
Integrating Rehabilomics into the Multi-Omics Approach in the Management of Multiple Sclerosis: The Way for Precision Medicine?

{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
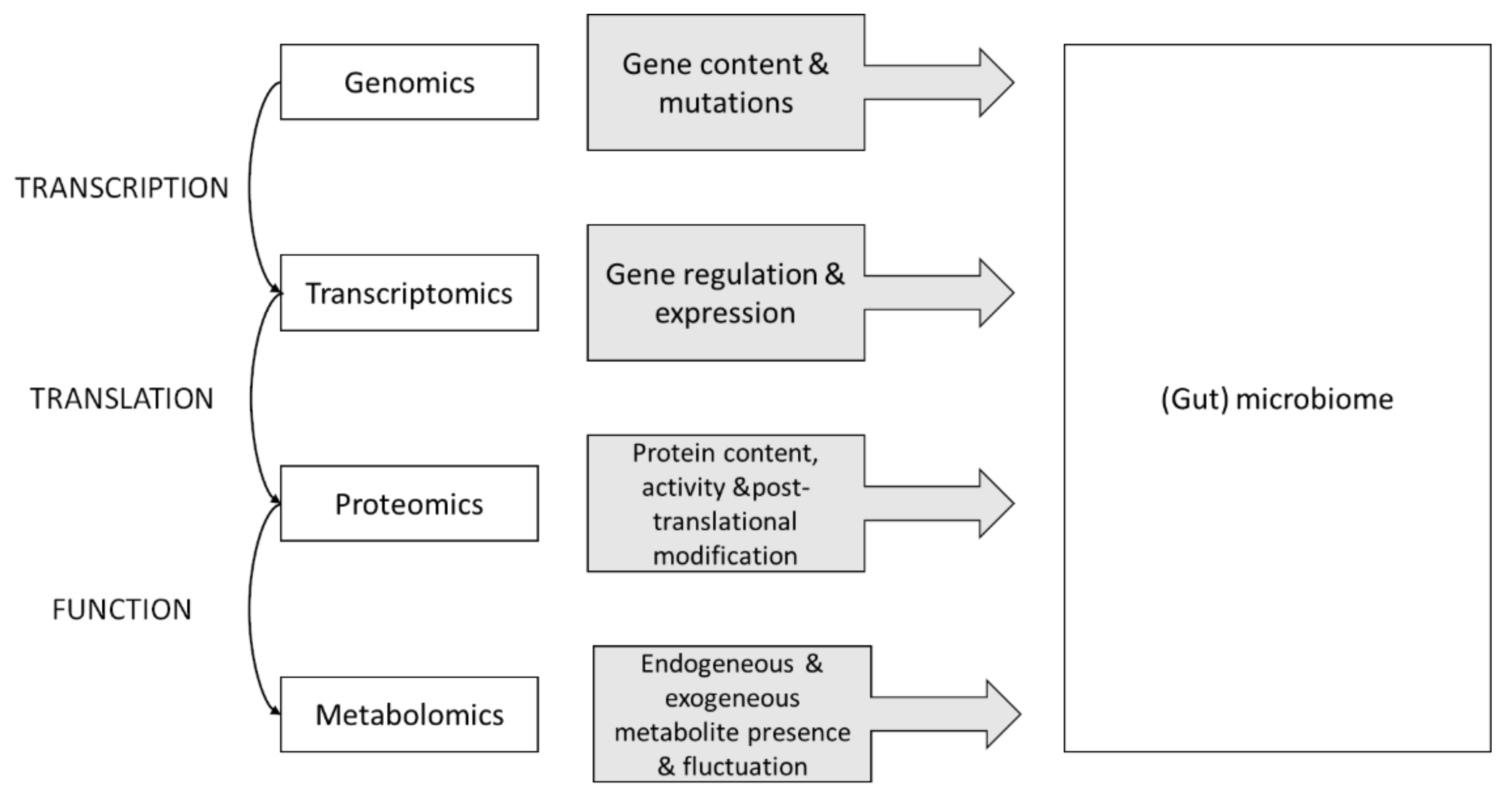
2. The Multi-Omics Approach

3. (Conventional) Rehabilitation
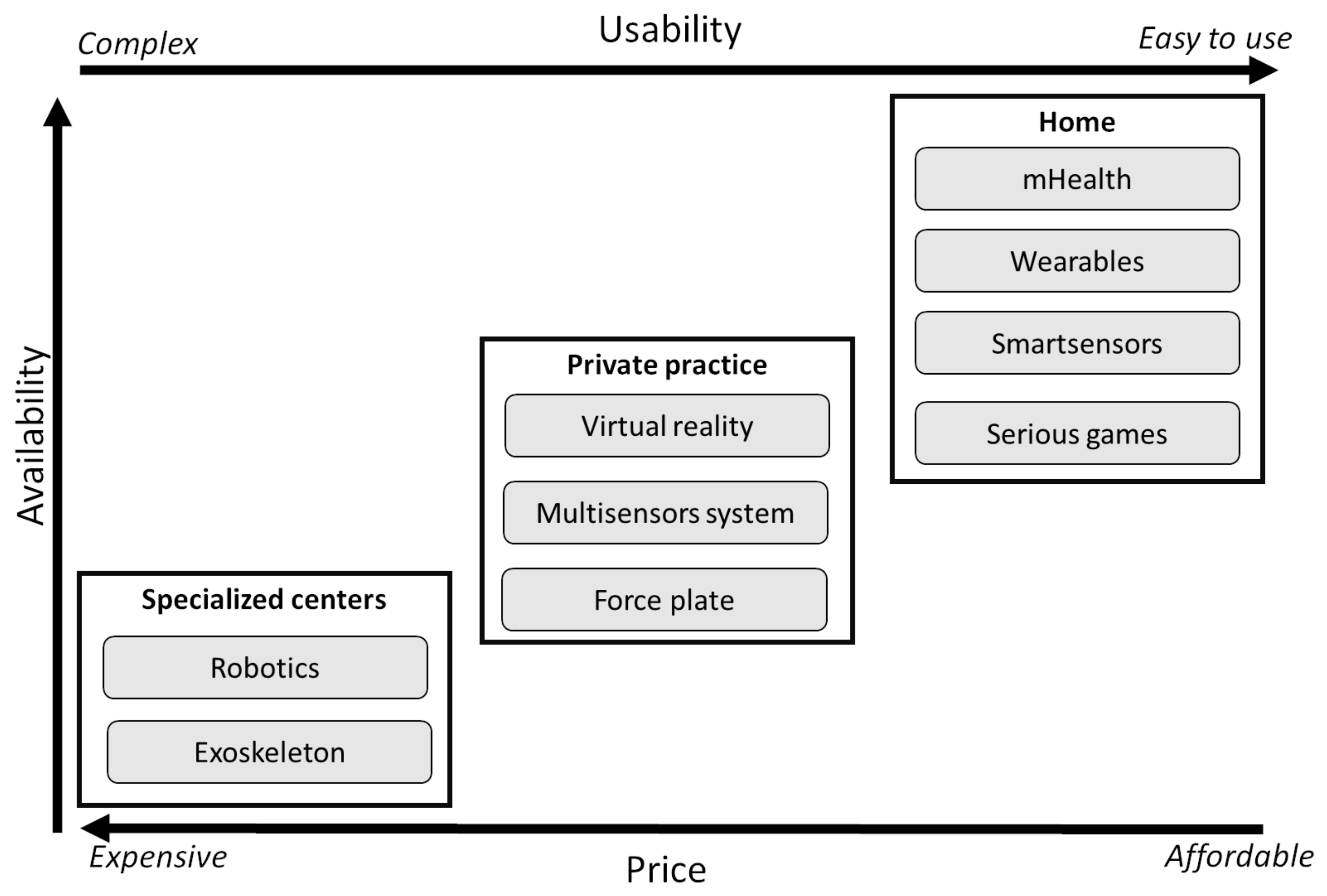
4. Technology-Supported Rehabilitation
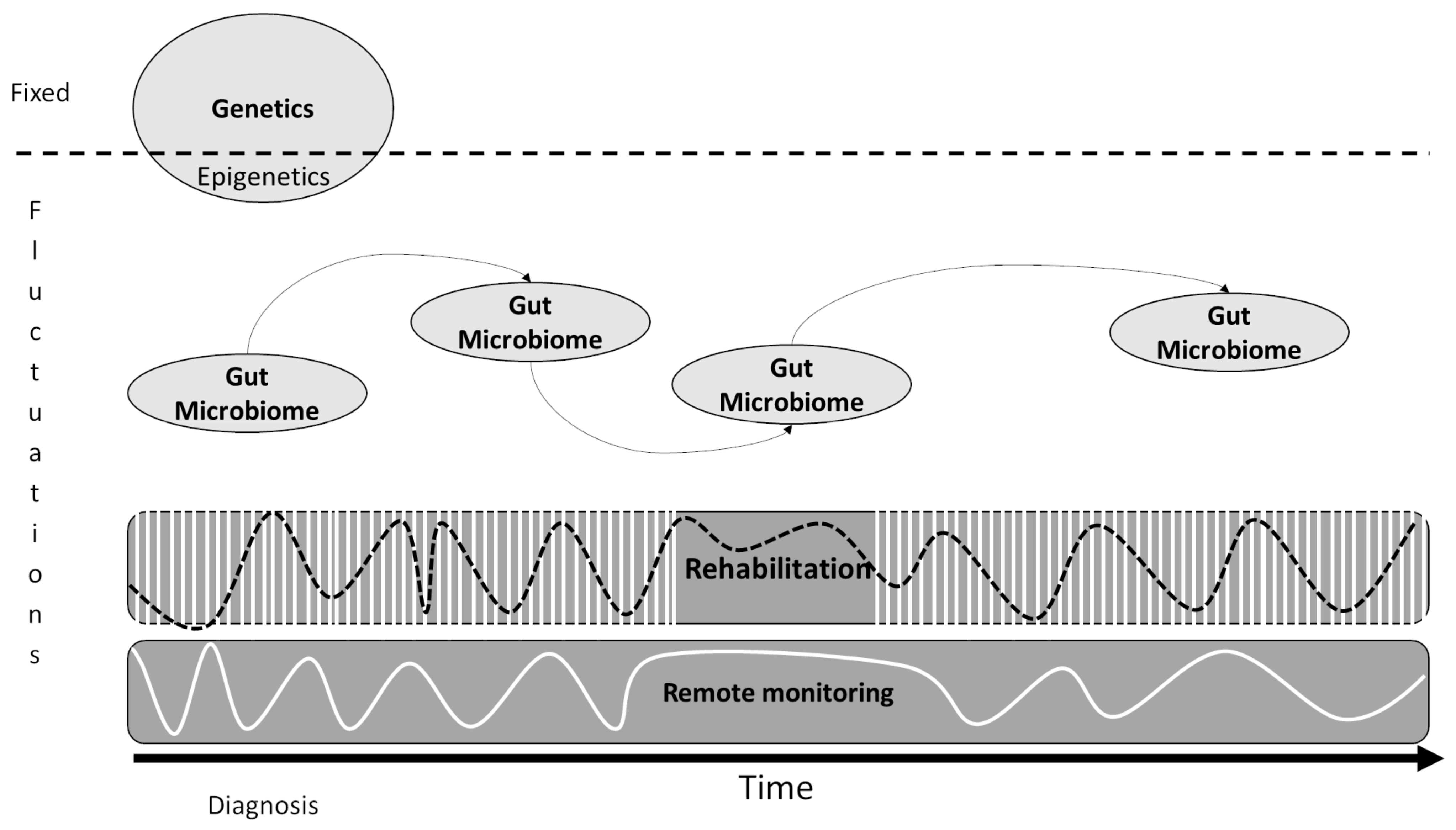
5. Toward a (More) Integrated Approach: The Precision Medicine

6. Current Challenges and Call for Actions
7. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L.; et al. Diagnostic Criteria for Multiple Sclerosis: 2010 Revisions to the McDonald Criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Razazian, N.; Kazeminia, M.; Moayedi, H.; Daneshkhah, A.; Shohaimi, S.; Mohammadi, M.; Jalali, R.; Salari, N. The Impact of Physical Exercise on the Fatigue Symptoms in Patients with Multiple Sclerosis: A Systematic Review and Meta-Analysis. BMC Neurol. 2020, 20, 93. [Google Scholar] [CrossRef] [PubMed]
- Boeschoten, R.E.; Braamse, A.M.J.; Beekman, A.T.F.; Cuijpers, P.; van Oppen, P.; Dekker, J.; Uitdehaag, B.M.J. Prevalence of Depression and Anxiety in Multiple Sclerosis: A Systematic Review and Meta-Analysis. J. Neurol. Sci. 2017, 372, 331–341. [Google Scholar] [CrossRef] [PubMed]
- Kalb, R.; Beier, M.; Benedict, R.H.; Charvet, L.; Costello, K.; Feinstein, A.; Gingold, J.; Goverover, Y.; Halper, J.; Harris, C.; et al. Recommendations for Cognitive Screening and Management in Multiple Sclerosis Care. Mult. Scler. Houndmills Basingstoke Engl. 2018, 24, 1665–1680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McGinley, M.P.; Goldschmidt, C.H.; Rae-Grant, A.D. Diagnosis and Treatment of Multiple Sclerosis: A Review. JAMA 2021, 325, 765–779. [Google Scholar] [CrossRef]
- Negaresh, R.; Motl, R.W.; Zimmer, P.; Mokhtarzade, M.; Baker, J.S. Effects of Exercise Training on Multiple Sclerosis Biomarkers of Central Nervous System and Disease Status: A Systematic Review of Intervention Studies. Eur. J. Neurol. 2019, 26, 711–721. [Google Scholar] [CrossRef]
- Negaresh, R.; Motl, R.W.; Mokhtarzade, M.; Dalgas, U.; Patel, D.; Shamsi, M.M.; Majdinasab, N.; Ranjbar, R.; Zimmer, P.; Baker, J.S. Effects of Exercise Training on Cytokines and Adipokines in Multiple Sclerosis: A Systematic Review. Mult. Scler. Relat. Disord. 2018, 24, 91–100. [Google Scholar] [CrossRef] [Green Version]
- Rintala, A.; Hakala, S.; Paltamaa, J.; Heinonen, A.; Karvanen, J.; Sjögren, T. Effectiveness of Technology-Based Distance Physical Rehabilitation Interventions on Physical Activity and Walking in Multiple Sclerosis: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Disabil. Rehabil. 2018, 40, 373–387. [Google Scholar] [CrossRef] [Green Version]
- Conesa, A.; Beck, S. Making Multi-Omics Data Accessible to Researchers. Sci. Data 2019, 6, 251. [Google Scholar] [CrossRef] [Green Version]
- Krassowski, M.; Das, V.; Sahu, S.K.; Misra, B.B. State of the Field in Multi-Omics Research: From Computational Needs to Data Mining and Sharing. Front. Genet. 2020, 11. [Google Scholar] [CrossRef]
