better to be dead?
2.2.2. Assessment of Sleep
- Difficulties falling asleep;
- Difficulties waking up;
- Repeated awakenings with difficulties falling asleep again;
- Not well-rested on awakening;
- Premature (final) awakenings;
- Disturbed/restless sleep;
- Feelings of being exhausted at awakening;
- Sleepy during school/work;
- Sleepy during leisure time;
- Involuntary sleep episodes during school/work;
- Involuntary sleep episodes during leisure time;
- Need to fight off sleep to stay awake.
2.2.3. Assessment of Family Maltreatment
2.2.4. Genotyping
2.2.5. Sex
2.2.6. Age
2.3. Statistical Analyses
2.3.1. Cross-Sectional Analyses
2.3.2. Longitudinal Analyses
3. Results
3.1. Crude Analyses
3.2. Cross-Sectional Analyses
3.2.1. Linear Regression with Outcome Core Depressive Symptoms
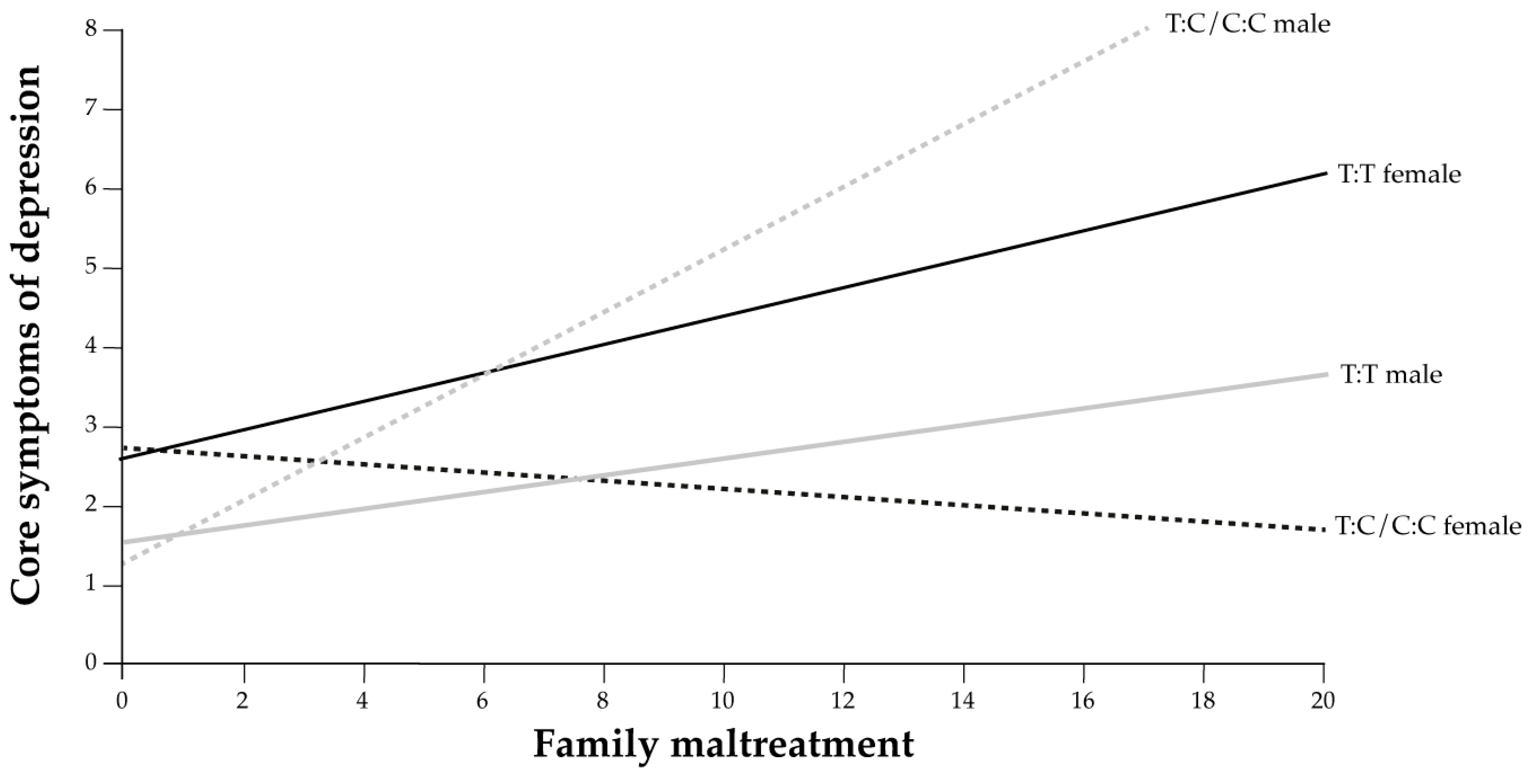
3.2.2. Moderation Model 3 with Outcome Core Depressive Symptoms Index in 2012
3.2.3. Linear Regression with Outcome Sleep Complaints Index, and Logistic Regression with Outcome Thoughts of Death and Suicide in 2012
3.3. Longitudinal Analyses
3.3.1. Outcomes in 2015
3.3.2. Outcomes in 2018
3.3.3. Moderation Model 3 with Outcome Core Depressive Symptoms Index in 2018
3.4. Analysis of Variance Results
3.4.1. Cross-Sectional Analyses
3.4.2. Longitudinal Analyses
4. Discussion
Strengths and Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- Cross-Sectional Analyses

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Independent Variables | p | β | (95% CI) |
|---|---|---|---|
| Sex | 0.005 | 4.477 | (1.581 to 12.678) |
| rs56013859 | 0.857 | 1.147 | (0.258 to 5.094) |
| Family maltreatment | <0.001 | 2.803 | (1.547 to 5.081) |
| Sex 1 × rs56013859 2 | 0.621 | 1.739 | (0.194 to 15.59) |
| Sex 1 × Family maltreatment | 0.163 | 1.793 | (0.79 to 4.072) |
| rs56013859 2 × Family maltreatment | 0.637 | 1.351 | (0.387 to 4.715) |
| Sex 1 × rs56013859 2 × Family maltreatment | 0.907 | 1.113 | (0.184 to 6.731) |
| χ2 = 160.190 | <0.001 |
| Independent Variables | p | OR | (95% CI) |
|---|---|---|---|
| Sex | 0.076 | 0.664 | (0.423 to 1.043) |
| rs56013859 | 0.442 | 1.382 | (0.606 to 3.151) |
| Family maltreatment | 0.004 | 0.799 | (0.686 to 0.93) |
| Sex 1 × rs56013859 2 | 0.371 | 0.637 | (0.237 to 1.711) |
| Sex 1 × Family maltreatment | 0.933 | 0.992 | (0.831 to 1.185) |
| rs56013859 2 × Family maltreatment | 0.795 | 0.954 | (0.669 to 1.36) |
| Sex 1 × rs56013859 2 × Family maltreatment | 0.953 | 1.013 | (0.657 to 1.562) |
| χ2 = 51.172 | <0.001 |
- Longitudinal Analyses
| Independent Variables | p | β | (95% CI) |
|---|---|---|---|
| Sex | <0.001 | 4.466 | (3.408 to 5.852) |
| rs56013859 | 0.257 | 1.26 | (0.845 to 1.88) |
| Family maltreatment | <0.001 | 1.334 | (1.16 to 1.534) |
| Sex 1 × rs56013859 2 | 0.034 | 0.535 | (0.3 to 0.955) |
| Sex 1 × Family maltreatment | 0.984 | 0.998 | (0.84 to 1.186) |
| rs56013859 2 × Family maltreatment | 0.151 | 0.775 | (0.547 to 1.097) |
| Sex 1 × rs56013859 2 × Family maltreatment | 0.06 | 1.491 | (0.984 to 2.261) |
| χ2 = 215.557 | <0.001 |
| Independent Variables | p | β | (95% CI) |
|---|---|---|---|
| Sex | <0.001 | 136.441 | (35.906 to 518.466) |
| rs56013859 | 0.824 | 1.275 | (0.15 to 10.865) |
| Family maltreatment | 0.003 | 2.571 | (1.369 to 4.828) |
| Sex 1 × rs56013859 2 | 0.282 | 0.219 | (0.014 to 3.496) |
| Sex 1 × Family maltreatment | 0.503 | 1.291 | (0.612 to 2.721) |
| rs56013859 2 × Family maltreatment | 0.899 | 0.891 | (0.15 to 5.273) |
| Sex 1 × rs56013859 2 × Family maltreatment | 0.639 | 1.727 | (0.176 to 16.991) |
| χ2 = 129.194 | <0.001 |
| Independent Variables | p | β | (95% CI) |
|---|---|---|---|
| Sex | <0.001 | 19.609 | (2.976 to 0.8116) |
| rs56013859 | 0.678 | 0.612 | (−0.49 to 1.1809) |
| Family maltreatment | 0.006 | 3.24 | (1.175 to 0.4244) |
| Sex 1× rs56013859 2 | 0.96 | 0.922 | (−0.081 to 1.6043) |
| Sex 1 × Family maltreatment | 0.691 | 0.815 | (−0.205 to 0.5159) |
| rs56013859 2 × Family maltreatment | 0.7 | 1.51 | (0.412 to 1.0707) |
| Sex 1 × rs56013859 2 × Family maltreatment | 0.969 | 0.949 | (−0.052 to 1.3396) |
| χ2 = 52.751 | <0.001 |
| Independent Variables | p | OR | (95% CI) |
|---|---|---|---|
| Sex | 0.365 | 0.825 | (0.543 to 1.252) |
| rs56013859 | 0.89 | 1.053 | (0.505 to 2.197) |
| Family maltreatment | 0.041 | 0.826 | (0.687 to 0.992) |
| Sex 1 × rs56013859 2 | 0.562 | 0.768 | (0.315 to 1.873) |
| Sex 1 × Family maltreatment | 0.474 | 1.077 | (0.878 to 1.321) |
| rs56013859 2 × Family maltreatment | 0.204 | 0.796 | (0.559 to 1.132) |
| Sex 1 × rs56013859 2 × Family maltreatment | 0.089 | 1.627 | (0.929 to 2.849) |
