
Serum MicroRNAs as Predictors for HCV Progression and Response to Treatment in Pakistani Patients

 , , ,
, , ,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data and Sample Collection
2.2. Parameter Analysis
- All of the chemical parameters related to the liver were done using a kit method based on spectrophotometry.
- A commercial ELISA kit determined α fetoproteins.
- RT PCR determined HCV RNA (viral load).
2.3. Expression Analysis
2.4. cDNA Synthesis by Reverse Transcriptase
2.5. PCR for Expression Analysis of Selected miRNA Genes (miRNA-182, miRNA-122, mi-RNA21, miRNA-199, miRNA-150, and miRNA-222)
2.6. Statistical Analysis
3. Results
3.1. Demographics Variables
3.2. Association Analysis
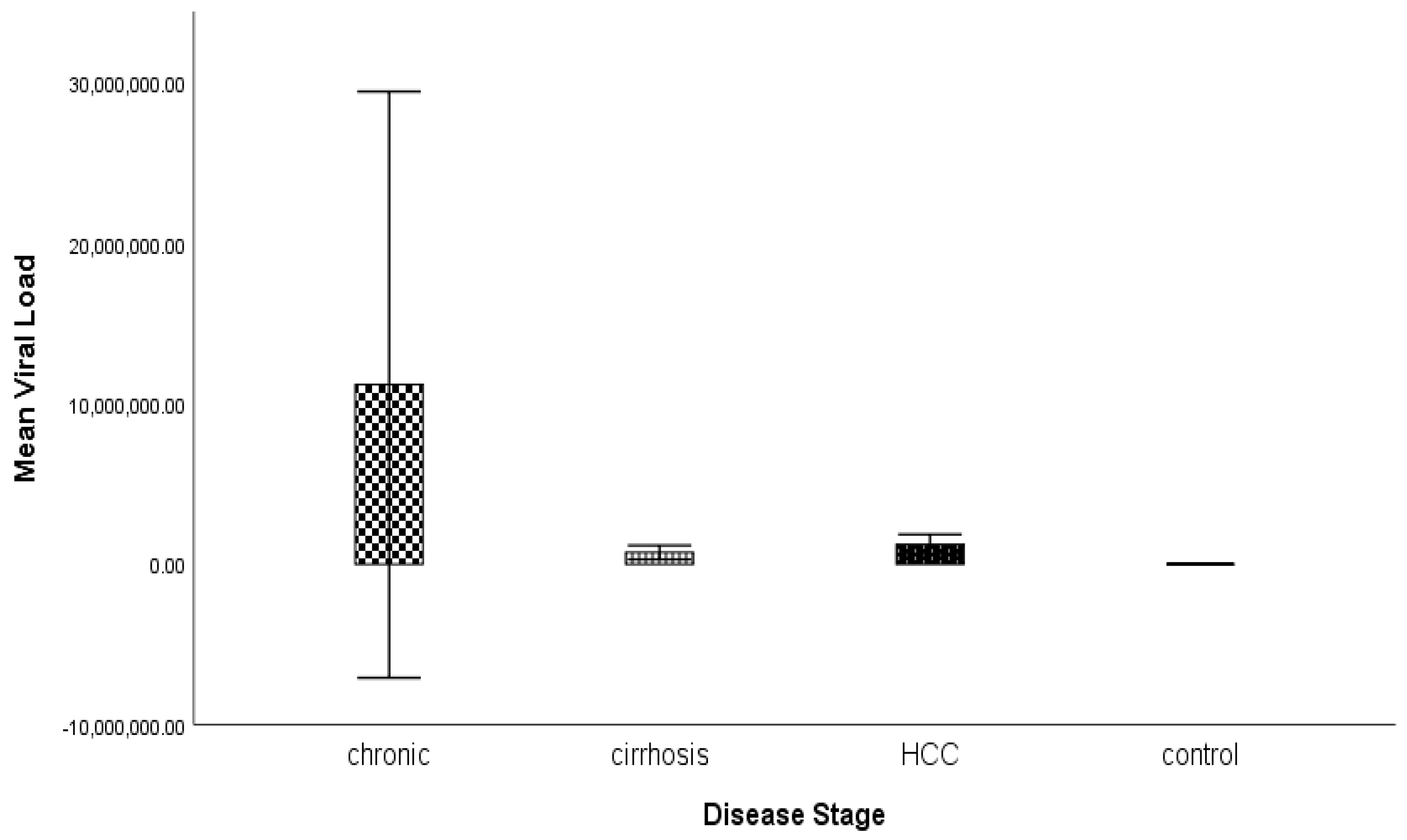
3.3. Analysis of Variance
3.4. Association Analysis
3.5. Expression Analysis of miRNAs in Diseased and Control Groups Using Real-Time PCR
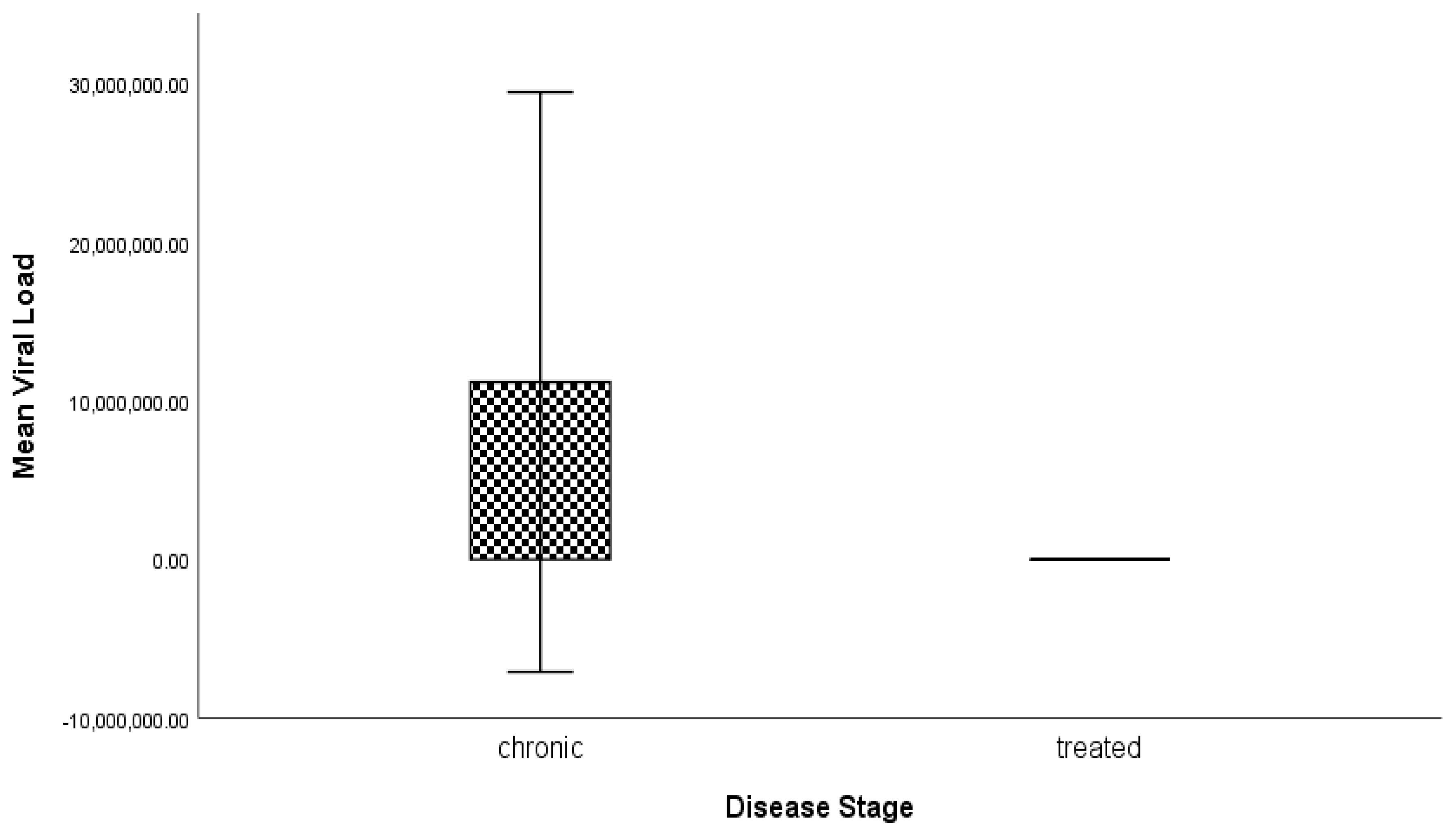
3.6. Expression Analysis of miRNA in Chronic Patient and Treated Groups Using Real-Time PCR
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chen, G.; Cheung, R.; Tom, J.W. Hepatitis: Sedation and anesthesia implications. Anesth. Prog. 2017, 64, 106–118. [Google Scholar] [CrossRef]
- Qu, C.; Zhang, S.; Li, Y.; Wang, Y.; Peppelenbosch, M.P.; Pan, Q. Mitochondria in the biology, pathogenesis, and treatment of hepatitis virus infections. Rev. Med. Virol. 2019, 29, e2075. [Google Scholar] [CrossRef]
- Dubuisson, J.; Cosset, F.L. Virology and cell biology of the hepatitis C virus life cycle–An update. J. Hepatol. 2014, 61, S3–S13. [Google Scholar] [CrossRef]
- Warkad, S.D.; Nimse, S.B.; Song, K.S.; Kim, T. HCV detection, discrimination, and genotyping technologies. Sensors 2018, 18, 3423. [Google Scholar] [CrossRef] [PubMed]
- Page, K.; Hahn, J.A.; Evans, J.; Shiboski, S.; Lum, P.; Delwart, E. Acute hepatitis C virus infection in young adult injection drug users: A prospective study of incident infection, resolution, and reinfection. J. Infect. Dis. 2009, 200, 1216–1226. [Google Scholar] [CrossRef]
