Viral Sequences Detection by High-Throughput Sequencing in Cerebrospinal Fluid of Individuals with and without Central Nervous System Disease

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
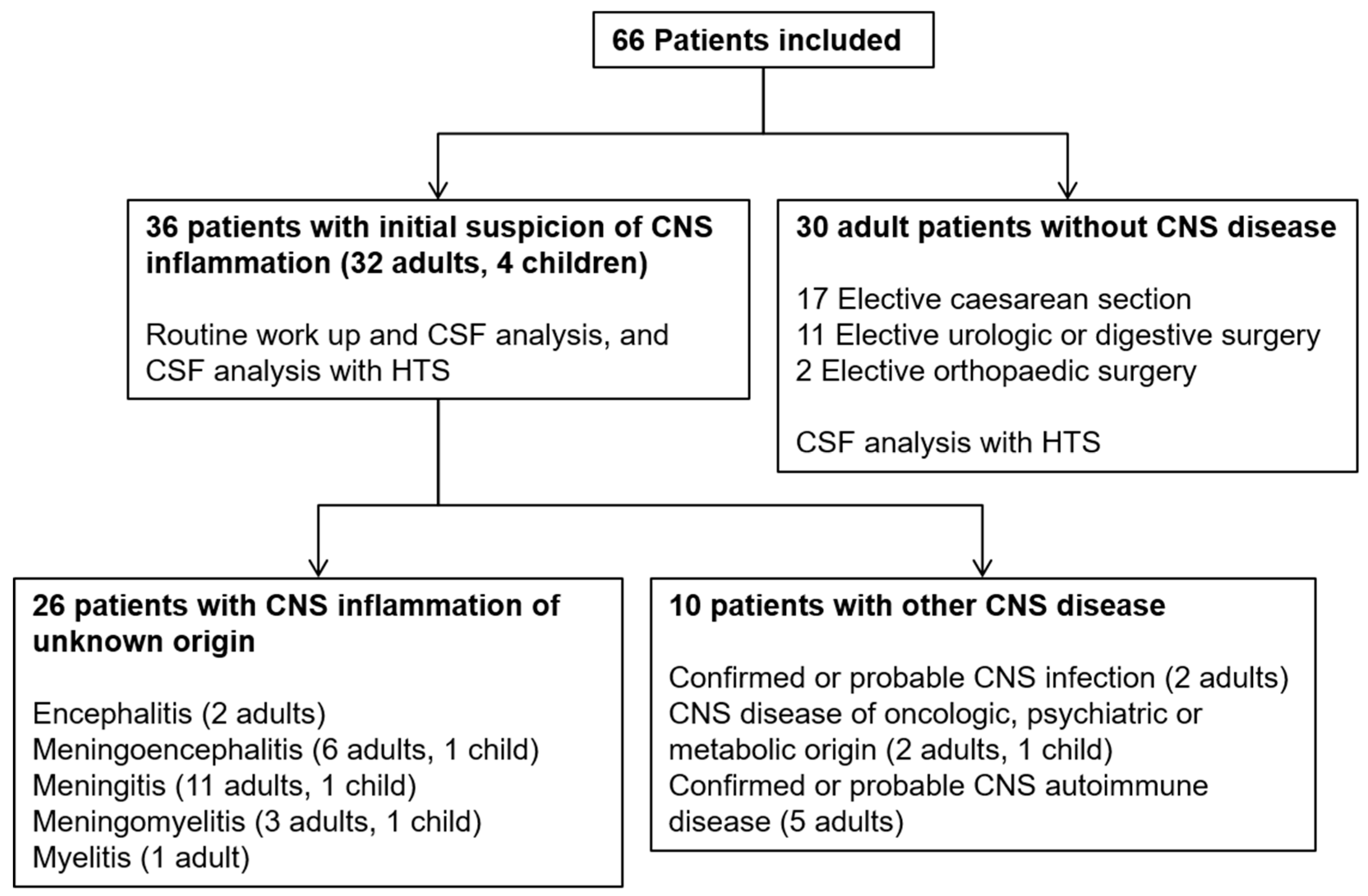
3.1. Clinical and Paraclinical Data
3.2. HTS Analysis and r(RT-)PCR Results
3.2.1. Detection of Nonsignificant Viral Sequences and Reagent Contamination
3.2.2. Sequence Cross-Contamination
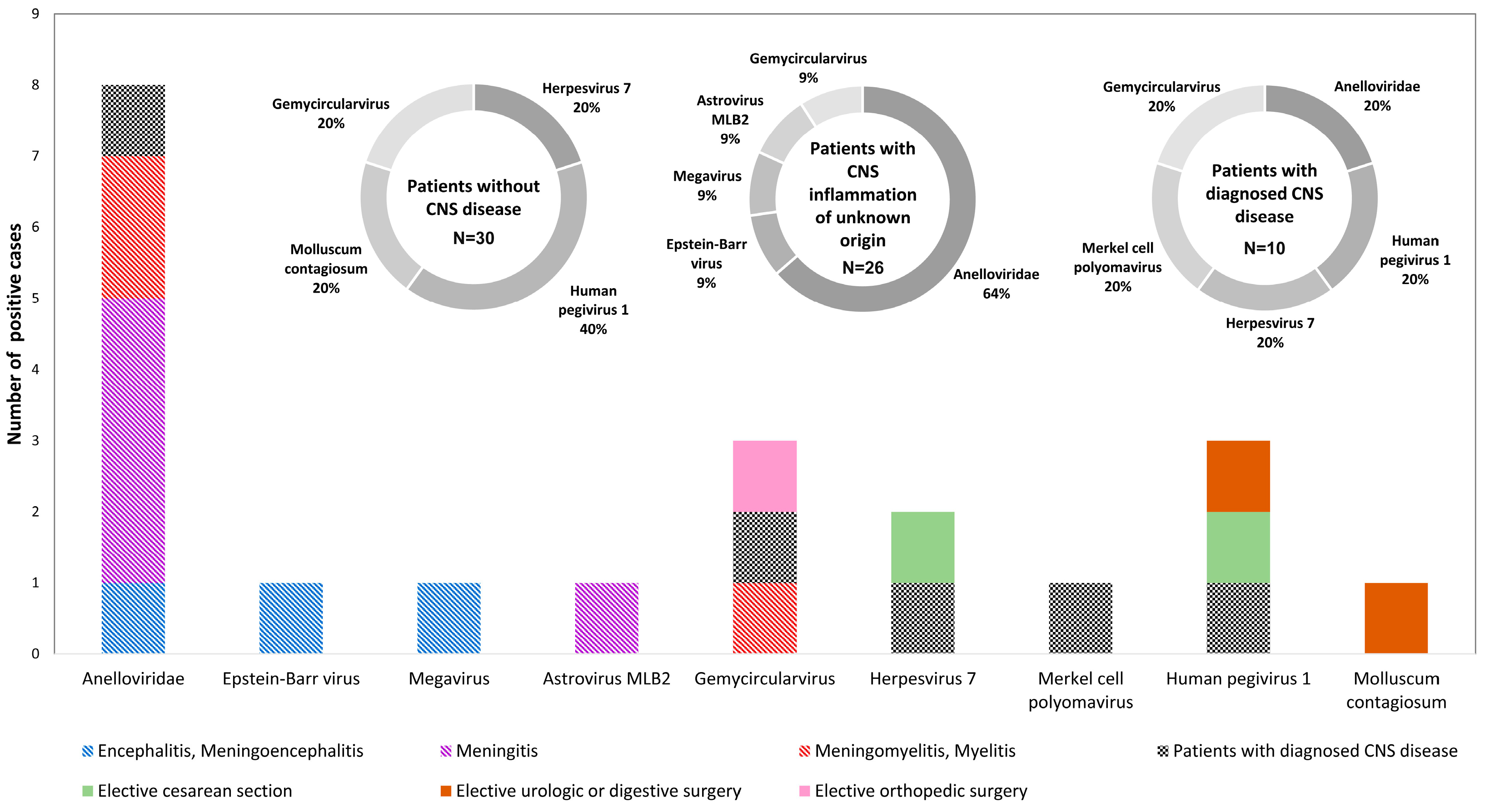
3.2.3. Viral Sequences Assigned to Pathogenic or Commensal Viruses
Control Patients
Patients with CNS Inflammation of Unknown Origin
Patients with Diagnosed CNS Disease
3.2.4. De Novo Analysis of the HTS Data
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dalmau, J.; Graus, F. Antibody-Mediated Encephalitis. N. Engl. J. Med. 2018, 378, 840–851. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Granerod, J.; Ambrose, H.E.; Davies, N.W.; Clewley, J.P.; Walsh, A.L.; Morgan, D.; Cunningham, R.; Zuckerman, M.; Mutton, K.J.; Solomon, T.; et al. Causes of encephalitis and differences in their clinical presentations in England: A multicentre, population-based prospective study. Lancet Infect. Dis. 2010, 10, 835–844. [Google Scholar] [CrossRef]
- Mailles, A.; Stahl, J.P.; Steering, C.; Investigators, G. Infectious encephalitis in france in 2007: A national prospective study. Clin. Infect. Dis. 2009, 49, 1838–1847. [Google Scholar] [CrossRef]
- Swanson, P.A., II; McGavern, D.B. Viral diseases of the central nervous system. Curr. Opin. Virol. 2015, 11, 44–54. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Boucher, A.; Herrmann, J.L.; Morand, P.; Buzele, R.; Crabol, Y.; Stahl, J.P.; Mailles, A. Epidemiology of infectious encephalitis causes in 2016. Med. Mal. Infect. 2017, 47, 221–235. [Google Scholar] [CrossRef] [PubMed]
- Mailles, A.; Stahl, J.P.; Bloch, K.C. Update and new insights in encephalitis. Clin. Microbiol. Infect. 2017, 23, 607–613. [Google Scholar] [CrossRef] [Green Version]
- Wilson, M.R.; Sample, H.A.; Zorn, K.C.; Arevalo, S.; Yu, G.; Neuhaus, J.; Federman, S.; Stryke, D.; Briggs, B.; Langelier, C.; et al. Clinical Metagenomic Sequencing for Diagnosis of Meningitis and Encephalitis. N. Engl. J. Med. 2019, 380, 2327–2340. [Google Scholar] [CrossRef] [PubMed]
