
PCR-Based Screening of Spinal Muscular Atrophy for Newborn Infants in Hyogo Prefecture, Japan
 , , , , , , , , , and add
Show full author list
, , , , , , , , , and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Fetuses with SMA
2.2. Implementation of SMA-NBS in Hyogo Prefecture
2.3. SMN1 Deletion Screening with Dried Blood Spots
2.4. Definitive Diagnosis with Freshly Collected Blood
2.5. Inspection of Inhibitory Effect of Heparin on PCR Assay with DBS
2.6. Statistical Analysis
3. Results
3.1. Births of SMA Infants in Hyogo Prefecture during the Period 2007–2016
3.2. Estimated Incidence of SMA in Hyogo Prefecture
3.3. Frequency of False-Positive Cases
3.4. Influencing Factors for PCR-Based Screening
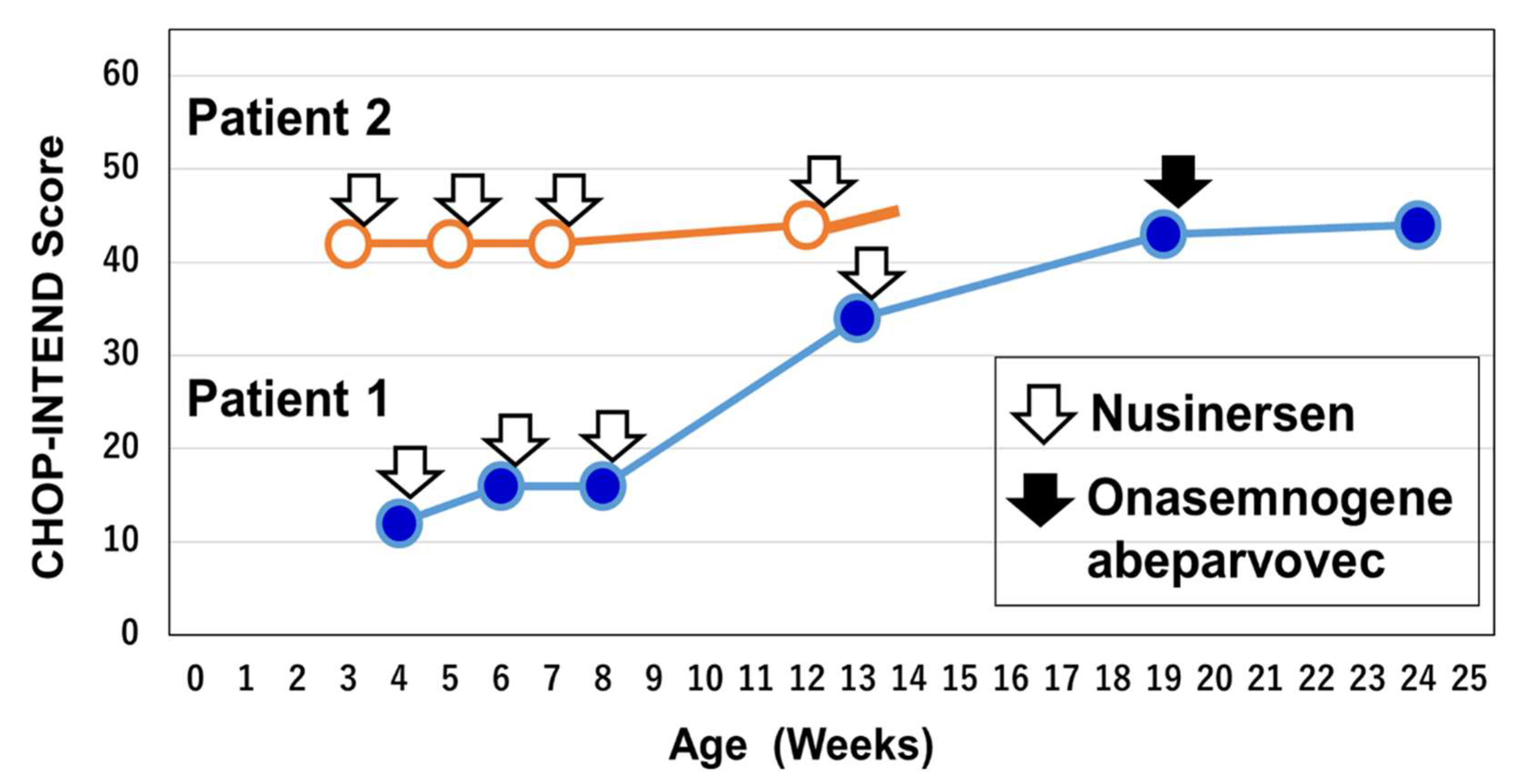
3.5. Patient 1: A Symptomatic Patient Identified by SMA-NBS
3.6. Patient 2: A Pre-Symptomatic Patient Identified by SMA-NBS
4. Discussion
4.1. Newborn Infants with SMA and Aborted Fetuses in the Period 2007–2016
4.2. Incidence Rates of SMA Based on Newborn Screening
4.3. False-Positive Cases in Hyogo Prefecture
4.4. SMA-NBS and Pre-Symptomatic Treatment
4.5. SMA-NBS and Post-Symptomatic Treatment
4.6. Research Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nurputra, D.K.; Lai, P.S.; Harahap, N.I.F.; Morikawa, S.; Yamamoto, T.; Nishimura, N.; Kubo, Y.; Takeuchi, A.; Saito, T.; Takeshima, Y.; et al. Spinal Muscular Atrophy: From Gene Discovery to Clinical Trials. Ann. Hum. Genet. 2013, 77, 435–463. [Google Scholar] [CrossRef]
- Verhaart, I.E.C.; Robertson, A.; Leary, R.; McMacken, G.; König, K.; Kirschner, J.; Jones, C.C.; Cook, S.F.; Lochmüller, H. Multi-source approach to determine SMA incidence and research ready population. J. Neurol. 2017, 264, 1465–1473. [Google Scholar] [CrossRef] [PubMed]
- Arnold, W.D.; Kassar, D.; Kissel, J.T. Spinal muscular atrophy: Diagnosis and management in a new therapeutic era. Muscle. Nerve. 2015, 51, 157–167. [Google Scholar] [CrossRef]
- Kimizu, T.; Ida, S.; Okamoto, K.; Awano, H.; Niba, E.T.E.; Wijaya, Y.O.S.; Okazaki, S.; Shimomura, H.; Lee, T.; Tominaga, K.; et al. Spinal Muscular Atrophy: Diagnosis, Incidence, and Newborn Screening in Japan. Int. J. Neonatal Screen. 2021, 7, 45. [Google Scholar] [CrossRef] [PubMed]
- Lally, C.; Jones, C.; Farwell, W.; Reyna, S.P.; Cook, S.F.; Flanders, W.D. Indirect Estimation of the Prevalence of Spinal Muscular Atrophy Type I, II, and III in the United States. Orphanet J. Rare Dis. 2017, 12, 175. [Google Scholar] [CrossRef]
