
Risk-Stratified Breast Cancer Screening Incorporating a Polygenic Risk Score: A Survey of UK General Practitioners’ Knowledge and Attitudes

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey Population and Administration
2.2. Survey Design
- GP role
- Years of experience
- Location of practice
- Gender
- Ethnicity
- Familiarity with the concept of PRS
- Confidence communicating to a patient:
- ○
- polygenic inheritance
- ○
- advantages and disadvantages of a personalised breast cancer risk assessment (PBCRA)
- ○
- PBCRA result as a 10-year absolute risk
- Views on the current National Health Service Breast Screening Programme (NHSBSP) (Likert)
- Views on different targeted screening approaches (Likert)
- Perception of potential impact of risk-stratified screening (sliding scale):
- ○
- on both patients
- ○
- on general practice
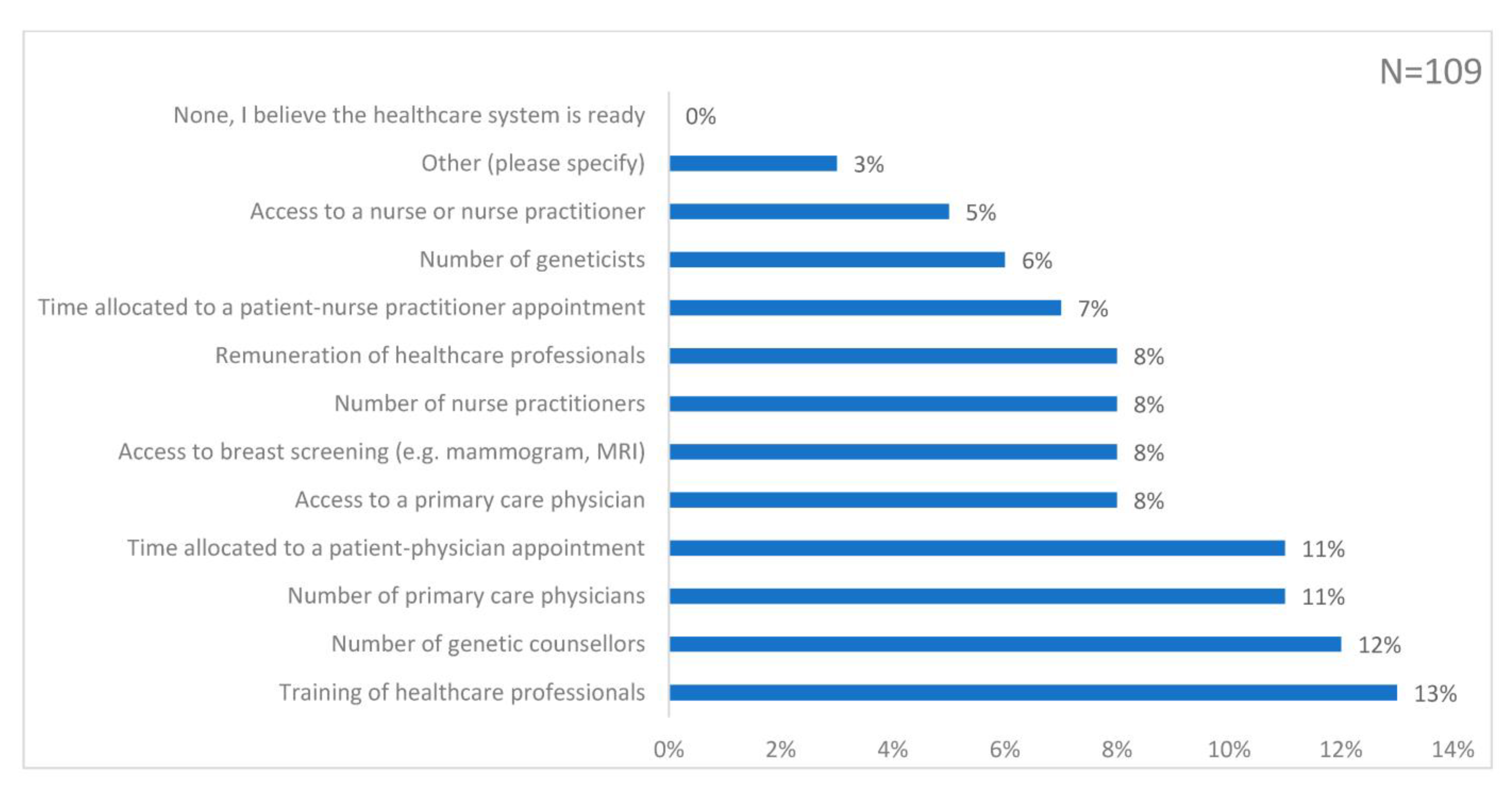
- Views on aspects of the NHS that would need to be enhanced to deliver risk-stratified screening (multiple choice question, MCQ)
- Desired clinical resources
- Formats for learning more about risk-stratified screening
- How they received the survey
- Any additional comments
2.3. Statistical Analysis
3. Results
3.1. Characteristics of Survey Respondents
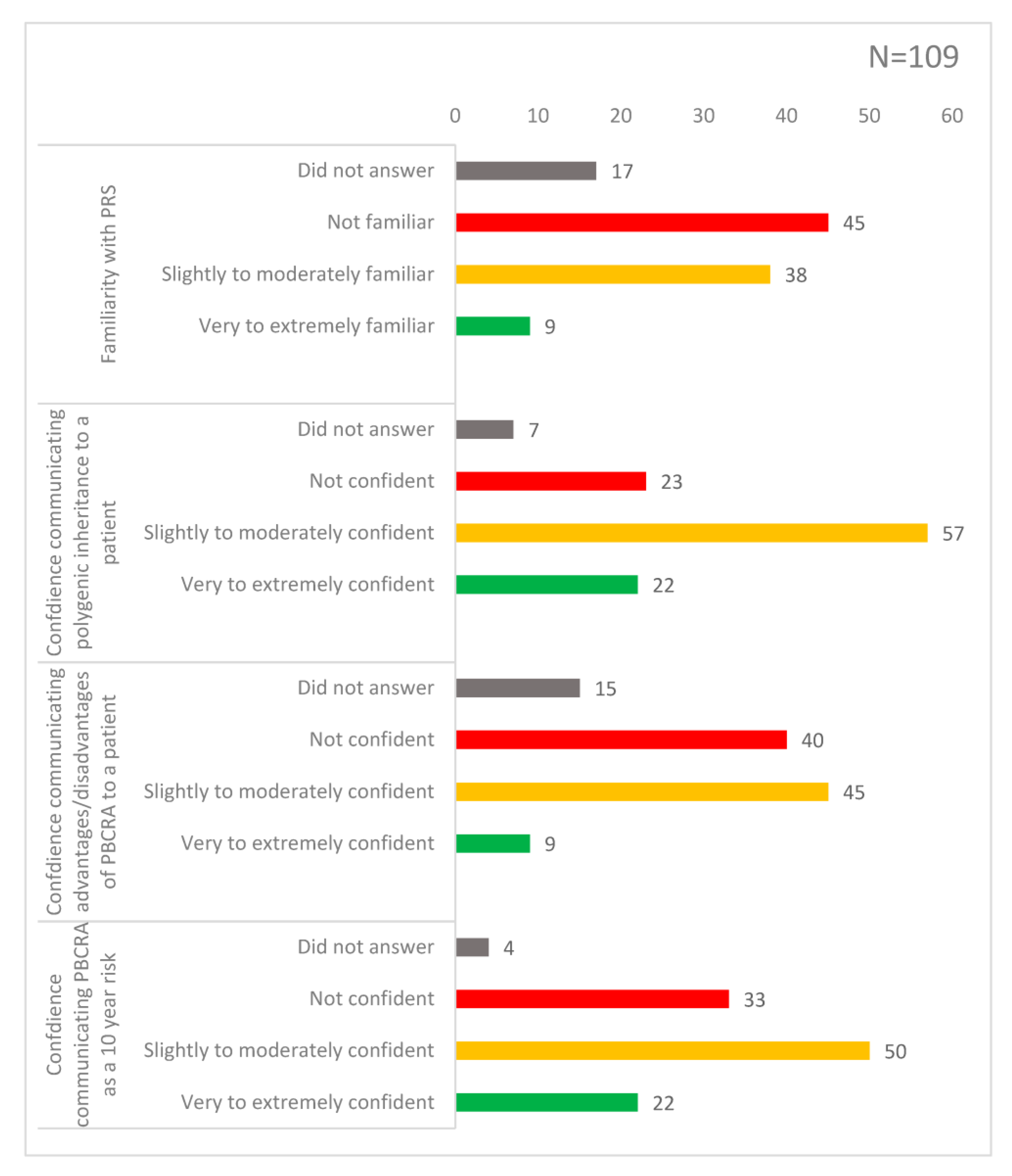
3.2. Knowledge of PRS and Risk-Stratified Screening Incorporating PRS
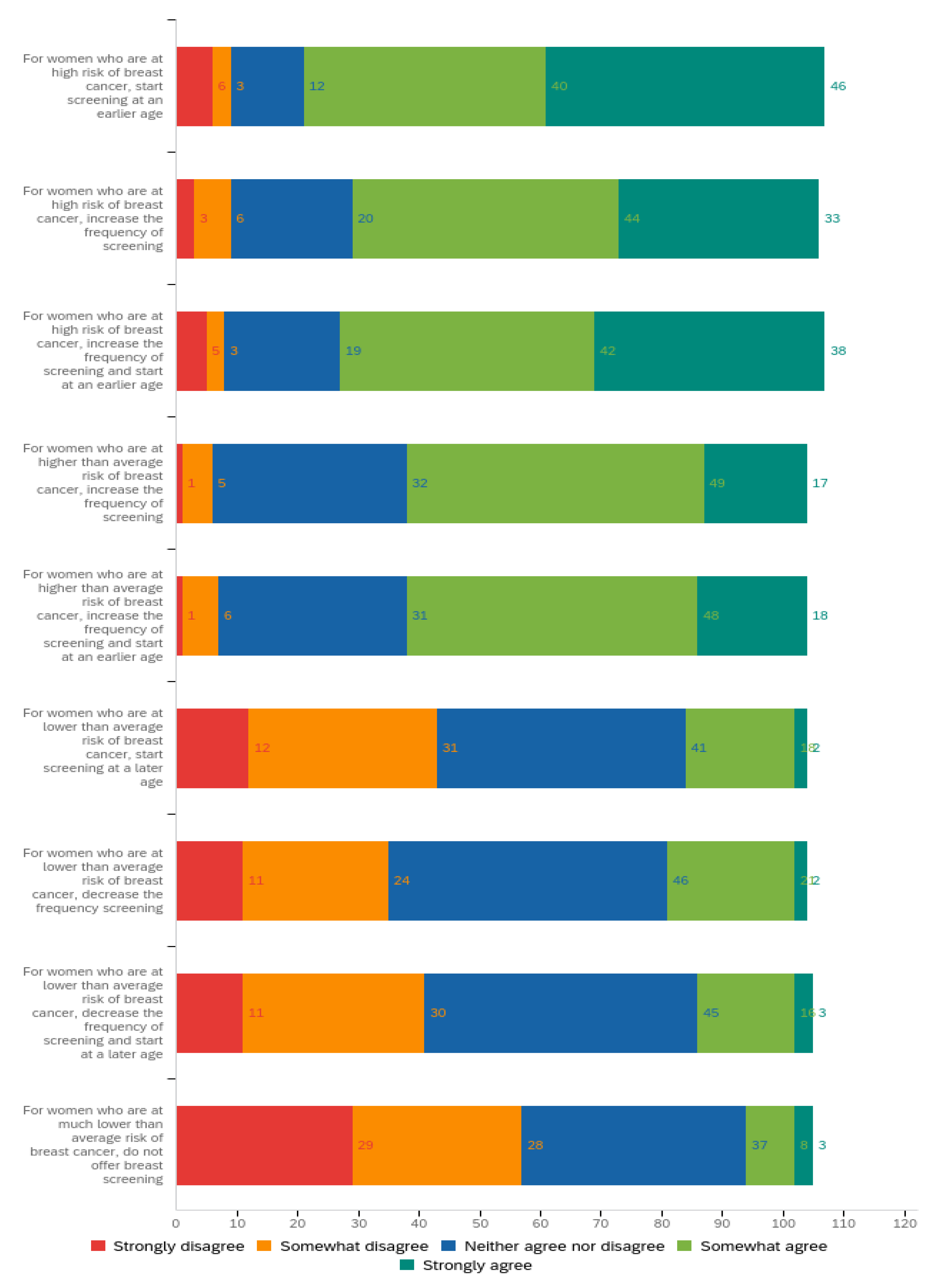
3.3. Attitudes towards Future Implementation of Risk-Stratified Screening
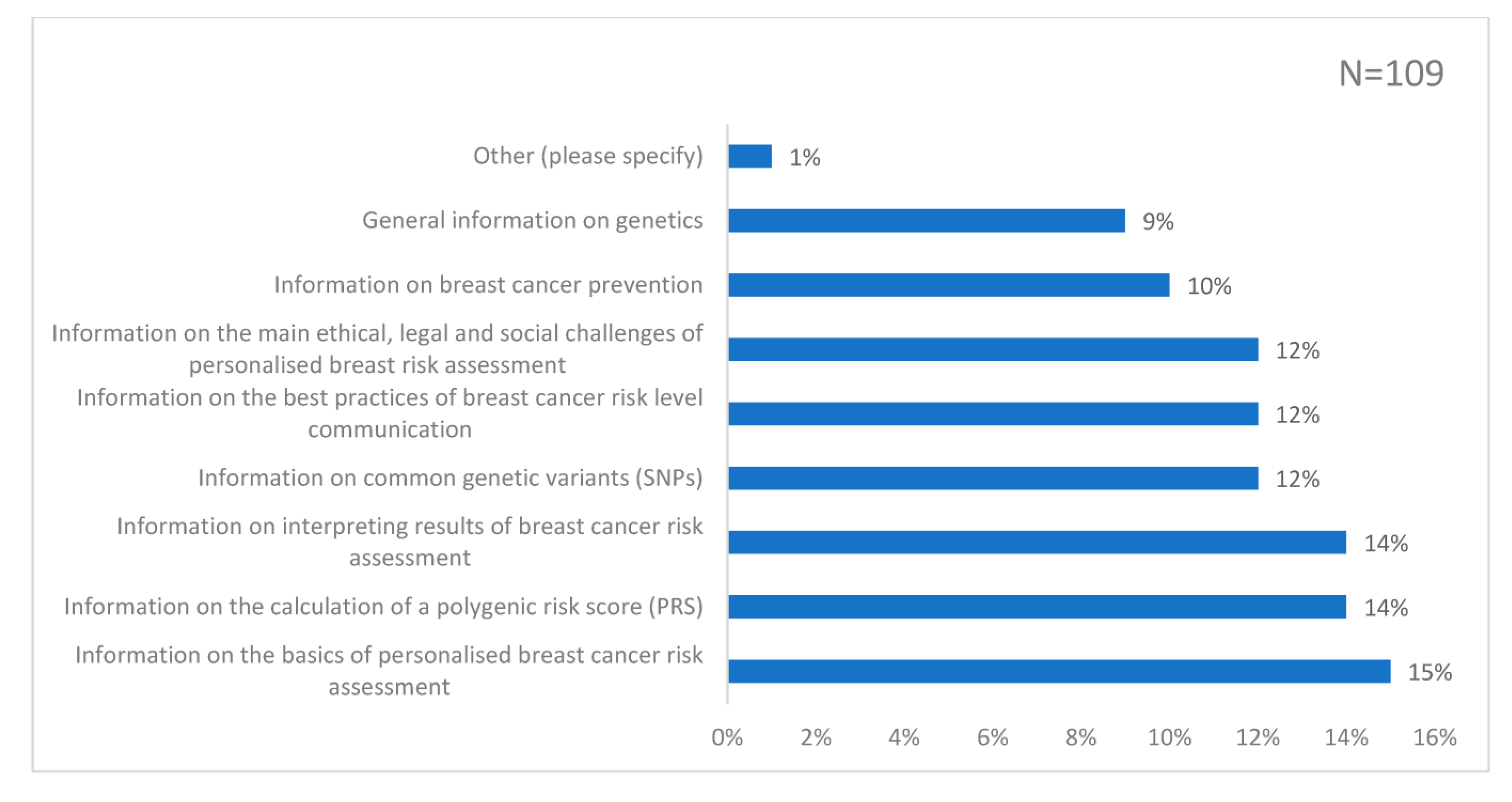
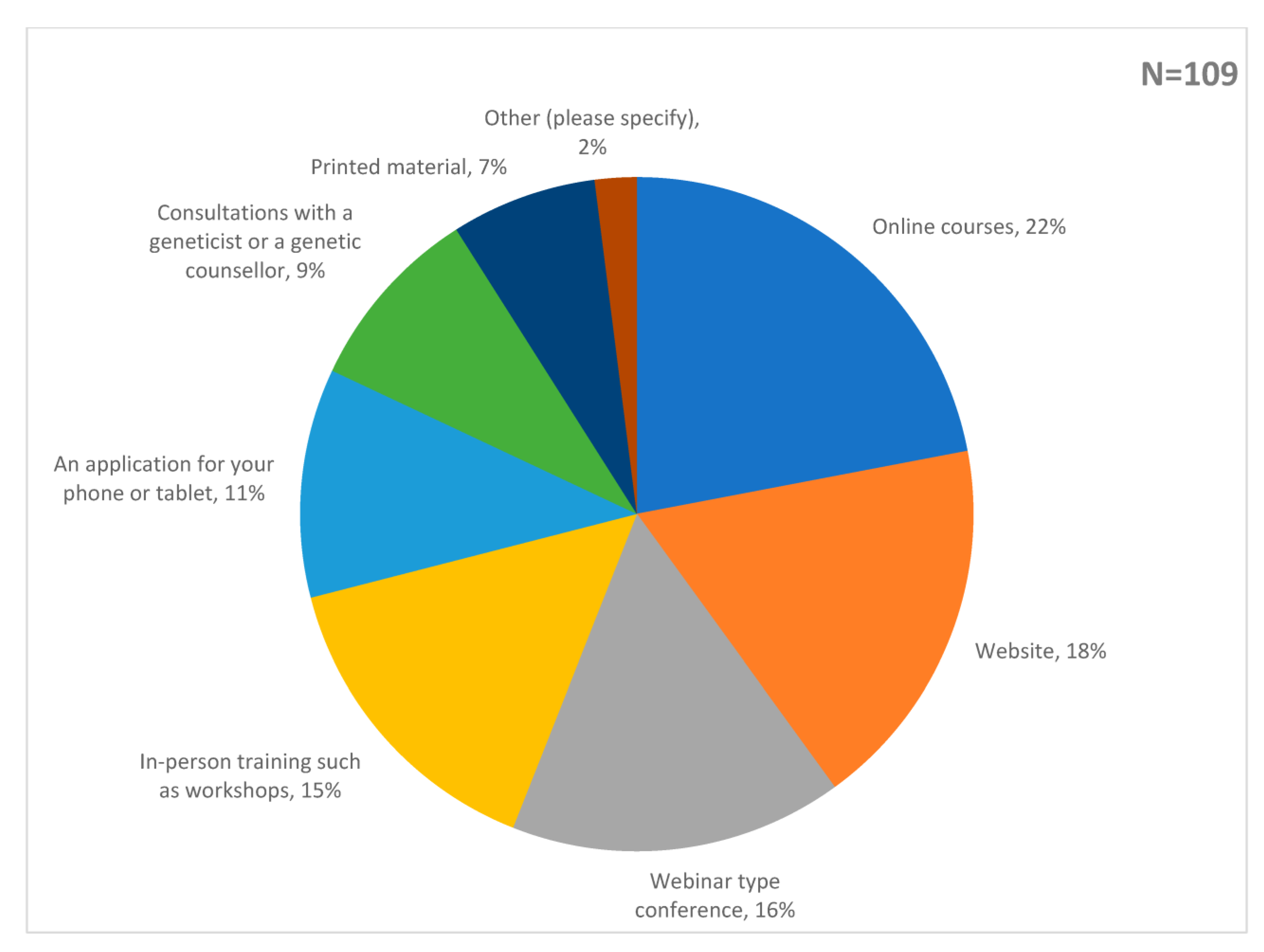
3.4. Preferences for Future Learning about Risk-Stratified Screening
4. Discussion
4.1. Main Findings
4.2. Strengths and Limitations
4.3. Comparison with Existing Literature