- Zanella, M.C.; Lenggenhager, L.; Schrenzel, J.; Cordey, S.; Kaiser, L. High-throughput sequencing for the aetiologic identification of viral encephalitis, meningoencephalitis, and meningitis. A narrative review and clinical appraisal. Clin. Microbiol. Infect. 2019, 25, 422–430. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.Y.; Chang, Y.C.; Huang, C.C.; Lui, C.C.; Lee, K.W.; Huang, S.C. Acute flaccid paralysis in infants and young children with enterovirus 71 infection: MR imaging findings and clinical correlates. Am. J. Neuroradiol. 2001, 22, 200–205. [Google Scholar] [PubMed]
- Kraushaar, G.; Patel, R.; Stoneham, G.W. West Nile Virus: A case report with flaccid paralysis and cervical spinal cord: MR imaging findings. Am. J. Neuroradiol. 2005, 26, 26–29. [Google Scholar] [PubMed]
- Venkatesan, A.; Tunkel, A.R.; Bloch, K.C.; Lauring, A.S.; Sejvar, J.; Bitnun, A.; Stahl, J.P.; Mailles, A.; Drebot, M.; Rupprecht, C.E.; et al. Case definitions, diagnostic algorithms, and priorities in encephalitis: Consensus statement of the international encephalitis consortium. Clin. Infect. Dis. 2013, 57, 1114–1128. [Google Scholar] [CrossRef] [PubMed]
- Leber, A.L.; Everhart, K.; Balada-Llasat, J.M.; Cullison, J.; Daly, J.; Holt, S.; Lephart, P.; Salimnia, H.; Schreckenberger, P.C.; DesJarlais, S.; et al. Multicenter Evaluation of BioFire FilmArray Meningitis/Encephalitis Panel for Detection of Bacteria, Viruses, and Yeast in Cerebrospinal Fluid Specimens. J. Clin. Microbiol. 2016, 54, 2251–2261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petty, T.J.; Cordey, S.; Padioleau, I.; Docquier, M.; Turin, L.; Preynat-Seauve, O.; Zdobnov, E.M.; Kaiser, L. Comprehensive human virus screening using high-throughput sequencing with a user-friendly representation of bioinformatics analysis: A pilot study. J. Clin. Microbiol. 2014, 52, 3351–3361. [Google Scholar] [CrossRef]
- Wright, E.S.; Vetsigian, K.H. Quality filtering of Illumina index reads mitigates sample cross-talk. BMC Genom. 2016, 17, 876. [Google Scholar] [CrossRef] [PubMed]
- Peng, Y.; Leung, H.C.; Yiu, S.M.; Chin, F.Y. IDBA-UD: A de novo assembler for single-cell and metagenomic sequencing data with highly uneven depth. Bioinformatics 2012, 28, 1420–1428. [Google Scholar] [CrossRef] [PubMed]