| χ2 = 17.63 | <0.014 |
- Cross-Sectional Analyses
| Independent Variables | B | 95% CI | SE 1 | t | ηp 2 | p |
|---|---|---|---|---|---|---|
| Sex | 0.644 | (0.439 to 0.85) | 0.105 | 6.14 | 0.023 | <0.001 |
| rs56013859 2 | −0.052 | (−0.304 to 0.199) | 0.128 | −0.406 | 0 | 0.685 |
| Family maltreatment | 0.321 | (0.19 to 0.453) | 0.067 | 4.797 | 0.014 | <0.001 |
| Sex 1 × rs56013859 2 | −0.133 | (−0.349 to 0.083) | 0.11 | −1.21 | 0.001 | 0.226 |
| Sex 1 × Family maltreatment | 0.042 | (−0.375 to 0.459) | 0.213 | 0.195 | 0 | 0.845 |
| rs56013859 2 × Family maltreatment | 0.008 | (−0.167 to 0.183) | 0.089 | 0.09 | 0 | 0.928 |
| Sex 1 × rs56013859 2 × Family maltreatment | 0.372 | (0.032 to 0.713) | 0.173 | 2.146 | 0.003 | 0.032 |
| R2 | 0.132 |
| Independent Variables | B | 95% CI | SE 1 | t | ηp 2 | p |
|---|---|---|---|---|---|---|
| Sex | 1.499 | (0.448 to 2.55) | 0.536 | 2.797 | 0.005 | 0.005 |
| rs56013859 | 0.137 | (−1.369 to 1.642) | 0.768 | 0.178 | 0 | 0.859 |
| Family maltreatment | 1.031 | (0.417 to 1.644) | 0.313 | 3.296 | 0.007 | 0.001 |
| Sex 1 × rs56013859 2 | 0.301 | (−1.001 to 1.602) | 0.664 | 0.453 | 0 | 0.651 |
| Sex 1 × Family maltreatment | 0.553 | (−1.664 to 2.771) | 1.13 | 0.489 | 0 | 0.625 |
| rs56013859 2 × Family maltreatment | 0.584 | (−0.269 to 1.438) | 0.435 | 1.342 | 0.001 | 0.18 |
| Sex 1 × rs56013859 2 × Family maltreatment | 0.107 | (−1.797 to 2.011) | 0.971 | 0.11 | 0 | 0.912 |
| R2 | 0.1 |
- Longitudinal Analyses
| Independent Variables | B | 95% CI | SE 1 | t | ηp 2 | p |
|---|---|---|---|---|---|---|
| Sex | 1.496 | (1.225 to 1.768) | 0.139 | 10.798 | 0.077 | <0.001 |
| rs56013859 | 0.231 | (−0.174 to 0.637) | 0.207 | 1.12 | 0.001 | 0.263 |
| Family maltreatment | 0.288 | (0.143 to 0.433) | 0.074 | 3.898 | 0.011 | <0.001 |
| Sex 1 × rs56013859 2 | −0.255 | (−0.631 to 0.121) | 0.192 | −1.33 | 0.001 | 0.184 |
| Sex 1 × Family maltreatment | −0.625 | (−1.21 to −0.041) | 0.298 | −2.098 | 0.003 | 0.036 |
| rs56013859 2 × Family maltreatment | −0.002 | (−0.18 to 0.176) | 0.091 | −0.02 | 0 | 0.984 |
| Sex 1 × rs56013859 2 × Family maltreatment | 0.4 | (−0.045 to 0.844) | 0.227 | 1.764 | 0.002 | 0.078 |
| R2 | 0.142 |
| Independent Variables | B | 95% CI | SE 1 | t | ηp 2 | p |
|---|---|---|---|---|---|---|
| Sex | 4.916 | (3.575 to 6.257) | 0.684 | 7.191 | 0.037 | <0.001 |
| rs56013859 | 0.243 | (−1.932 to 2.418) | 1.109 | 0.219 | 0 | 0.826 |
| Family maltreatment | 0.944 | (0.297 to 1.591) | 0.33 | 2.862 | 0.006 | 0.004 |
| Sex 1 × rs56013859 2 | −0.116 | (−2.072 to 1.841) | 0.997 | −0.116 | 0 | 0.908 |
| Sex 1 × Family maltreatment | −1.52 | (−4.33 to 1.289) | 1.432 | −1.062 | 0.001 | 0.289 |
| rs56013859 2 × Family maltreatment | 0.255 | (−0.51 to 1.02) | 0.39 | 0.654 | 0 | 0.513 |
| Sex 1 × rs56013859 2 × Family maltreatment | 0.547 | (−1.941 to 3.034) | 1.268 | 0.431 | 0 | 0.667 |
| R2 | 0.09 |
| Independent Variables | B | 95% CI | SE 1 | t | ηp 2 | p |
|---|---|---|---|---|---|---|
| Sex | 1.046 | (0.669 to 1.423) | 0.192 | 5.441 | 0.027 | <0.001 |
| rs56013859 | −0.301 | (−0.871 to 0.27) | 0.291 | −1.035 | 0.001 | 0.301 |
| Family maltreatment | 0.105 | (−0.112 to 0.322) | 0.111 | 0.947 | 0.001 | 0.344 |
| Sex 1 × rs56013859 2 | 0.292 | (−0.177 to 0.762) | 0.239 | 1.222 | 0.001 | 0.222 |
| Sex 1 × Family maltreatment | 0.435 | (−0.331 to 1.2) | 0.39 | 1.115 | 0.001 | 0.265 |
| rs56013859 2 × Family maltreatment | 0.074 | (−0.167 to 0.315) | 0.123 | 0.603 | 0 | 0.547 |
| Sex 1 × rs56013859 2 × Family maltreatment | −0.524 | (−1.083 to 0.035) | 0.285 | −1.839 | 0.003 | 0.066 |
| R2 | 0.064 |
| Independent Variables | B | 95% CI | SE 1 | t | ηp 2 | p |
|---|---|---|---|---|---|---|
| Sex | 2.976 | (1.373 to 4.579) | 0.817 | 3.644 | 0.013 | <0.001 |
| rs56013859 | −0.49 | (−2.866 to 1.885) | 1.21 | −0.405 | 0 | 0.685 |
| Family maltreatment | 1.175 | (0.31 to 2.041) | 0.441 | 2.666 | 0.007 | 0.008 |
| Sex 1 × rs560138592 | 0.412 | (−1.954 to 2.778) | 1.206 | 0.342 | 0 | 0.733 |
| Sex 1 × Family maltreatment | −0.081 | (−3.285 to 3.123) | 1.633 | −0.05 | 0 | 0.961 |
| rs56013859 2 × Family maltreatment | −0.205 | (−1.259 to 0.849) | 0.537 | −0.381 | 0 | 0.703 |
| Sex 1 × rs56013859 2 × Family maltreatment | −0.052 | (−2.947 to 2.842) | 1.475 | −0.035 | 0 | 0.972 |
| R2 | 0.049 |
References
- Institute for Health Metrics and Evaluation. Global Burden of Disease (GBD). Available online: www.healthdata.org/gbd (accessed on 23 February 2023).
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013; Volume 1, p. 945. [Google Scholar]