4.3.1. Familiarity with PRS and Confidence Communicating PBCRA Is Low amongst GPs
4.3.2. GPs Support Risk-Stratified Screening but Have Reservations about a Low-Risk Screening Pathway
4.3.3. Risk-Stratified Screening Requires Evaluation of Potential Psychological Harms to Women
4.3.4. More Research Is Needed to Evaluate the Effects of Risk Stratification on Health Inequity
4.4. Implications for Research and Practice
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Evans, D.G.; Howell, S.J.; Gandhi, A.; van Veen, E.M.; Woodward, E.R.; Harvey, J.; Barr, L.; Wallace, A.; Lalloo, F.; Wilson, M.; et al. Breast cancer incidence and early diagnosis in a family history risk and prevention clinic: 33-year experience in 14,311 women. Breast Cancer Res. Treat. 2021, 189, 677–687. [Google Scholar] [CrossRef] [PubMed]
- Pashayan, N.; Morris, S.; Gilbert, F.J.; Pharoah, P.D.P. Cost-effectiveness and Benefit-to-Harm Ratio of Risk-Stratified Screening for Breast Cancer: A Life-Table Model. JAMA Oncol. 2018, 4, 1504–1510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Independent UK Panel on Breast Cancer Screening. The benefits and harms of breast cancer screening: An independent review. Lancet 2012, 380, 1778–1786. [Google Scholar] [CrossRef]
- Lee, A.; Mavaddat, N.; Wilcox, A.N.; Cunningham, A.P.; Carver, T.; Hartley, S.; de Villiers, C.B.; Izquierdo, A.; Simard, J.; Schmidt, M.K.; et al. BOADICEA: A comprehensive breast cancer risk prediction model incorporating genetic and nongenetic risk factors. Genet. Med. 2019, 21, 1708–1718. [Google Scholar] [CrossRef] [Green Version]