- Kubsik-Gidlewska, A.M.; Klimkiewicz, P.; Klimkiewicz, R.; Janczewska, K.; Woldańska-Okońska, M. Rehabilitation in Multiple Sclerosis. Adv. Clin. Exp. Med. Off. Organ Wroc. Med. Univ. 2017, 26, 709–715. [Google Scholar] [CrossRef]
- Subramanian, I.; Verma, S.; Kumar, S.; Jere, A.; Anamika, K. Multi-Omics Data Integration, Interpretation, and Its Application. Bioinforma. Biol. Insights 2020, 14, 1177932219899051. [Google Scholar] [CrossRef] [Green Version]
- Voigt, I.; Inojosa, H.; Dillenseger, A.; Haase, R.; Akgün, K.; Ziemssen, T. Digital Twins for Multiple Sclerosis. Front. Immunol. 2021, 12, 669811. [Google Scholar] [CrossRef]
- Jansson, J.; Baker, E. A Multi-Omic Future for Microbiome Studies. Nat. Microbiol. 2016, 1, 1–3. [Google Scholar] [CrossRef]
- McCombie, W.R.; McPherson, J.D.; Mardis, E.R. Next-Generation Sequencing Technologies. Cold Spring Harb. Perspect. Med. 2019, 9, a036798. [Google Scholar] [CrossRef]
- Hedlund, E.; Deng, Q. Single-Cell RNA Sequencing: Technical Advancements and Biological Applications. Mol. Asp. Med. 2018, 59, 36–46. [Google Scholar] [CrossRef]
- Li, Y. Modern Epigenetics Methods in Biological Research. Methods San Diego Calif 2021, 187, 104–113. [Google Scholar] [CrossRef]
- Rozanova, S.; Barkovits, K.; Nikolov, M.; Schmidt, C.; Urlaub, H.; Marcus, K. Quantitative Mass Spectrometry-Based Proteomics: An Overview. Methods Mol. Biol. Clifton NJ 2021, 2228, 85–116. [Google Scholar] [CrossRef]
- Bauermeister, A.; Mannochio-Russo, H.; Costa-Lotufo, L.V.; Jarmusch, A.K.; Dorrestein, P.C. Mass Spectrometry-Based Metabolomics in Microbiome Investigations. Nat. Rev. Microbiol. 2022, 20, 143–160. [Google Scholar] [CrossRef]
- International Multiple Sclerosis Genetics Consortium; Patsopoulos, N.A.; Baranzini, S.E.; Santaniello, A.; Shoostari, P.; Cotsapas, C.; Wong, G.; Beecham, A.H.; James, T.; Replogle, J.; et al. Multiple Sclerosis Genomic Map Implicates Peripheral Immune Cells and Microglia in Susceptibility. Science 2019, 365, eaav7188. [Google Scholar] [CrossRef]
- Ascherio, A. Environmental Factors in Multiple Sclerosis. Expert Rev. Neurother. 2013, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Sasmita, A.O. Modification of the Gut Microbiome to Combat Neurodegeneration. Rev. Neurosci. 2019. [Google Scholar] [CrossRef] [PubMed]
- Westfall, S.; Lomis, N.; Kahouli, I.; Dia, S.Y.; Singh, S.P.; Prakash, S. Microbiome, Probiotics and Neurodegenerative Diseases: Deciphering the Gut Brain Axis. Cell. Mol. Life Sci. CMLS 2017, 74, 3769–3787. [Google Scholar] [CrossRef] [PubMed]
- Abdel-Haq, R.; Schlachetzki, J.C.M.; Glass, C.K.; Mazmanian, S.K. Microbiome–Microglia Connections via the Gut–Brain Axis. J. Exp. Med. 2019, 216, 41–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cryan, J.F.; O’Riordan, K.J.; Cowan, C.S.M.; Sandhu, K.V.; Bastiaanssen, T.F.S.; Boehme, M.; Codagnone, M.G.; Cussotto, S.; Fulling, C.; Golubeva, A.V.; et al. The Microbiota-Gut-Brain Axis. Physiol. Rev. 2019, 99, 1877–2013. [Google Scholar] [CrossRef]
- Socała, K.; Doboszewska, U.; Szopa, A.; Serefko, A.; Włodarczyk, M.; Zielińska, A.; Poleszak, E.; Fichna, J.; Wlaź, P. The Role of Microbiota-Gut-Brain Axis in Neuropsychiatric and Neurological Disorders. Pharmacol. Res. 2021, 172, 105840. [Google Scholar] [CrossRef]