- Arvia, R.; Sollai, M.; Pierucci, F.; Urso, C.; Massi, D.; Zakrzewska, K. Droplet digital PCR (ddPCR) vs quantitative real-time PCR (qPCR) approach for detection and quantification of Merkel cell polyomavirus (MCPyV) DNA in formalin fixed paraffin embedded (FFPE) cutaneous biopsies. J. Virol. Methods 2017, 246, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Chivero, E.T.; Bhattarai, N.; Rydze, R.T.; Winters, M.A.; Holodniy, M.; Stapleton, J.T. Human pegivirus RNA is found in multiple blood mononuclear cells in vivo and serum-derived viral RNA-containing particles are infectious in vitro. J. Gen. Virol. 2014, 95, 1307–1319. [Google Scholar] [CrossRef] [PubMed]
- Kimura, H.; Morita, M.; Yabuta, Y.; Kuzushima, K.; Kato, K.; Kojima, S.; Matsuyama, T.; Morishima, T. Quantitative analysis of Epstein-Barr virus load by using a real-time PCR assay. J. Clin. Microbiol. 1999, 37, 132–136. [Google Scholar] [PubMed]
- Masouridi-Levrat, S.; Pradier, A.; Simonetta, F.; Kaiser, L.; Chalandon, Y.; Roosnek, E. Torque teno virus in patients undergoing allogeneic hematopoietic stem cell transplantation for hematological malignancies. Bone Marrow Transplant. 2016, 51, 440–442. [Google Scholar] [CrossRef]
- Verheyen, J.; Timmen-Wego, M.; Laudien, R.; Boussaad, I.; Sen, S.; Koc, A.; Uesbeck, A.; Mazou, F.; Pfister, H. Detection of adenoviruses and rotaviruses in drinking water sources used in rural areas of Benin, West Africa. Appl. Environ. Microbiol. 2009, 75, 2798–2801. [Google Scholar] [CrossRef]
- Cordey, S.; Vu, D.L.; Schibler, M.; L’Huillier, A.G.; Brito, F.; Docquier, M.; Posfay-Barbe, K.M.; Petty, T.J.; Turin, L.; Zdobnov, E.M.; et al. Astrovirus MLB2, a New Gastroenteric Virus Associated with Meningitis and Disseminated Infection. Emerg. Infect. Dis. 2016, 22, 846–853. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kriesel, J.D.; Hobbs, M.R.; Jones, B.B.; Milash, B.; Nagra, R.M.; Fischer, K.F. Deep sequencing for the detection of virus-like sequences in the brains of patients with multiple sclerosis: Detection of GBV-C in human brain. PLoS ONE 2012, 7, e31886. [Google Scholar] [CrossRef] [PubMed]