- Blyuss, O.; Dibden, A.; Massat, N.J.; Parmar, D.; Cuzick, J.; Duffy, S.W.; Sasieni, P. A case–control study to evaluate the impact of the breast screening programme on breast cancer incidence in England. Cancer Med. 2022. [Google Scholar] [CrossRef]
- Long, H.; Brooks, J.M.; Harvie, M.; Maxwell, A.; French, D.P. How do women experience a false-positive test result from breast screening? A systematic review and thematic synthesis of qualitative studies. Br. J. Cancer 2019, 121, 351–358. [Google Scholar] [CrossRef] [Green Version]
- Wand, H.; Lambert, S.A.; Tamburro, C.; Iacocca, M.A.; O’Sullivan, J.W.; Sillari, C.; Kullo, I.J.; Rowley, R.; Dron, J.S.; Brockman, D.; et al. Improving reporting standards for polygenic scores in risk prediction studies. Nature 2021, 591, 211–219. [Google Scholar] [CrossRef]
- Mavaddat, N.; Michailidou, K.; Dennis, J.; Lush, M.; Fachal, L.; Lee, A.; Tyrer, J.P.; Chen, T.H.; Wang, Q.; Bolla, M.K.; et al. Polygenic Risk Scores for Prediction of Breast Cancer and Breast Cancer Subtypes. Am. J. Hum. Genet. 2019, 104, 21–34. [Google Scholar] [CrossRef] [Green Version]
- Wolfson, M.; Gribble, S.; Pashayan, N.; Easton, D.F.; Antoniou, A.C.; Lee, A.; van Katwyk, S.; Simard, J. Potential of polygenic risk scores for improving population estimates of women’s breast cancer genetic risks. Genet. Med. 2021, 23, 2114–2121. [Google Scholar] [CrossRef]
- Evans, D.G.R.; van Veen, E.M.; Harkness, E.F.; Brentnall, A.R.; Astley, S.M.; Byers, H.; Woodward, E.R.; Sampson, S.; Southworth, J.; Howell, S.J.; et al. Breast cancer risk stratification in women of screening age: Incremental effects of adding mammographic density, polygenic risk, and a gene panel. Genet. Med. 2022, 24, 1485–1494. [Google Scholar] [CrossRef]
- MyPeBS. Home Page—MyPeBS. 2022. Available online: https://www.mypebs.eu/ (accessed on 30 September 2022).
