
Synergistic Hepatoprotective Effects of Mesenchymal Stem Cells and Platelet-Rich Plasma in a Rat Model of Bile Duct Ligation-Induced Liver Cirrhosis

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Experimental Animals
2.2. Isolation, Culture, and Characterisation of ADMSCs
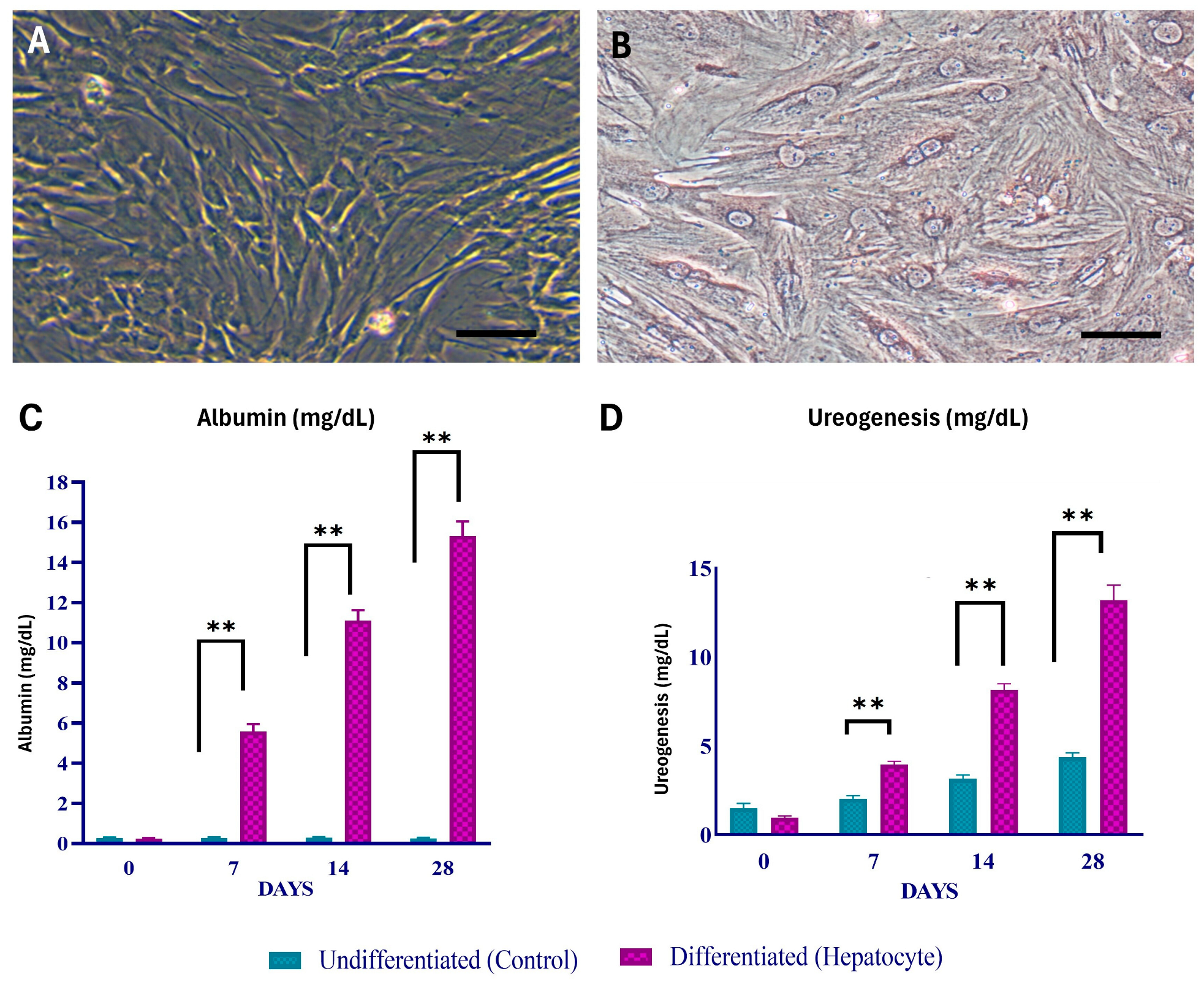
2.3. Hepatogenic Differentiation and Characterisation
2.4. Preparation and Characterisation of Platelet-Rich Plasma
2.5. Surgical Techniques of Bile-Induced Cholestasis
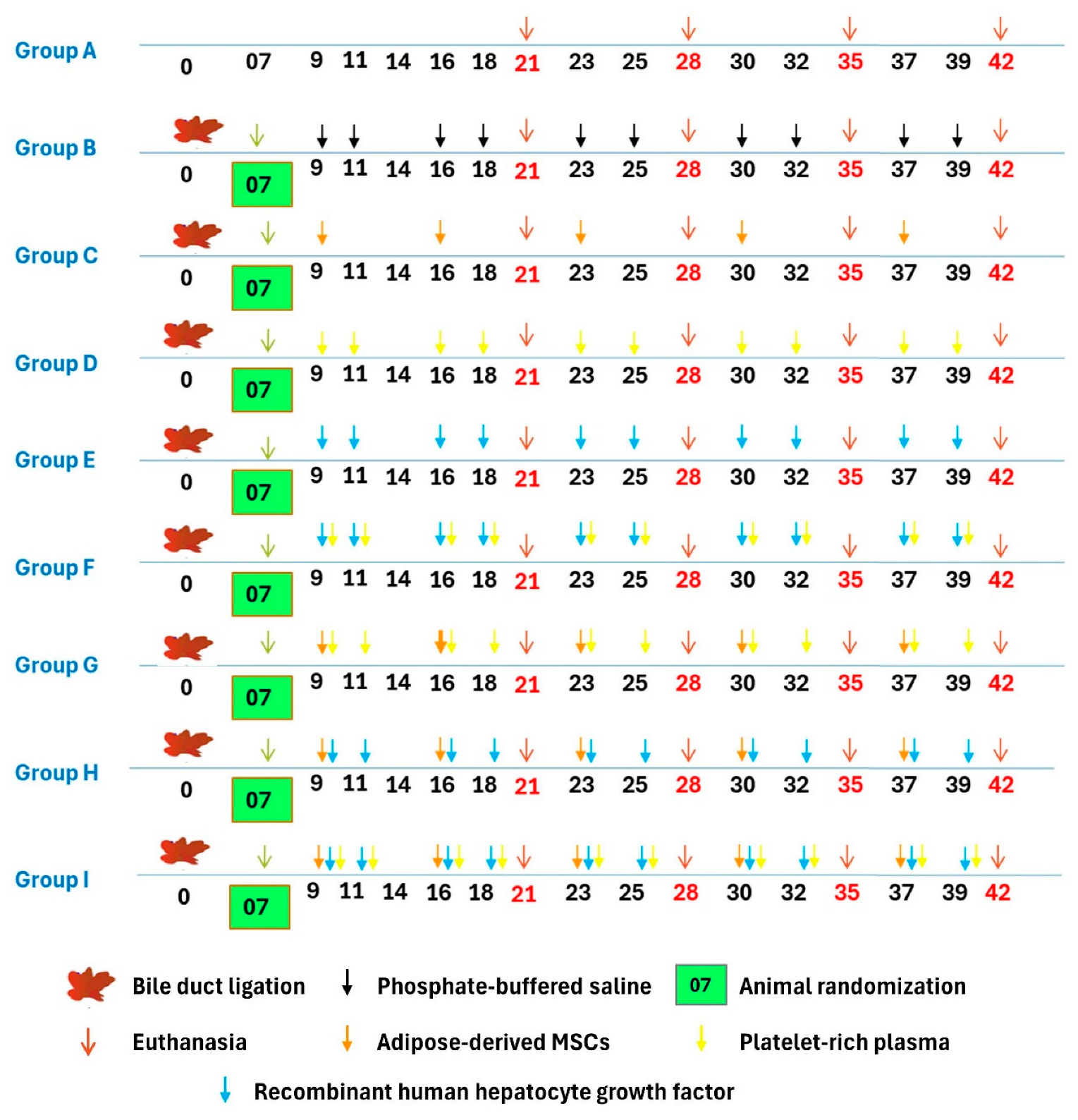
2.6. Experimental Design
2.7. Clinical Signs and Body Weight
2.8. Biochemical Liver Function Analysis
2.9. Morphology and Histopathological Examination
2.10. Colour Digital Imaging
2.11. Immunohistochemistry (IHC)
2.12. Tracking of Transplanted Cells
2.13. Statistical Analysis
3. Result
3.1. Isolation, Culture, and Characterisation of ADMSCs
3.2. Characterisation of PRP
3.3. In Vivo Trial for Evaluation of the Hepatoprotective Effect of Rat ADMSC, PRP, and rh-HGF on Obstructive Cholestasis-Induced Liver Cirrhosis/Fibrosis
3.4. Clinical Observations
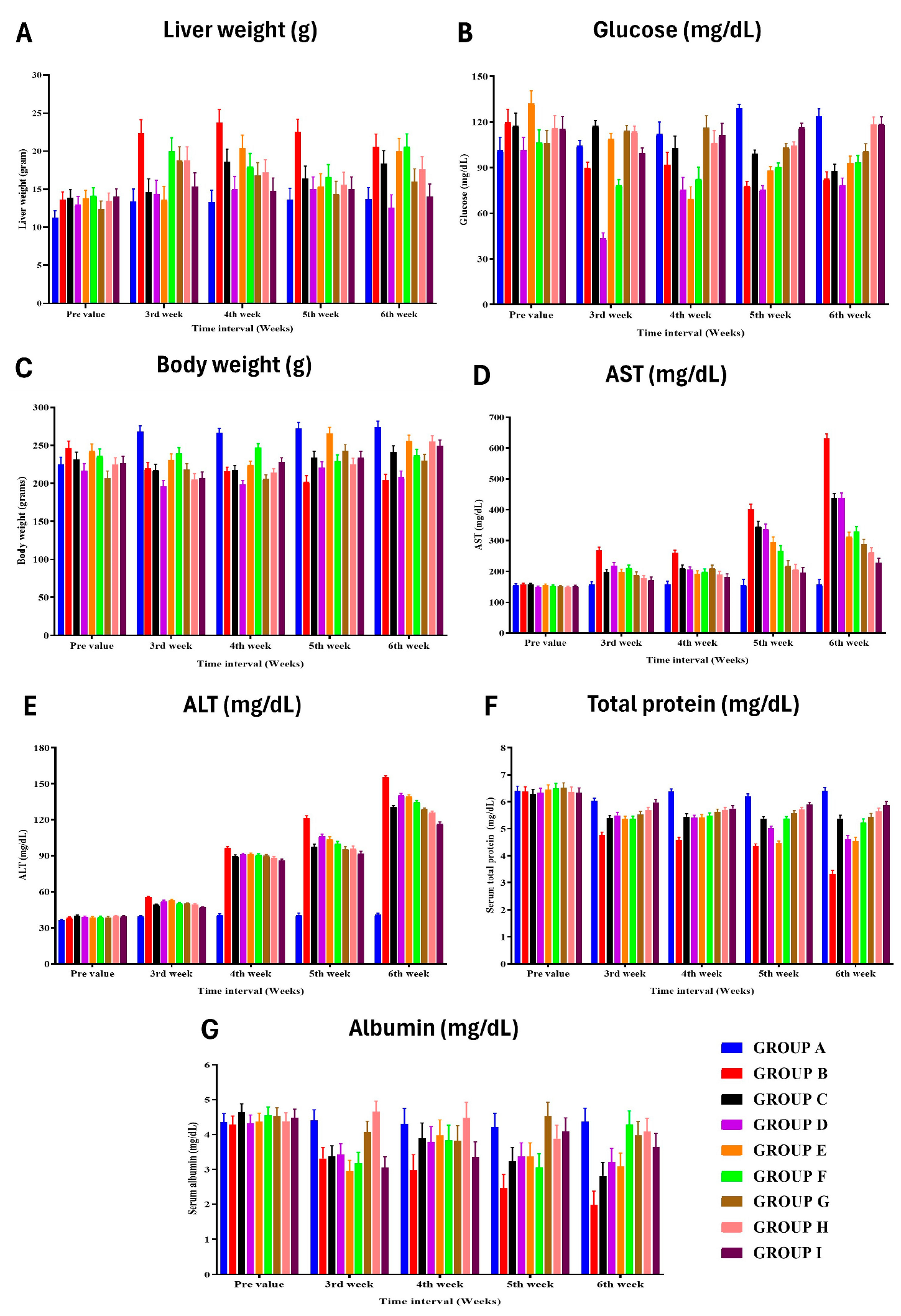
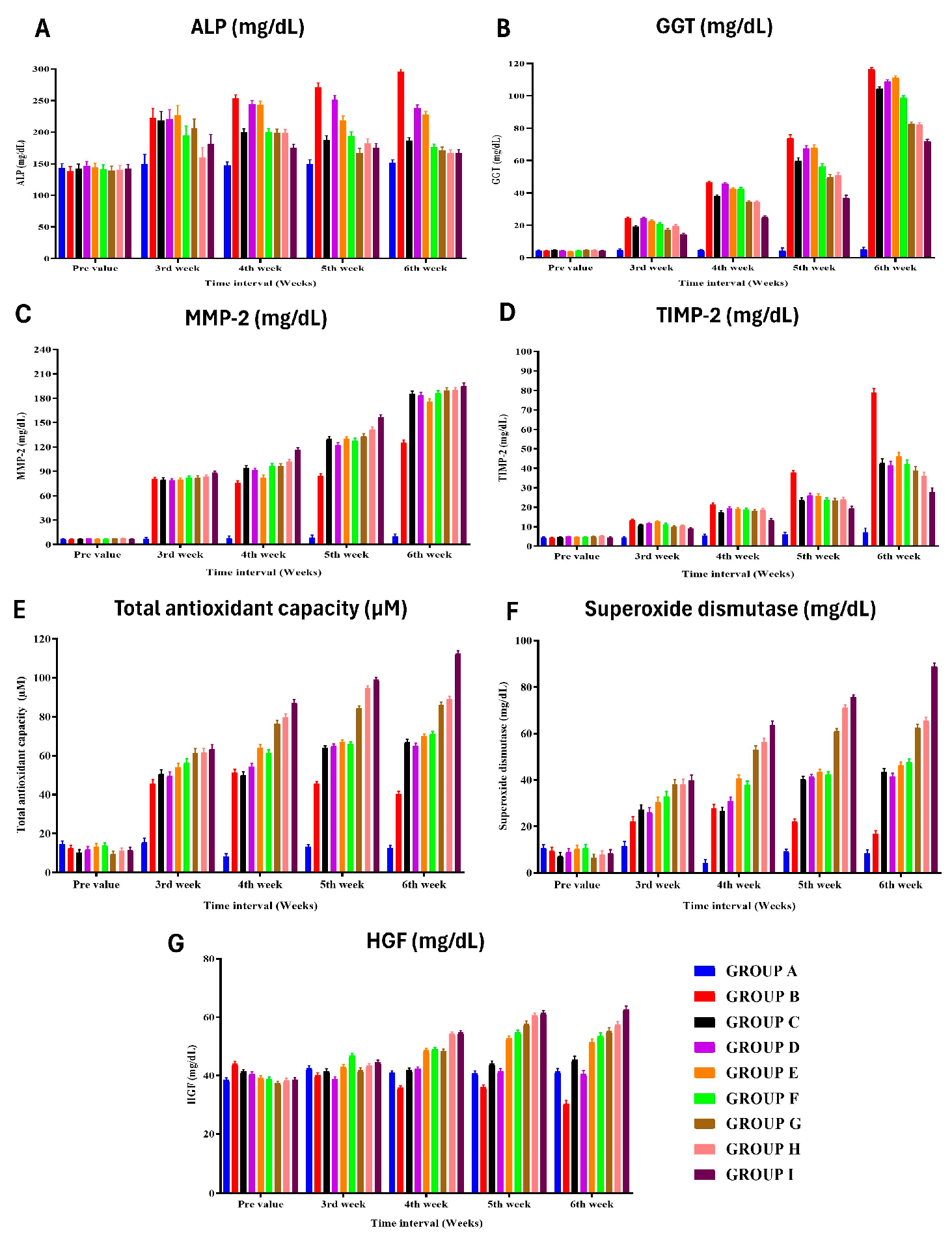
3.5. Biochemical Liver Function Analysis
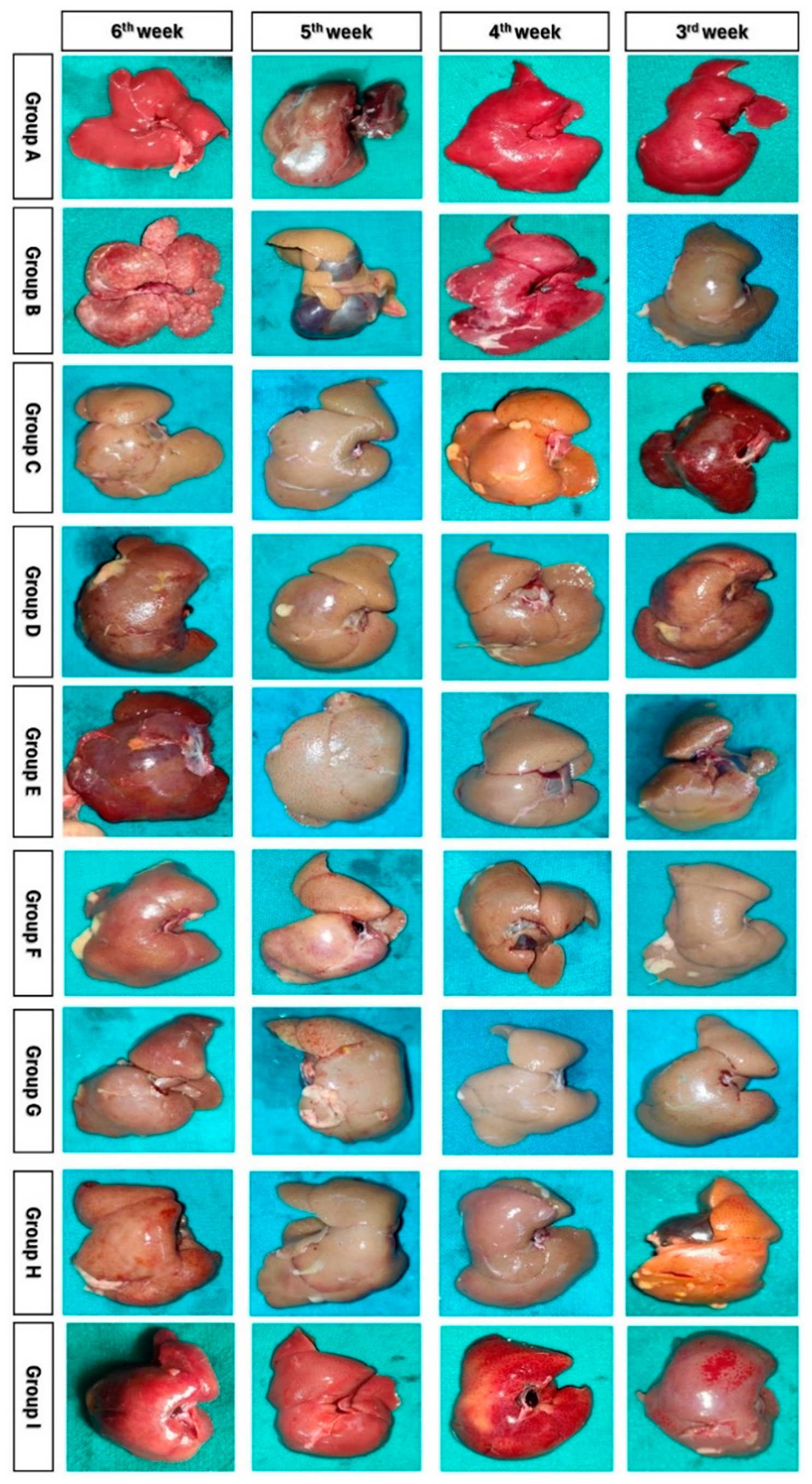
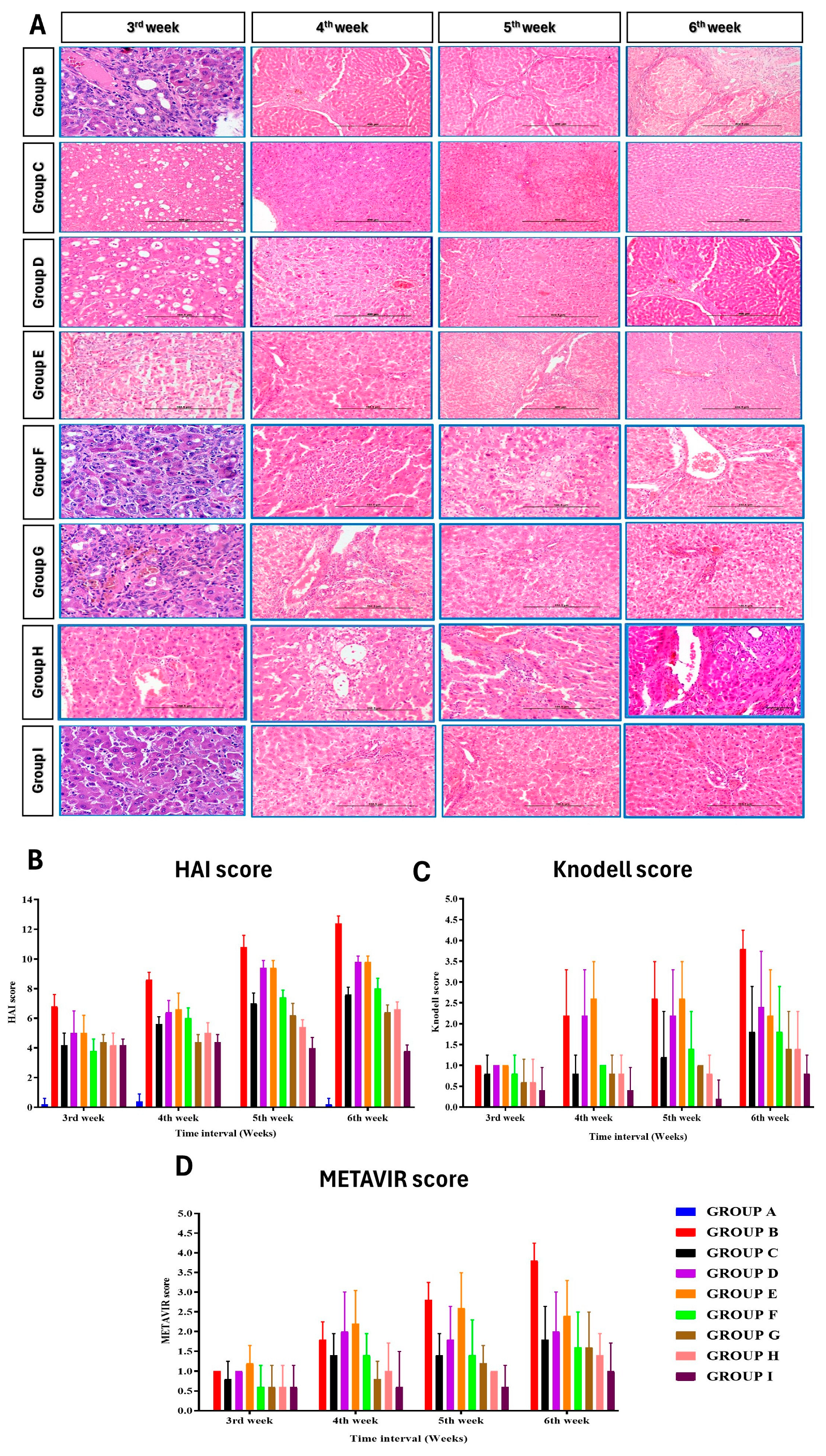
3.6. Histopathological Observations
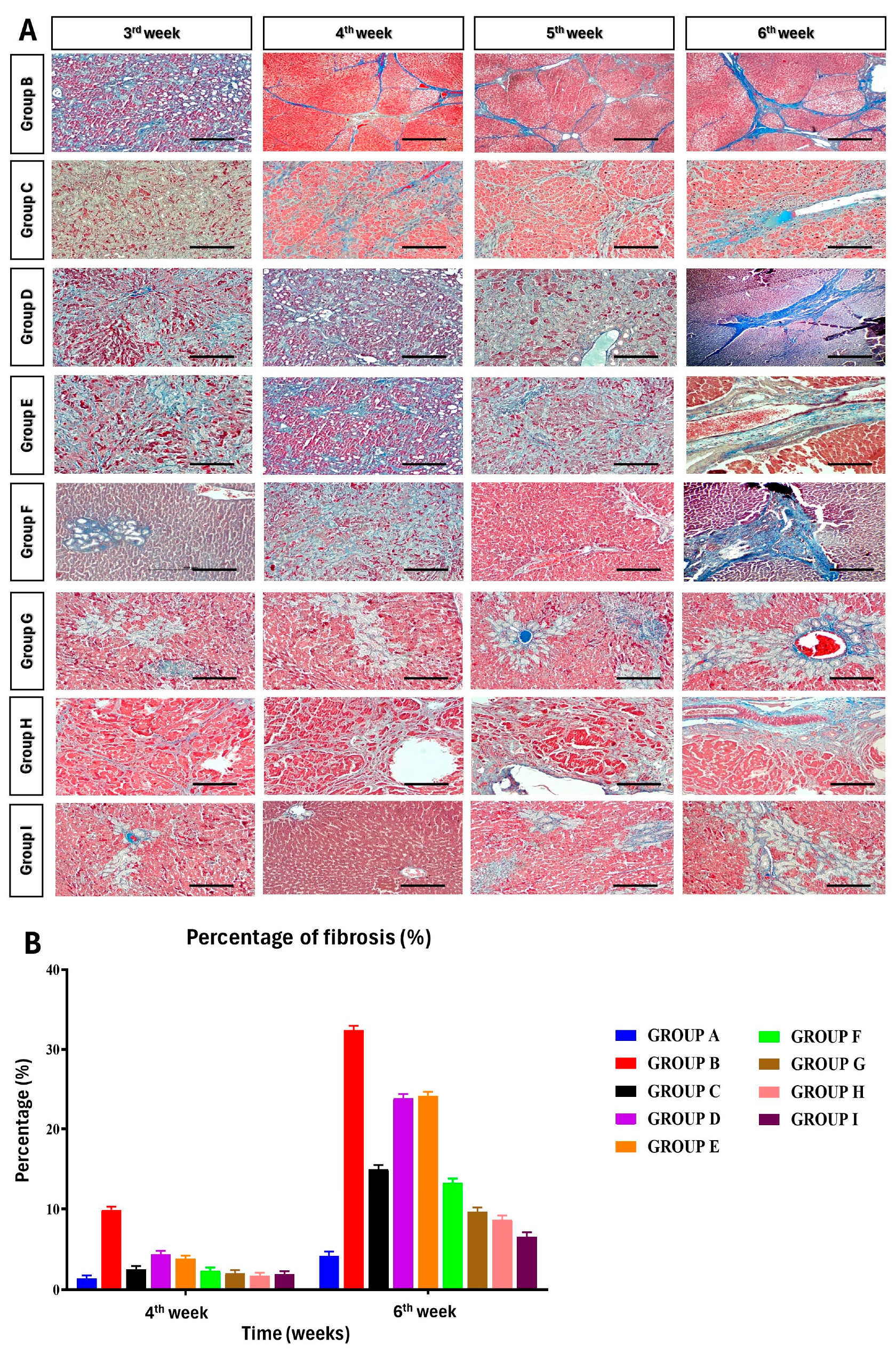
3.7. Percentage of Fibrosis
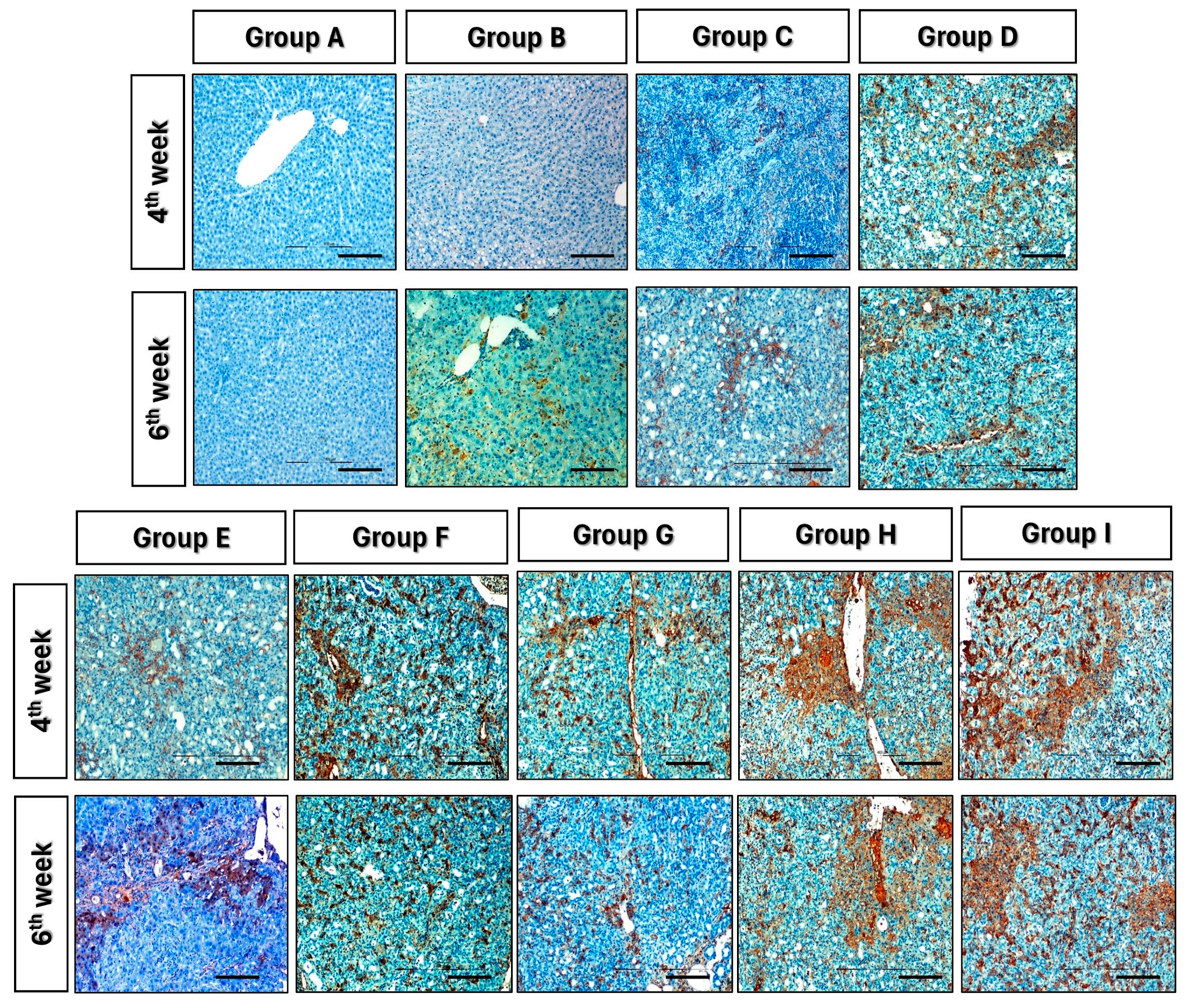
3.8. Immunohistochemistry
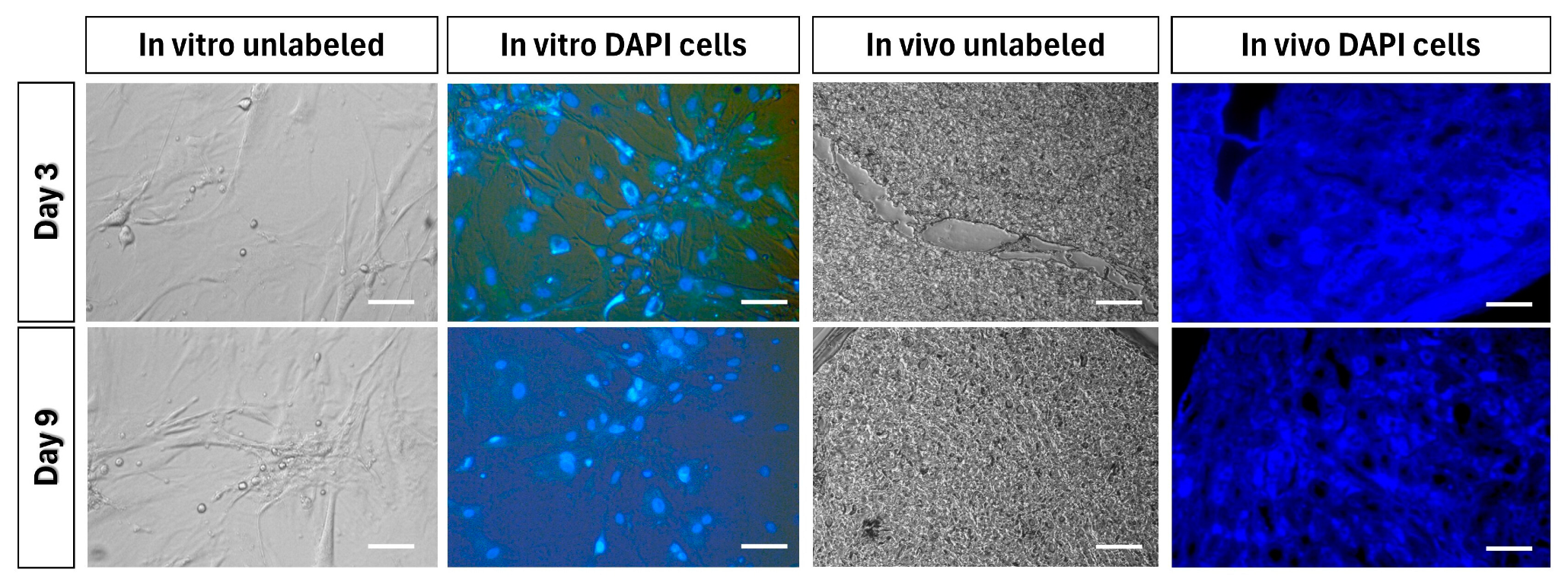
3.9. Tracking of Transplanted Cells
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Piryaei, A.; Valojerdi, M.R.; Shahsavani, M.; Baharvand, H. Differentiation of Bone Marrow-Derived Mesenchymal Stem Cells into Hepatocyte-like Cells on Nanofibers and Their Transplantation into a Carbon Tetrachloride-Induced Liver Fibrosis Model. Stem Cell Rev. Rep. 2011, 7, 103–118. [Google Scholar] [CrossRef] [PubMed]
- Alshawsh, M.A.; Abdulla, M.A.; Ismail, S.; Amin, Z.A. Hepatoprotective Effects of Orthosiphon Stamineus Extract on Thioacetamide-Induced Liver Cirrhosis in Rats. Evid.-Based Complement. Altern. Med. ECAM 2011, 2011, 103039. [Google Scholar] [CrossRef] [PubMed]