- Liu, Z.; Zhang, Y.; Wei, F.; Xu, M.; Mou, D.; Zhang, T.; Li, W.; Chen, D.; Wu, H. Detection of GB virus C genomic sequence in the cerebrospinal fluid of a HIV-infected patient in China: A case report and literature review. Epidemiol. Infect. 2016, 144, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Hardie, D.; Smuts, H. Human pegivirus-1 in the CSF of patients with HIV-associated neurocognitive disorder (HAND) may be derived from blood in highly viraemic patients. J. Clin. Virol. 2017, 91, 58–61. [Google Scholar] [CrossRef] [PubMed]
- Maggi, F.; Fornai, C.; Vatteroni, M.L.; Siciliano, G.; Menichetti, F.; Tascini, C.; Specter, S.; Pistello, M.; Bendinelli, M. Low prevalence of TT virus in the cerebrospinal fluid of viremic patients with central nervous system disorders. J. Med. Virol. 2001, 65, 418–422. [Google Scholar] [CrossRef] [PubMed]
- Pollicino, T.; Raffa, G.; Squadrito, G.; Costantino, L.; Cacciola, I.; Brancatelli, S.; Alafaci, C.; Florio, M.G.; Raimondo, G. TT virus has a ubiquitous diffusion in human body tissues: Analyses of paired serum and tissue samples. J. Viral Hepat. 2003, 10, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Zhang, S.; Gong, Q.; Hao, A. A novel gemycircularvirus in an unexplained case of child encephalitis. Virol. J. 2015, 12, 197. [Google Scholar] [CrossRef]
- Maggi, F.; Fornai, C.; Zaccaro, L.; Morrica, A.; Vatteroni, M.L.; Isola, P.; Marchi, S.; Ricchiuti, A.; Pistello, M.; Bendinelli, M. TT virus (TTV) loads associated with different peripheral blood cell types and evidence for TTV replication in activated mononuclear cells. J. Med. Virol. 2001, 64, 190–194. [Google Scholar] [CrossRef]
- Desai, M.; Pal, R.; Deshmukh, R.; Banker, D. Replication of TT virus in hepatocyte and leucocyte cell lines. J. Med. Virol. 2005, 77, 136–143. [Google Scholar] [CrossRef]
- Maggi, F.; Bendinelli, M. Human anelloviruses and the central nervous system. Rev. Med. Virol. 2010, 20, 392–407. [Google Scholar] [CrossRef]
- Phan, T.G.; Mori, D.; Deng, X.; Rajindrajith, S.; Ranawaka, U.; Fan Ng, T.F.; Bucardo-Rivera, F.; Orlandi, P.; Ahmed, K.; Delwart, E. Small circular single stranded DNA viral genomes in unexplained cases of human encephalitis, diarrhea, and in untreated sewage. Virology 2015, 482, 98–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamberto, I.; Gunst, K.; Muller, H.; Zur Hausen, H.; de Villiers, E.M. Mycovirus-like DNA virus sequences from cattle serum and human brain and serum samples from multiple sclerosis patients. Genome Announc. 2014, 2. [Google Scholar] [CrossRef] [PubMed]