- Wu, Q.; Wang, Q.; Mao, G.; Dowling, C.A.; Lundy, S.K.; Mao-Draayer, Y. Dimethyl Fumarate Selectively Reduces Memory T Cells and Shifts the Balance between Th1/Th17 and Th2 in Multiple Sclerosis Patients. J. Immunol. Baltim. Md 1950 2017, 198, 3069–3080. [Google Scholar] [CrossRef] [Green Version]
- Bonnechère, B.; Amin, N.; van Duijn, C. What Are the Key Gut Microbiota Involved in Neurological Diseases? A Systematic Review. Int. J. Mol. Sci. 2022, 23, 13665. [Google Scholar] [CrossRef]
- Xing, J.; Li, X.; Sun, Y.; Zhao, J.; Miao, S.; Xiong, Q.; Zhang, Y.; Zhang, G. Comparative Genomic and Functional Analysis of Akkermansia Muciniphila and Closely Related Species. Genes Genom. 2019, 41, 1253–1264. [Google Scholar] [CrossRef] [Green Version]
- Geerlings, S.Y.; Kostopoulos, I.; de Vos, W.M.; Belzer, C. Akkermansia Muciniphila in the Human Gastrointestinal Tract: When, Where, and How? Microorganisms 2018, 6, 75. [Google Scholar] [CrossRef]
- Bonnechère, B.; Amin, N.; van Duijn, C. The Role of Gut Microbiota in Neuropsychiatric Diseases—Creation of An Atlas-Based on Quantified Evidence. Front. Cell. Infect. Microbiol. 2022, 12, 831666. [Google Scholar] [CrossRef]
- Marrie, R.A.; Fisk, J.D.; Tremlett, H.; Wolfson, C.; Warren, S.; Tennakoon, A.; Leung, S.; Patten, S.B. CIHR Team in the Epidemiology and Impact of Comorbidity on Multiple Sclerosis Differences in the Burden of Psychiatric Comorbidity in MS vs the General Population. Neurology 2015, 85, 1972–1979. [Google Scholar] [CrossRef] [Green Version]
- Binzer, S.; Jiang, X.; Hillert, J.; Manouchehrinia, A. Depression and Multiple Sclerosis: A Bidirectional Mendelian Randomisation Study. Mult. Scler. J. 2021, 27, 1799–1802. [Google Scholar] [CrossRef]
- Hajjar, J.; Mendoza, T.; Zhang, L.; Fu, S.; Piha-Paul, S.A.; Hong, D.S.; Janku, F.; Karp, D.D.; Ballhausen, A.; Gong, J.; et al. Associations between the Gut Microbiome and Fatigue in Cancer Patients. Sci. Rep. 2021, 11, 5847. [Google Scholar] [CrossRef]
- Monda, V.; Villano, I.; Messina, A.; Valenzano, A.; Esposito, T.; Moscatelli, F.; Viggiano, A.; Cibelli, G.; Chieffi, S.; Monda, M.; et al. Exercise Modifies the Gut Microbiota with Positive Health Effects. Oxid. Med. Cell. Longev. 2017, 2017, 1–8. [Google Scholar] [CrossRef]
- Batacan, R.B.; Fenning, A.S.; Dalbo, V.J.; Scanlan, A.T.; Duncan, M.J.; Moore, R.J.; Stanley, D. A Gut Reaction: The Combined Influence of Exercise and Diet on Gastrointestinal Microbiota in Rats. J. Appl. Microbiol. 2017, 122, 1627–1638. [Google Scholar] [CrossRef]
- Mokhtarzade, M.; Agha-Alinejad, H.; Motl, R.W.; Negaresh, R.; Baker, J.S.; Zimmer, P. Weight Control and Physical Exercise in People with Multiple Sclerosis: Current Knowledge and Future Perspectives. Complement. Ther. Med. 2019, 43, 240–246. [Google Scholar] [CrossRef] [Green Version]
- Negaresh, R.; Motl, R.; Mokhtarzade, M.; Ranjbar, R.; Majdinasab, N.; Khodadoost, M.; Zimmer, P.; Baker, J.S.; Patel, D. Effect of Short-Term Interval Exercise Training on Fatigue, Depression, and Fitness in Normal Weight vs. Overweight Person with Multiple Sclerosis. Explore 2019, 15, 134–141. [Google Scholar] [CrossRef] [Green Version]