- El-Serag, H.B. Epidemiology of viral hepatitis and hepatocellular carcinoma. Gastroenterology 2012, 142, 1264–1273. [Google Scholar] [CrossRef] [PubMed]
- Rabaan, A.A.; Al-Ahmed, S.H.; Bazzi, A.M.; Alfouzan, W.A.; Alsuliman, S.A.; Aldrazi, F.A.; Haque, S. Overview of hepatitis C infection, molecular biology, and new treatment. J. Infect. Public Health 2020, 13, 773–783. [Google Scholar] [CrossRef] [PubMed]
- Zafar, A.; Imran, M.; Zahoor, S.; Shah, Z.H.; Ali, M.; Afzal, M.S. Prevalence and treatment of untypable HCV variants in different districts of Punjab, Pakistan. Viral Immunol. 2018, 31, 426–432. [Google Scholar] [CrossRef]
- Arshad, A.; Ashfaq, U.A. Epidemiology of hepatitis C infection in Pakistan: Current estimate and major risk factors. Crit. Rev. Eukaryot. Gene Expr. 2017, 27, 63–77. [Google Scholar] [CrossRef]
- Hayes, C.N.; Imamura, M.; Tanaka, J.; Chayama, K. Road to elimination of HCV: Clinical challenges in HCV management. Liver Int. 2022, 42, 1935–1944. [Google Scholar] [CrossRef]
- Grebely, J.; Applegate, T.L.; Cunningham, P.; Feld, J.J. Hepatitis C point-of-care diagnostics: In search of a single visit diagnosis. Expert Rev. Mol. Diagn. 2017, 17, 1109–1115. [Google Scholar] [CrossRef] [PubMed]
- Hayes, C.N.; Chayama, K. MicroRNAs as biomarkers for liver disease and hepatocellular carcinoma. Int. J. Mol. Sci. 2016, 17, 280. [Google Scholar] [CrossRef] [PubMed]
- He, S.; Hu, X.W.; Wang, D.; Han, L.F.; Zhang, D.C.; Wei, C. Accuracy of microRNAs for the diagnosis of hepatocellular carcinoma: A systematic review and meta-analysis. Clin. Res. Hepatol. Gastroenterol. 2016, 40, 405–417. [Google Scholar] [CrossRef]
- Aronson, J.K.; Ferner, R.E. Biomarkers—A general review. Curr. Protoc. Pharmacol. 2017, 76, 9–23. [Google Scholar] [CrossRef]
- Wang, X.; He, Y.; Mackowiak, B.; Gao, B. MicroRNAs as regulators, biomarkers and therapeutic targets in liver diseases. Gut 2021, 70, 784–795. [Google Scholar] [CrossRef]