- Fried, E.I.; Epskamp, S.; Nesse, R.M.; Tuerlinckx, F.; Borsboom, D. What are ‘good’ depression symptoms? Comparing the centrality of DSM and non-DSM symptoms of depression in a network analysis. J. Affect. Disord 2016, 189, 314–320. [Google Scholar] [CrossRef]
- Minor, K.L.; Champion, J.E.; Gotlib, I.H. Stability of DSM-IV criterion symptoms for major depressive disorder. J. Psychiatr. Res 2005, 39, 415–420. [Google Scholar] [CrossRef]
- Merikangas, K.R.; He, J.P.; Burstein, M.; Swanson, S.A.; Avenevoli, S.; Cui, L.; Benjet, C.; Georgiades, K.; Swendsen, J. Lifetime prevalence of mental disorders in U.S. adolescents: Results from the National Comorbidity Survey Replication—Adolescent Supplement (NCS-A). J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 980–989. [Google Scholar] [CrossRef]
- Saluja, G.; Iachan, R.; Scheidt, P.C.; Overpeck, M.D.; Sun, W.; Giedd, J.N. Prevalence of and risk factors for depressive symptoms among young adolescents. Arch. Pediatr. Adolesc. Med. 2004, 158, 760–765. [Google Scholar] [CrossRef]
- Piccinelli, M.; Wilkinson, G. Gender differences in depression. Critical review. Br. J. Psychiatry 2000, 177, 486–492. [Google Scholar] [CrossRef]
- Kessing, L.V. Epidemiology of subtypes of depression. Acta Psychiatr. Scand. 2007, 115, 85–89. [Google Scholar] [CrossRef] [PubMed]
- Brent, D.A.; Kalas, R.; Edelbrock, C.; Costello, A.J.; Dulcan, M.K.; Conover, N. Psychopathology and its relationship to suicidal ideation in childhood and adolescence. J. Am. Acad. Child Psychiatry 1986, 25, 666–673. [Google Scholar] [CrossRef] [PubMed]
- Ivarsson, T.; Larsson, B.; Gillberg, C. A 2–4 year follow up of depressive symptoms, suicidal ideation, and suicide attempts among adolescent psychiatric inpatients. Eur. Child Adolesc. Psychiatry 1998, 7, 96–104. [Google Scholar] [CrossRef] [PubMed]
- Beautrais, A.L.; Joyce, P.R.; Mulder, R.T. Risk factors for serious suicide attempts among youths aged 13 through 24 years. J. Am. Acad. Child Adolesc. Psychiatry 1996, 35, 1174–1182. [Google Scholar] [CrossRef]
- Benarous, X.; Consoli, A.; Cohen, D.; Renaud, J.; Lahaye, H.; Guilé, J.M. Suicidal behaviors and irritability in children and adolescents: A systematic review of the nature and mechanisms of the association. Eur. Child Adolesc. Psychiatry 2019, 28, 667–683. [Google Scholar] [CrossRef] [PubMed]
- Silverman, J.J.; Galanter, M.; Jackson-Triche, M.; Jacobs, D.G.; Lomax, J.W.; Riba, M.B.; Tong, L.D.; Watkins, K.E.; Fochtmann, L.J.; Rhoads, R.S.; et al. The American Psychiatric Association Practice Guidelines for the Psychiatric Evaluation of Adults. Am. J. Psychiatry 2015, 172, 798–802. [Google Scholar] [CrossRef] [PubMed]
- Miranda, R.; Ortin, A.; Scott, M.; Shaffer, D. Characteristics of suicidal ideation that predict the transition to future suicide attempts in adolescents. J. Child Psychol. Psychiatry 2014, 55, 1288–1296. [Google Scholar] [CrossRef] [PubMed]
- Harmer, B.; Lee, S.; Duong, T.V.H.; Saadabadi, A. Suicidal Ideation. In StatPearls; StatPearls Publishing LLC.: Treasure Island FL, USA, 2022. [Google Scholar]
- Nock, M.K.; Borges, G.; Bromet, E.J.; Alonso, J.; Angermeyer, M.; Beautrais, A.; Bruffaerts, R.; Chiu, W.T.; de Girolamo, G.; Gluzman, S.; et al. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br. J. Psychiatry 2008, 192, 98–105. [Google Scholar] [CrossRef] [PubMed]
- Ho, T.C.; Gifuni, A.J.; Gotlib, I.H. Psychobiological risk factors for suicidal thoughts and behaviors in adolescence: A consideration of the role of puberty. Mol. Psychiatry 2022, 27, 606–623. [Google Scholar] [CrossRef]
- Kokkevi, A.; Rotsika, V.; Arapaki, A.; Richardson, C. Adolescents’ self-reported suicide attempts, self-harm thoughts and their correlates across 17 European countries. J. Child Psychol. Psychiatry 2012, 53, 381–389. [Google Scholar] [CrossRef]
- Lewinsohn, P.M.; Rohde, P.; Seeley, J.R.; Baldwin, C.L. Gender differences in suicide attempts from adolescence to young adulthood. J. Am. Acad. Child Adolesc. Psychiatry 2001, 40, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Fergusson, D.M.; Woodward, L.J.; Horwood, L.J. Risk factors and life processes associated with the onset of suicidal behaviour during adolescence and early adulthood. Psychol. Med. 2000, 30, 23–39. [Google Scholar] [CrossRef]
- Dunn, E.C.; McLaughlin, K.A.; Slopen, N.; Rosand, J.; Smoller, J.W. Developmental timing of child maltreatment and symptoms of depression and suicidal ideation in young adulthood: Results from the National Longitudinal Study of Adolescent Health. Depress. Anxiety 2013, 30, 955–964. [Google Scholar] [CrossRef]
