
LncRNA HULC and miR-122 Expression Pattern in HCC-Related HCV Egyptian Patients

Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Design
2.2. Study Groups
- Inclusion criteria:
- Exclusion criteria:
2.3. Blood Samples
2.4. miR-122 (NR_029667) and LncRNA HULC (NR_004855.2) Gene Expression Analysis
- PCR primers
2.5. Research Ethics Statement
2.6. Statistical Analysis
3. Results
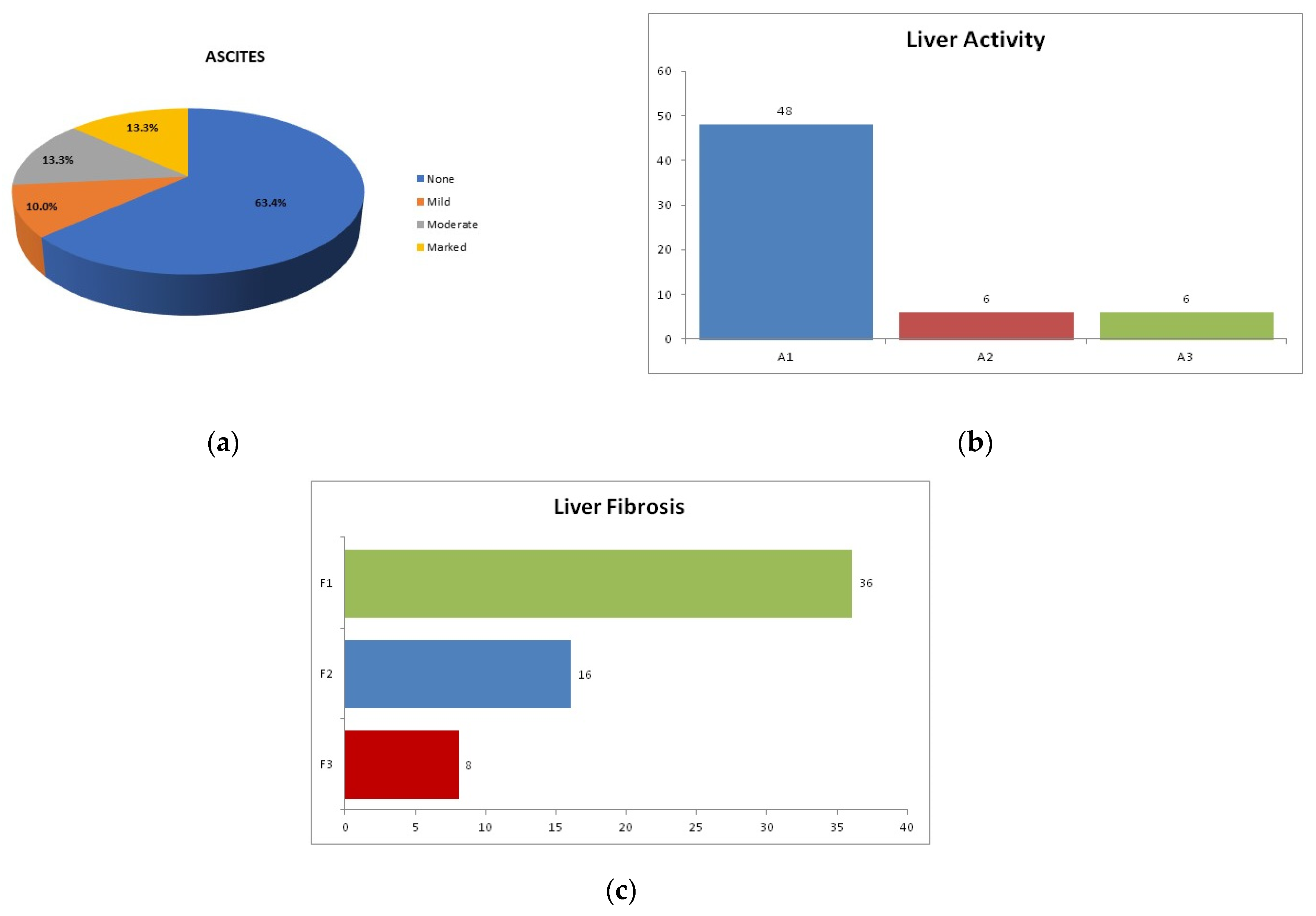