- Yu, M.L.; Chen, P.J.; Dai, C.Y.; Hu, T.H.; Huang, C.F.; Huang, Y.H.; Chuang, W.L. 2020 Taiwan consensus statement on the management of hepatitis C: Part (II) special populations. J. Formos. Med. Assoc. 2020, 119, 1135–1157. [Google Scholar] [CrossRef] [PubMed]
- Neamatallah, M.A.; El-Missiry, M.A.; Said, M.M.; Elbendary, M.; Othman, A.I.; Ammar, O.A. TP53 polymorphism as a risk factor for hepatocellular carcinoma in hepatitis C virus-infected Egyptian patients. Egypt. J. Basic Appl. Sci. 2014, 1, 9–15. [Google Scholar] [CrossRef]
- Sheth, S.G.; Flamm, S.L.; Gordon, F.D.; Chopra, S. AST/ALT ratio predicts cirrhosis in patients with chronic hepatitis C virus infection. Am. J. Gastroenterol. 1998, 93, 44–48. [Google Scholar] [CrossRef]
- Carr, B.I.; Guerra, V.; Giannini, E.G.; Farinati, F.; Ciccarese, F.; Rapaccini, G.L.; Italian Liver Cancer (ITA. LI. CA) Group. Association of abnormal plasma bilirubin with aggressive hepatocellular carcinoma phenotype. Semin. Oncol. 2014, 41, 252–258. [Google Scholar] [CrossRef] [PubMed]
- Saini, N.; Bhagat, A.; Sharma, S.; Duseja, A.; Chawla, Y. Evaluation of clinical and biochemical parameters in hepatocellular carcinoma: Experience from an Indian center. Clin. Chim. Acta. 2006, 371, 183–186. [Google Scholar] [CrossRef]
- Acharya, S.K. Epidemiology of hepatocellular carcinoma in India. J. Clin. Exp. Hepatol. 2014, 4, S27–S33. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Chen, M.; Huang, H.; Yuan, T.; Zhang, M.; Zhang, K.; Deng, S. Circulating microRNA-122a as a diagnostic marker for hepatocellular carcinoma. Onco Targets Ther. 2013, 6, 577. [Google Scholar]
- Shrivastava, S.; Steele, R.; Ray, R.; Ray, R.B. MicroRNAs: Role in hepatitis C virus pathogenesis. Genes Dis. 2015, 2, 35–45. [Google Scholar] [CrossRef]
- Li, J.; Jin, B.; Wang, T.; Li, W.; Wang, Z.; Zhang, H.; Li, N. Serum microRNA expression profiling identifies serum biomarkers for HCV-related hepatocellular carcinoma. Cancer Biomark 2019, 26, 501–512. [Google Scholar] [CrossRef]
