
The Role of Preservation Solutions upon Saphenous Vein Endothelial Integrity and Function: Systematic Review and UK Practice Survey

 ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
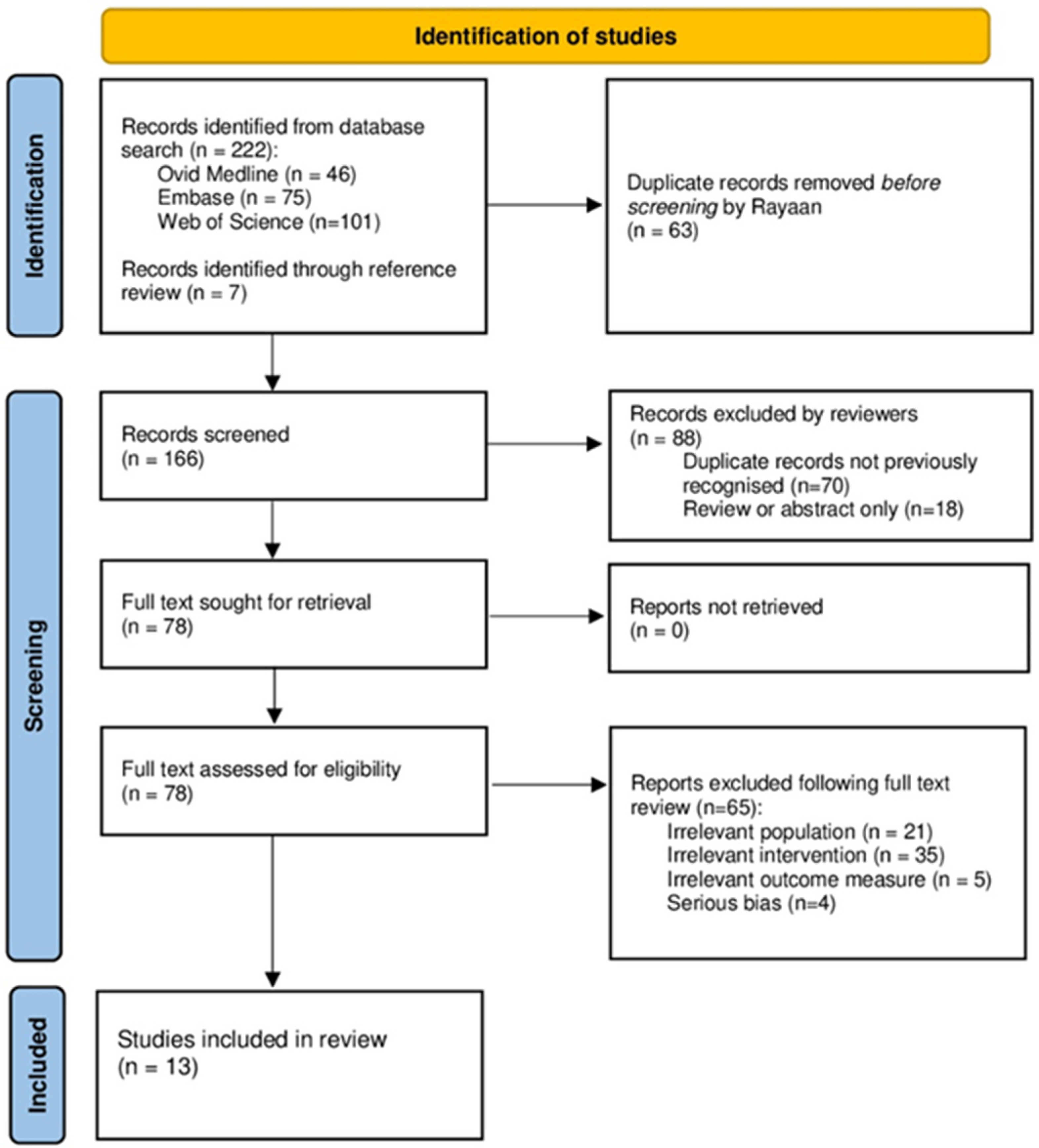
2. Materials and Methods
2.1. Study Eligibility
- Any studies utilising preservation solutions during or following the process of saphenous vein harvest;
- Analysing the effect of these solutions on saphenous vein endothelial cell integrity, function, or both, versus a control. Accepted control solutions were saline with or without heparin;
- Human subjects undergoing coronary artery bypass grafting; and
- All study models (in vivo, in vitro, and ex vivo).
- 5.
- No implementation of preservation solutions;
- 6.
- No provision of a control group who received standard of care, as defined by study authors;
- 7.
- Non-human subjects;
- 8.
- Analysing arterial endothelial cell integrity or function;
- 9.
- Systematic review or meta-analyses not reporting original data;
- 10.
- Conference and meeting abstracts, case reports and literature reviews;
- 11.
- Studies not published in English.