- Fergusson, D.M.; Boden, J.M.; Horwood, L.J. Exposure to childhood sexual and physical abuse and adjustment in early adulthood. Child Abus. Negl. 2008, 32, 607–619. [Google Scholar] [CrossRef]
- Castellví, P.; Miranda-Mendizábal, A.; Parés-Badell, O.; Almenara, J.; Alonso, I.; Blasco, M.J.; Cebrià, A.; Gabilondo, A.; Gili, M.; Lagares, C.; et al. Exposure to violence, a risk for suicide in youths and young adults. A meta-analysis of longitudinal studies. Acta Psychiatr. Scand. 2017, 135, 195–211. [Google Scholar] [CrossRef]
- Brown, J.; Cohen, P.; Johnson, J.G.; Smailes, E.M. Childhood abuse and neglect: Specificity of effects on adolescent and young adult depression and suicidality. J. Am. Acad. Child Adolesc. Psychiatry 1999, 38, 1490–1496. [Google Scholar] [CrossRef]
- Harris, L.M.; Huang, X.; Linthicum, K.P.; Bryen, C.P.; Ribeiro, J.D. Sleep disturbances as risk factors for suicidal thoughts and behaviours: A meta-analysis of longitudinal studies. Sci. Rep. 2020, 10, 1–11. [Google Scholar] [CrossRef]
- Perlis, M.L.; Grandner, M.A.; Chakravorty, S.; Bernert, R.A.; Brown, G.K.; Thase, M.E. Suicide and sleep: Is it a bad thing to be awake when reason sleeps? Sleep Med. Rev. 2015, 29, 101–107. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.-W.; Tu, Y.-K.; Lai, Y.-F.; Lee, H.-C.; Tsai, P.-S.; Chen, T.-J.; Huang, H.-C.; Chen, Y.-T.; Chiu, H.-Y. Associations between sleep disturbances and suicidal ideation, plans, and attempts in adolescents: A systematic review and meta-analysis. Sleep 2019, 42, zsz054. [Google Scholar] [CrossRef] [PubMed]
- Kearns, J.C.; Coppersmith, D.D.; Santee, A.C.; Insel, C.; Pigeon, W.R.; Glenn, C.R. Sleep problems and suicide risk in youth: A systematic review, developmental framework, and implications for hospital treatment. Gen. Hosp. Psychiatry 2020, 63, 141–151. [Google Scholar] [CrossRef]
- Grigsby, T.J.; Rogers, C.J.; Albers, L.D.; Benjamin, S.M.; Lust, K.; Eisenberg, M.E.; Forster, M. Adverse Childhood Experiences and Health Indicators in a Young Adult, College Student Sample: Differences by Gender. Int. J. Behav. Med. 2020, 27, 660–667. [Google Scholar] [CrossRef]
- Zimmerman, M.; McGlinchey, J.B.; Young, D.; Chelminski, I. Diagnosing major depressive disorder introduction: An examination of the DSM-IV diagnostic criteria. J. Nerv. Ment. 2006, 194, 151–154. [Google Scholar] [CrossRef]
- Li, S.X.; Liu, L.J.; Xu, L.Z.; Gao, L.; Wang, X.F.; Zhang, J.T.; Lu, L. Diurnal alterations in circadian genes and peptides in major depressive disorder before and after escitalopram treatment. Psychoneuroendocrinology 2013, 38, 2789–2799. [Google Scholar] [CrossRef] [PubMed]
- Melhuish Beaupre, L.; Brown, G.M.; Kennedy, J.L. Circadian genes in major depressive disorder. World J. Biol. Psychiatry 2020, 21, 80–90. [Google Scholar] [CrossRef]
- Bunney, B.G.; Li, J.Z.; Walsh, D.M.; Stein, R.; Vawter, M.P.; Cartagena, P.; Barchas, J.D.; Schatzberg, A.F.; Myers, R.M.; Watson, S.J.; et al. Circadian dysregulation of clock genes: Clues to rapid treatments in major depressive disorder. Mol. Psychiatry 2015, 20, 48–55. [Google Scholar] [CrossRef]
- Bechtel, W. Circadian Rhythms and Mood Disorders: Are the Phenomena and Mechanisms Causally Related? Front. Psychiatry 2015, 6, 118. [Google Scholar] [CrossRef]
- Tafti, M.; Maret, S.; Dauvilliers, Y. Genes for normal sleep and sleep disorders. Ann. Med. 2005, 37, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Touitou, Y. Adolescent sleep misalignment: A chronic jet lag and a matter of public health. J Physiol. 2013, 107, 323–326. [Google Scholar] [CrossRef]
- Bruce, E.S.; Lunt, L.; McDonagh, J.E. Sleep in adolescents and young adults. Clin. Med. 2017, 17, 424–428. [Google Scholar] [CrossRef]
- Colrain, I.M.; Baker, F.C. Changes in sleep as a function of adolescent development. Neuropsychol. Rev. 2011, 21, 5–21. [Google Scholar] [CrossRef] [PubMed]
- Badin, E.; Haddad, C.; Shatkin, J.P. Insomnia: The Sleeping Giant of Pediatric Public Health. Curr. Psychiatry. Rep. 2016, 18, 47. [Google Scholar] [CrossRef] [PubMed]
- Nadorff, M.R.; Nazem, S.; Fiske, A. Insomnia symptoms, nightmares, and suicidal ideation in a college student sample. Sleep 2011, 34, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Nadorff, M.R.; Nazem, S.; Fiske, A. Insomnia Symptoms, Nightmares, and Suicide Risk: Duration of Sleep Disturbance Matters. Suicide Life-Threat. Behav. 2013, 43, 139–149. [Google Scholar] [CrossRef]
- World Health Organisation Child maltreatment. Available online: https://www.who.int/news-room/fact-sheets/detail/child-maltreatment (accessed on 17 March 2023).