- Shaheen, N.M.H.; Zayed, N.; Riad, N.M.; Tamim, H.H.; Shahin, R.M.H.; Labib, D.A.; Yosry, A. Role of circulating miR-182 and miR-150 as biomarkers for cirrhosis and hepatocellular carcinoma post HCV infection in Egyptian patients. Virus Res. 2018, 255, 77–84. [Google Scholar] [CrossRef]
- Khairy, R.M.; Hmmad, S.S.; Sayed, M.; Ahmed, H.A.; Esmail, M.A.M. Serum MicroRNAs as predictors for fibrosis progression and response to direct-acting antivirals treatment in hepatitis C virus genotype-4 Egyptian patients. Int. J. Clin. Pract. Suppl. 2021, 75, e13954. [Google Scholar] [CrossRef] [PubMed]
- Nasser, M.Z.; Zayed, N.A.; Mohamed, A.M.; Attia, D.; Esmat, G.; Khairy, A. Circulating microRNAs (miR-21, miR-223, miR-885-5p) along the clinical spectrum of HCV-related chronic liver disease in Egyptian patients. Arab. J. Gastroenterol. 2019, 20, 198–204. [Google Scholar] [CrossRef] [PubMed]
- Bihrer, V.; Waidmann, O.; Friedrich-Rust, M.; Forestier, N.; Susser, S.; Haupenthal, J.; Piiper, A. Serum microRNA-21 as marker for necroinflammation in hepatitis C patients with and without hepatocellular carcinoma. PLoS ONE 2011, 6, e26971. [Google Scholar] [CrossRef]
- El-Abd, N.E.; Fawzy, N.A.; El-Sheikh, S.M.; Soliman, M.E. Circulating miRNA-122, miRNA-199a, and miRNA-16 as biomarkers for early detection of hepatocellular carcinoma in Egyptian patients with chronic hepatitis C virus infection. Mol. Diagn Ther. 2015, 19, 213–220. [Google Scholar] [CrossRef] [PubMed]
- El-Guendy, N.M.; Helwa, R.; El-Halawany, M.S.; Ali, S.A.R.; Aly, M.T.; Alieldin, N.H.; Abdel-Wahab, A.H.A. The liver MicroRNA expression profiles associated with chronic hepatitis C virus (HCV) genotype-4 infection: A preliminary study. Hepat. Mon. 2016, 16, e33881. [Google Scholar] [CrossRef]
- Dubin, P.H.; Yuan, H.; Devine, R.K.; Hynan, L.S.; Jain, M.K.; Lee, W.M.; Acute Liver Failure Study Group. Micro-RNA-122 levels in acute liver failure and chronic hepatitis C. J. Med. Virol. 2014, 86, 1507–1514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Markovic, J.; Sharma, A.D.; Balakrishnan, A. MicroRNA-221: A fine tuner and potential biomarker of chronic liver injury. Cells 2020, 9, 1767. [Google Scholar] [CrossRef] [PubMed]