2.2. Search Strategy
2.3. Data Extraction
2.4. Study Outcomes
2.5. Data Synthesis
2.6. Survey of National Practice
3. Results
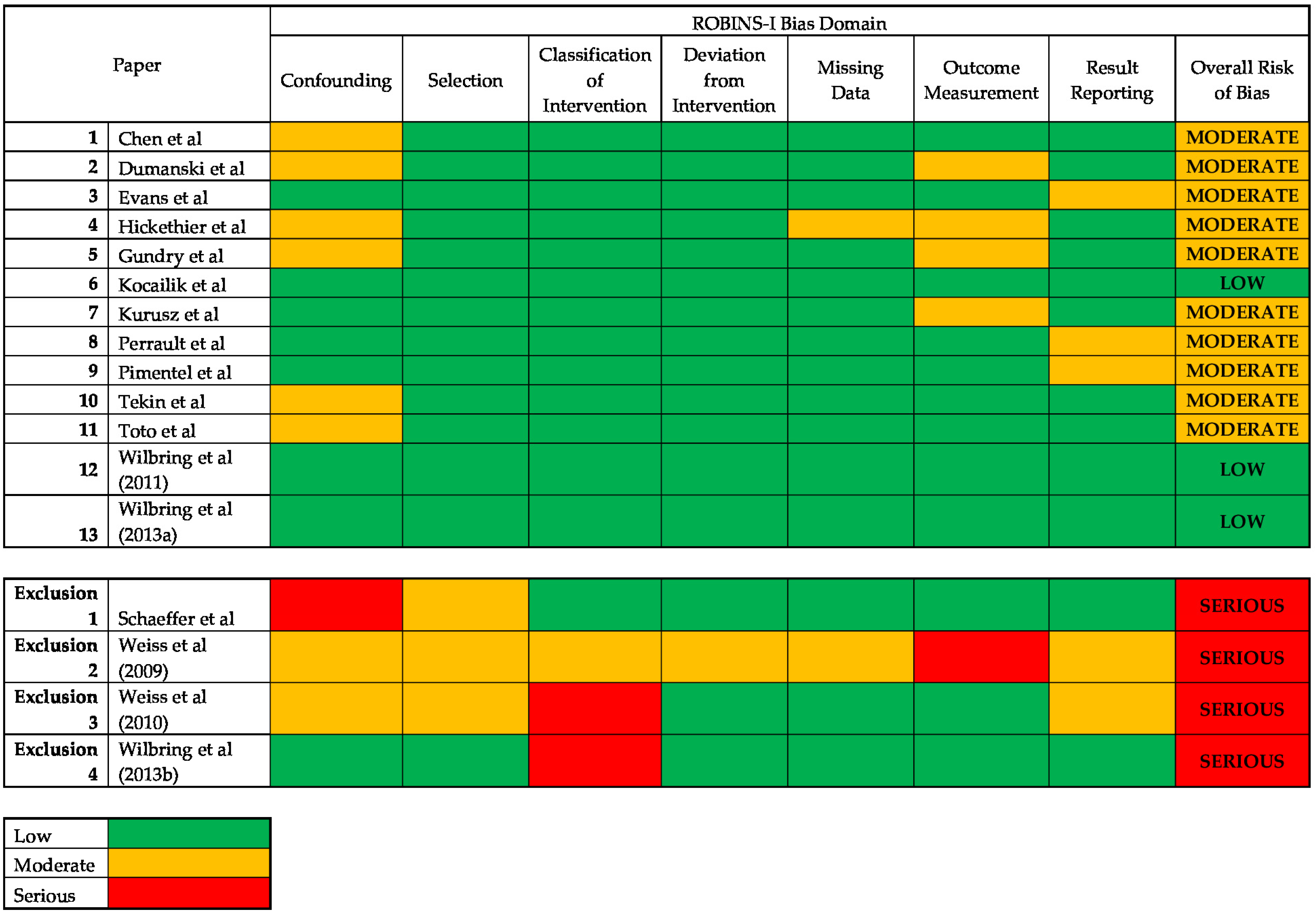
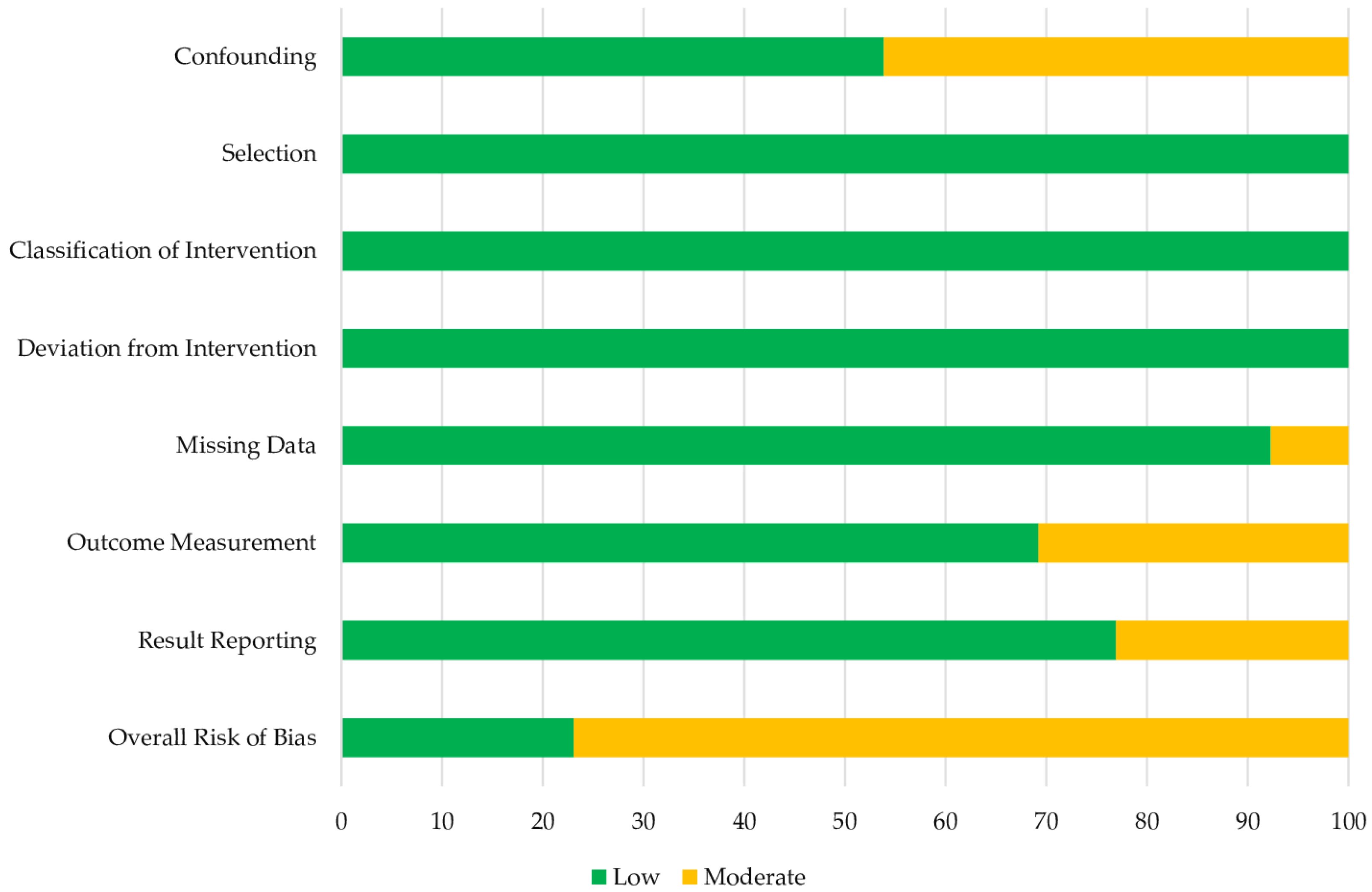
3.1. Risk of Bias
3.2. Endothelial Preservation
3.3. Endothelial Inflammation and Oxidative Response