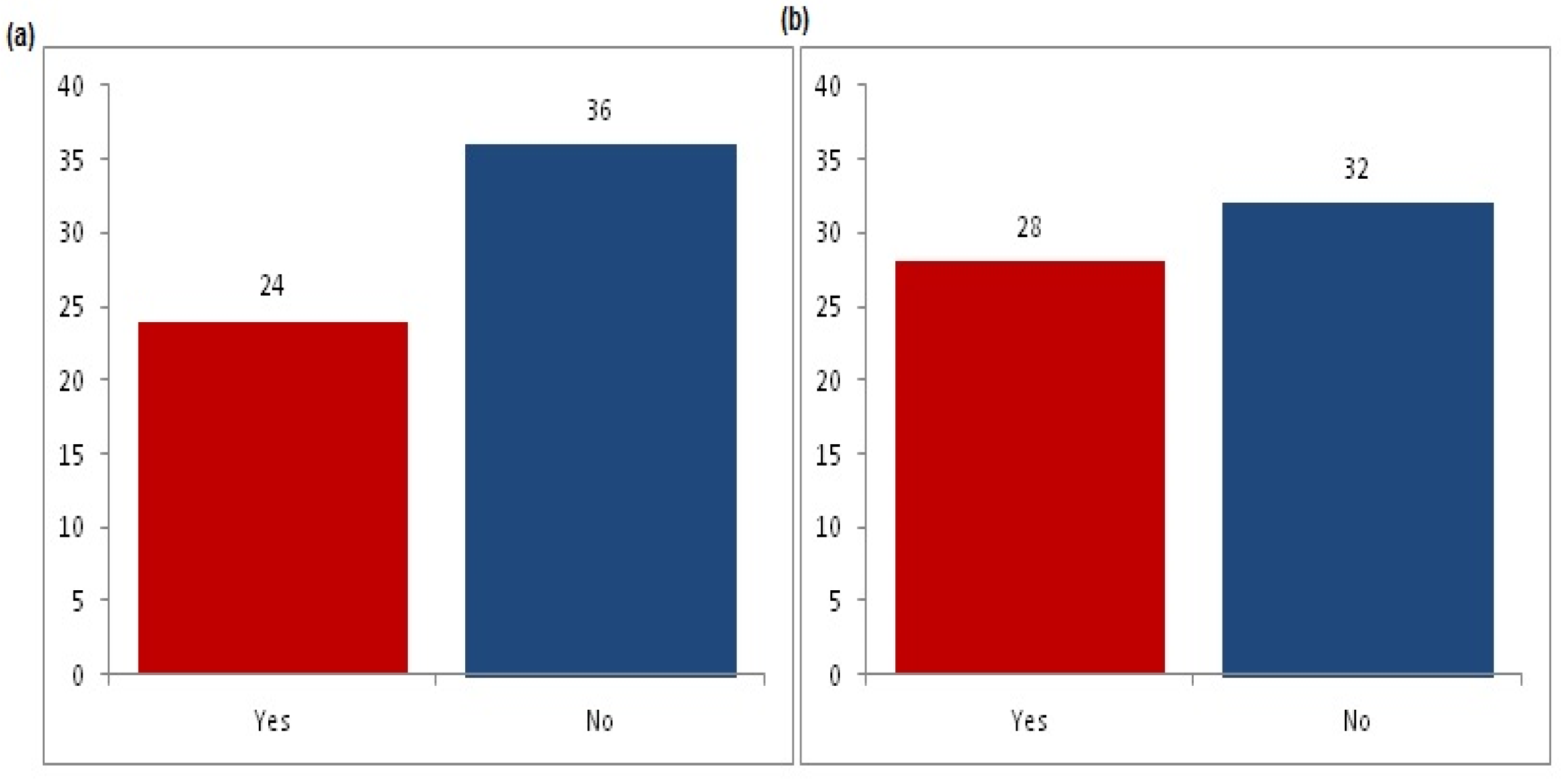
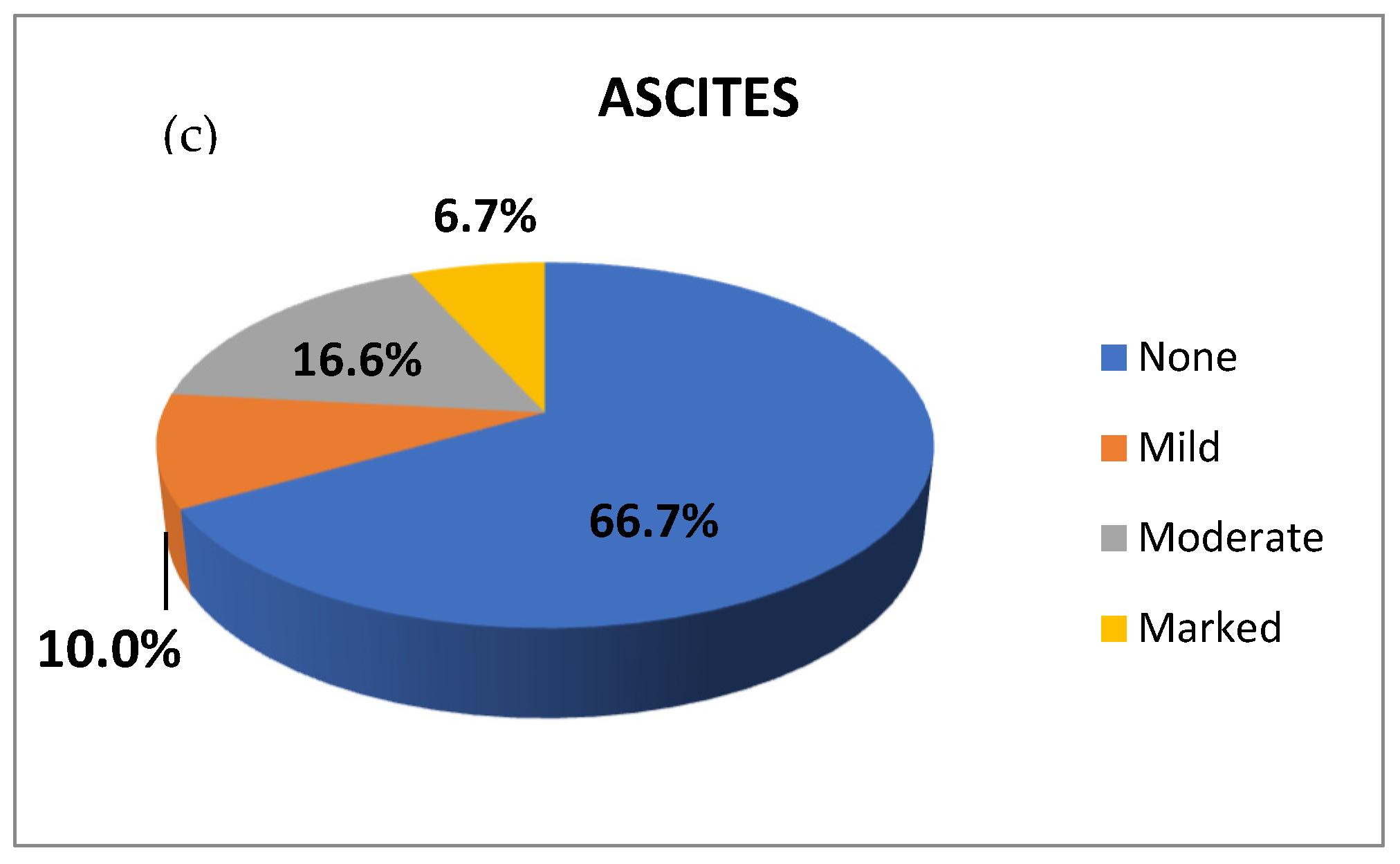
3.1. Patients’ Demographics and Clinico-Pathological Data
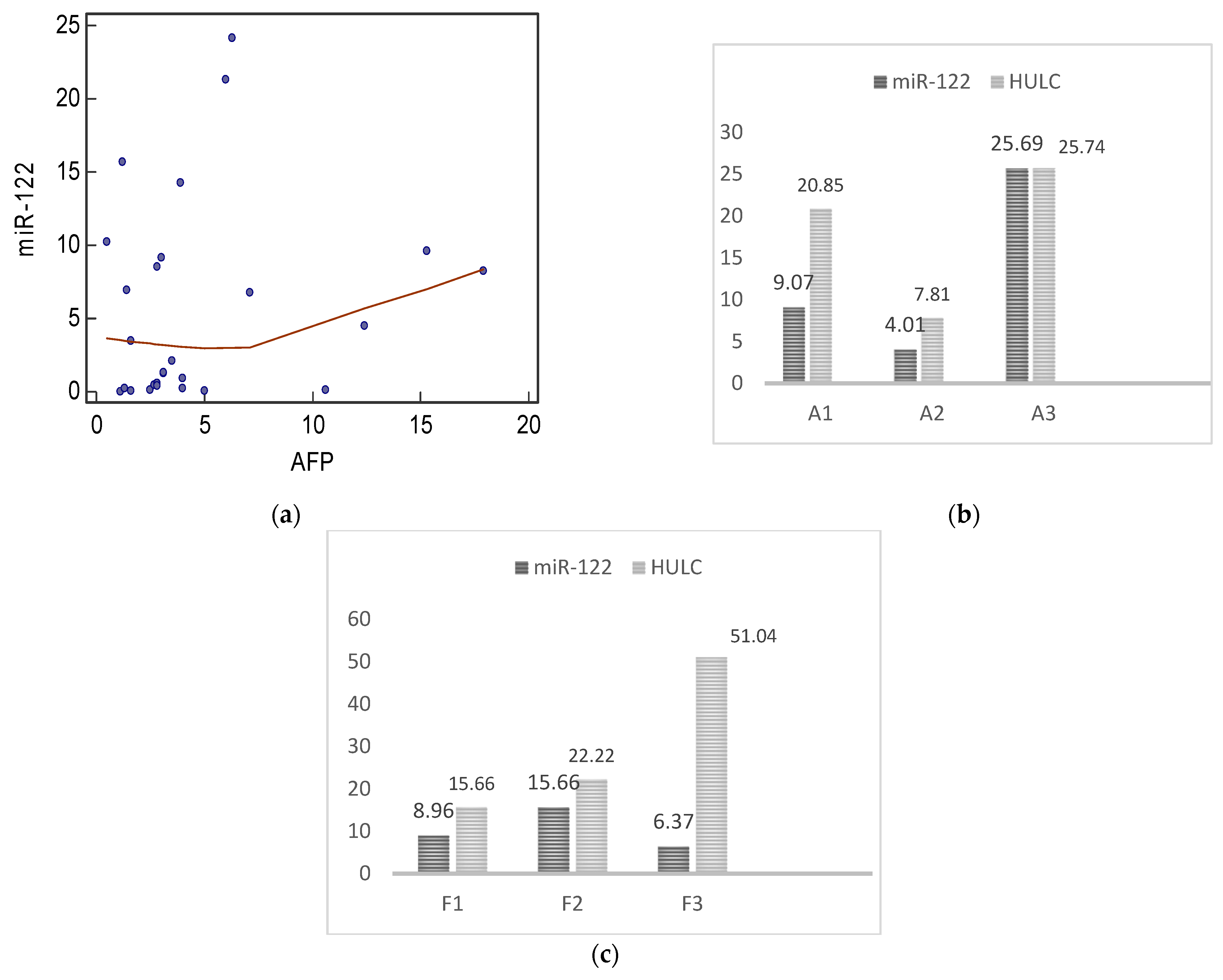
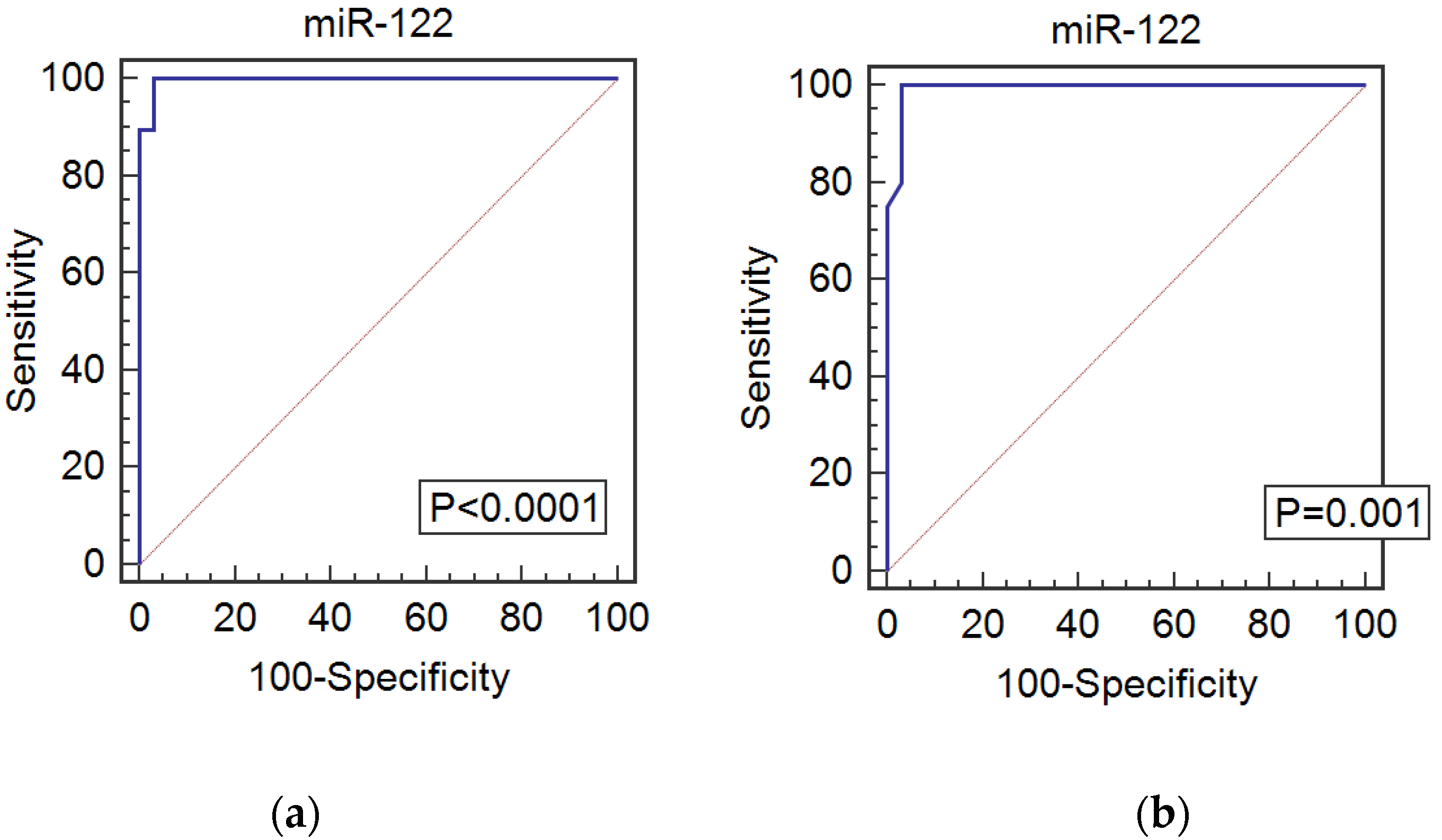