- Esserman, L.J. The WISDOM Study: Breaking the deadlock in the breast cancer screening debate. NPJ Breast Cancer 2017, 3, 1–7. [Google Scholar] [CrossRef] [PubMed]
- French, D.P.; Woof, V.G.; Ruane, H.; Evans, D.G.; Ulph, F.; Donnelly, L.S. The feasibility of implementing risk stratification into a national breast cancer screening programme: A focus group study investigating the perspectives of healthcare personnel responsible for delivery. BMC Womens Health 2022, 22, 142. [Google Scholar] [CrossRef] [PubMed]
- Brooks, J.D.; Nabi, H.H.; Andrulis, I.L.; Antoniou, A.C.; Chiquette, J.; Despres, P.; Devilee, P.; Dorval, M.; Droit, A.; Easton, D.F.; et al. Personalized Risk Assessment for Prevention and Early Detection of Breast Cancer: Integration and Implementation (PERSPECTIVE I&I). J. Pers. Med. 2021, 11, 511. [Google Scholar] [PubMed]
- Brédart, A.; De Pauw, A.; Tüchler, A.; Lakeman, I.M.M.; Anota, A.; Rhiem, K.; Schmutzler, R.; van Asperen, C.J.; Devilee, P.; Stoppa-Lyonnet, D.; et al. Genetic clinicians’ confidence in BOADICEA comprehensive breast cancer risk estimates and counselees’ psychosocial outcomes: A prospective study. Clin. Genet. 2022, 102, 30–39. [Google Scholar] [CrossRef]
- Esquivel-Sada, D.; Lévesque, E.; Hagan, J.; Knoppers, B.M.; Simard, J. Envisioning Implementation of a Personalized Approach in Breast Cancer Screening Programs: Stakeholder Perspectives. Heal. Policy 2019, 15, 39–54. [Google Scholar] [CrossRef]
- Woof, V.G.; McWilliams, L.; Donnelly, L.S.; Howell, A.; Evans, D.G.; Maxwell, A.J.; French, D.P. Introducing a low-risk breast screening pathway into the NHS Breast Screening Programme: Views from healthcare professionals who are delivering risk-stratified screening. Womens Health 2021, 17, 17455065211009746. [Google Scholar] [CrossRef]