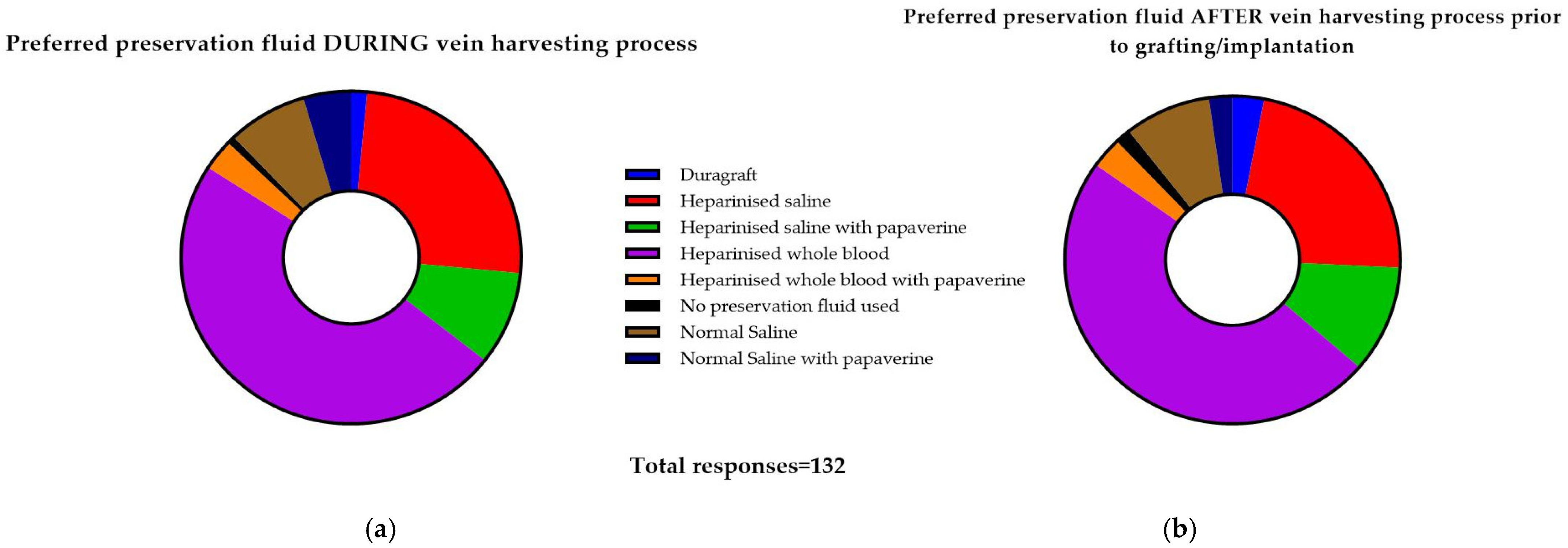
3.4. Survey of National Practice
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A
- What is your role?
- Which hospital are you answering on behalf of?
- How many consultants (performing adult cardiac procedures) are there within your unit?