- Oskoui, M.; Levy, G.; Garland, C.J.; Gray, J.M.; O′Hagen, J.; Vivo, D.C.D.; Kaufmann, P. The Changing Natural History of Spinal Muscular Atrophy Type 1. Neurology 2007, 69, 1931–1936. [Google Scholar] [CrossRef]
- Farrar, M.A.; Park, S.B.; Vucic, S.; Carey, K.A.; Turner, B.J.; Gillingwater, T.H.; Swoboda, K.J.; Kiernan, M.C. Emerging Therapies and Challenges in Spinal Muscular Atrophy. Ann. Neurol. 2017, 81, 355–368. [Google Scholar] [CrossRef] [PubMed]
- Lefebvre, S.; Bürglen, L.; Reboullet, S.; Clermont, O.; Burlet, P.; Viollet, L.; Benichou, B.; Cruaud, C.; Millasseau, P.; Zeviani, M. Identification and Characterization of a Spinal Muscular Atrophy-Determining Gene. Cell 1995, 80, 155–165. [Google Scholar] [CrossRef]
- Calucho, M.; Bernal, S.; Alías, L.; March, F.; Venceslá, A.; Rodríguez-Álvarez, F.J.; Aller, E.; Fernández, R.M.; Borrego, S.; Millán, J.M.; et al. Correlation between SMA Type and SMN2 Copy Number Revisited: An Analysis of 625 Unrelated Spanish Patients and a Compilation of 2834 Reported Cases. Neuromuscul. Disord. 2018, 28, 208–215. [Google Scholar] [CrossRef]
- Butchbach, M.E.R. Copy Number Variations in the Survival Motor Neuron Genes: Implications for Spinal Muscular Atrophy and Other Neurodegenerative Diseases. Front. Mol. Biosci. 2016, 3, 7. [Google Scholar] [CrossRef]
- Finkel, R.S.; Mercuri, E.; Darras, B.T.; Connolly, A.M.; Kuntz, N.L.; Kirschner, J.; Chiriboga, C.A.; Saito, K.; Servais, L.; Tizzano, E.; et al. Nusinersen versus Sham Control in Infantile-Onset Spinal Muscular Atrophy. N. Engl. J. Med. 2017, 377, 1723–1732. [Google Scholar] [CrossRef] [PubMed]
- Mendell, J.R.; Al-Zaidy, S.; Shell, R.; Arnold, W.D.; Rodino-Klapac, L.R.; Prior, T.W.; Lowes, L.; Alfano, L.; Berry, K.; Church, K.; et al. Single-Dose Gene-Replacement Therapy for Spinal Muscular Atrophy. N. Engl. J. Med. 2017, 377, 1713–1722. [Google Scholar] [CrossRef]
- Baranello, G.; Darras, B.T.; Day, J.W.; Deconinck, N.; Klein, A.; Masson, R.; Mercuri, E.; Rose, K.; El-Khairi, M.; Gerber, M.; et al. Risdiplam in Type 1 Spinal Muscular Atrophy. N. Engl. J. Med. 2021, 384, 915–923. [Google Scholar] [CrossRef] [PubMed]
- Vivo, D.C.D.; Bertini, E.; Swoboda, K.J.; Hwu, W.-L.; Crawford, T.O.; Finkel, R.S.; Kirschner, J.; Kuntz, N.L.; Parsons, J.A.; Ryan, M.M.; et al. Nusinersen Initiated in Infants during the Presymptomatic Stage of Spinal Muscular Atrophy: Interim Efficacy and Safety Results from the Phase 2 NURTURE Study. Neuromuscul. Disord. 2019, 29, 842–856. [Google Scholar] [CrossRef]