- Friedman, S.L. Liver Fibrosis—From Bench to Bedside. J. Hepatol. 2003, 38 (Suppl. S1), S38–S53. [Google Scholar] [CrossRef] [PubMed]
- Arriazu, E.; Ruiz de Galarreta, M.; Cubero, F.J.; Varela-Rey, M.; Pérez de Obanos, M.P.; Leung, T.M.; Lopategi, A.; Benedicto, A.; Abraham-Enachescu, I.; Nieto, N. Extracellular Matrix and Liver Disease. Antioxid. Redox Signal. 2014, 21, 1078–1097. [Google Scholar] [CrossRef]
- Poynard, T.; Mathurin, P.; Lai, C.-L.; Guyader, D.; Poupon, R.; Tainturier, M.-H.; Myers, R.P.; Muntenau, M.; Ratziu, V.; Manns, M.; et al. A Comparison of Fibrosis Progression in Chronic Liver Diseases. J. Hepatol. 2003, 38, 257–265. [Google Scholar] [CrossRef]
- Dai, L.-J.; Li, H.Y.; Guan, L.-X.; Ritchie, G.; Zhou, J.X. The Therapeutic Potential of Bone Marrow-Derived Mesenchymal Stem Cells on Hepatic Cirrhosis. Stem Cell Res. 2009, 2, 16–25. [Google Scholar] [CrossRef] [PubMed]
- Nadri, S.; Soleimani, M.; Hosseni, R.H.; Massumi, M.; Atashi, A.; Izadpanah, R. An Efficient Method for Isolation of Murine Bone Marrow Mesenchymal Stem Cells. Int. J. Dev. Biol. 2007, 51, 723–729. [Google Scholar] [CrossRef]
- Abdel Aziz, M.T.; Atta, H.M.; Mahfouz, S.; Fouad, H.H.; Roshdy, N.K.; Ahmed, H.H.; Rashed, L.A.; Sabry, D.; Hassouna, A.A.; Hasan, N.M. Therapeutic Potential of Bone Marrow-Derived Mesenchymal Stem Cells on Experimental Liver Fibrosis. Clin. Biochem. 2007, 40, 893–899. [Google Scholar] [CrossRef]
- Watt, F.M.; Hogan, B.L. Out of Eden: Stem Cells and Their Niches. Science 2000, 287, 1427–1430. [Google Scholar] [CrossRef]
- Snykers, S.; De Kock, J.; Tamara, V.; Rogiers, V. Hepatic Differentiation of Mesenchymal Stem Cells: In Vitro Strategies. Methods Mol. Biol. 2011, 698, 305–314. [Google Scholar] [CrossRef]
- Berardis, S.; Lombard, C.; Evraerts, J.; El Taghdouini, A.; Rosseels, V.; Sancho-Bru, P.; Lozano, J.J.; van Grunsven, L.; Sokal, E.; Najimi, M. Gene Expression Profiling and Secretome Analysis Differentiate Adult-Derived Human Liver Stem/Progenitor Cells and Human Hepatic Stellate Cells. PLoS ONE 2014, 9, e86137. [Google Scholar] [CrossRef] [PubMed]
- Sarvandi, S.S.; Joghataei, M.T.; Parivar, K.; Khosravi, M.; Sarveazad, A.; Sanadgol, N. In Vitro Differentiation of Rat Mesenchymal Stem Cells to Hepatocyte Lineage. Iran. J. Basic Med. Sci. 2015, 18, 89–97. [Google Scholar] [PubMed]