- Smit, A.K.; Sharman, A.R.; Espinoza, D.; Wallingford, C.; Young, M.A.; Dunlop, K.; Tiller, J.; Newson, A.J.; Meiser, B.; Cust, A.E.; et al. Knowledge, views and expectations for cancer polygenic risk testing in clinical practice: A cross-sectional survey of health professionals. Clin. Genet. 2021, 100, 430–439. [Google Scholar] [CrossRef]
- Lapointe, J.; Buron, A.-C.; Mbuya-Bienge, C.; Dorval, M.; Pashayan, N.; Brooks, J.D.; Walker, M.J.; Chiquette, J.; Eloy, L.; Blackmore, K.; et al. Polygenic risk scores and risk-stratified breast cancer screening: Familiarity and perspectives of health care professionals. Genet. Med. 2022, 24, 2380–2388. [Google Scholar] [CrossRef]
- Adeyemo, A.; Balaconis, M.K.; Darnes, D.R.; Fatumo, S.; Moreno, P.G.; Hodonsky, C.J.; Inouye, M.; Kanai, M.; Kato, K.; Knoppers, B.M.; et al. Responsible use of polygenic risk scores in the clinic: Potential benefits, risks and gaps. Nat. Med. 2021, 27, 1876–1884. [Google Scholar]
- Marcon, A.R.; Bieber, M.; Caulfield, T. Representing a “revolution”: How the popular press has portrayed personalized medicine. Genet. Med. 2018, 20, 950–956. [Google Scholar] [CrossRef] [Green Version]
- Puzhko, S.; Gagnon, J.; Simard, J.; Knoppers, B.M.; Siedlikowski, S.; Bartlett, G. Health professionals’ perspectives on breast cancer risk stratification: Understanding evaluation of risk versus screening for disease. Public Health Rev. 2019, 40, 2. [Google Scholar] [CrossRef] [Green Version]
- Qualtrics. Qualtrics XM—Experience Management Software. 2022. Available online: https://www.qualtrics.com/ (accessed on 30 September 2022).