- Strauss, K.A.; Farrar, M.A.; Muntoni, F.; Saito, K.; Mendell, J.R.; Servais, L.; McMillan, H.J.; Finkel, R.S.; Swoboda, K.J.; Kwon, J.M.; et al. Onasemnogene Abeparvovec for Presymptomatic Infants with Two Copies of SMN2 at Risk for Spinal Muscular Atrophy Type 1: The Phase III SPR1NT Trial. Nat. Med. 2022, 28, 1381–1389. [Google Scholar] [CrossRef]
- Strauss, K.A.; Farrar, M.A.; Muntoni, F.; Saito, K.; Mendell, J.R.; Servais, L.; McMillan, H.J.; Finkel, R.S.; Swoboda, K.J.; Kwon, J.M.; et al. Onasemnogene Abeparvovec for Presymptomatic Infants with Three Copies of SMN2 at Risk for Spinal Muscular Atrophy: The Phase III SPR1NT Trial. Nat. Med. 2022, 28, 1390–1397. [Google Scholar] [CrossRef]
- Schorling, D.C.; Pechmann, A.; Kirschner, J. Advances in Treatment of Spinal Muscular Atrophy–New Phenotypes, New Challenges, New Implications for Care. J. Neuromuscul. Dis. 2020, 7, 1–13. [Google Scholar] [CrossRef]
- Dangouloff, T.; Vrščaj, E.; Servais, L.; Osredkar, D.; Adoukonou, T.; Aryani, O.; Barisic, N.; Bashiri, F.; Bastaki, L.; Benitto, A.; et al. Newborn Screening Programs for Spinal Muscular Atrophy Worldwide: Where We Stand and Where to Go. Neuromuscul. Disord. 2021, 31, 574–582. [Google Scholar] [CrossRef]
- Sawada, T.; Kido, J.; Sugawara, K.; Yoshida, S.; Ozasa, S.; Nomura, K.; Okada, K.; Fujiyama, N.; Nakamura, K. Newborn Screening for Spinal Muscular Atrophy in Japan: One Year of Experience. Mol. Genet. Metab. Rep. 2022, 32, 100908. [Google Scholar] [CrossRef] [PubMed]
- McAndrew, P.E.; Parsons, D.W.; Simard, L.R.; Rochette, C.; Ray, P.N.; Mendell, J.R.; Prior, T.W.; Burghes, A.H. Identification of Proximal Spinal Muscular Atrophy Carriers and Patients by Analysis of SMNT and SMNC Gene Copy Number. Am. J. Hum. Genet. 1997, 60, 1411–1422. [Google Scholar] [CrossRef]
- Abràmoff, M.D.; Magalhães, P.J.; Ram, S.J. Image Processing with ImageJ. Biophotonics Int. 2004, 11, 36–42. [Google Scholar]
- Ito, M.; Yamauchi, A.; Urano, M.; Kato, T.; Matsuo, M.; Nakashima, K.; Saito, K. Epidemiological Investigation of Spinal Muscular Atrophy in Japan. Brain Dev. 2022, 44, 2–16. [Google Scholar] [CrossRef] [PubMed]
- Chien, Y.-H.; Chiang, S.-C.; Weng, W.-C.; Lee, N.-C.; Lin, C.-J.; Hsieh, W.-S.; Lee, W.-T.; Jong, Y.-J.; Ko, T.-M.; Hwu, W.-L. Presymptomatic Diagnosis of Spinal Muscular Atrophy Through Newborn Screening. J. Pediatr. 2017, 190, 124–129. [Google Scholar] [CrossRef]