- Welly, R.J.; Liu, T.-W.; Zidon, T.M.; Rowles, J.L.; Park, Y.-M.; Smith, T.N.; Swanson, K.S.; Padilla, J.; Vieira-Potter, V.J. Comparison of Diet versus Exercise on Metabolic Function and Gut Microbiota in Obese Rats. Med. Sci. Sports Exerc. 2016, 48, 1688–1698. [Google Scholar] [CrossRef] [Green Version]
- Mills, J.-A.; Cieza, A.; Short, S.D.; Middleton, J.W. Development and Validation of the WHO Rehabilitation Competency Framework: A Mixed Methods Study. Arch. Phys. Med. Rehabil. 2021, 102, 1113–1123. [Google Scholar] [CrossRef]
- WHO. Fact Sheets: Rehabilitation; WHO: Geneva, Switzerland, 2020. [Google Scholar]
- Khan, F.; Amatya, B. Rehabilitation in Multiple Sclerosis: A Systematic Review of Systematic Reviews. Arch. Phys. Med. Rehabil. 2017, 98, 353–367. [Google Scholar] [CrossRef] [PubMed]
- Kidd, T.; Carey, N.; Mold, F.; Westwood, S.; Miklaucich, M.; Konstantara, E.; Sterr, A.; Cooke, D. A Systematic Review of the Effectiveness of Self-Management Interventions in People with Multiple Sclerosis at Improving Depression, Anxiety and Quality of Life. PLoS ONE 2017, 12, e0185931. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Inojosa, H.; Schriefer, D.; Ziemssen, T. Clinical Outcome Measures in Multiple Sclerosis: A Review. Autoimmun. Rev. 2020, 19, 102512. [Google Scholar] [CrossRef] [PubMed]
- Werner, C.; Schönhammer, J.G.; Steitz, M.K.; Lambercy, O.; Luft, A.R.; Demkó, L.; Easthope, C.A. Using Wearable Inertial Sensors to Estimate Clinical Scores of Upper Limb Movement Quality in Stroke. Front. Physiol. 2022, 13, 877563. [Google Scholar] [CrossRef] [PubMed]
- Song, X.; van de Ven, S.S.; Chen, S.; Kang, P.; Gao, Q.; Jia, J.; Shull, P.B. Proposal of a Wearable Multimodal Sensing-Based Serious Games Approach for Hand Movement Training After Stroke. Front. Physiol. 2022, 13, 811950. [Google Scholar] [CrossRef]
- Bonnechere, B.; Jansen, B.; Omelina, L.; Sholukha, V.; Van Sint Jan, S. Validation of the balance board for clinical evaluation of balance during serious gaming rehabilitation exercises. Telemed. e-Health 2016, 22, 709–717. [Google Scholar] [CrossRef]
- Gavrilović, M.M.; Janković, M.M. Temporal Synergies Detection in Gait Cyclograms Using Wearable Technology. Sensors 2022, 22, 2728. [Google Scholar] [CrossRef]
- Bonnechère, B.; Jansen, B.; Haack, I.; Omelina, L.; Feipel, V.; Van Sint Jan, S.; Pandolfo, M. Automated Functional Upper Limb Evaluation of Patients with Friedreich Ataxia Using Serious Games Rehabilitation Exercises. J. Neuroeng. Rehabil. 2018, 15, 87. [Google Scholar] [CrossRef]
- Bonnechère, B.; Klass, M.; Langley, C.; Sahakian, B.J. Brain Training Using Cognitive Apps Can Improve Cognitive Performance and Processing Speed in Older Adults. Sci. Rep. 2021, 11, 12313. [Google Scholar] [CrossRef]
- Biomarkers Definitions Working Group. Biomarkers and Surrogate Endpoints: Preferred Definitions and Conceptual Framework. Clin. Pharmacol. Ther. 2001, 69, 89–95. [Google Scholar] [CrossRef]
- Wagner, A.K. TBI Translational Rehabilitation Research in the 21st Century: Exploring a Rehabilomics Research Model. Eur. J. Phys. Rehabil. Med. 2010, 46, 549–556. [Google Scholar]