- Asplund, M.; Kjartansdottir, K.R.; Mollerup, S.; Vinner, L.; Fridholm, H.; Herrera, J.A.R.; Friis-Nielsen, J.; Hansen, T.A.; Jensen, R.H.; Nielsen, I.B.; et al. Contaminating viral sequences in high-throughput sequencing viromics: A linkage study of 700 sequencing libraries. Clin. Microbiol. Infect. 2019. [Google Scholar] [CrossRef]
- Sadeghi, F.; Salehi-Vaziri, M.; Alizadeh, A.; Ghodsi, S.M.; Bokharaei-Salim, F.; Fateh, A.; Monavari, S.H.; Keyvani, H. Detection of Merkel cell polyomavirus large T-antigen sequences in human central nervous system tumors. J. Med. Virol. 2015, 87, 1241–1247. [Google Scholar] [CrossRef] [PubMed]
- Lam, W.Y.; Leung, B.W.; Chu, I.M.; Chan, A.C.; Ng, H.K.; Chan, P.K. Survey for the presence of BK, JC, KI, WU and Merkel cell polyomaviruses in human brain tissues. J. Clin. Virol. 2010, 48, 11–14. [Google Scholar] [CrossRef] [PubMed]
- Giraud, G.; Ramqvist, T.; Pastrana, D.V.; Pavot, V.; Lindau, C.; Kogner, P.; Orrego, A.; Buck, C.B.; Allander, T.; Holm, S.; et al. DNA from KI, WU and Merkel cell polyomaviruses is not detected in childhood central nervous system tumours or neuroblastomas. PLoS ONE 2009, 4, e8239. [Google Scholar] [CrossRef] [PubMed]
- Cordey, S.; Bel, M.; Petty, T.J.; Docquier, M.; Sacco, L.; Turin, L.; Cherpillod, P.; Emonet, S.; Louis-Simonet, M.; Zdobnov, E.M.; et al. Toscana virus meningitis case in Switzerland: An example of the ezVIR bioinformatics pipeline utility for the identification of emerging viruses. Clin. Microbiol. Infect. 2015, 21, 387.e1–387.e4. [Google Scholar] [CrossRef] [PubMed]
- Cordey, S.; Hartley, M.A.; Keitel, K.; Laubscher, F.; Brito, F.; Junier, T.; Kagoro, F.; Samaka, J.; Masimba, J.; Said, Z.; et al. Detection of novel astroviruses MLB1 and MLB2 in the sera of febrile Tanzanian children. Emerg. Microbes Infect. 2018, 7, 1–3. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, S.H.; Cordey, S.; Bhuva, N.; Laubscher, F.; Hartley, M.A.; Boillat-Blanco, N.; Mbarack, Z.; Samaka, J.; Mlaganile, T.; Jain, K.; et al. Investigation of the Plasma Virome from Cases of Unexplained Febrile Illness in Tanzania from 2013 to 2014: A Comparative Analysis between Unbiased and VirCapSeq-VERT High-Throughput Sequencing Approaches. mSphere 2018, 3. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Encephalitis and Meningo-Encephalitis | Meningitis | Myelitis and Meningomyelitis |