- Kraszewski, J.N.; Kay, D.M.; Stevens, C.F.; Koval, C.; Haser, B.; Ortiz, V.; Albertorio, A.; Cohen, L.L.; Jain, R.; Andrew, S.P.; et al. Pilot study of population-based newborn screening for spinal muscular atrophy in New York state. Genet. Med. 2018, 20, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Boemer, F.; Caberg, J.H.; Beckers, P.; Dideberg, V.; di Fiore, S.; Bours, V.; Marie, S.; Dewulf, J.; Marcelis, L.; Deconinck, N.; et al. Three years pilot of spinal muscular atrophy newborn screening turned into official program in Southern Belgium. Sci. Rep. 2021, 11, 19922. [Google Scholar] [CrossRef]
- Czibere, L.; Burggraf, S.; Fleige, T.; Glück, B.; Keitel, L.M.; Landt, O.; Durner, J.; Röschinger, W.; Hohenfellner, K.; Wirth, B.; et al. High-Throughput Genetic Newborn Screening for Spinal Muscular Atrophy by Rapid Nucleic Acid Extraction from Dried Blood Spots and 384-Well QPCR. Eur. J. Hum. Genet. EJHG 2020, 28, 23–30. [Google Scholar] [CrossRef]
- Kariyawasam, D.S.T.; Russell, J.S.; Wiley, V.; Alexander, I.E.; Farrar, M.A. The Implementation of Newborn Screening for Spinal Muscular Atrophy: The Australian Experience. Genet. Med. 2020, 22, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Kay, D.M.; Stevens, C.F.; Parker, A.; Saavedra-Matiz, C.A.; Sack, V.; Chung, W.K.; Chiriboga, C.A.; Engelstad, K.; Laureta, E.; Farooq, O.; et al. Implementation of Population-Based Newborn Screening Reveals Low Incidence of Spinal Muscular Atrophy. Genet. Med. 2020, 22, 1296–1302. [Google Scholar] [CrossRef] [PubMed]
- Baker, M.W.; Mochal, S.T.; Dawe, S.J.; Wiberley-Bradford, A.E.; Cogley, M.F.; Zeitler, B.R.; Piro, Z.D.; Harmelink, M.M.; Kwon, J.M. Newborn Screening for Spinal Muscular Atrophy: The Wisconsin First Year Experience. Neuromuscul. Disord. NMD 2022, 32, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.; Tokunaga, S.; Taniguchi, N.; Fujino, T.; Saito, M.; Shimomura, H.; Takeshima, Y. Views of the general population on newborn screening for spinal muscular atrophy in Japan. Children 2021, 8, 694. [Google Scholar] [CrossRef]
- Shinohara, M.; Niba, E.T.E.; Wijaya, Y.O.S.; Takayama, I.; Mitsuishi, C.; Kumasaka, S.; Kondo, Y.; Takatera, A.; Hokuto, I.; Morioka, I.; et al. SMA-NBS PILOT STUDY GROUP. A Novel System for Spinal Muscular Atrophy Screening in Newborns: Japanese Pilot Study. Int. J. Neonatal Screen. 2019, 5, 41. [Google Scholar] [CrossRef]
- Vill, K.; Schwartz, O.; Blaschek, A.; Gläser, D.; Nennstiel, U.; Wirth, B.; Burggraf, S.; Röschinger, W.; Becker, M.; Czibere, L.; et al. Newborn Screening for Spinal Muscular Atrophy in Germany: Clinical Results after 2 Years. Orphanet J. Rare Dis. 2021, 16, 153. [Google Scholar] [CrossRef]