- General Medical Council. What our data tell us about general practitioners working in the UK in England and Scotland. 2018. Available online: https://www.gmc-uk.org/-/media/documents/what-our-data-tells-us-about-gps_pdf-74830685.pdf (accessed on 30 September 2022).
- French, D.P.; Astley, S.; Brentnall, A.R.; Cuzick, J.; Dobrashian, R.; Duffy, S.W.; Gorman, L.S.; Harkness, E.F.; Harrison, F.; Harvie, M.; et al. What are the benefits and harms of risk stratified screening as part of the NHS breast screening Programme? Study protocol for a multi-site non-randomised comparison of BC-predict versus usual screening (NCT04359420). BMC Cancer 2020, 20, 570. [Google Scholar] [CrossRef] [PubMed]
- Lewis, A.C.F.; Green, R.C. Polygenic risk scores in the clinic: New perspectives needed on familiar ethical issues. Genome Med. 2021, 13, 14. [Google Scholar] [CrossRef] [PubMed]
- Venning, B.; Saya, S.; De Abreu Lourenco, R.; Street, D.J.; Emery, J.D. Preferences for a polygenic test to estimate cancer risk in a general Australian population. Genet. Med. 2022, 24, 2144–2154. [Google Scholar] [CrossRef] [PubMed]
- Morrow, A.; Chan, P.; Tucker, K.M.; Taylor, N. The design, implementation, and effectiveness of intervention strategies aimed at improving genetic referral practices: A systematic review of the literature. Genet. Med. 2021, 23, 2239–2249. [Google Scholar] [CrossRef]
- Nippert, I.; Harris, H.; Julian-Reynier, C.; Kristoffersson, U.; Kate, L.; Anionwu, E.; Benjamin, C.; Challen, K.; Schmidtke, J.; Nippert, R.; et al. Confidence of primary care physicians in their ability to carry out basic medical genetic tasks—A European survey in five countries-Part 1. J. Community Genet. 2011, 2, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Das Gupta, K.; Gregory, G.; Meiser, B.; Kaur, R.; Scheepers-Joynt, M.; McInerny, S.; Taylor, S.; Barlow-Stewart, K.; Antill, Y.; Salmon, L.; et al. Communicating polygenic risk scores in the familial breast cancer clinic. Patient Educ. Couns. 2021, 104, 2512–2521. [Google Scholar] [CrossRef]
- Gregory, G.; Gupta, K.D.; Meiser, B.; Barlow-Stewart, K.; Geelan-Small, P.; Kaur, R.; Scheepers-Joynt, M.; McInerny, S.; Taylor, S.; Antill, Y.; et al. Polygenic risk in familial breast cancer: Changing the dynamics of communicating genetic risk. J. Genet. Couns. 2022, 31, 120–129. [Google Scholar] [CrossRef]
- McGuinness, M.; Fassi, E.; Wang, C.; Hacking, C.; Ellis, V. Breast cancer polygenic risk scores in the clinical cancer genetic counseling setting: Current practices and impact on patient management. J. Genet. Couns. 2021, 30, 588–597. [Google Scholar] [CrossRef]
- Wilkes, M.S.; Day, F.C.; Fancher, T.L.; McDermott, H.; Lehman, E.; Bell, R.A.; Green, M.J. Increasing confidence and changing behaviors in primary care providers engaged in genetic counselling. BMC Med. Educ. 2017, 17, 163. [Google Scholar] [CrossRef] [Green Version]
- Carroll, J.C.; Allanson, J.; Morrison, S.; Miller, F.A.; Wilson, B.J.; Permaul, J.A.; Telner, D. Informing Integration of Genomic Medicine Into Primary Care: An Assessment of Current Practice, Attitudes, and Desired Resources. Front. Genet. 2019, 10, 1189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Institute for Clinical Excellence. Overview—Familial Breast Cancer: Classification, Care and Managing Breast Cancer and Related Risks in People with a Family History of Breast Cancer. 2022. Available online: https://www.nice.org.uk/guidance/cg164 (accessed on 30 September 2022).