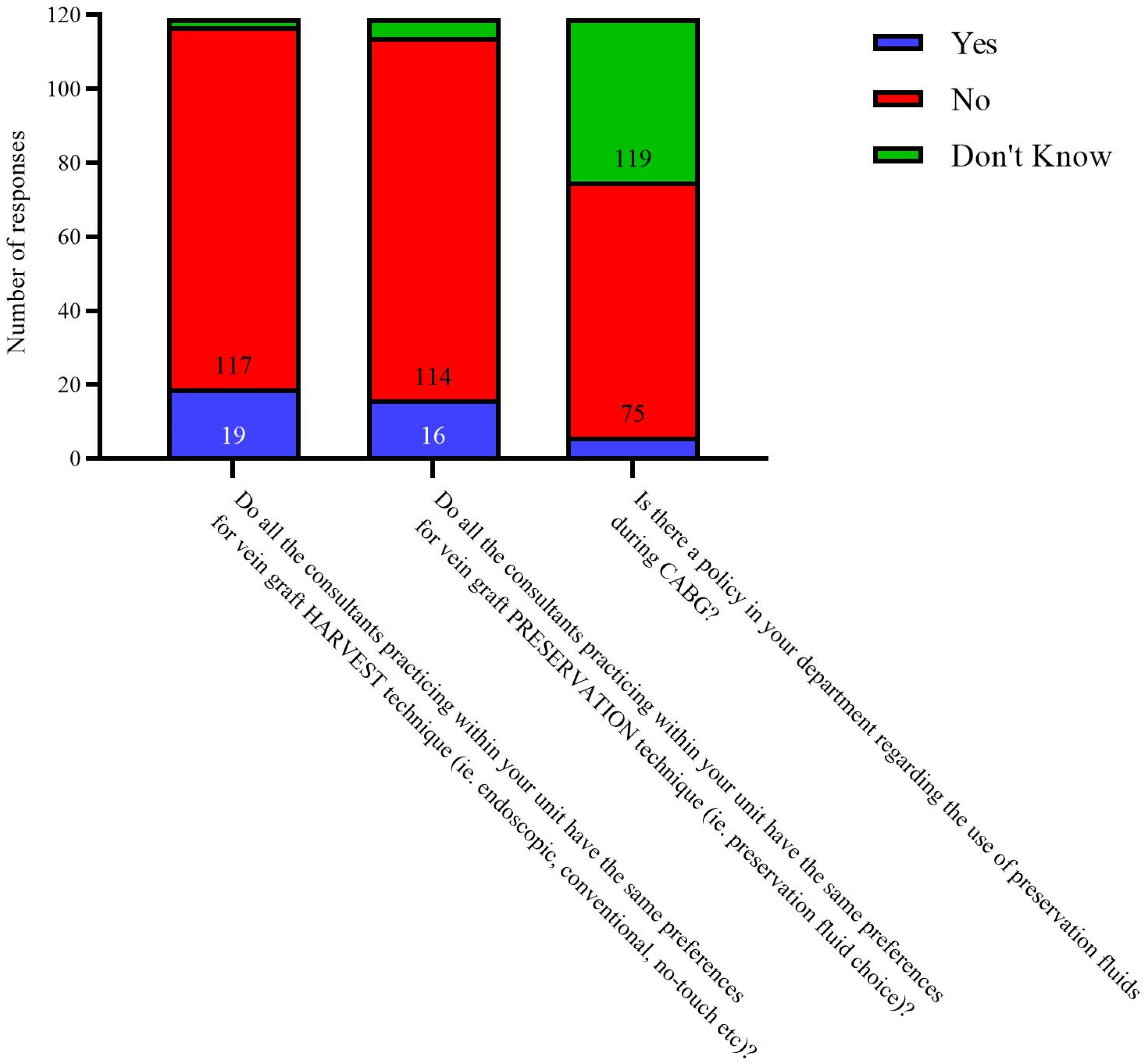
- Do all the consultants practicing within your unit have the same preferences for vein graft HARVEST technique (ie. Endoscopic, conventional, no-touch etc)?
- Do all the consultants practicing within your unit have the same preferences for vein graft PRESERVATION technique (ie. Preservation fluid choice)?
- Is there a policy in your department regarding the use of preservation fluids during CABG?