- Donnelly, P.D.; Ward, C.L. Oxford Textbook of Violence Prevention: Epidemiology, Evidence, and Policy; Oxford Textbooks in Public Heath; Oxford University Press: Oxford, UK, 2015. [Google Scholar]
- Finkelhor, D.; Vanderminden, J.; Turner, H.; Hamby, S.; Shattuck, A. Child maltreatment rates assessed in a national household survey of caregivers and youth. Child Abus. Negl. 2014, 38, 1421–1435. [Google Scholar] [CrossRef]
- Anda, R.F.; Felitti, V.J.; Bremner, J.D.; Walker, J.D.; Whitfield, C.; Perry, B.D.; Dube, S.R.; Giles, W.H. The enduring effects of abuse and related adverse experiences in childhood: A convergence of evidence from neurobiology and epidemiology. Eur. Arch. Psychiatry Clin. Neurosci. 2006, 256, 174–186. [Google Scholar] [CrossRef]
- Gerson, R.; Rappaport, N. Traumatic stress and posttraumatic stress disorder in youth: Recent research findings on clinical impact, assessment, and treatment. J. Adolesc. Health 2013, 52, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Cicchetti, D.; Rogosch, F.A.; Gunnar, M.R.; Toth, S.L. The differential impacts of early physical and sexual abuse and internalizing problems on daytime cortisol rhythm in school-aged children. Child Dev. 2010, 81, 252–269. [Google Scholar] [CrossRef] [PubMed]
- Caspi, A.; Sugden, K.; Moffitt, T.E.; Taylor, A.; Craig, I.W.; Harrington, H.; McClay, J.; Mill, J.; Martin, J.; Braithwaite, A. Influence of life stress on depression: Moderation by a polymorphism in the 5-HTT gene. Science 2003, 301, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Sunley, A.K.; Lok, A.; White, M.J.; Snijder, M.B.; van Zuiden, M.; Zantvoord, J.B.; Derks, E.M. Ethnic and sex differences in the association of child maltreatment and depressed mood. The HELIUS study. Child Abus. Negl. 2020, 99, 104239. [Google Scholar] [CrossRef]
- Gallo, E.A.G.; Munhoz, T.N.; de Mola, C.L.; Murray, J. Gender differences in the effects of childhood maltreatment on adult depression and anxiety: A systematic review and meta-analysis. Child Abus. Negl. 2018, 79, 107–114. [Google Scholar] [CrossRef]
- Keijser, R. Depressive Symptoms among Adolescents and Young Adults: Psychometrics and the Influence of Family Environment, and Candidate Gene–Environment Interactions. Doctoral Dissertation, Uppsala University, Uppsala, Sweden, 2021. [Google Scholar]
- Lewis, A.J.; Kremer, P.; Douglas, K.; Toumborou, J.W.; Hameed, M.A.; Patton, G.C.; Williams, J. Gender differences in adolescent depression: Differential female susceptibility to stressors affecting family functioning. Aust. J. Psychol. 2015, 67, 131–139. [Google Scholar] [CrossRef]
- Weizmann Institute of Science. GeneCards the Human Gene Database PER2 Gene-Period Circadian Regulator. Available online: https://www.genecards.org/cgi-bin/carddisp.pl?gene=PER2 (accessed on 24 March 2023).
- Lavebratt, C.; Sjoholm, L.K.; Partonen, T.; Schalling, M.; Forsell, Y. PER2 Variantion Is Associated with Depression Vulnerability. Am. J. Med. Genet. B 2010, 153B, 570–581. [Google Scholar] [CrossRef]
- Ripperger, J.A.; Albrecht, U. The circadian clock component PERIOD2: From molecular to cerebral functions. Prog. Brain Res. 2012, 199, 233–245. [Google Scholar] [CrossRef] [PubMed]
- Hampp, G.; Ripperger, J.A.; Houben, T.; Schmutz, I.; Blex, C.; Perreau-Lenz, S.; Brunk, I.; Spanagel, R.; Ahnert-Hilger, G.; Meijer, J.H.; et al. Regulation of monoamine oxidase A by circadian-clock components implies clock influence on mood. Curr. Biol. 2008, 18, 678–683. [Google Scholar] [CrossRef]
- Spanagel, R.; Pendyala, G.; Abarca, C.; Zghoul, T.; Sanchis-Segura, C.; Magnone, M.C.; Lascorz, J.; Depner, M.; Holzberg, D.; Soyka, M. The clock gene Per2 influences the glutamatergic system and modulates alcohol consumption. Nat. Med. 2005, 11, 35–42. [Google Scholar] [CrossRef]
- Comasco, E.; Nordquist, N.; Göktürk, C.; Åslund, C.; Hallman, J.; Oreland, L.; Nilsson, K.W. The clock gene PER2 and sleep problems: Association with alcohol consumption among Swedish adolescents. Ups. J. Med. Sci. 2010, 115, 41–48. [Google Scholar] [CrossRef]
- McCarthy, M.J.; Fernandes, M.; Kranzler, H.R.; Covault, J.M.; Welsh, D.K. Circadian clock period inversely correlates with illness severity in cells from patients with alcohol use disorders. Alcohol. Clin. Exp. Res. 2013, 37, 1304–1310. [Google Scholar] [CrossRef]
- National Library of Medicine, National Center for Biotechnology Information. dbSNP Short Genetic Variations: rs56013859. Available online: https://www.ncbi.nlm.nih.gov/snp/?term=rs566013859 (accessed on 24 March 2023).
- SNPedia rs56013859. Available online: https://www.snpedia.com/index.php/Rs560138599 (accessed on 21 March 2023).
- Rose, A.B. Introns as Gene Regulators: A Brick on the Accelerator. Front. Genet. 2019, 9, 672. [Google Scholar] [CrossRef]
- Jo, B.S.; Choi, S.S. Introns: The Functional Benefits of Introns in Genomes. Genom. Inform. 2015, 13, 112–118. [Google Scholar] [CrossRef] [PubMed]
- OMIM, John Hopkins University. # 604348 Advanced Sleep Phase Syndrome, Familial, 1; FASPS1. Available online: https://www.omim.org/entry/604348 (accessed on 1 March 2023).