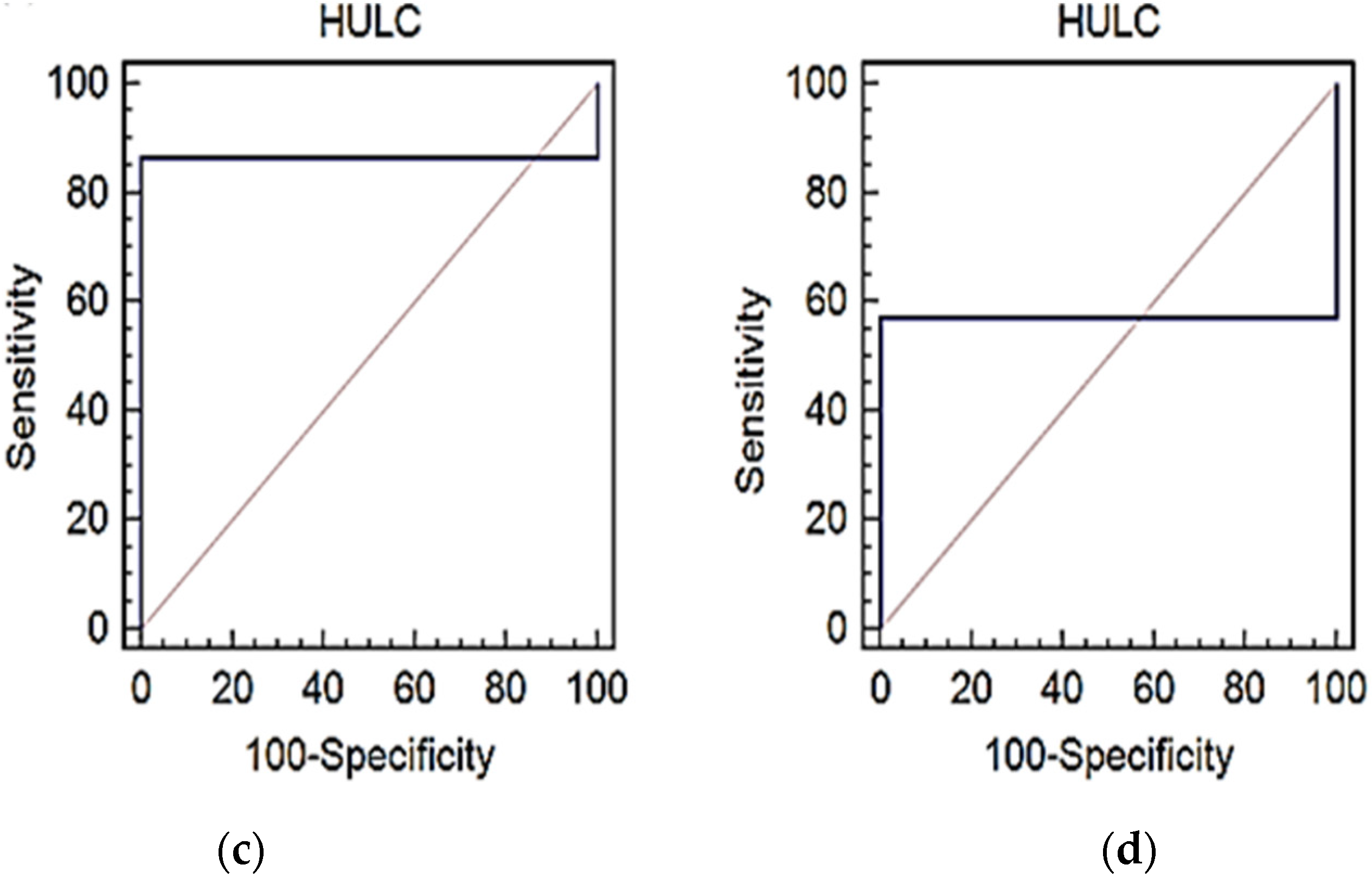
3.2. Gene Expression Analysis of Serum miR-122 and LncRNA HULC and Their Diagnostic Potential in HCV
3.3. Gene Expression Analysis of Serum miR-122 and LncRNA HULC and Their Diagnostic Potential in HCC