- Sierra, M.A.; Wheeler, J.C.; Devereux, L.; Trainer, A.H.; Keogh, L. Exploring Implementation of Personal Breast Cancer Risk Assessments. J. Pers. Med. 2021, 11, 992. [Google Scholar] [CrossRef] [PubMed]
- Meisel, S.F.; Pashayan, N.; Rahman, B.; Side, L.; Fraser, L.; Gessler, S.; Lanceley, A.; Wardle, J. Adjusting the frequency of mammography screening on the basis of genetic risk: Attitudes among women in the UK. Breast 2015, 24, 237–241. [Google Scholar] [CrossRef] [Green Version]
- Koitsalu, M.; Sprangers, M.A.; Eklund, M.; Czene, K.; Hall, P.; Gronberg, H.; Brandberg, Y. Public interest in and acceptability of the prospect of risk-stratified screening for breast and prostate cancer. Acta Oncol. 2016, 55, 45–51. [Google Scholar] [CrossRef] [Green Version]
- Wheeler, J.C.W.; Keogh, L.; Sierra, M.A.; Devereux, L.; Jones, K.; MJ, I.J.; Trainer, A.H. Heterogeneity in how women value risk-stratified breast screening. Genet. Med. 2022, 24, 146–156. [Google Scholar] [CrossRef]
- Rainey, L.; van der Waal, D.; Donnelly, L.S.; Southworth, J.; French, D.P.; Evans, D.G.; Broeders, M.J. Women’s health behaviour change after receiving breast cancer risk estimates with tailored screening and prevention recommendations. BMC Cancer 2022, 22, 1–13. [Google Scholar] [CrossRef]
- Dunlop, K.; Rankin, N.M.; Smit, A.K.; Salgado, Z.; Newson, A.J.; Keogh, L.; Cust, A.E. Acceptability of risk-stratified population screening across cancer types: Qualitative interviews with the Australian public. Health Expect. 2021, 24, 1326–1336. [Google Scholar] [CrossRef]
- French, D.P.; Howell, A.; Evans, D.G. Psychosocial issues of a population approach to high genetic risk identification: Behavioural, emotional and informed choice issues. Breast 2018, 37, 148–153. [Google Scholar] [CrossRef] [Green Version]
- Young, M.A.; Forrest, L.E.; Rasmussen, V.M.; James, P.; Mitchell, G.; Sawyer, S.D.; Reeve, K.; Hallowell, N. Making Sense of SNPs: Women’s Understanding and Experiences of Receiving a Personalized Profile of Their Breast Cancer Risks. J. Genet. Couns. 2018, 27, 702–708. [Google Scholar] [CrossRef]
- Yanes, T.; Meiser, B.; Kaur, R.; Scheepers-Joynt, M.; McInerny, S.; Taylor, S.; Barlow-Stewart, K.; Antill, Y.; Salmon, L.; Smyth, C.; et al. Uptake of polygenic risk information among women at increased risk of breast cancer. Clin. Genet. 2020, 97, 492–501. [Google Scholar] [CrossRef]
- Yanes, T.; Kaur, R.; Meiser, B.; Scheepers-Joynt, M.; McInerny, S.; Barlow-Stewart, K.; Antill, Y.; Salmon, L.; Smyth, C.; James, P.A.; et al. Women’s responses and understanding of polygenic breast cancer risk information. Fam. Cancer 2020, 19, 297–306. [Google Scholar] [CrossRef]
- Willis, A.M.; Smith, S.K.; Meiser, B.; James, P.A.; Ballinger, M.L.; Thomas, D.M.; Yanes, T.; Young, M.A. Influence of lived experience on risk perception among women who received a breast cancer polygenic risk score: ‘Another piece of the pie’. J. Genet. Couns. 2021, 30, 849–860. [Google Scholar] [CrossRef] [PubMed]
- Yanes, T.; Meiser, B.; Kaur, R.; Young, M.A.; Mitchell, P.B.; Scheepers-Joynt, M.; McInerny, S.; Taylor, S.; Barlow-Stewart, K.; Antill, Y.; et al. Breast cancer polygenic risk scores: A 12-month prospective study of patient reported outcomes and risk management behavior. Genet. Med. 2021, 23, 2316–2323. [Google Scholar] [CrossRef]
- Hurson, A.N.; Choudhury, P.P.; Gao, C.; Hüsing, A.; Eriksson, M.; Shi, M.; Jones, M.E.; Evans, D.G.R.; Milne, R.L.; Gaudet, M.M.; et al. Prospective evaluation of a breast-cancer risk model integrating classical risk factors and polygenic risk in 15 cohorts from six countries. Int. J. Epidemiol. 2022, 50, 1897–1911. [Google Scholar] [CrossRef] [PubMed]
- Evans, D.G.R.; Harkness, E.F.; Brentnall, A.R.; van Veen, E.M.; Astley, S.M.; Byers, H.; Sampson, S.; Southworth, J.; Stavrinos, P.; Howell, S.J.; et al. Breast cancer pathology and stage are better predicted by risk stratification models that include mammographic density and common genetic variants. Breast Cancer Res. Treat. 2019, 176, 141–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, D.G.; Astley, S.; Stavrinos, P.; Harkness, E.; Donnelly, L.S.; Dawe, S.; Jacob, I.; Harvie, M.; Cuzick, J.; Brentnall, A. Improvement in Risk Prediction, Early detection and Prevention of Breast Cancer in the NHS Breast Screening Programme and Family History Clinics: A Dual Cohort Study; NIHR Journals Library: Southampton, UK, 2016. [Google Scholar]
- NHS England. Primary Care. 2022. Available online: https://www.england.nhs.uk/five-year-forward-view/next-steps-on-the-nhs-five-year-forward-view/primary-care/ (accessed on 30 September 2022).