- Wagner, A.K. A Rehabilomics Framework for Personalized and Translational Rehabilitation Research and Care for Individuals with Disabilities: Perspectives and Considerations for Spinal Cord Injury. J. Spinal Cord Med. 2014, 37, 493–502. [Google Scholar] [CrossRef] [Green Version]
- Adans-Dester, C.; Hankov, N.; O’Brien, A.; Vergara-Diaz, G.; Black-Schaffer, R.; Zafonte, R.; Dy, J.; Lee, S.I.; Bonato, P. Enabling Precision Rehabilitation Interventions Using Wearable Sensors and Machine Learning to Track Motor Recovery. NPJ Digit. Med. 2020, 3, 121. [Google Scholar] [CrossRef]
- Chae, S.H.; Kim, Y.; Lee, K.-S.; Park, H.-S. Development and Clinical Evaluation of a Web-Based Upper Limb Home Rehabilitation System Using a Smartwatch and Machine Learning Model for Chronic Stroke Survivors: Prospective Comparative Study. JMIR MHealth UHealth 2020, 8, e17216. [Google Scholar] [CrossRef]
- Warmerdam, E.; Hausdorff, J.M.; Atrsaei, A.; Zhou, Y.; Mirelman, A.; Aminian, K.; Espay, A.J.; Hansen, C.; Evers, L.J.W.; Keller, A.; et al. Long-Term Unsupervised Mobility Assessment in Movement Disorders. Lancet Neurol. 2020, 19, 462–470. [Google Scholar] [CrossRef]
- Majumder, S.; Mondal, T.; Deen, M.J. Wearable Sensors for Remote Health Monitoring. Sensors 2017, 17, E130. [Google Scholar] [CrossRef]
- Bonnechère, B.; Sholukha, V.; Omelina, L.; Van Vooren, M.; Jansen, B.; Van Sint Jan, S. Suitability of Functional Evaluation Embedded in Serious Game Rehabilitation Exercises to Assess Motor Development across Lifespan. Gait Posture 2017, 57, 35–39. [Google Scholar] [CrossRef]
- Joshi, M.; Ashrafian, H.; Aufegger, L.; Khan, S.; Arora, S.; Cooke, G.; Darzi, A. Wearable Sensors to Improve Detection of Patient Deterioration. Expert Rev. Med. Devices 2019, 16, 145–154. [Google Scholar] [CrossRef]
- Dillenseger, A.; Weidemann, M.L.; Trentzsch, K.; Inojosa, H.; Haase, R.; Schriefer, D.; Voigt, I.; Scholz, M.; Akgün, K.; Ziemssen, T. Digital Biomarkers in Multiple Sclerosis. Brain Sci. 2021, 11, 1519. [Google Scholar] [CrossRef]
- Dorsey, E.R.; Papapetropoulos, S.; Xiong, M.; Kieburtz, K. The First Frontier: Digital Biomarkers for Neurodegenerative Disorders. Digit. Biomark. 2017, 1, 6–13. [Google Scholar] [CrossRef]
- Adams, J.L.; Dinesh, K.; Xiong, M.; Tarolli, C.G.; Sharma, S.; Sheth, N.; Aranyosi, A.J.; Zhu, W.; Goldenthal, S.; Biglan, K.M.; et al. Multiple Wearable Sensors in Parkinson and Huntington Disease Individuals: A Pilot Study in Clinic and at Home. Digit. Biomark. 2017, 1, 52–63. [Google Scholar] [CrossRef] [PubMed]
- Torous, J.; Rodriguez, J.; Powell, A. The New Digital Divide for Digital BioMarkers. Digit. Biomark. 2017, 1, 87–91. [Google Scholar] [CrossRef] [PubMed]
- Dagum, P. Digital Biomarkers of Cognitive Function. NPJ Digit. Med. 2018, 1, 10. [Google Scholar] [CrossRef] [PubMed]
- Bonnechère, B.; Van Vooren, M.; Bier, J.-C.; De Breucker, S.; Van Hove, O.; Van Sint Jan, S.; Feipel, V.; Jansen, B. The Use of Mobile Games to Assess Cognitive Function of Elderly with and without Cognitive Impairment. J. Alzheimer’s Dis. JAD 2018, 64, 1285–1293. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, D.; Farid, L.; Ferré, S.; Herraez, K.; Gracies, J.-M.; Hutin, E. Evaluation of the Validity and Reliability of Connected Insoles to Measure Gait Parameters in Healthy Adults. Sensors 2021, 21, 6543. [Google Scholar] [CrossRef]