- Gailite, L.; Sterna, O.; Konika, M.; Isakovs, A.; Isakova, J.; Micule, I.; Setlere, S.; Diriks, M.; Auzenbaha, M. New-Born Screening for Spinal Muscular Atrophy: Results of a Latvian Pilot Study. Int. J. Neonatal Screen. 2022, 8, 15. [Google Scholar] [CrossRef] [PubMed]
- D′Silva, A.M.; Kariyawasam, D.S.T.; Best, S.; Wiley, V.; Farrar, M.A.; NSW SMA NBS Study Group. Integrating Newborn Screening for Spinal Muscular Atrophy into Health Care Systems: An Australian Pilot Programme. Dev. Med. Child Neurol. 2022, 64, 625–632. [Google Scholar] [CrossRef] [PubMed]
- Kucera, K.S.; Taylor, J.L.; Robles, V.R.; Clinard, K.; Migliore, B.; Boyea, B.L.; Okoniewski, K.C.; Duparc, M.; Rehder, C.W.; Shone, S.M.; et al. A Voluntary Statewide Newborn Screening Pilot for Spinal Muscular Atrophy: Results from Early Check. Int. J. Neonatal Screen. 2021, 7, 20. [Google Scholar] [CrossRef]
- Tavares, V.L.R.; Monfardini, F.; Lourenço, N.C.V.; da Rocha, K.M.; Weinmann, K.; Pavanello, R.; Zatz, M. Newborn Screening for 5q Spinal Muscular Atrophy: Comparisons between Real-Time PCR Methodologies and Cost Estimations for Future Implementation Programs. Int. J. Neonatal Screen. 2021, 7, 53. [Google Scholar] [CrossRef] [PubMed]
- Bradford, N.K.; Edwards, R.M.; Chan, R.J. Normal Saline (0.9% Sodium Chloride) versus Heparin Intermittent Flushing for the Prevention of Occlusion in Long-term Central Venous Catheters in Infants and Children. Cochrane Database Syst. Rev. 2020, 4, CD010996. [Google Scholar]
- Tizzano, E.F.; Finkel, R.S. Spinal Muscular Atrophy: A Changing Phenotype beyond the Clinical Trials. Neuromuscul. Disord. 2017, 27, 883–889. [Google Scholar] [CrossRef]
- Sumner, C.J.; Crawford, T.O. Two Breakthrough Gene-Targeted Treatments for Spinal Muscular Atrophy: Challenges Remain. J. Clin. Investigation 2018, 128, 3219–3227. [Google Scholar] [CrossRef]
- Watihayati, M.S.; Fatemeh, H.; Marini, M.; Atif, A.B.; Zahiruddin, W.M.; Sasongko, T.H.; Tang, T.H.; Zabidi-Hussin, Z.; Nishio, H.; Zilfalil, B.A. Combination of SMN2 Copy Number and NAIP Deletion Predicts Disease Severity in Spinal Muscular Atrophy. Brain Dev. 2009, 31, 42–45. [Google Scholar] [CrossRef]
- Kariyawasam, D.S.T.; D′Silva, A.M.; Vetsch, J.; Wakefield, C.E.; Wiley, V.; Farrar, M.A. “We Needed This”: Perspectives of Parents and Healthcare Professionals Involved in a Pilot Newborn Screening Program for Spinal Muscular Atrophy. eClinicalMedicine 2021, 33, 100742. [Google Scholar] [CrossRef] [PubMed]
- Finkel, R.; Bertini, E.; Muntoni, F.; Mercuri, E. 209th ENMC International Workshop: Outcome Measures and Clinical Trial Readiness in Spinal Muscular Atrophy 7–9 November 2014, Heemskerk, The Netherlands. Neuromuscul. Disord. 2015, 25, 593–602. [Google Scholar] [CrossRef]