- Clift, A.K.; Dodwell, D.; Lord, S.; Petrou, S.; Brady, S.M.; Collins, G.S.; Hippisley-Cox, J. The current status of risk-stratified breast screening. Br. J. Cancer 2022, 126, 533–550. [Google Scholar] [CrossRef] [PubMed]
- Zeinomar, N.; Chung, W.K. Cases in Precision Medicine: The Role of Polygenic Risk Scores in Breast Cancer Risk Assessment. Ann. Intern. Med. 2021, 174, 408–412. [Google Scholar] [CrossRef]
- Evans, D.G.; van Veen, E.M.; Byers, H.; Roberts, E.; Howell, A.; Howell, S.J.; Harkness, E.F.; Brentnall, A.; Cuzick, J.; Newman, W.G. The importance of ethnicity: Are breast cancer polygenic risk scores ready for women who are not of White European origin? Int. J. Cancer 2022, 150, 73–79. [Google Scholar] [CrossRef]
- Lakeman, I.M.M.; van den Broek, A.J.; Vos, J.A.M.; Barnes, D.R.; Adlard, J.; Andrulis, I.L.; Arason, A.; Arnold, N.; Arun, B.K.; Balmaña, J.; et al. The predictive ability of the 313 variant-based polygenic risk score for contralateral breast cancer risk prediction in women of European ancestry with a heterozygous BRCA1 or BRCA2 pathogenic variant. Genet. Med. 2021, 23, 1726–1737. [Google Scholar] [CrossRef]
- Liu, C.; Zeinomar, N.; Chung, W.K.; Kiryluk, K.; Gharavi, A.G.; Hripcsak, G.; Crew, K.D.; Shang, N.; Khan, A.; Fasel, D.; et al. Generalizability of Polygenic Risk Scores for Breast Cancer Among Women With European, African, and Latinx Ancestry. JAMA Netw. Open 2021, 4, e2119084. [Google Scholar] [CrossRef]
- Ho, W.K.; Tan, M.M.; Mavaddat, N.; Tai, M.C.; Mariapun, S.; Li, J.; Ho, P.J.; Dennis, J.; Tyrer, J.P.; Bolla, M.K.; et al. European polygenic risk score for prediction of breast cancer shows similar performance in Asian women. Nat. Commun. 2020, 11, 3833. [Google Scholar] [CrossRef] [PubMed]
- Palmer, J.R. Polygenic Risk Scores for Breast Cancer Risk Prediction: Lessons Learned and Future Opportunities. J. Natl. Cancer Inst. 2020, 112, 555–556. [Google Scholar] [CrossRef] [PubMed]
- Du, Z.; Gao, G.; Adedokun, B.; Ahearn, T.; Lunetta, K.L.; Zirpoli, G.; Troester, M.A.; Ruiz-Narváez, E.A.; Haddad, S.A.; PalChoudhury, P.; et al. Evaluating Polygenic Risk Scores for Breast Cancer in Women of African Ancestry. J. Natl. Cancer Inst. 2021, 113, 1168–1176. [Google Scholar] [CrossRef] [PubMed]
- Department of Health and Social Care UK. Genome UK: The future of healthcare. 2020. Available online: https://www.gov.uk/government/publications/genome-uk-the-future-of-healthcare (accessed on 30 September 2022).
- Confluence Project for Breast Cancer Genetics—NCI. 2020. Available online: https://dceg.cancer.gov/research/cancer-types/breast-cancer/confluence-study-project.pdf (accessed on 30 September 2022).
- Manolio, T.A. Using the Data We Have: Improving Diversity in Genomic Research. Am. J. Hum. Genet 2019, 105, 233–236. [Google Scholar] [CrossRef]
- Jack, R.H.; Møller, H.; Robson, T.; Davies, E.A. Breast cancer screening uptake among women from different ethnic groups in London: A population-based cohort study. BMJ Open 2014, 4, e005586. [Google Scholar] [CrossRef] [Green Version]
- Cancer Research UK. Risk Factors for Breast Cancer. 2022. Available online: https://www.cancerresearchuk.org/about-cancer/breast-cancer/risks-causes/risk-factors (accessed on 30 September 2022).
- Yılmazel, G. Health Literacy, Mammogram Awareness and Screening Among Tertiary Hospital Women Patients. J. Cancer Educ. 2018, 33, 89–94. [Google Scholar] [CrossRef]
- Health Education England. Welcome to Genomics Education Programme—Genomics Education Programme. 2022. Available online: https://www.genomicseducation.hee.nhs.uk/ (accessed on 30 September 2022).
- Carver, T.; Hartley, S.; Lee, A.; Cunningham, A.P.; Archer, S.; de Villiers, C.B.; Roberts, J.; Ruston, R.; Walter, F.M.; Tischkowitz, M.; et al. CanRisk Tool-A Web Interface for the Prediction of Breast and Ovarian Cancer Risk and the Likelihood of Carrying Genetic Pathogenic Variants. Cancer Epidemiol. Biomark. Prev. 2021, 30, 469–473. [Google Scholar] [CrossRef]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ayoub, A.; Lapointe, J.; Nabi, H.; Pashayan, N. Risk-Stratified Breast Cancer Screening Incorporating a Polygenic Risk Score: A Survey of UK General Practitioners’ Knowledge and Attitudes. Genes 2023, 14, 732. https://doi.org/10.3390/genes14030732
Ayoub A, Lapointe J, Nabi H, Pashayan N. Risk-Stratified Breast Cancer Screening Incorporating a Polygenic Risk Score: A Survey of UK General Practitioners’ Knowledge and Attitudes. Genes. 2023; 14(3):732. https://doi.org/10.3390/genes14030732
Chicago/Turabian StyleAyoub, Aya, Julie Lapointe, Hermann Nabi, and Nora Pashayan. 2023. "Risk-Stratified Breast Cancer Screening Incorporating a Polygenic Risk Score: A Survey of UK General Practitioners’ Knowledge and Attitudes" Genes 14, no. 3: 732. https://doi.org/10.3390/genes14030732