- Hoang, N.; Yuen, R.K.C.; Howe, J.; Drmic, I.; Ambrozewicz, P.; Russell, C.; Vorstman, J.; Weiss, S.K.; Anagnostou, E.; Malow, B.A.; et al. Sleep phenotype of individuals with autism spectrum disorder bearing mutations in the PER2 circadian rhythm gene. Am. J. Med. Genet. Part A 2021, 185, 1120–1130. [Google Scholar] [CrossRef] [PubMed]
- Gamble, K.L.; Motsinger-Reif, A.A.; Hida, A.; Borsetti, H.M.; Servick, S.V.; Ciarleglio, C.M.; Robbins, S.; Hicks, J.; Carver, K.; Hamilton, N. Shift work in nurses: Contribution of phenotypes and genotypes to adaptation. PLoS ONE 2011, 6, e18395. [Google Scholar] [CrossRef]
- Partonen, T.; Treutlein, J.; Alpman, A.; Frank, J.; Johansson, C.; Depner, M.; Aron, L.; Rietschel, M.; Wellek, S.; Soronen, P. Three circadian clock genes Per2, Arntl, and Npas2 contribute to winter depression. Ann. Med. 2007, 39, 229–238. [Google Scholar] [CrossRef] [PubMed]
- Hampp, G.; Albrecht, U. The circadian clock and mood-related behavior. Commun. Integr. Biol. 2008, 1, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Jiang, W.-G.; Li, S.-X.; Zhou, S.-J.; Sun, Y.; Shi, J.; Lu, L. Chronic unpredictable stress induces a reversible change of PER2 rhythm in the suprachiasmatic nucleus. Brain Res. 2011, 1399, 25–32. [Google Scholar] [CrossRef]
- Logan, R.W.; Edgar, N.; Gillman, A.G.; Hoffman, D.; Zhu, X.; McClung, C.A. Chronic stress induces brain region-specific alterations of molecular rhythms that correlate with depression-like behavior in mice. Biol. Psychiatry 2015, 78, 249–258. [Google Scholar] [CrossRef]
- Perreau-Lenz, S.; Spanagel, R. Clock genes× stress× reward interactions in alcohol and substance use disorders. Ann. Med. 2007, 49, 351–357. [Google Scholar] [CrossRef] [PubMed]
- Blomeyer, D.; Buchmann, A.F.; Lascorz, J.; Zimmermann, U.S.; Esser, G.; Desrivieres, S.; Schmidt, M.H.; Banaschewski, T.; Schumann, G.; Laucht, M. Association of PER2 genotype and stressful life events with alcohol drinking in young adults. PLoS ONE 2013, 8, e59136. [Google Scholar] [CrossRef] [PubMed]
- Johannessen, E.L.; Andersson, H.W.; Bjørngaard, J.H.; Pape, K. Anxiety and depression symptoms and alcohol use among adolescents—A cross sectional study of Norwegian secondary school students. BMC Public Health 2017, 17, 494. [Google Scholar] [CrossRef] [PubMed]
- Vadlin, S.; Aslund, C.; Nilsson, K.W. A longitudinal study of the individual- and group-level problematic gaming and associations with problem gambling among Swedish adolescents. Brain Behav. 2018, 8, e00949. [Google Scholar] [CrossRef] [PubMed]
- Svanborg, P.; Ekselius, L. Self-assessment of DSM-IV criteria for major depression in psychiatric out- and inpatients. Nord. J. Psychiatry 2003, 57, 291–296. [Google Scholar] [CrossRef]
- Rice, F.; Riglin, L.; Lomax, T.; Souter, E.; Potter, R.; Smith, D.; Thapar, A.; Thapar, A. Adolescent and adult differences in major depression symptom profiles. J. Affect. Disord. 2019, 243, 175–181. [Google Scholar] [CrossRef]
- Åslund, C.; Leppert, J.; Starrin, B.; Nilsson, K.W. Subjective social status and shaming experiences in relation to adolescent depression. Arch. Pediatr. Adolesc. Med. 2009, 163, 55–60. [Google Scholar] [CrossRef]
- Åslund, C.; Leppert, J.; Comasco, E.; Nordquist, N.; Oreland, L.; Nilsson, K.W. Impact of the interaction between the 5HTTLPR polymorphism and maltreatment on adolescent depression. A population-based study. Behav. Genet. 2009, 39, 524–531. [Google Scholar] [CrossRef]
- Hieronymus, F.; Emilsson, J.F.; Nilsson, S.; Eriksson, E. Consistent superiority of selective serotonin reuptake inhibitors over placebo in reducing depressed mood in patients with major depression. Mol. Psychiatry 2016, 21, 523–530. [Google Scholar] [CrossRef]
- Trivedi, M.H.; Rush, A.J.; Ibrahim, H.M.; Carmody, T.J.; Biggs, M.M.; Suppes, T.; Crismon, M.L.; Shores-Wilson, K.; Toprac, M.G.; Dennehy, E.B.; et al. The Inventory of Depressive Symptomatology, Clinician Rating (IDS-C) and Self-Report (IDS-SR), and the Quick Inventory of Depressive Symptomatology, Clinician Rating (QIDS-C) and Self-Report (QIDS-SR) in public sector patients with mood disorders: A psychometric evaluation. Psychol. Med. 2004, 34, 73–82. [Google Scholar] [CrossRef]
- Nordin, M.; Akerstedt, T.; Nordin, S. Psychometric evaluation and normative data for the Karolinska Sleep Questionnaire. Sleep Biol. Rhythm. 2013, 11, 216–226. [Google Scholar] [CrossRef]
- Aslund, C.; Nordquist, N.; Comasco, E.; Leppert, J.; Oreland, L.; Nilsson, K.W. Maltreatment, MAOA, and delinquency: Sex differences in gene-environment interaction in a large population-based cohort of adolescents. Behav. Genet. 2011, 41, 262–272. [Google Scholar] [CrossRef] [PubMed]
- Peacock Janet and Peacock, P. Oxford Handbook of Medical Statistics, 1st ed.; OUP Oxford: Oxford, UK, 2010; p. 544. [Google Scholar]
- Daryanto, A. Tutorial on heteroskedasticity using heteroskedasticityV3 SPSS macro. Quant. Methods Psychol. 2020, 16, 8–20. [Google Scholar] [CrossRef]
- Great Lakes e-Learning Services. Generalized Linear Model: What Does It Mean? Available online: https://www.mygreatlearning.com/blog/generalized-linear-models/ (accessed on 14 April 2023).
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- Hayes, A.F. PROCESS: A Versatile Computational Tool for Observed Variable Mediation, Moderation, and Conditional Process Modeling. 2012. Available online: https://www.afhayes.com/public/process2012.pdf (accessed on 21 July 2023).
- Hayes, A.F.; Cai, L. Using heteroskedasticity-consistent standard error estimators in OLS regression: An introduction and software implementation. Behav. Res. Methods 2007, 39, 709–722. [Google Scholar] [CrossRef]
- Bender, R.; Lange, S. Adjusting for multiple testing—When and how? J. Clin. Epidemiol. 2001, 54, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Gauderman, A. QUANTO 1.1: A Computer Program for Power and Sample Size Calculations for Genetic-Epidemiology Studies. 2006. Available online: https://www.semanticscholar.org (accessed on 21 July 2023).