- Kern, S.; Eichler, H.; Stoeve, J.; Klüter, H.; Bieback, K. Comparative Analysis of Mesenchymal Stem Cells from Bone Marrow, Umbilical Cord Blood, or Adipose Tissue. Stem Cells 2006, 24, 1294–1301. [Google Scholar] [CrossRef] [PubMed]
- De Pascale, M.R.; Sommese, L.; Casamassimi, A.; Napoli, C. Platelet Derivatives in Regenerative Medicine: An Update. Transfus. Med. Rev. 2015, 29, 52–61. [Google Scholar] [CrossRef] [PubMed]
- Morishita, R.; Aoki, M.; Yo, Y.; Ogihara, T. Hepatocyte Growth Factor as Cardiovascular Hormone: Role of HGF in the Pathogenesis of Cardiovascular Disease. Endocr. J. 2002, 49, 273–284. [Google Scholar] [CrossRef]
- Ding, B.-S.; Nolan, D.J.; Butler, J.M.; James, D.; Babazadeh, A.O.; Rosenwaks, Z.; Mittal, V.; Kobayashi, H.; Shido, K.; Lyden, D.; et al. Inductive Angiocrine Signals from Sinusoidal Endothelium Are Required for Liver Regeneration. Nature 2010, 468, 310–315. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Lian, F.; Li, J.; Fan, W.; Xu, H.; Yang, X.; Liang, L.; Chen, W.; Yang, J. Adipose Derived Mesenchymal Stem Cells Transplantation via Portal Vein Improves Microcirculation and Ameliorates Liver Fibrosis Induced by CCl4 in Rats. J. Transl. Med. 2012, 10, 133. [Google Scholar] [CrossRef]
- Takahashi, K.; Murata, S.; Fukunaga, K.; Ohkohchi, N. Human Platelets Inhibit Liver Fibrosis in Severe Combined Immunodeficiency Mice. World J. Gastroenterol. WJG 2013, 19, 5250–5260. [Google Scholar] [CrossRef]
- Kusumoto, K.; Ido, A.; Moriuchi, A.; Katsura, T.; Kim, I.; Takahama, Y.; Numata, M.; Kodama, M.; Hasuike, S.; Nagata, K.; et al. Repeated Intravenous Injection of Recombinant Human Hepatocyte Growth Factor Ameliorates Liver Cirrhosis but Causes Albuminuria in Rats. Int. J. Mol. Med. 2006, 17, 503–509. [Google Scholar] [CrossRef]
- Hải Nam, N.; Le, T.V.; Do, H.; Dang, M.T.; Nguyen, Y.; Vo, N.; Nhung, T. Human Adipose-Derived Stem Cells Pre-Treated with Platelet-Rich Plasma and Hepatocyte Growth Factor Alleviate Liver Fibrosis in Mice. Biomed. Res. Ther. 2018, 5, 2332–2348. [Google Scholar] [CrossRef]