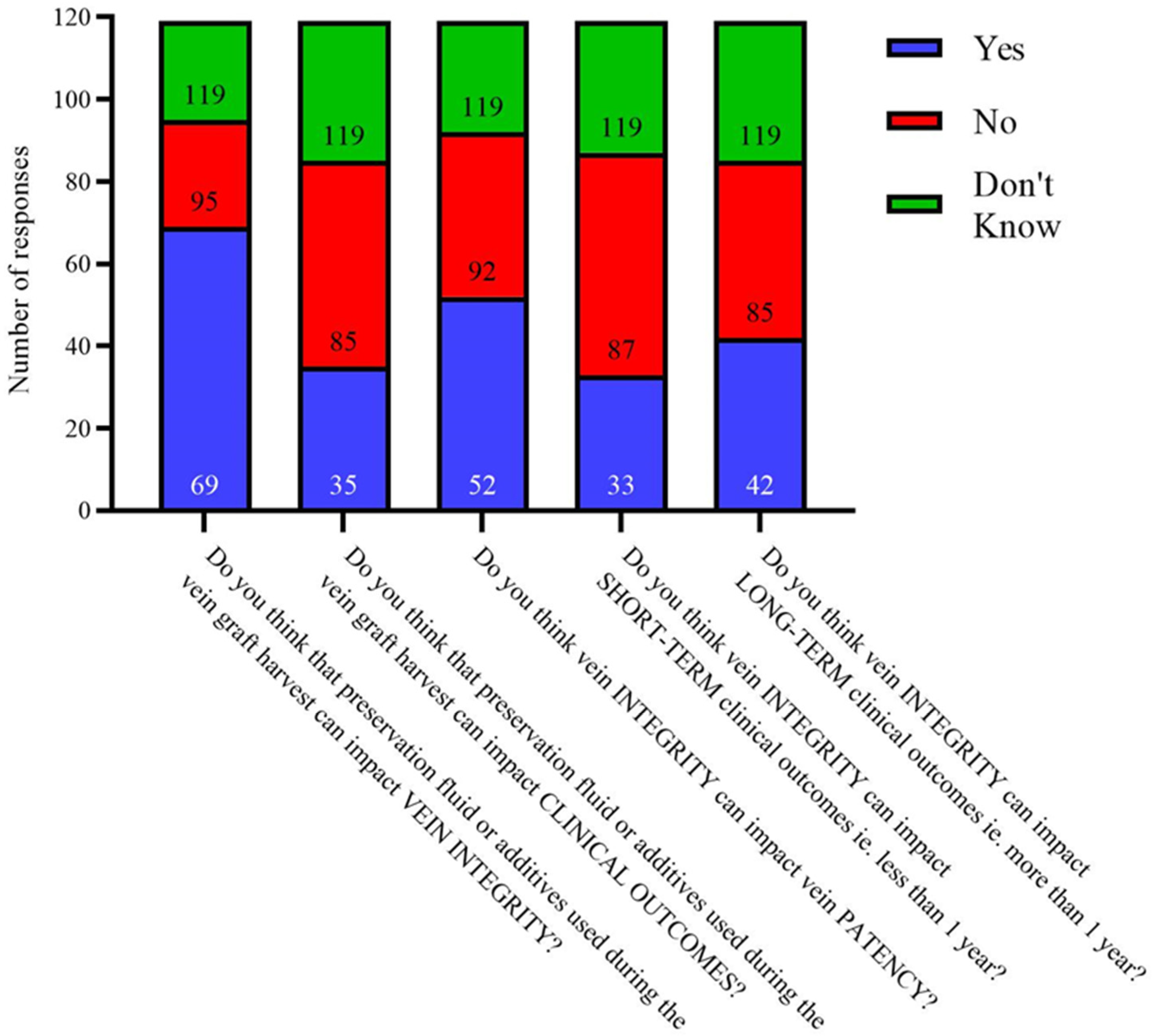
- Do you think that preservation fluid or additives used during the vein graft harvest can impact VEIN INTEGRITY?
- Do you think that preservation fluid or additives used during the vein graft harvest can impact CLINICAL OUTCOMES?
- Do you think vein INTEGRITY can impact vein PATENCY?
- Do you think vein INTEGRITY can impact SHORT-TERM clinical outcomes ie. Less than 1 year?
- Do you think vein INTEGRITY can impact LONG-TERM clinical outcomes ie. More than 1 year?
- Which is more important after CABG?
- Which of these harvest techniques are used in your unit? Please select all which are used.
- Do your unit perform functional intra-operative ultra-sound flow assessment after completion of CABG?
- “If you answered ‘No’ to““Do your unit perform functional intra-operative ultra-sound flow assessment after completion of CABG?”“, why not? If known ie. Resource limitation, surgeon preference, anaesthetist preference etc.”
- Which is these fluids is the preferred choice to distend the vein DURING the harvesting process?
- Which is these fluids is the preferred choice to distend the vein AFTER the harvesting process, prior to grafting/implantation?
- Would you like to provide information for another consultant? (If yes, option to provide information for up to ten consultant surgeons).
- Which is these fluids is the preferred choice to distend the vein DURING the harvesting process?
- Which is these fluids is the preferred choice to distend the vein AFTER the harvesting process, prior to grafting/implantation?
- Would you like to provide information for another consultant?
- Which is these fluids is the preferred choice to distend the vein DURING the harvesting process?
- Which is these fluids is the preferred choice to distend the vein AFTER the harvesting process, prior to grafting/implantation?
References
- Ward, A.O.; Angelini, G.D.; Caputo, M.; Evans, P.C.; Johnson, J.L.; Suleiman, M.S.; Tulloh, R.M.; George, S.J.; Zakkar, M. NF-κB inhibition prevents acute shear stress-induced inflammation in the saphenous vein graft endothelium. Sci. Rep. 2020, 10, 15133. [Google Scholar] [CrossRef]
- Guida, G.; Ward, A.O.; Bruno, V.D.; George, S.J.; Caputo, M.; Angelini, G.D.; Zakkar, M. Saphenous vein graft disease, pathophysiology, prevention, and treatment. A review of the literature. J. Card. Surg. 2020, 35, 1314–1321. [Google Scholar] [CrossRef] [PubMed]
- Ladak, S.S.; McQueen, L.W.; Layton, G.R.; Aujla, H.; Adebayo, A.; Zakkar, M. The Role of Endothelial Cells in the Onset, Development and Modulation of Vein Graft Disease. Cells 2022, 11, 3066. [Google Scholar] [CrossRef] [PubMed]
- Winkler, B.; Reineke, D.; Heinisch, P.P.; Schönhoff, F.; Huber, C.; Kadner, A.; Englberger, L.; Carrel, T. Graft preservation solutions in cardiovascular surgery. Interact. Cardiovasc. Thorac. Surg. 2016, 23, 300–309. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 350, g7647. [Google Scholar] [CrossRef] [Green Version]
- Zakkar, M.L.G.; Ladak, S.; McQueen, L. Solutions for the preservation of vein graft endothelial cells: A systematic review. 2022. PROSPERO CRD42022358828. [Google Scholar]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan-a web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [Green Version]
- Rohatgi, A. WebPlotDigitizer—Extract Data from Plots, Images, and Maps. Available online: https://automeris.io/WebPlotDigitizer/ (accessed on 17 February 2023).