- Talbot, K.; Tizzano, E.F. The Clinical Landscape for SMA in a New Therapeutic Era. Gene Ther. 2017, 24, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Cuscó, I.; Bernal, S.; Blasco-Pérez, L.; Calucho, M.; Alias, L.; Fuentes-Prior, P.; Tizzano, E.F. Practical Guidelines to Manage Discordant Situations of SMN2 Copy Number in Patients with Spinal Muscular Atrophy. Neurol. Genet. 2020, 6, e530. [Google Scholar] [CrossRef]
- Kitaoka, H.; Shitara, Y.; Uchida, Y.; Kondo, U.; Omori, I. Case of Spinal Muscular Atrophy Type 0 with Mild Prognosis. Pediatr. Int. 2020, 62, 106–107. [Google Scholar] [CrossRef]
- Schwartz, O.; Kölbel, H.; Blaschek, A.; Gläser, D.; Burggraf, S.; Röschinger, W.; Schara, U.; Müller-Felber, W.; Vill, K. Spinal Muscular Atrophy-Is Newborn Screening Too Late for Children with Two SMN2 Copies? J. Neuromuscul. Dis. 2022, 9, 389–396. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| (1) Prediction of the number of SMA patients |
| Incidence studies of SMA before SMA-NBS started (Section 3.1 and Section 3.2) |
| (2) Pitfalls of SMA-NBS |
| Case studies with false-positive results (Section 3.3 and Section 3.4) |
| (3) Patients identified by SMA-NBS |
| Case reports of patients received pre-symptomatic or post-symptomatic treatment (Section 3.5 and Section 3.6) |
| Number of Patients with SMA Types I, II, III | Number of Patients with SMA Type I | ||||||
|---|---|---|---|---|---|---|---|
| Live Births | Affected Infants | Affected Fetuses | Affected Infants and Fetuses | Affected Infants | Affected Fetus | Affected Infants and Fetuses | |
| 2007 | 48,685 | 2 | 1 | 3 | 1 | 1 | 2 |
| 2008 | 48,833 | 3 | 0 | 3 | 2 | 0 | 2 |
| 2009 | 47,592 | 1 | 0 | 1 | 0 | 0 | 0 |
| 2010 | 47,834 | 2 | 0 | 2 | 1 | 0 | 1 |
| 2011 | 47,351 | 1 | 0 | 1 | 1 | 0 | 1 |
| 2012 | 46,436 | 1 | 0 | 1 | 1 | 0 | 1 |
| 2013 | 45,673 | 3 | 0 | 3 | 1 | 0 | 1 |
| 2014 | 44,352 | 3 | 3 | 6 | 1 | 2 | 3 |
| 2015 | 44,015 | 1 | 0 | 1 | 0 | 0 | 0 |
| 2016 | 43,378 | 1 | 1 | 2 | 1 | 1 | 2 |
| Total | 464,149 | 18 | 5 | 23 | 9 | 4 | 13 |
| Average | 46,415 | 1.8 | 0.5 | 2.3 | 0.9 | 0.4 | 1.3 |
| Incidence (in 100,000) | Affected infants only 3.88 [95% CI: 0.02, 7.74] | Affected infants only 1.94 [95%CI: −0.79, 4.67] | |||||
| Affected infants and fetuses 4.96 [95% CI: 0.59, 9.32] | Affected infants and fetuses 2.80 [95%CI: −0.48, 6.08] | ||||||