- Lucarelli, E.; Beccheroni, A.; Donati, D.; Sangiorgi, L.; Cenacchi, A.; Del Vento, A.M.; Meotti, C.; Bertoja, A.Z.; Giardino, R.; Fornasari, P.M.; et al. Platelet-Derived Growth Factors Enhance Proliferation of Human Stromal Stem Cells. Biomaterials 2003, 24, 3095–3100. [Google Scholar] [CrossRef] [PubMed]
- Hesami, Z.; Jamshidzadeh, A.; Ayatollahi, M.; Geramizadeh, B.; Farshad, O.; Vahdati, A. Effect of Platelet-Rich Plasma on CCl4-Induced Chronic Liver Injury in Male Rats. Int. J. Hepatol. 2014, 2014, 932930. [Google Scholar] [CrossRef]
- Salem, N.A.; Hamza, A.; Alnahdi, H.; Ayaz, N. Biochemical and Molecular Mechanisms of Platelet-Rich Plasma in Ameliorating Liver Fibrosis Induced by Dimethylnitrosurea. Cell. Physiol. Biochem. Int. J. Exp. Cell. Physiol. Biochem. Pharmacol. 2018, 47, 2331–2339. [Google Scholar] [CrossRef] [PubMed]
- Ishak, K.; Baptista, A.; Bianchi, L.; Callea, F.; De Groote, J.; Gudat, F.; Denk, H.; Desmet, V.; Korb, G.; MacSween, R.N. Histological Grading and Staging of Chronic Hepatitis. J. Hepatol. 1995, 22, 696–699. [Google Scholar] [CrossRef] [PubMed]
- Brunt, E.M. Grading and Staging the Histopathological Lesions of Chronic Hepatitis: The Knodell Histology Activity Index and Beyond. Hepatology 2000, 31, 241–246. [Google Scholar] [CrossRef] [PubMed]
- Sant’Anna, L.B.; Cargnoni, A.; Ressel, L.; Vanosi, G.; Parolini, O. Amniotic Membrane Application Reduces Liver Fibrosis in a Bile Duct Ligation Rat Model. Cell Transplant. 2011, 20, 441–453. [Google Scholar] [CrossRef] [PubMed]
- Teixeira, C.; Franco, E.; Oliveira, P.A.; Colaço, B.; Gama, A.; Carrola, J.; Pires, C.A.; Colaço, A.; Pires, M.J. Effects of Nebivolol on Liver Fibrosis Induced by Bile Duct Ligation in Wistar Rats. In Vivo 2013, 27, 635–640. [Google Scholar]
- Ricci, E.; Vanosi, G.; Lindenmair, A.; Hennerbichler, S.; Peterbauer-Scherb, A.; Wolbank, S.; Cargnoni, A.; Signoroni, P.B.; Campagnol, M.; Gabriel, C.; et al. Anti-Fibrotic Effects of Fresh and Cryopreserved Human Amniotic Membrane in a Rat Liver Fibrosis Model. Cell Tissue Bank. 2013, 14, 475–488. [Google Scholar] [CrossRef]
- Fallon, M.B.; Abrams, G.A.; McGrath, J.W.; Hou, Z.; Luo, B. Common Bile Duct Ligation in the Rat: A Model of Intrapulmonary Vasodilatation and Hepatopulmonary Syndrome. Am. J. Physiol. 1997, 272, G779–G784. [Google Scholar] [CrossRef]