- Bala, S.; Tilahun, Y.; Taha, O.; Alao, H.; Kodys, K.; Catalano, D.; Szabo, G. Increased microRNA-155 expression in the serum and peripheral monocytes in chronic HCV infection. J. Transl. Med. 2012, 10, 151. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Primer Name | Primer Sequence |
|---|---|
| miRNA-182-F | 5′-TGCGGTTTGGCAATGGTAGAAC-3’ |
| miRNA-182-R | 5’-CCAGTGCAGGGTCCGAGGT-3’ |
| miRNA-122–F | 5′-ACACTCCAGCTGGGTGGAGTGTGACAATCC-3′ |
| miRNA-122R | 5′-TGGTGTCGTGGAGTCG-3′ |
| miRNA-21-F | 5′-GCCCGCTAGCTTATCAGACTGATG-3′ |
| miRNA-21-R | 5′-CAGTGCAGGGTCC GAGGT-3 |
| miRNA-199–F | 5′-GCGGCGGACAGTAGTCTGCAC-3′ |
| miRNA-199–R | 5′-ATCCAGTGCAGGGTCCGAGG-3′ |
| miRNA-150-F | 5′TCTCCCAACCCTTGTACCAGTG3′ |
| miRNA-150-R | 5′CAGTGCGTCGTGGAGT3′ |
| miRNA-222-F | 5′-GTTCGTGGGAGCTACATTGTCTGC-3′ |
| miRNA-222-R | 5′-GTGTCGTGGAGTCGGCAATTC-3′ |
| U6 snRNA-F | CTCGCTTCGGCAGCACATATAC |
| U6 snRNA-R | ACGCTTCACGAATTTGCGTGTC |
| Variables | Chronic (n = 40) | Cirrhosis (n = 40) | HCC (n = 40) | Treated (n = 40) | Control (n = 40) | p Value | |
|---|---|---|---|---|---|---|---|
| Gender | Male | 20 (50%) | 20 (50%) | 30 (75%) | 18 (45%) | 20 (50%) | 0.057 |
| Female | 20 (50%) | 20 (50%) | 10 (25%) | 22 (55%) | 20 (50%) | ||
| Age | 21–40 | 22 (55%) | 8 (20%) | 1 (2.5%) | 10 (25%) | 30 (75%) | 0.001 |
| 41–60 | 15 (37.5%) | 29 (72.5%) | 29 (72.5%) | 26 (65%) | 6 (15%) | ||
| 61–80 | 3 (7.5%) | 3 (7.5%) | 10 (25%) | 4 (10%) | 4 (10%) | ||
| Male (n = 108) | Female (n = 92) | p Value | |
|---|---|---|---|
| Variables | M ± SD | M ± SD | |
| Age | 48.96 ± 11.96 | 44.48 ± 10.65 | 0.006 |
| ALT | 35.18 ± 17.50 | 32.48 ± 11.08 | 0.20 |
| AST | 34.43 ± 15.69 | 31.34 ± 10.74 | 0.11 |
| ALP | 175.05 ± 105.46 | 157.52 ± 57.62 | 0.16 |
| Viral Load | 3,952,923.66 ± 34,763,237.74 | 1,081,468.79 ± 4,053,847.94 | 0.43 |