| Case | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| Hospital | A | B | B | B | B | B | C | B | B | B |
| Year (month) | 2021 (March) | 2021 (August) | 2021 (August) | 2021 (August) | 2021 (August) | 2021 (September) | 2021 (November) | 2022 (May) | 2022 (July) | 2022 (July) |
| Sex | male | female | male | male | female | male | female | male | male | male |
| Gestational age | 37 weeks | 40 weeks | 34 weeks | 36 weeks | 39 weeks | 38 weeks | 31 weeks | 39 weeks | 40 weeks | 41 weeks |
| Birth weight | 2188 g | 3084 g | 2840 g | 2572 g | 2620 g | 3800 g | 1588 g | 3990 g | 3372 g | 3478 g |
| Events in perinatal period | gastric mucosal lesion | none | none | apnea | none | pneumo-thorax | low birth weight | none | none | none |
| SMN1 copy number * | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| Patient 1 | Patient 2 | |
|---|---|---|
| Sex | female | female |
| Weight | 3266 g | 3120 g |
| Gestational age | 41 weeks and 5 days | 41 weeks and 2 days |
| DBS sampling | 4 days | 4 days |
| Notification of NBS results | 21 days | 17 days |
| Examination and inspection | 22 days | 18 days |
| Notification of inspection results | 24 days | 21 days |
| Events in peri-neonatal period | MAS and floppy status | healthy condition |
| Initiation of SMA treatment (First injection of nusinersen) | 25 days | 22 days |
| Gene therapy with onasemnogene abeparvovec | 19 weeks | not done |
| CHOP-INTEND score | (23 days; before treatment) 12 (13 weeks) 34 (24 weeks) 44 | (21 days; before treatment) 42 (12 weeks) 44 |
| CMAP amplitude | (33 days, median nerve) 0.08 mV | (24 days, ulnar nerve) 3.5 mV |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Noguchi, Y.; Bo, R.; Nishio, H.; Matsumoto, H.; Matsui, K.; Yano, Y.; Sugawara, M.; Ueda, G.; Wijaya, Y.O.S.; Niba, E.T.E.; et al. PCR-Based Screening of Spinal Muscular Atrophy for Newborn Infants in Hyogo Prefecture, Japan. Genes 2022, 13, 2110. https://doi.org/10.3390/genes13112110
Noguchi Y, Bo R, Nishio H, Matsumoto H, Matsui K, Yano Y, Sugawara M, Ueda G, Wijaya YOS, Niba ETE, et al. PCR-Based Screening of Spinal Muscular Atrophy for Newborn Infants in Hyogo Prefecture, Japan. Genes. 2022; 13(11):2110. https://doi.org/10.3390/genes13112110
Chicago/Turabian StyleNoguchi, Yoriko, Ryosuke Bo, Hisahide Nishio, Hisayuki Matsumoto, Keiji Matsui, Yoshihiko Yano, Masami Sugawara, Go Ueda, Yogik Onky Silvana Wijaya, Emma Tabe Eko Niba, and et al. 2022. "PCR-Based Screening of Spinal Muscular Atrophy for Newborn Infants in Hyogo Prefecture, Japan" Genes 13, no. 11: 2110. https://doi.org/10.3390/genes13112110