- Lam, K.-H.; Twose, J.; McConchie, H.; Licitra, G.; Meijer, K.; de Ruiter, L.; van Lierop, Z.; Moraal, B.; Barkhof, F.; Uitdehaag, B.; et al. Smartphone-Derived Keystroke Dynamics Are Sensitive to Relevant Changes in Multiple Sclerosis. Eur. J. Neurol. 2022, 29, 522–534. [Google Scholar] [CrossRef]
- Chen, H.-M.; Chen, C.C.; Hsueh, I.-P.; Huang, S.-L.; Hsieh, C.-L. Test-Retest Reproducibility and Smallest Real Difference of 5 Hand Function Tests in Patients with Stroke. Neurorehabil. Neural Repair 2009, 23, 435–440. [Google Scholar] [CrossRef]
- Gladstone, D.J.; Danells, C.J.; Black, S.E. The Fugl-Meyer Assessment of Motor Recovery after Stroke: A Critical Review of Its Measurement Properties. Neurorehabil. Neural Repair 2002, 16, 232–240. [Google Scholar] [CrossRef]
- Barone, M.; Mendozzi, L.; D’Amico, F.; Saresella, M.; Rampelli, S.; Piancone, F.; La Rosa, F.; Marventano, I.; Clerici, M.; d’Arma, A.; et al. Influence of a High-Impact Multidimensional Rehabilitation Program on the Gut Microbiota of Patients with Multiple Sclerosis. Int. J. Mol. Sci. 2021, 22, 7173. [Google Scholar] [CrossRef]
- Mokhtarzade, M.; Molanouri Shamsi, M.; Abolhasani, M.; Bakhshi, B.; Sahraian, M.A.; Quinn, L.S.; Negaresh, R. Home-Based Exercise Training Influences Gut Bacterial Levels in Multiple Sclerosis. Complement. Ther. Clin. Pract. 2021, 45, 101463. [Google Scholar] [CrossRef]
- Peeters, L.M.; van Munster, C.E.; Van Wijmeersch, B.; Bruyndonckx, R.; Lamers, I.; Hellings, N.; Popescu, V.; Thalheim, C.; Feys, P. Multidisciplinary Data Infrastructures in Multiple Sclerosis: Why They Are Needed and Can Be Done! Mult. Scler. Houndmills Basingstoke Engl. 2019, 25, 500–509. [Google Scholar] [CrossRef]
- Ziemssen, T.; Kern, R.; Thomas, K. Multiple Sclerosis: Clinical Profiling and Data Collection as Prerequisite for Personalized Medicine Approach. BMC Neurol. 2016, 16, 124. [Google Scholar] [CrossRef] [Green Version]
- Baranzini, S.; Sawcer, S.; International Multiple Sclerosis Genetics Consortium; MultipleMS Consortium. Genetic analysis of multiple sclerosis severity identifies a novel locus and implicates CNS resilience as a major determinant of outcome. Res. Sq. 2022. preprint. [Google Scholar] [CrossRef]
- Simões, C.D.; Maukonen, J.; Kaprio, J.; Rissanen, A.; Pietiläinen, K.H.; Saarela, M. Habitual Dietary Intake Is Associated with Stool Microbiota Composition in Monozygotic Twins. J. Nutr. 2013, 143, 417–423. [Google Scholar] [CrossRef] [Green Version]
- Proctor, C.; Thiennimitr, P.; Chattipakorn, N.; Chattipakorn, S.C. Diet, Gut Microbiota and Cognition. Metab. Brain Dis. 2017, 32, 1–17. [Google Scholar] [CrossRef]
- Tian, H.; Chen, Q.; Yang, B.; Qin, H.; Li, N. Analysis of Gut Microbiome and Metabolite Characteristics in Patients with Slow Transit Constipation. Dig. Dis. Sci. 2021, 66, 3026–3035. [Google Scholar] [CrossRef]