- Dick, D.M.; Agrawal, A.; Keller, M.C.; Adkins, A.; Aliev, F.; Monroe, S.; Hewitt, J.K.; Kendler, K.S.; Sher, K.J. Candidate gene–environment interaction research: Reflections and recommendations. Perspect. Psychol. Sci. 2015, 10, 37–59. [Google Scholar] [CrossRef]
- Ozsoy, F.; Karakus, N.B.; Yigit, S.; Kulu, M. Effect of AUTS2 gene rs6943555 variant in male patients with schizophrenia in a Turkish population. Gene 2020, 756, 144913. [Google Scholar] [CrossRef] [PubMed]
- Fleiss, J.L. Significance tests have a role in epidemiologic research: Reactions to AM Walker. Am. J. Public Health 1986, 76, 559–560. [Google Scholar] [CrossRef]
- Ben-Efraim, Y.J.; Wasserman, D.; Wasserman, J.; Sokolowski, M. Family-based study of AVPR1B association and interaction with stressful life events on depression and anxiety in suicide attempts. Neuropsychopharmacology 2013, 38, 1504–1511. [Google Scholar] [CrossRef]
- Humphreys, K.L.; LeMoult, J.; Wear, J.G.; Piersiak, H.A.; Lee, A.; Gotlib, I.H. Child maltreatment and depression: A meta-analysis of studies using the Childhood Trauma Questionnaire. Child Abus. Negl. 2020, 102, 104361. [Google Scholar] [CrossRef]
- Partonen, T. Seasons, Clocks and Mood. In Neuroendocrine Clocks and Calendars; Springer: Cham, Switzerland, 2020; pp. 177–187. [Google Scholar]
- Partonen, T. Chronotype and Health Outcomes. Curr. Sleep Med. Rep. 2015, 1, 205–211. [Google Scholar] [CrossRef]
- Cao, R.; Gao, T.; Ren, H.; Hu, Y.; Qin, Z.; Liang, L.; Li, C.; Mei, S. Unique and cumulative effects of lifestyle-related behaviors on depressive symptoms among Chinese adolescents. Int. J. Soc. Psychiatry 2021, 68, 354–364. [Google Scholar] [CrossRef]
- Herman-Stahl, M.; Petersen, A.C. The protective role of coping and social resources for depressive symptoms among young adolescents. J. Youth Adolesc. 1996, 25, 733–753. [Google Scholar] [CrossRef]
- Aschard, H.; Chen, J.; Cornelis, M.C.; Chibnik, L.B.; Karlson, E.W.; Kraft, P. Inclusion of Gene-Gene and Gene-Environment Interactions Unlikely to Dramatically Improve Risk Prediction for Complex Diseases. Am. J. Hum. Genet. 2012, 90, 962–972. [Google Scholar] [CrossRef]
- Checknita, D.; Tiihonen, J.; Hodgins, S.; Nilsson, K.W. Associations of age, sex, sexual abuse, and genotype with monoamine oxidase a gene methylation. J. Neural Transm. 2021, 128, 1721–1739. [Google Scholar] [CrossRef]
- Hoth, K.F.; Voorhies, K.; Wu, A.C.; Lange, C.; Potash, J.B.; Lutz, S.M. The Role of Sex in Genetic Association Studies of Depression. J. Psychiatry Brain Sci. 2022, 7. [Google Scholar] [CrossRef]
- Kang, H.-J.; Park, Y.; Yoo, K.-H.; Kim, K.-T.; Kim, E.-S.; Kim, J.-W.; Kim, S.-W.; Shin, I.-S.; Yoon, J.-S.; Kim, J.H. Sex differences in the genetic architecture of depression. Sci. Rep. 2020, 10, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Angold, A.; Costello, E.; Erkanli, A.; Worthman, C. Pubertal changes in hormone levels and depression in girls. Psychol. Med. 1999, 29, 1043–1053. [Google Scholar] [CrossRef]
- Jiang, Z.; Rajamanickam, S.; Justice, N.J. CRF signaling between neurons in the paraventricular nucleus of the hypothalamus (PVN) coordinates stress responses. Neurobiol. Stress 2019, 11, 100192. [Google Scholar] [CrossRef] [PubMed]
- Labonté, B.; Engmann, O.; Purushothaman, I.; Menard, C.; Wang, J.; Tan, C.; Scarpa, J.R.; Moy, G.; Loh, Y.E.; Cahill, M.; et al. Sex-specific transcriptional signatures in human depression. Nat. Med. 2017, 23, 1102–1111. [Google Scholar] [CrossRef]
- Nutt, D.J. Relationship of neurotransmitters to the symptoms of major depressive disorder. J. Clin. Psychiatry 2008, 69, 4–7. [Google Scholar] [PubMed]
- Hirschfeld, R.M. History and evolution of the monoamine hypothesis of depression. J. Clin. Psychiatry 2000, 61, 4–6. [Google Scholar] [PubMed]
- Plotsky, P.M.; Owens, M.J.; Nemeroff, C.B. Psychoneuroendocrinology of depression: Hypothalamic-pituitary-adrenal axis. Psychiatr. Clin. N. Am. 1998, 21, 293–307. [Google Scholar] [CrossRef] [PubMed]
- Corella, D.; Ordovas, J.M. Basic Concepts in Molecular Biology Related to Genetics and Epigenetics. Rev. Esp. Cardiol. 2017, 70, 744–753. [Google Scholar] [CrossRef]
- Chorev, M.; Carmel, L. The function of introns. Front. Genet. 2012, 3, 55. [Google Scholar] [CrossRef]
- Jiang, S.; Postovit, L.; Cattaneo, A.; Binder, E.B.; Aitchison, K.J. Epigenetic modifications in stress response genes associated with childhood trauma. Front. Psychiatry 2019, 10, 808. [Google Scholar] [CrossRef] [PubMed]
- Chi-Castañeda, D.; Ortega, A. Circadian regulation of glutamate transporters. Front. Endocrinol. 2018, 9, 340. [Google Scholar] [CrossRef]
- Sanacora, G.; Treccani, G.; Popoli, M. Towards a glutamate hypothesis of depression: An emerging frontier of neuropsychopharmacology for mood disorders. Neuropharmacology 2012, 62, 63–77. [Google Scholar] [CrossRef]
- Onaolapo, A.Y.; Onaolapo, O.J. Glutamate and depression: Reflecting a deepening knowledge of the gut and brain effects of a ubiquitous molecule. World J. Psychiatry 2021, 11, 297–315. [Google Scholar] [CrossRef]
- Trullas, R.; Skolnick, P. Functional antagonists at the NMDA receptor complex exhibit antidepressant actions. Eur. J. Pharmacol. 1990, 185, 1–10. [Google Scholar] [CrossRef]
- Koike, H.; Chaki, S. Requirement of AMPA receptor stimulation for the sustained antidepressant activity of ketamine and LY341495 during the forced swim test in rats. Behav. Brain Res. 2014, 271, 111–115. [Google Scholar] [CrossRef] [PubMed]
- Kumar, P.; Kraal, A.Z.; Prawdzik, A.M.; Ringold, A.E.; Ellingrod, V. Dietary Glutamic Acid, Obesity, and Depressive Symptoms in Patients with Schizophrenia. Front. Psychiatry 2020, 11, 620097. [Google Scholar] [CrossRef]
- Baek, J.H.; Vignesh, A.; Son, H.; Lee, D.H.; Roh, G.S.; Kang, S.S.; Cho, G.J.; Choi, W.S.; Kim, H.J. Glutamine Supplementation Ameliorates Chronic Stress-induced Reductions in Glutamate and Glutamine Transporters in the Mouse Prefrontal Cortex. Exp. Neurobiol. 2019, 28, 270–278. [Google Scholar] [CrossRef]
- Scarr, S. Developmental theories for the 1990s: Development and individual differences. Child Dev. 1992, 63, 1–19. [Google Scholar] [CrossRef]
- Schønning, V.; Sivertsen, B.; Hysing, M.; Dovran, A.; Askeland, K.G. Childhood maltreatment and sleep in children and adolescents: A systematic review and meta-analysis. Sleep Med. Rev. 2022, 63, 101617. [Google Scholar] [CrossRef] [PubMed]