4. Discussion
5. Conclusions
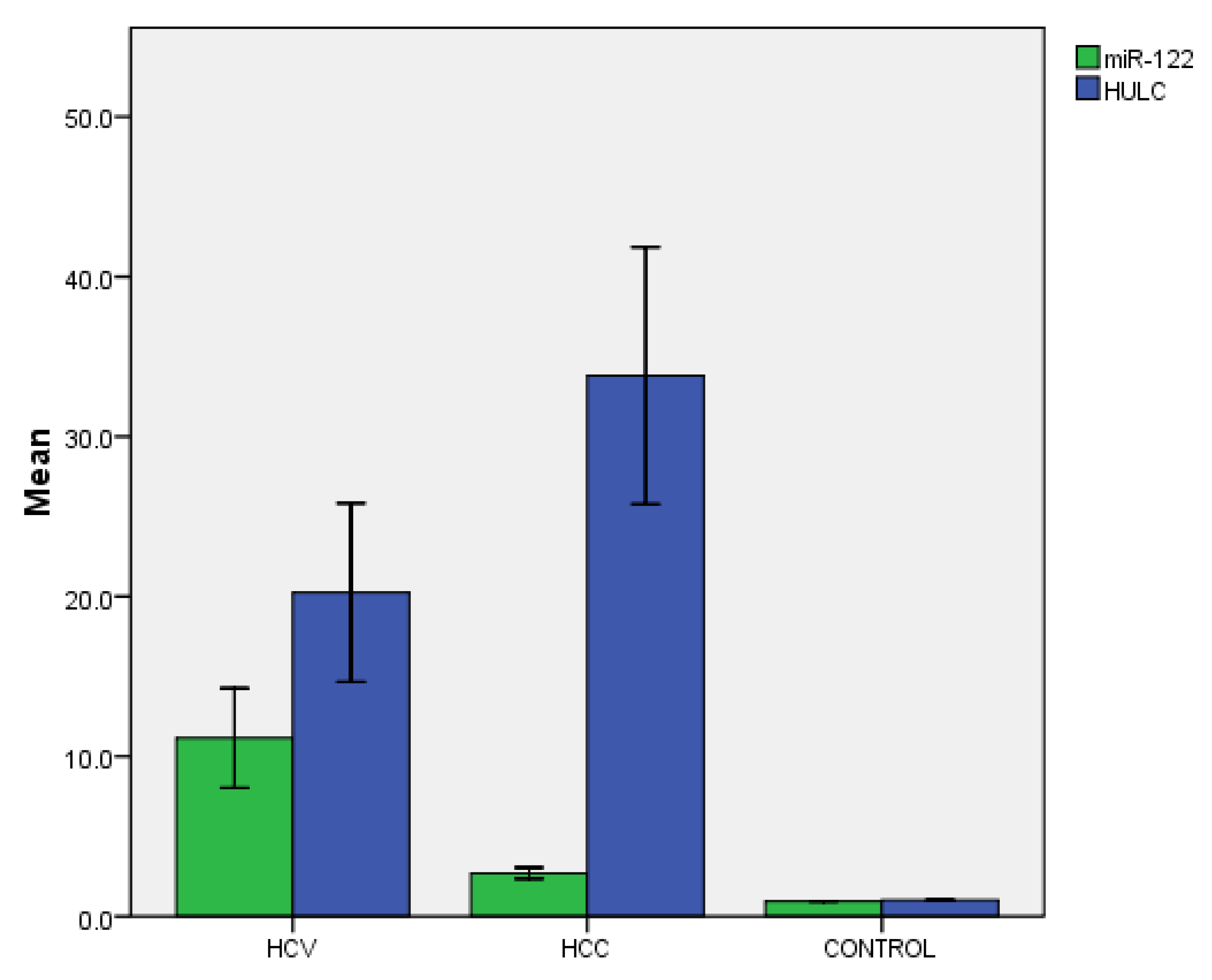
- Our study demonstrated the expression of lncRNA HULC and miR-122 in HCC patients compared to HCV patients and a normal control.