- Rinninella, E.; Raoul, P.; Cintoni, M.; Franceschi, F.; Miggiano, G.A.D.; Gasbarrini, A.; Mele, M.C. What Is the Healthy Gut Microbiota Composition? A Changing Ecosystem across Age, Environment, Diet, and Diseases. Microorganisms 2019, 7, 14. [Google Scholar] [CrossRef] [Green Version]
- Anderson, G.; Rodriguez, M.; Reiter, R.J. Multiple Sclerosis: Melatonin, Orexin, and Ceramide Interact with Platelet Activation Coagulation Factors and Gut-Microbiome-Derived Butyrate in the Circadian Dysregulation of Mitochondria in Glia and Immune Cells. Int. J. Mol. Sci. 2019, 20, E5500. [Google Scholar] [CrossRef] [Green Version]
- Park, H.J.; Kim, S.A.; Kang, W.S.; Kim, J.W. Early-Life Stress Modulates Gut Microbiota and Peripheral and Central Inflammation in a Sex-Dependent Manner. Int. J. Mol. Sci. 2021, 22, 1899. [Google Scholar] [CrossRef]
- Gao, R.; Zhang, X.; Huang, L.; Shen, R.; Qin, H. Gut Microbiota Alteration After Long-Term Consumption of Probiotics in the Elderly. Probiotics Antimicrob. Proteins 2019, 11, 655–666. [Google Scholar] [CrossRef]
- Grothe, M.; Gross, S.; Süße, M.; Strauss, S.; Penner, I.K. The Seasonal Fluctuation of Fatigue in Multiple Sclerosis. Front. Neurol. 2022, 13, 900792. [Google Scholar] [CrossRef] [PubMed]
- Bonnechère, B.; Sholukha, V.; Omelina, L.; Van Sint Jan, S.; Jansen, B. 3D analysis of upper limbs motion during rehabilitation exercises using the KinectTM sensor: Development, laboratory validation and clinical application. Sensors 2018, 18, 2216. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garro, F.; Chiappalone, M.; Buccelli, S.; De Michieli, L.; Semprini, M. Neuromechanical Biomarkers for Robotic Neurorehabilitation. Front. Neurorobotics 2021, 15, 742163. [Google Scholar] [CrossRef] [PubMed]
- Severin, R.; Sabbahi, A.; Arena, R.; Phillips, S.A. Precision Medicine and Physical Therapy: A Healthy Living Medicine Approach for the Next Century. Phys. Ther. 2021, pzab253. [Google Scholar] [CrossRef] [PubMed]
- D’Amico, E.; Haase, R.; Ziemssen, T. Review: Patient-Reported Outcomes in Multiple Sclerosis Care. Mult. Scler. Relat. Disord. 2019, 33, 61–66. [Google Scholar] [CrossRef]
- Babrak, L.M.; Menetski, J.; Rebhan, M.; Nisato, G.; Zinggeler, M.; Brasier, N.; Baerenfaller, K.; Brenzikofer, T.; Baltzer, L.; Vogler, C.; et al. Traditional and Digital Biomarkers: Two Worlds Apart? Digit. Biomark. 2019, 3, 92–102. [Google Scholar] [CrossRef]
- Scott Kruse, C.; Karem, P.; Shifflett, K.; Vegi, L.; Ravi, K.; Brooks, M. Evaluating Barriers to Adopting Telemedicine Worldwide: A Systematic Review. J. Telemed. Telecare 2018, 24, 4–12. [Google Scholar] [CrossRef] [Green Version]
- Rangachari, P.; Mushiana, S.S.; Herbert, K. A Narrative Review of Factors Historically Influencing Telehealth Use across Six Medical Specialties in the United States. Int. J. Environ. Res. Public. Health 2021, 18, 4995. [Google Scholar] [CrossRef]
- U.S. Food & Drug Administration FDA Permits Marketing of First Game-Based Digital Therapeutic to Improve Attention Function in Children with ADHD. Available online: https://www.fda.gov/news-events/press-announcements/fda-permits-marketing-first-game-based-digital-therapeutic-improve-attention-function-children-adhd (accessed on 28 June 2021).