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.W.; Chu, Y.; Wu, V.C.; Tsai, F.C.; Nan, Y.Y.; Lee, H.F.; Chang, C.H.; Chu, P.H.; Wu, S.; Lin, P.J. Microenvironment of saphenous vein graft preservation prior to coronary artery bypass grafting. Interact. Cardiovasc. Thorac. Surg. 2019, 28, 71–78. [Google Scholar] [CrossRef]
- Dumanski, A.; Sopel, M.; Pelczar, M.; Szłapka, M.; Kustrzycki, W.; Zabel, M. Influence of pressure on the endothelium of the saphenous vein coronary artery bypass graft. Vivo 2007, 21, 785–789. [Google Scholar]
- Evans, A.M.M.G.; Sileri, P.; Zhang, W.; Jarzembowski, T.; Kpodonu, J.; Geha, A.S.; Benedetti, E. Effects of procurement and preservation media on cellular apoptosis in autologous saphenous vein grafts. J. Appl. Res. 2004, 4, 453–463. [Google Scholar]
- Gundry, S.R.; Jones, M.; Ishihara, T.; Ferrans, V.J. Optimal preparation techniques for human saphenous vein grafts. Surgery 1980, 88, 785–794. [Google Scholar] [PubMed]
- Hickethier, T.; Dämmrich, J.; Silber, R.E.; Finster, S.; Elert, O. Ultrastructural investigations for reducing endothelial cell damage of vein grafts during CABG-operation and practical consequences. J. Cardiovasc. Surg. 1999, 40, 71–76. [Google Scholar]
- Kocailik, A.; Basaran, M.; Ugurlucan, M.; Ozbek, C.; Kafali, E.; Yerebakan, C.; Selimoglu, O.; Banach, M.; Ucak, A.; Ogus, T.N.; et al. Papaverine solution improves preservation of saphenous vein grafts used during cardiac surgery. Acta Cardiol. 2008, 63, 445–449. [Google Scholar] [CrossRef]
- Kurusz, M.; Christman, E.W.; Derrick, J.R.; Tyers, G.F.; Williams, E.H. Use of cold cardioplegic solution for vein graft distention and preservation: A light and scanning electron microscopic study. Ann. Thorac. Surg. 1981, 32, 68–74. [Google Scholar] [CrossRef]
- Perrault, L.P.; Carrier, M.; Voisine, P.; Olsen, P.S.; Noiseux, N.; Jeanmart, H.; Cardemartiri, F.; Veerasingam, D.; Brown, C.; Guertin, M.C.; et al. Sequential multidetector computed tomography assessments after venous graft treatment solution in coronary artery bypass grafting. J. Thorac. Cardiovasc. Surg. 2019, 161, 96–106. [Google Scholar] [CrossRef]
- Pimentel, M.D.; Lobo Filho, J.G.; Lobo Filho, H.G.; de Castro Miguel, E.; Pinheiro Paiva, S.K.; Silva Matos, J.I.; Mesquita Fernandes, M.A.; Fechine Jamacaru, F.V. Effect of preservation solution and distension pressure on saphenous vein’s endothelium. Interact. Cardiovasc. Thorac. Surg. 2022, 35, ivac124. [Google Scholar] [CrossRef]
- Tekin, I.; Demir, M.; Özdem, S. Effect of different storage solutions on oxidative stress in human saphenous vein grafts. J. Cardiothorac. Surg. 2022, 17, 7. [Google Scholar] [CrossRef]
- Toto, F.; Torre, T.; Turchetto, L.; Lo Cicero, V.; Soncin, S.; Klersy, C.; Demertzis, S.; Ferrari, E. Efficacy of Intraoperative Vein Graft Storage Solutions in Preserving Endothelial Cell Integrity during Coronary Artery Bypass Surgery. J. Clin. Med. 2022, 11, 1093. [Google Scholar] [CrossRef]
- Wilbring, M.; Tugtekin, S.M.; Zatschler, B.; Ebner, A.; Reichenspurner, H.; Matschke, K.; Deussen, A. Even short-time storage in physiological saline solution impairs endothelial vascular function of saphenous vein grafts. Eur. J. Cardiothorac. Surg. 2011, 40, 811–815. [Google Scholar] [CrossRef]
- Wilbring, M.; Tugtekin, S.M.; Zatschler, B.; Ebner, A.; Reichenspurner, H.; Kappert, U.; Matschke, K.; Deussen, A. Preservation of endothelial vascular function of saphenous vein grafts after long-time storage with a recently developed potassium-chloride and N-acetylhistidine enriched storage solution. Thorac. Cardiovasc. Surg. 2013, 61, 656–662. [Google Scholar] [CrossRef] [PubMed]
- Weiss, D.R.; Juchem, G.; Eblenkamp, M.; Kemkes, B.M.; Gansera, B.; Geier, M.; Nees, S. Search for optimized conditions for sealing and storage of bypass vessels: Influence of preservation solution and filling pressure on the degree of endothelialization. Int. J. Clin. Exp. Med. 2010, 3, 10–27. [Google Scholar] [PubMed]
- Weiss, D.R.; Juchem, G.; Kemkes, B.M.; Gansera, B.; Nees, S. Extensive deendothelialization and thrombogenicity in routinely prepared vein grafts for coronary bypass operations: Facts and remedy. Int. J. Clin. Exp. Med. 2009, 2, 95–113. [Google Scholar]