- miR-122 was markedly expressed in the HCV group compared to the HCC group. It can be considered a non-invasive diagnostic biomarker for HCV with a sensitivity of 96.8% and specificity of 99%.
- miR-122 was significantly more highly expressed in the HCV group compared to the HCC group, indicating its prognostic value as a predictor of HCC in patients with chronic HCV.
- HULC was markedly expressed in the HCC group compared to the HCV group and control group. It can be considered a non-invasive diagnostic biomarker for HCC with a sensitivity of 57% and specificity of 100%.
- HULC was also expressed in the HCV group; hence, it can be considered a non-invasive diagnostic biomarker with a sensitivity of 84% and specificity of 99%.
- It is recommended to use other miRNAs to make an miRNAs signature through the development of panels containing many miRNA biomarkers and LncRNAs, or to add even conventional α-fetoprotein to these panels in the diagnosis and screening of HCV and HCC, which would help achieve greater accuracy.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Rawla, P.; Sunkarar, T.; Muralidharan, P.; Raj, J.P. Update in global trends and aetiology of hepatocellular carcinoma. Contemp. Oncol. 2018, 22, 141–150. [Google Scholar] [CrossRef] [PubMed]
- Slotta, J.E.; Kollmar, O.; Ellenrieder, V.; Ghadimi, B.M.; Homayounfar, K. Hepatocellular carcinoma: Surgeon’s view on latest findings and future perspectives. World J. Hepatol. 2015, 7, 1168–1183. [Google Scholar] [CrossRef] [PubMed]
- Altekruse, S.F.; McGlynn, K.A.; Reichman, M.E. Hepatocellular Carcinoma Incidence, Mortality, and Survival Trends in the United States From 1975 to 2005. J. Clin. Oncol. 2009, 27, 1485–1491. [Google Scholar] [CrossRef]
- Zhang, H.; Zhang, W.; Jiang, L.; Chen, Y. Recent advances in systemic therapy for hepatocellular carcinoma. Biomark. Res. 2022, 10, 3. [Google Scholar] [CrossRef]
- Dhanoa, J.K.; Sethi, R.S.; Verma, R.; Arora, J.S.; Mukhopadhyay, C.S. Long non coding RNA: Its Evolutionary Relics and Biological Implications in Mammals: A review. J. Anim. Sci. Technol. 2018, 60, 25. [Google Scholar] [CrossRef] [PubMed]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2 (−Delta Delta C (T)) method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef] [PubMed]
- Khothari, C.R. Research Methodology: Methods and Techniques, 2nd ed.; New Age International Publishers: New Delhi, India, 2004. [Google Scholar]
- Shaker, O.; Mahfouz, H.; Salama, A.; Medhat, E. Long Non-Coding HULC and miRNA-372 as diagnostic biomarkers in hepatocellular carcinoma. Rep. Biochem. Mol. Biol. 2020, 9, 230–240. [Google Scholar] [CrossRef]
- Kitabayashi, J.; Shirasaki, T.; Shimakami, T.; Nishiyama, T.; Welsch, C.; Funaki, M.; Murai, K.; Sumiyadorj, A.; Takatori, H.; Kitamura, K.; et al. Upregulation of the Long Noncoding RNA HULC by Hepatitis C Virus and Its Regulation of Viral Replication. J. Infect. Dis. 2020, 226, 407–419. [Google Scholar] [CrossRef]
- Rashed, W.M.; Kandeil, M.A.M.; Mahmoud, M.O.; Ezzat, S. Hepatocellular Carcinoma (HCC) in Egypt: A comprehensive overview. J. Egypt. Natl. Cancer Inst. 2020, 32, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carrieri, C.; Cimatti, L.; Biagioli, M.; Beugnet, A.; Zucchelli, S.; Fedele, S.; Pesce, E.; Ferrer, I.; Collavin, L.; Santoro, C.; et al. Long non-coding antisense RNA controls Uchl1 translation through an embedded SINEB2 repeat. Nature 2012, 491, 454–457. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, J.; Hayder, H.; Zayed, Y.; Peng, C. Overview of microRNA biogenesis, mechanisms of actions, and circulation. Front. Endocrinol. 2018, 9, 402. [Google Scholar] [CrossRef]
- Toh, T.B.; Lim, J.J.; Chow, E. Epigenetics of hepatocellular carcinoma. Clin. Transl. Med. 2019, 8, e13. [Google Scholar] [CrossRef] [PubMed]