- Luo, B.; Liu, L.; Tang, L.; Zhang, J.; Ling, Y.; Fallon, M.B. ET-1 and TNF-Alpha in HPS: Analysis in Prehepatic Portal Hypertension and Biliary and Nonbiliary Cirrhosis in Rats. Am. J. Physiol. Gastrointest. Liver Physiol. 2004, 286, G294–G303. [Google Scholar] [CrossRef]
- Katsuta, Y.; Zhang, X.-J.; Ohsuga, M.; Akimoto, T.; Komeichi, H.; Shimizu, S.; Kato, Y.; Miyamoto, A.; Satomura, K.; Takano, T. Arterial Hypoxemia and Intrapulmonary Vasodilatation in Rat Models of Portal Hypertension. J. Gastroenterol. 2005, 40, 811–819. [Google Scholar] [CrossRef]
- Geerts, A.M.; Vanheule, E.; Praet, M.; Van Vlierberghe, H.; De Vos, M.; Colle, I. Comparison of Three Research Models of Portal Hypertension in Mice: Macroscopic, Histological and Portal Pressure Evaluation. Int. J. Exp. Pathol. 2008, 89, 251–263. [Google Scholar] [CrossRef]
- Aller, M.A.; Duran, M.; Ortega, L.; Arias, J.L.; Nava, M.P.; Prieto, I.; Arias, J. Comparative Study of Macro- and Microsurgical Extrahepatic Cholestasis in the Rat. Microsurgery 2004, 24, 442–447. [Google Scholar] [CrossRef]
- Yang, Y.; Chen, B.; Chen, Y.; Zu, B.; Yi, B.; Lu, K. A Comparison of Two Common Bile Duct Ligation Methods to Establish Hepatopulmonary Syndrome Animal Models. Lab. Anim. 2015, 49, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, S.; Georgiev, P.; Weber, A.; Vergopoulos, A.; Graf, R.; Clavien, P.-A. Partial Bile Duct Ligation in Mice: A Novel Model of Acute Cholestasis. Surgery 2011, 149, 445–451. [Google Scholar] [CrossRef]
- Miranda-Díaz, A.G.; Alonso-Martínez, H.; Hernández-Ojeda, J.; Arias-Carvajal, O.; Rodríguez-Carrizalez, A.D.; Román-Pintos, L.M. Toll-like Receptors in Secondary Obstructive Cholangiopathy. Gastroenterol. Res. Pract. 2011, 2011, 265093. [Google Scholar] [CrossRef]
- Snowdon, V.K.; Fallowfield, J.A. Models and Mechanisms of Fibrosis Resolution. Alcohol. Clin. Exp. Res. 2011, 35, 794–799. [Google Scholar] [CrossRef]
- Mohamed, H.; Elswefy, S.; Rashed, L.A.; Younis, N.N.; Shaheen, M.; Ghanim, A. Cholestatic Liver Fibrosis in a Rat Model of Bile Duct Ligation: Evaluating Biochemical versus Histopathological Changes. Int. J. Pharm. Pharm. Sci. 2015, 7, 349–354. [Google Scholar]
- Asrani, S.K.; Devarbhavi, H.; Eaton, J.; Kamath, P.S. Burden of Liver Diseases in the World. J. Hepatol. 2019, 70, 151–171. [Google Scholar] [CrossRef]