- Sekowski, M.; Gambin, M.; Cudo, A.; Wozniak-Prus, M.; Penner, F.; Fonagy, P.; Sharp, C. The relations between childhood maltreatment, shame, guilt, depression and suicidal ideation in inpatient adolescents. J. Affect. Disord. 2020, 276, 667–677. [Google Scholar] [CrossRef] [PubMed]
- Wray, N.R.; Pergadia, M.L.; Blackwood, D.H.; Penninx, B.W.; Gordon, S.D.; Nyholt, D.R.; Ripke, S.; MacIntyre, D.J.; McGhee, K.A.; Maclean, A.W.; et al. Genome-wide association study of major depressive disorder: New results, meta-analysis, and lessons learned. Mol. Psychiatry 2012, 17, 36–48. [Google Scholar] [CrossRef]
- Park, J.-H.; Gail, M.H.; Weinberg, C.R.; Carroll, R.J.; Chung, C.C.; Wang, Z.; Chanock, S.J.; Fraumeni, J.F.; Chatterjee, N. Distribution of allele frequencies and effect sizes and their interrelationships for common genetic susceptibility variants. Proc. Natl. Acad. Sci. USA 2011, 108, 18026–18031. [Google Scholar] [CrossRef] [PubMed]
- Nilsson, K.W.; Sjöberg, R.L.; Wargelius, H.L.; Leppert, J.; Lindström, L.; Oreland, L. The monoamine oxidase A (MAO-A) gene, family function and maltreatment as predictors of destructive behaviour during male adolescent alcohol consumption. Addiction 2007, 102, 389–398. [Google Scholar] [CrossRef]
- Nilsson, K.W.; Wargelius, H.L.; Sjöberg, R.L.; Leppert, J.; Oreland, L. The MAO-A gene, platelet MAO-B activity and psychosocial environment in adolescent female alcohol-related problem behaviour. Drug Alcohol Depend. 2008, 93, 51–62. [Google Scholar] [CrossRef]
- Strawbridge, R.; Young, A.H.; Cleare, A.J. Biomarkers for depression: Recent insights, current challenges and future prospects. Neuropsychiatr. Dis. Treat. 2017, 13, 1245–1262. [Google Scholar] [CrossRef] [PubMed]
- Rodenburg, R.J. The functional genomics laboratory: Functional validation of genetic variants. J. Inherit. Metab. Dis. 2018, 41, 297–307. [Google Scholar] [CrossRef] [PubMed]
- Reis, A. PCR in Linkage Analysis of Genetic Diseases. In PCR Topics: Usage of Polymerase Chain Reaction in Genetic and Infectious Diseases; Rolfs, A., Schumacher, H.C., Marx, P., Eds.; Springer: Berlin/Heidelberg, Germany, 1991; pp. 75–79. [Google Scholar]




| 2012 sample (n = 1834) | |||||
| Missing n (%) | n (%) | Female | Male | X2/Z (p) | |
| Sex b (%) | 1019 (56) | 815 (44) | |||
| Age, years a (SD) | 14.4 (1) | 14.4 (1) | NS | ||
| Thoughts of death and suicide b | 7 (0.4) | ||||
| No | 893 | 750 | |||
| Yes | 184 (10.1) | 124 (6.8) | 60 (3.2) | *** | |
| Core depressive symptoms index a Mean (SD) | 22 (1.2) | 1007 1.737 (2.184) | 805 0.906 (1.495) | *** | |
| Sleep complaints index a Mean (SD) | 151 (8.23) | 928 12.831 (9.435) | 755 10.535 (8.065) | *** | |
| Family maltreatment index a Mean (SD) | 33 (1.86) | 964 4.875 (1.905) | 775 4.698 (1.375) | NS | |
| PER2: rs56013859 b | 157 (8.6) | NS | |||
| T:T (%) | 1288 (76.8) | 733 (77.5) | 555 (75.9) | ||
| C:T/C:C (%) | 389 (23.2) | 213 (22.5) | 176 (24.1) | ||
| 2015 sample (n = 1644) | |||||
| Missing n (%) | n (%) | Female | Male | X2/Z (p) | |
| Sex b (%) | 961 (58.4) | 683 (41.6) | |||
| Age, years a (SD) | 2 (0.12) | 17.3 (1) | 17.3 (1) | NS | |
| Core depressive symptoms index a Mean (SD) | 24 (1.5) | 943 2.787 (2.49) | 667 1.3 (1.86) | *** | |
| Sleep complaints index a Mean (SD) | 64 (3.9) | 928 20.125 (10.689) | 615 15.081 (9.958) | *** | |
| Family maltreatment index a Mean (SD) | 87 (5.29) | 901 0.842 (1.843) | 656 0.675 (1.358) | NS | |
| PER2: rs56013859 b | 184 (11.2) | NS | |||
| T:T (%) | 1122 (76) | 961 (77) | 461 (76.6) | ||
| C:T/C:C (%) | 338 (23) | 184 (23) | 141 (23.4) | ||
| 2018 sample (n = 1212) | |||||
| Missing n (%) | n (%) | Female | Male | X2/Z (p) | |
| Sex b (%) | 753 (62.1) | 459 (37.9) | |||
| Age years a (SD) | 20.4 (1) | 20.4 (1) | NS | ||
| Thoughts of death and suicide b | |||||
| No | 605 | 378 | |||
| Yes | 201 (19.25) | 148 (12.2) | 81 (6.7) | NS | |
| Core depressive symptoms index a Mean (SD) | 1 (0.01) | 752 2.778 (2.584) | 459 1.593 (2.275) | *** | |
| Sleep complaints index a Mean (SD) | 8 (0.7) | 749 20.427 (10.972) | 455 17.317 (10.068) | *** | |
| Family maltreatment index a Mean (SD) | 53 (4.37) | 715 0.857 (1.91) | 444 0.664 (1.328) | NS | |
| PER2: rs56013859 b | 123 (10.15) | NS | |||
| T:T (%) | 828 (76) | 520 (76.1) | 308 (75.9) | ||
| C:T/C:C (%) | 261 (24) | 163 (23.9) | 98 (24.1) | ||
| Independent Variables | p | β | (95% CI) |
|---|---|---|---|
| Sex | <0.001 | 1.905 | (1.553 to 2.336) |
| rs56013859 | 0.682 | 0.949 | (0.74 to 1.218) |
| Family maltreatment | <0.001 | 1.379 | (1.214 to 1.566) |
| Sex 1 × rs56013859 2 | 0.844 | 1.042 | (0.69 to 1.576) |
| Sex 1 × Family maltreatment | 0.925 | 1.008 | (0.851 to 1.194) |
| rs56013859 2 × Family maltreatment | 0.211 | 0.875 | (0.71 to 1.078) |
| Sex 1 × rs56013859 2 × Family maltreatment | 0.025 | 1.451 | (1.048 to 2.009) |
| χ2 = 231.685 | <0.001 |
| Independent Variables | p | β | (95% CI) |
|---|---|---|---|
| Sex | <0.001 | 2.845 | (1.958 to 4.135) |
| rs56013859 | 0.292 | 0.74 | (0.423 to 1.294) |
| Family maltreatment | 0.308 | 1.111 | (0.908 to 1.358) |
| Sex 1 × rs56013859 2 | 0.258 | 1.544 | (0.727 to 3.281) |
| Sex 1 × Family maltreatment | 0.52 | 1.077 | (0.859 to 1.349) |
| rs56013859 2 × Family maltreatment | 0.172 | 1.34 | (0.881 to 2.038) |
| Sex 1 × rs56013859 2 × Family maltreatment | 0.044 | 0.592 | (0.355 to 0.986) |
| χ2 = 70.428 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Torres Soler, C.; Kanders, S.H.; Rehn, M.; Olofsdotter, S.; Åslund, C.; Nilsson, K.W. A Three-Way Interaction of Sex, PER2 rs56013859 Polymorphism, and Family Maltreatment in Depressive Symptoms in Adolescents. Genes 2023, 14, 1723. https://doi.org/10.3390/genes14091723
Torres Soler C, Kanders SH, Rehn M, Olofsdotter S, Åslund C, Nilsson KW. A Three-Way Interaction of Sex, PER2 rs56013859 Polymorphism, and Family Maltreatment in Depressive Symptoms in Adolescents. Genes. 2023; 14(9):1723. https://doi.org/10.3390/genes14091723
Chicago/Turabian StyleTorres Soler, Catalina, Sofia H. Kanders, Mattias Rehn, Susanne Olofsdotter, Cecilia Åslund, and Kent W. Nilsson. 2023. "A Three-Way Interaction of Sex, PER2 rs56013859 Polymorphism, and Family Maltreatment in Depressive Symptoms in Adolescents" Genes 14, no. 9: 1723. https://doi.org/10.3390/genes14091723