- Panzitt, K.; Tschernatsch, M.M.; Guelly, C.; Moustafa, T.; Stradner, M.; Strohmaier, H.M.; Buck, C.R.; Denk, H.; Schroeder, R.; Trauner, M.; et al. Characterization of HULC, a novel gene with striking up-regulation in hepatocellular carcinoma, as noncoding RNA. Gastroenterology 2007, 132, 330–342. [Google Scholar] [CrossRef] [PubMed]
- Kutay, H.; Bai, S.; Datta, J.; Motiwala, T.; Pogribny, I.; Frankel, W.; Jacob, S.T.; Ghoshal, K. Downregulation of miR-122 in the rodent and human hepatocellular carcinomas. J. Cell. Biochem. 2006, 99, 671–678. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, Y.; Jiang, W.; Li, Q.; Lan, Y. The clinical significance of microRNA-122 in predicting the prognosis of patients with hepatocellular carcinoma: A meta-analysis validated by the Cancer Genome Atlas dataset. Medicine 2019, 98, e14810. [Google Scholar] [CrossRef] [PubMed]
- Gopal, P.; Yopp, A.C.; Waljee, A.K.; Chiang, J.; Nehra, M.; Kandunoori, P.; Singal, A.G. Factors that affect accuracy of α-fetoprotein test in detection of hepatocellular carcinoma in patients with cirrhosis. Clin. Gastroenterol. Hepatol. 2014, 12, 870–877. [Google Scholar] [CrossRef] [PubMed]
- Axley, P.; Ahmed, Z.; Ravi, S.; Singal, A.K. Hepatitis C virus and hepatocellular carcinoma: A narrative review. J. Clin. Transl. Hepatol. 2018, 6, 79–84. [Google Scholar] [CrossRef]
- Montaser, M.F.; Sakr, M.A.; Khalifa, M.O. Alpha-L-fucosidase as a tumour marker of hepatocellular carcinoma. Arab. J. Gastroenterol. 2012, 13, 9–13. [Google Scholar] [CrossRef]
- Knight, K.; Wade, S.; Balducci, L. Prevalence and outcomes of anemia in cancer: A systematic review of the literature. Am. J. Med. 2004, 116, 11–26. [Google Scholar] [CrossRef] [PubMed]
- Finkelmeier, F.; Bettinger, D.; Köberle, V.; Schultheiß, M.; Zeuzem, S.; Kronenberger, B.; Piiper, A.; Waidmann, O. Single measurement of hemoglobin predicts outcome of HCC patients. Med. Oncol. 2014, 31, 806. [Google Scholar] [CrossRef] [PubMed]
- Bandiera, S.; Pfeffer, S.; Baumert, T.F.; Zeisel, M.B. miR-122–a key factor and therapeutic target in liver disease. J. Hepatol. 2015, 62, 448–457. [Google Scholar] [CrossRef] [PubMed]
- Tsai, W.; Hsu, P.W.; Lai, T.; Chau, G.; Lin, C.; Chen, C.; Lin, C.; Liao, Y.; Wang, J.; Chau, Y.; et al. MicroRNA-122, a tumor suppressor microRNA that regulates intrahepatic metastasis of hepatocellular carcinoma. Hepatology 2009, 49, 1571–1582. [Google Scholar] [CrossRef]
- Turato, C.; Fornari, F.; Pollutri, D.; Fassan, M.; Quarta, S.; Villano, G.; Ruvoletto, G.; Bolondi, L.; Gramantieri, L.; Pontisso, P. MiR-122 Targets SerpinB3 and Is Involved in Sorafenib Resistance in Hepatocellular Carcinoma. J. Clin. Med. 2019, 8, 171. [Google Scholar] [CrossRef] [PubMed]
- Parizadeh, S.M.; Jafarzadeh-Esfehani, R.; Ghandehari, M.; Goldani, F.; Parizadeh, S.M.R.; Hassanian, S.M.; Ghayour-Mobarhan, M.; Ferns, G.A.; Avan, A. MicroRNAs as potential diagnostic and prognostic biomarkers in hepatocellular carcinoma. Curr. Drug Targets 2019, 20, 1129–1140. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Jiang, D.; Rao, H.; Zhao, J.; Wang, Y.; Wei, L. Absolute quantification of serum microRNA-122 and its correlation with liver inflammation grade and serum alanine aminotransferase in chronic hepatitis C patients. Int. J. Infect. Dis. 2015, 30, 52–56. [Google Scholar] [CrossRef]
- Xu, J.; Wu, C.; Che, X.; Wang, L.; Yu, D.; Zhang, T.; Huang, L.; Li, H.; Tan, W.; Wang, C.; et al. Circulating microRNAs, miR-21, miR-122, and miR-223, in patients with hepatocellular carcinoma or chronic hepatitis. Mol. Carcinog. 2011, 50, 136–142. [Google Scholar] [CrossRef] [PubMed]