- Campana, L.; Iredale, J.P. Regression of Liver Fibrosis. Semin. Liver Dis. 2017, 37, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, S.; Nakamura, T. Hepatocyte Growth Factor: A Regenerative Drug for Acute Hepatitis and Liver Cirrhosis. Regen. Med. 2007, 2, 161–170. [Google Scholar] [CrossRef]
- Saito, Y.; Shimada, M.; Utsunomiya, T.; Ikemoto, T.; Yamada, S.; Morine, Y.; Imura, S.; Mori, H.; Sugimoto, K.; Iwahashi, S.; et al. The Protective Effect of Adipose-Derived Stem Cells against Liver Injury by Trophic Molecules. J. Surg. Res. 2013, 180, 162–168. [Google Scholar] [CrossRef]
- Kim, W.-H.; Matsumoto, K.; Bessho, K.; Nakamura, T. Growth Inhibition and Apoptosis in Liver Myofibroblasts Promoted by Hepatocyte Growth Factor Leads to Resolution from Liver Cirrhosis. Am. J. Pathol. 2005, 166, 1017–1028. [Google Scholar] [CrossRef]
- Kurzyk, A.; Dębski, T.; Święszkowski, W.; Pojda, Z. Comparison of Adipose Stem Cells Sources from Various Locations of Rat Body for Their Application for Seeding on Polymer Scaffolds. J. Biomater. Sci. Polym. Ed. 2019, 30, 376–397. [Google Scholar] [CrossRef] [PubMed]
- Gronthos, S.; Simmons, P.J. The Growth Factor Requirements of STRO-1-Positive Human Bone Marrow Stromal Precursors under Serum-Deprived Conditions in Vitro. Blood 1995, 85, 929–940. [Google Scholar] [CrossRef] [PubMed]
- Ayatollahi, M.; Soleimani, M.; Tabei, S.Z.; Kabir Salmani, M. Hepatogenic Differentiation of Mesenchymal Stem Cells Induced by Insulin like Growth Factor-I. World J. Stem Cells 2011, 3, 113–121. [Google Scholar] [CrossRef]
- Zhu, Y.; Yuan, M.; Meng, H.Y.; Wang, A.Y.; Guo, Q.Y.; Wang, Y.; Peng, J. Basic Science and Clinical Application of Platelet-Rich Plasma for Cartilage Defects and Osteoarthritis: A Review. Osteoarthr. Cartil. 2013, 21, 1627–1637. [Google Scholar] [CrossRef] [PubMed]
- Cavallo, C.; Roffi, A.; Grigolo, B.; Mariani, E.; Pratelli, L.; Merli, G.; Kon, E.; Marcacci, M.; Filardo, G. Platelet-Rich Plasma: The Choice of Activation Method Affects the Release of Bioactive Molecules. BioMed Res. Int. 2016, 2016, 6591717. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Campos, S.; Tuñón, M.J.; González, P.; González-Gallego, J. Oxidative Stress and Changes in Liver Antioxidant Enzymes Induced by Experimental Dicroceliosis in Hamsters. Parasitol. Res. 1999, 85, 468–474. [Google Scholar] [CrossRef]