- Wilbring, M.; Ebner, A.; Schoenemann, K.; Knaut, M.; Tugtekin, S.M.; Zatschler, B.; Waldow, T.; Alexiou, K.; Matschke, K.; Deussen, A. Heparinized blood better preserves cellular energy charge and vascular functions of intraoperatively stored saphenous vein grafts in comparison to isotonic sodium-chloride-solution. Clin. Hemorheol. Microcirc. 2013, 55, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Schaeffer, U.; Tanner, B.; Strohschneider, T.; Stadtmüller, A.; Hannekum, A. Damage to arterial and venous endothelial cells in bypass grafts induced by several solutions used in bypass surgery. Thorac. Cardiovasc. Surg. 1997, 45, 168–171. [Google Scholar] [CrossRef]
- Wise, E.S.; Hocking, K.M.; Eagle, S.; Absi, T.; Komalavilas, P.; Cheung-Flynn, J.; Brophy, C.M. Preservation solution impacts physiologic function and cellular viability of human saphenous vein graft. Surgery 2015, 158, 537–546. [Google Scholar] [CrossRef] [Green Version]
- Bouhout, I.; Ali, W.B.; Perrault, L.P. The effect of storage solutions on endothelial function and saphenous vein graft patency. Indian J. Thorac. Cardiovasc. Surg. 2018, 34, 258–265. [Google Scholar] [CrossRef]
- Commandeur, F.; Goeller, M.; Dey, D. Cardiac CT: Technological Advances in Hardware, Software, and Machine Learning Applications. Curr. Cardiovasc. Imaging Rep. 2018, 11, 1–2. [Google Scholar] [CrossRef]
- Di Lazzaro, D.; Crusco, F. CT angio for the evaluation of graft patency. J. Thorac. Dis. 2017, 9, S283–S288. [Google Scholar] [CrossRef] [Green Version]
- Shuhaiber, J.H.; Evans, A.N.; Massad, M.G.; Geha, A.S. Mechanisms and future directions for prevention of vein graft failure in coronary bypass surgery. Eur. J. Cardiothorac. Surg. 2002, 22, 387–396. [Google Scholar] [CrossRef] [PubMed]
- Petrenko, A.; Carnevale, M.; Somov, A.; Osorio, J.; Rodríguez, J.; Guibert, E.; Fuller, B.; Froghi, F. Organ Preservation into the 2020s: The Era of Dynamic Intervention. Transfus. Med. Hemother. 2019, 46, 151–172. [Google Scholar] [CrossRef] [Green Version]
- Kieser, T.M.; Taggart, D.P. Current status of intra-operative graft assessment: Should it be the standard of care for coronary artery bypass graft surgery? J. Card. Surg. 2018, 33, 219–228. [Google Scholar] [CrossRef]
- Maltais, S.; Widmer, R.J.; Bell, M.R.; Daly, R.C.; Dearani, J.A.; Greason, K.L.; Joyce, D.L.; Joyce, L.D.; Schaff, H.V.; Stulak, J.M. Reoperation for Coronary Artery Bypass Grafting Surgery: Outcomes and Considerations for Expanding Interventional Procedures. Ann. Thorac. Surg. 2017, 103, 1886–1892. [Google Scholar] [CrossRef] [Green Version]
- Yap, C.H.; Sposato, L.; Akowuah, E.; Theodore, S.; Dinh, D.T.; Shardey, G.C.; Skillington, P.D.; Tatoulis, J.; Yii, M.; Smith, J.A.; et al. Contemporary results show repeat coronary artery bypass grafting remains a risk factor for operative mortality. Ann. Thorac. Surg. 2009, 87, 1386–1391. [Google Scholar] [CrossRef] [PubMed]
- Ferrari, G.; Geijer, H.; Cao, Y.; Souza, D.; Samano, N. Percutaneous coronary intervention in saphenous vein grafts after coronary artery bypass grafting: A systematic review and meta-analysis. Scand. Cardiovasc. J. 2021, 55, 245–253. [Google Scholar] [CrossRef]
- Sabik, J.F., 3rd. Understanding saphenous vein graft patency. Circulation 2011, 124, 273–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xenogiannis, I.; Zenati, M.; Bhatt, D.L.; Rao, S.V.; Rodés-Cabau, J.; Goldman, S.; Shunk, K.A.; Mavromatis, K.; Banerjee, S.; Alaswad, K.; et al. Saphenous Vein Graft Failure: From Pathophysiology to Prevention and Treatment Strategies. Circulation 2021, 144, 728–745. [Google Scholar] [CrossRef]
- Aldea, G.S.; Bakaeen, F.G.; Pal, J.; Fremes, S.; Head, S.J.; Sabik, J.; Rosengart, T.; Kappetein, A.P.; Thourani, V.H.; Firestone, S.; et al. The Society of Thoracic Surgeons Clinical Practice Guidelines on Arterial Conduits for Coronary Artery Bypass Grafting. Ann. Thorac. Surg. 2016, 101, 801–809. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gaudino, M.; Benedetto, U.; Fremes, S.; Ballman, K.; Biondi-Zoccai, G.; Sedrakyan, A.; Nasso, G.; Raman, J.; Buxton, B.; Hayward, P.A.; et al. Association of Radial Artery Graft vs. Saphenous Vein Graft With Long-term Cardiovascular Outcomes Among Patients Undergoing Coronary Artery Bypass Grafting: A Systematic Review and Meta-analysis. JAMA 2020, 324, 179–187. [Google Scholar] [CrossRef]
- Gaudino, M.F.L.; Leonard, J.R.; Taggart, D.P. Lessons learned from Radial Artery Database International ALliance (RADIAL). Ann. Cardiothorac. Surg. 2018, 7, 598–603. [Google Scholar] [CrossRef] [Green Version]
- Ireland SfCSiGBa. 7th Cardiac Surgery Blue Book. Available online: https://scts.org/professionals/reports/resources/default.aspx (accessed on 17 February 2023).