- Trebicka, J.; Anadol, E.; Elfimova, N.; Strack, I.; Roggendorf, M.; Viazov, S.; Wedemeyer, I.; Drebber, U.; Rockstroh, J.; Sauerbruch, T.; et al. Hepatic and serum levels of miR-122 after chronic HCV-induced fibrosis. J. Hepatol. 2013, 58, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Waidmann, O.; Köberle, V.; Brunner, F.; Zeuzem, S.; Piiper, A.; Kronenberger, B. Serum microRNA-122 predicts survival in patients with liver cirrhosis. PLoS ONE 2012, 7, e45652. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Liu, X.; Wu, H.; Ni, P.; Gu, Z.; Qiao, Y.; Chen, N.; Sun, F.; Fan, Q. CREB up-regulates long non-coding RNA, HULC expression through interaction with microRNA-372 in liver cancer. Nucleic Acids Res. 2010, 38, 5366–5383. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, M.; Chen, W.; Qi, F.; Xia, R.; Sun, M.; Xu, T.; Yin, L.; Zhang, E.; De, W.; Shu, Y. Long non-coding RNA ANRIL is upregulated in hepatocellular carcinoma and regulates cell apoptosis by epigenetic silencing of KLF2. J. Hematol. Oncol. 2015, 8, 50. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Xu, H.; Yu, Y.; He, J.; Wang, Z.; Xu, Y.; Wang, C.; Zhang, H.; Zhang, R.; Zhang, J.; et al. LncRNA HULC enhances epithelial-mesenchymal transition to promote tumorigenesis and metastasis of hepatocellular carcinoma via the miR-200a-3p/ZEB1 signaling pathway. Oncotarget 2016, 7, 42431. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Jiang, X.; Li, X.; Song, S.; Meng, Q.; Wang, L.; Lu, Y.; Xin, X.; Pu, H.; Gui, X.; et al. Long noncoding RNA HULC accelerates the growth of human liver cancer stem cells by upregulating CyclinD1 through miR675- PKM2 pathway via autophagy. Stem Cell Res. Ther. 2020, 11, 8. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.A.; Fawzi, M.; Sabri, D.; Sedrak, H.; Mausa, S.; El-Saadi, A. Liver Specific Serum Micro RNA122 as a Prognostic Marker in Egyptian Patients with Liver Cirrhosis. Arch. Hepat. Res. 2017, 3, 4–9. [Google Scholar] [CrossRef]
- Zhao, X.F.; Li, N.; Lin, D.D.; Sun, L.B. Circulating MicroRNA-122 for the diagnosis of hepatocellular carcinoma: A meta-analysis. Biomed. Res. Int. 2020, 2020, 5353695. [Google Scholar] [CrossRef]
- Xie, H.; Ma, H.; Zhou, D. Plasma HULC as a promising novel biomarker for the detection of hepatocellular carcinoma. Biomed. Res. Int. 2013, 2013, 136106. [Google Scholar] [CrossRef] [Green Version]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical Data | HCV (N = 60) | HCC (N = 60) | Control (N = 30) | p-Value |
|---|---|---|---|---|
| Age (years) | 38.20 ± 8.20 | 60.47 ± 7.28 | 34.47 ± 3.70 | 0.0001 a 0.029 b 0.001 c |
| Gender | ||||
| Female | 12 (20%) | 10 (16.7%) | 11 (36.7%) | |
| Male | 48 (80%) | 50 (88.3%) | 19 (66.3%) | 0.15 |
| Clinical Data | HCV (N = 60) | HCC (N = 60) | Control (N = 30) | p-Value |
|---|---|---|---|---|
| ALT (U/L) | 59.6 ± 41.8 | 84.8 ± 52.5 | 30.2 ± 6.6 | 0.045 a 0.001 b 0.000 c |
| AST (U/L) | 49.03 ± 36.1 | 114.6 ± 65.5 | 25.70 ± 5.8 | 0.0001 a 0.001 b 0.000 c |
| ALP (U/L) | 151.2 ± 159.3 | 184.3 ± 162.6 | - | 0.43 |
| Albumin (g/dL) | 3.81 ± 0.73 | 3.5 ± 1.16 | - | 0.26 |
| Total Bilirubin (mg/dL) | 1.02 ± 0.66 | 1.635 ± 1.1147 | - | 0.013 |
| Indirect Bilirubin (mg/dL) | 0.33 ± 0.356 | 0.71 ± 0.65 | - | 0.008 |
| Hb (g/dL) | 13.30 ± 1.9 | 11.24 ± 2.5 | 13.32 ± 1.22 | 0.021 a 0.20 b 0.0001 c |
| TLC x1000/µL | 6.6 ± 2.30 | 5.5 ± 2.2 | 6.2 ± 1.41 | 0.077 a 0.39 b 0.10 c |
| Plts x1000/µL | 206.37 ± 96.36 | 119.60 ± 52.25 | 296.6 ± 61.8 | 0.001 a 0.002 b 0.001 c |
| AFP (ng/mL) | 5.71 ± 6.63 | 1449.08 ± 2911.0 | - | 0.0001 |
| Urea (mg/dL) | 25.89 ± 6.07 | 11.39 ± 3.38 | 29.16 ± 6.06 | 0.001 a 0.20 b 0.05 c |
| GGT (U/L) | - | 68.79 ± 60.9 | - | - |
| Creatinine (mg/dL) | 0.84 ± 0.17 | 1.08 ± 0.43 | 0.78 ± 0.13 | 0.04 a 0.1 b 0.01 c |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gaber, D.A.; Shaker, O.; Younis, A.T.; El-Kassas, M. LncRNA HULC and miR-122 Expression Pattern in HCC-Related HCV Egyptian Patients. Genes 2022, 13, 1669. https://doi.org/10.3390/genes13091669
Gaber DA, Shaker O, Younis AT, El-Kassas M. LncRNA HULC and miR-122 Expression Pattern in HCC-Related HCV Egyptian Patients. Genes. 2022; 13(9):1669. https://doi.org/10.3390/genes13091669
Chicago/Turabian StyleGaber, Dalia A., Olfat Shaker, Alaa Tarek Younis, and Mohamed El-Kassas. 2022. "LncRNA HULC and miR-122 Expression Pattern in HCC-Related HCV Egyptian Patients" Genes 13, no. 9: 1669. https://doi.org/10.3390/genes13091669