|---|---|---|
| Major criteria (required) Altered mental status (defined as decreased or altered level of consciousness, lethargy or personality change) lasting ≥24 hours with no alternative cause identified Minor criteria (2 required for possible encephalitis, ≥3 required for probable, or confirmed encephalitis)
| ≥2 following criteria
AND CSF leukocyte count ≥5 M/L | Major criteria (≥1 required)
Minor criteria (optional)
|
| All | CNS Inflammation of Unknown Origin | Diagnosed CNS Disease | |
|---|---|---|---|
| Number (%) | 36 (100) | 26 (72.2) | 10 (27.8) |
| Male | 22 (61.1) | 16 (61.5) | 6 (60) |
| Mean age, years (SD) | 41.6 (18.5) | 38.7 (18.5) | 49.2 (17.1) |
| <18 years old (%) | 4 (11.1) | 3 (11.5) | 1 (10.0) |
| All | Urologic or Digestive Surgery | Orthopaedic Surgery | Caesarean Section | |
|---|---|---|---|---|
| Number (%) | 30 (100) | 11 (36.6) | 2 (6.7) | 17 (56.7) |
| Male | 9 (30) | 9 (81.8) | 0 | 0 |
| Mean age, years (SD) | 53.4 (22.5) | 77.4 (7.5) | 81 (1.4) | 34.7 (4.1) |
| All (N = 26) | Encephalitis and Meningo-encephalitis (n = 9) | Meningitis (n = 12) | Myelitis and Meningo-myelitis (n = 5) | |
|---|---|---|---|---|
| Clinical features, n (%) | ||||
| Headache | 19 (73.1) | 5 (55.6) | 11 (91.7) | 3 (60.0) |
| Neck stiffness | 3 (11.5) | 2 (22.2) | 1 (8.3) | 0 |
| Fever (≥38,2 °C) *1 | 13 (50.0) | 3 (33.3) | 7 (58.3) | 3 (60.0) |
| Nausea/vomiting | 2(7.7) | 0 | 2 (16.7) | 0 |
| Photophobia | 8 (30.8) | 2 (22.2) | 5 (41.6) | 1 (20.0) |
| Phonophobia | 4 (15.4) | 0 | 3 (25.0) | 1 (20.0) |
| Altered mental status *2 | 8 (30.8) | 8 (88.9) | 0 | 0 |
| Seizure | 2 (7.7) | 2 (22.2) | 0 | 0 |
| Suggestive abnormality on neuroimaging | 13 (50.0) | 5 (55.5) | 4 (33.3) | 4 (80.0) |
| Suggestive abnormality on EEG *3 | 8 (30.8) | 7 (77.8) | 1 (8.3) | 0 |
| Sensory or motor focal neurologic deficit | 9 (34.6) | 0 | 4 (33.3) | 5 (100.0) |
| Requiring intensive care | 4 (15.4) | 2 (22.2) | 0 | 2 (40.0) |