| Bilirubin | 1.01 ± 0.60 | 0.88 ± 0.55 | 0.11 |
| Variables | Chronic (n = 40) | Cirrhosis (n = 40) | HCC (n = 40) | Control (n = 40) | p Values |
|---|---|---|---|---|---|
| Age | 41.35 ± 11.55 | 49.08 ± 9.11 | 56.85 ± 6.62 | 38.50 ± 10.86 | 0.000 |
| ALT | 35.38 ± 15.70 | 35.13 ± 12.38 | 43.08 ± 20.42 | 29.05 ± 3.81 | 0.000 |
| AST | 33.13 ± 12.50 | 32.90 ± 12.74 | 41.65 ± 21.83 | 27.88 ± 3.04 | 0.000 |
| ALP | 179.53 ± 45.38 | 163.70 ± 68.85 | 210.85 ± 137.64 | 91.65 ± 19.83 | 0.000 |
| Viral Load | 11,191,265.55 ± 57,129,256.41 | 735,073.68 ± 1,357,141.14 | 1,233,932.88 ± 1,946,918 | 0.00 ± 0.00 | 0.25 |
| Bilirubin | 0.77 ± 0.26 | 0.94 ± 0.48 | 1.65 ± 0.75 | 0.64 ± 0.20 | 0.000 |
| AFP | 808.15 ± 1381.09 | NA |
| Chronic (n = 40) | Treated (n = 40) | p Value | |
|---|---|---|---|
| Variables | M ± SD | M ± SD | |
| Age | 41.35 ± 11.55 | 48.73 ± 9.52 | 0.003 ** |
| ALT | 35.38 ± 15.70 | 31.63 ± 4.67 | 0.15 |
| AST | 33.13 ± 12.50 | 29.50 ± 5.98 | 0.10 |
| ALP | 184.48 ± 35.17 | 189.20 ± 63.56 | 0.68 |
| Viral Load | 11,191,265.55 ± 57,129,256.41 | 0.00 ± 0.00 | 0.22 |
| Bilirubin | 0.77 ± 0.26 | 0.77 ± 0.39 | 0.95 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Manzoor, S.; Malik, I.R.; Jahan, S.; Sarwar, M.B.; Bashir, A.; Shams, S.; Hussain, A. Serum MicroRNAs as Predictors for HCV Progression and Response to Treatment in Pakistani Patients. Genes 2023, 14, 441. https://doi.org/10.3390/genes14020441
Manzoor S, Malik IR, Jahan S, Sarwar MB, Bashir A, Shams S, Hussain A. Serum MicroRNAs as Predictors for HCV Progression and Response to Treatment in Pakistani Patients. Genes. 2023; 14(2):441. https://doi.org/10.3390/genes14020441
Chicago/Turabian StyleManzoor, Sadia, Imran Riaz Malik, Shah Jahan, Muhammad Bilal Sarwar, Asma Bashir, Sulaiman Shams, and Abrar Hussain. 2023. "Serum MicroRNAs as Predictors for HCV Progression and Response to Treatment in Pakistani Patients" Genes 14, no. 2: 441. https://doi.org/10.3390/genes14020441