- Brigo, E.; Rintala, A.; Kossi, O.; Verwaest, F.; Vanhoof, O.; Feys, P.; Bonnechère, B. Using Telehealth to Guarantee the Continuity of Rehabilitation during the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public. Health 2022, 19, 10325. [Google Scholar] [CrossRef]
- Komaris, D.-S.; Tarfali, G.; O’Flynn, B.; Tedesco, S. Unsupervised IMU-Based Evaluation of at-Home Exercise Programmes: A Feasibility Study. BMC Sports Sci. Med. Rehabil. 2022, 14, 28. [Google Scholar] [CrossRef]
- Dalla-Costa, G.; Radaelli, M.; Maida, S.; Sangalli, F.; Colombo, B.; Moiola, L.; Comi, G.; Martinelli, V. Smart Watch, Smarter EDSS: Improving Disability Assessment in Multiple Sclerosis Clinical Practice. J. Neurol. Sci. 2017, 383, 166–168. [Google Scholar] [CrossRef]
- Matcham, F.; Leightley, D.; Siddi, S.; Lamers, F.; White, K.M.; Annas, P.; de Girolamo, G.; Difrancesco, S.; Haro, J.M.; Horsfall, M.; et al. Remote Assessment of Disease and Relapse in Major Depressive Disorder (RADAR-MDD): Recruitment, Retention, and Data Availability in a Longitudinal Remote Measurement Study. BMC Psychiatry 2022, 22, 136. [Google Scholar] [CrossRef]
- Totty, M.S.; Wade, E. Muscle Activation and Inertial Motion Data for Noninvasive Classification of Activities of Daily Living. IEEE Trans. Biomed. Eng. 2018, 65, 1069–1076. [Google Scholar] [CrossRef]
- Selvi, R.S.; Valarmathi, M.L. Optimal Feature Selection for Big Data Classification: Firefly with Lion-Assisted Model. Big Data 2020, 8, 125–146. [Google Scholar] [CrossRef]
- Ristevski, B.; Chen, M. Big Data Analytics in Medicine and Healthcare. J. Integr. Bioinforma. 2018, 15, 20170030. [Google Scholar] [CrossRef]
- Ahuja, Y.; Kim, N.; Liang, L.; Cai, T.; Dahal, K.; Seyok, T.; Lin, C.; Finan, S.; Liao, K.; Savovoa, G.; et al. Leveraging Electronic Health Records Data to Predict Multiple Sclerosis Disease Activity. Ann. Clin. Transl. Neurol. 2021, 8, 800–810. [Google Scholar] [CrossRef]
- Sun, Y.V.; Hu, Y.-J. Integrative Analysis of Multi-Omics Data for Discovery and Functional Studies of Complex Human Diseases. Adv. Genet. 2016, 93, 147–190. [Google Scholar] [CrossRef] [Green Version]
- Huang, C. Feature Selection and Feature Stability Measurement Method for High-Dimensional Small Sample Data Based on Big Data Technology. Comput. Intell. Neurosci. 2021, 2021, 3597051. [Google Scholar] [CrossRef]
- Almathami, H.K.Y.; Win, K.T.; Vlahu-Gjorgievska, E. Barriers and Facilitators That Influence Telemedicine-Based, Real-Time, Online Consultation at Patients’ Homes: Systematic Literature Review. J. Med. Internet Res. 2020, 22, e16407. [Google Scholar] [CrossRef]
- Engelsma, T.; Jaspers, M.W.M.; Peute, L.W. Considerate MHealth Design for Older Adults with Alzheimer’s Disease and Related Dementias (ADRD): A Scoping Review on Usability Barriers and Design Suggestions. Int. J. Med. Inf. 2021, 152, 104494. [Google Scholar] [CrossRef]
- Bonnechère, B.; Van Vooren, M.; Jansen, B.; Van Sint, J.S.; Rahmoun, M.; Fourtassi, M. Patients’ Acceptance of the Use of Serious Games in Physical Rehabilitation in Morocco. Games Health J. 2017, 6, 290–294. [Google Scholar] [CrossRef] [PubMed]
- Ottenbacher, K.J. Why Rehabilitation Research Does Not Work (as Well as We Think It Should). Arch. Phys. Med. Rehabil. 1995, 76, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Alfieri, F.M.; da Silva Dias, C.; de Oliveira, N.C.; Battistella, L.R. Gamification in Musculoskeletal Rehabilitation. Curr. Rev. Musculoskelet. Med. 2022, 15, 629–636. [Google Scholar] [CrossRef] [PubMed]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bonnechère, B. Integrating Rehabilomics into the Multi-Omics Approach in the Management of Multiple Sclerosis: The Way for Precision Medicine? Genes 2023, 14, 63. https://doi.org/10.3390/genes14010063
Bonnechère B. Integrating Rehabilomics into the Multi-Omics Approach in the Management of Multiple Sclerosis: The Way for Precision Medicine? Genes. 2023; 14(1):63. https://doi.org/10.3390/genes14010063
Chicago/Turabian StyleBonnechère, Bruno. 2023. "Integrating Rehabilomics into the Multi-Omics Approach in the Management of Multiple Sclerosis: The Way for Precision Medicine?" Genes 14, no. 1: 63. https://doi.org/10.3390/genes14010063