| Requiring immunosuppressive therapy | 6 (23.1) | 1 (11.1) | 1 (8.3) | 4 (80.0) |
| Clinical outcome *4 | ||||
| Complete resolution of signs and symptoms | 16 (61.5) | 3 (33.3) | 11 (91.6) | 2 (40.0) |
| Death | 0 | 0 | 0 | 0 |
| Laboratory features | ||||
| Cerebrospinal fluid | ||||
| WBC *5 count ≥ 5 M/L (%) | 26 (100.0) | 9 (100.0) | 12 (100.0) | 5 (100) |
| Median WBC count, M/L (range) | 76 (6–3706) | 53 (18–72) | 75(6–3706) | 161 (50–275) |
| Median glycorachia, mmol/L (range) (2.8–4.0 mmol/L) | 3.1 (2.5–5.4) | 3.2 (2.7–5.4) | 3.2 (2.7–4.5) | 2.8 (2.5–4.4) |
| Median proteinorachia (g/L) (range) (0.15–0.45 g/L) | 0.61 (0.24–2.32) | 0.7 (0.37–2.32) | 0.61 (0.24–2.27) | 0.53 (0.40–1.58) |
| Proteinorachia > 0.45 (%) | 21 (80.8) | 8 (88.9) | 9 (75.0) | 3 (60.0) |
| Proteinorachia < 0.15 (%) | 0 | 0 | 0 | 0 |
| Blood | ||||
| Median C-reactive protein mg/L, (range) (0–10 mg/L) *6 | 4.3 (0.0–266.1) | 1.7 (0.0–80.8) | 4.8 (1.6–266.1) | 18.1 (7.7–33.7) |
| Median Leucocytes G/L,(range) (4–11 G/L) *6 | 10.0 (3.9–25.1) | 7.4 (3.9–13.9) | 10.9 (4.9–25.1) | 14.4 (6.9–15.1) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schibler, M.; Brito, F.; Zanella, M.-C.; Zdobnov, E.M.; Laubscher, F.; L’Huillier, A.G.; Ambrosioni, J.; Wagner, N.; Posfay-Barbe, K.M.; Docquier, M.; et al. Viral Sequences Detection by High-Throughput Sequencing in Cerebrospinal Fluid of Individuals with and without Central Nervous System Disease. Genes 2019, 10, 625. https://doi.org/10.3390/genes10080625
Schibler M, Brito F, Zanella M-C, Zdobnov EM, Laubscher F, L’Huillier AG, Ambrosioni J, Wagner N, Posfay-Barbe KM, Docquier M, et al. Viral Sequences Detection by High-Throughput Sequencing in Cerebrospinal Fluid of Individuals with and without Central Nervous System Disease. Genes. 2019; 10(8):625. https://doi.org/10.3390/genes10080625
Chicago/Turabian StyleSchibler, Manuel, Francisco Brito, Marie-Céline Zanella, Evgeny M. Zdobnov, Florian Laubscher, Arnaud G L’Huillier, Juan Ambrosioni, Noémie Wagner, Klara M Posfay-Barbe, Mylène Docquier, and et al. 2019. "Viral Sequences Detection by High-Throughput Sequencing in Cerebrospinal Fluid of Individuals with and without Central Nervous System Disease" Genes 10, no. 8: 625. https://doi.org/10.3390/genes10080625