- DeLong, J.M.; Russell, R.P.; Mazzocca, A.D. Platelet-Rich Plasma: The PAW Classification System. Arthrosc. J. Arthrosc. Relat. Surg. Off. Publ. Arthrosc. Assoc. N. Am. Int. Arthrosc. Assoc. 2012, 28, 998–1009. [Google Scholar] [CrossRef]
- Martín-Solé, O.; Rodó, J.; García-Aparicio, L.; Blanch, J.; Cusí, V.; Albert, A. Effects of Platelet-Rich Plasma (PRP) on a Model of Renal Ischemia-Reperfusion in Rats. PLoS ONE 2016, 11, e0160703. [Google Scholar] [CrossRef]
- Akimoto, T.; Hayashi, N.; Adachi, M.; Kobayashi, N.; Zhang, X.-J.; Ohsuga, M.; Katsuta, Y. Viability and Plasma Vitamin K Levels in the Common Bile Duct-Ligated Rats. Exp. Anim. 2005, 54, 155–161. [Google Scholar] [CrossRef]
- Hao, T.; Chen, J.; Zhi, S.; Zhang, Q.; Chen, G.; Yu, F. Comparison of Bone Marrow-vs. Adipose Tissue-Derived Mesenchymal Stem Cells for Attenuating Liver Fibrosis. Exp. Ther. Med. 2017, 14, 5956–5964. [Google Scholar] [CrossRef]
- Adas, G.; Koc, B.; Adas, M.; Duruksu, G.; Subasi, C.; Kemik, O.; Kemik, A.; Sakiz, D.; Kalayci, M.; Purisa, S.; et al. Effects of Mesenchymal Stem Cells and VEGF on Liver Regeneration Following Major Resection. Langenbecks Arch. Surg. 2016, 401, 725–740. [Google Scholar] [CrossRef] [PubMed]
- Mungunsukh, O.; McCart, E.A.; Day, R.M. Hepatocyte Growth Factor Isoforms in Tissue Repair, Cancer, and Fibrotic Remodeling. Biomedicines 2014, 2, 301–326. [Google Scholar] [CrossRef]
- Kim, S.-J.; Park, K.C.; Lee, J.U.; Kim, K.-J.; Kim, D.-G. Therapeutic Potential of Adipose Tissue-Derived Stem Cells for Liver Failure According to the Transplantation Routes. J. Korean Surg. Soc. 2011, 81, 176–186. [Google Scholar] [CrossRef] [PubMed]
- Matsuo, R.; Ohkohchi, N.; Murata, S.; Ikeda, O.; Nakano, Y.; Watanabe, M.; Hisakura, K.; Myronovych, A.; Kubota, T.; Narimatsu, H.; et al. Platelets Strongly Induce Hepatocyte Proliferation with IGF-1 and HGF In Vitro. J. Surg. Res. 2008, 145, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Mizuno, S.; Ikebuchi, F.; Fukuta, K.; Kato, T.; Matsumoto, K.; Adachi, K.; Abe, T.; Nakamura, T. Recombinant Human Hepatocyte Growth Factor (HGF), but Not Rat HGF, Elicits Glomerular Injury and Albuminuria in Normal Rats via an Immune Complex-Dependent Mechanism. Clin. Exp. Pharmacol. Physiol. 2011, 38, 192–201. [Google Scholar] [CrossRef] [PubMed]
- Kaibori, M.; Kwon, A.H.; Nakagawa, M.; Wei, T.; Uetsuji, S.; Kamiyama, Y.; Okumura, T.; Kitamura, N. Stimulation of Liver Regeneration and Function after Partial Hepatectomy in Cirrhotic Rats by Continuous Infusion of Recombinant Human Hepatocyte Growth Factor. J. Hepatol. 1997, 27, 381–390. [Google Scholar] [CrossRef] [PubMed]
- Kaido, T.; Yoshikawa, A.; Seto, S.; Yamaoka, S.; Sato, M.; Ishii, T.; Imamura, M. Portal Branch Ligation with a Continuous Hepatocyte Growth Factor Supply Makes Extensive Hepatectomy Possible in Cirrhotic Rats. Hepatology 1998, 28, 756–760. [Google Scholar] [CrossRef]
- An, Y.; Xiao, Y.-B. Growth Hormone Prevents Acute Liver Injury Induced by Cardiopulmonary Bypass in a Rat Model. J. Thorac. Cardiovasc. Surg. 2007, 134, 342–350. [Google Scholar] [CrossRef] [PubMed]









Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shivaramu, S.; Maiti, S.K.; Banu, S.A.; Kalaiselvan, E.; Sharun, K.; Mishra, M.; Mohan, D.; Palakkara, S.; Kumar, S.; Sahoo, M.; et al. Synergistic Hepatoprotective Effects of Mesenchymal Stem Cells and Platelet-Rich Plasma in a Rat Model of Bile Duct Ligation-Induced Liver Cirrhosis. Cells 2024, 13, 404. https://doi.org/10.3390/cells13050404
Shivaramu S, Maiti SK, Banu SA, Kalaiselvan E, Sharun K, Mishra M, Mohan D, Palakkara S, Kumar S, Sahoo M, et al. Synergistic Hepatoprotective Effects of Mesenchymal Stem Cells and Platelet-Rich Plasma in a Rat Model of Bile Duct Ligation-Induced Liver Cirrhosis. Cells. 2024; 13(5):404. https://doi.org/10.3390/cells13050404
Chicago/Turabian StyleShivaramu, Shivaraju, Swapan Kumar Maiti, Shajahan Amitha Banu, Elangovan Kalaiselvan, Khan Sharun, Mamta Mishra, Divya Mohan, Sangeetha Palakkara, Sunil Kumar, Monalisa Sahoo, and et al. 2024. "Synergistic Hepatoprotective Effects of Mesenchymal Stem Cells and Platelet-Rich Plasma in a Rat Model of Bile Duct Ligation-Induced Liver Cirrhosis" Cells 13, no. 5: 404. https://doi.org/10.3390/cells13050404