- Zakkar, M.; Luong, L.A.; Chaudhury, H.; Ruud, O.; Punjabi, P.P.; Anderson, J.R.; Mullholand, J.W.; Clements, A.T.; Krams, R.; Foin, N. Dexamethasone arterializes venous endothelial cells by inducing mitogen-activated protein kinase phosphatase-1: A novel antiinflammatory treatment for vein grafts? Circulation 2011, 123, 524–532. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saunders, P.C.; Pintucci, G.; Bizekis, C.S.; Sharony, R.; Hyman, K.M.; Saponara, F.; Baumann, F.G.; Grossi, E.A.; Colvin, S.B.; Mignatti, P.; et al. Vein graft arterialization causes differential activation of mitogen-activated protein kinases. J. Thorac. Cardiovasc. Surg. 2004, 127, 1276–1284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, G.J.; Johnson, T.W.; Chamberlain, M.H.; Rizvi, S.I.; Wyatt, M.; George, S.J.; Angelini, G.D.; Karsch, K.R.; Oberhoff, M.; Newby, A.C. Short- and long-term effects of cytochalasin D, paclitaxel and rapamycin on wall thickening in experimental porcine vein grafts. Cardiovasc. Res. 2007, 73, 607–617. [Google Scholar] [CrossRef]
- Harskamp, R.E.; Alexander, J.H.; Schulte, P.J.; Brophy, C.M.; Mack, M.J.; Peterson, E.D.; Williams, J.B.; Gibson, C.M.; Califf, R.M.; Kouchoukos, N.T. Vein graft preservation solutions, patency, and outcomes after coronary artery bypass graft surgery: Follow-up from the PREVENT IV randomized clinical trial. JAMA Surg. 2014, 149, 798–805. [Google Scholar] [CrossRef]
- Komarova, Y.A.; Kruse, K.; Mehta, D.; Malik, A.B. Protein Interactions at Endothelial Junctions and Signaling Mechanisms Regulating Endothelial Permeability. Circ. Res. 2017, 120, 179–206. [Google Scholar] [CrossRef] [Green Version]
- Narula, J.; Chandrashekhar, Y.; Ahmadi, A.; Abbara, S.; Berman, D.S.; Blankstein, R.; Leipsic, J.; Newby, D.; Nicol, E.D.; Nieman, K.; et al. SCCT 2021 Expert Consensus Document on Coronary Computed Tomographic Angiography: A Report of the Society of Cardiovascular Computed Tomography. J. Cardiovasc. Comput. Tomogr. 2021, 15, 192–217. [Google Scholar] [CrossRef]
- de Winter, R.W.; Rahman, M.S.; van Diemen, P.A.; Schumacher, S.P.; Jukema, R.A.; Somsen, Y.B.O.; van Rossum, A.C.; Verouden, N.J.; Danad, I.; Delewi, R.; et al. Diagnostic and Management Strategies in Patients with Late Recurrent Angina after Coronary Artery Bypass Grafting. Curr. Cardiol. Rep. 2022, 24, 1309–1325. [Google Scholar] [CrossRef] [PubMed]
- Angelini, G.D.; Johnson, T.; Culliford, L.; Murphy, G.; Ashton, K.; Harris, T.; Edwards, J.; Clayton, G.; Kim, Y.; Newby, A.C.; et al. Comparison of alternate preparative techniques on wall thickness in coronary artery bypass grafts: The HArVeST randomized controlled trial. J. Card. Surg. 2021, 36, 1985–1995. [Google Scholar] [CrossRef]
- Adlam, D.; Antoniades, C.; Lee, R.; Diesch, J.; Shirodaria, C.; Taggart, D.; Leeson, P.; Channon, K.M. OCT characteristics of saphenous vein graft atherosclerosis. JACC Cardiovasc. Imaging 2011, 4, 807–809. [Google Scholar] [CrossRef] [Green Version]
- Lopes, R.D.; Hafley, G.E.; Allen, K.B.; Ferguson, T.B.; Peterson, E.D.; Harrington, R.A.; Mehta, R.H.; Gibson, C.M.; Mack, M.J.; Kouchoukos, N.T.; et al. Endoscopic versus open vein-graft harvesting in coronary-artery bypass surgery. N. Engl. J. Med. 2009, 361, 235–244. [Google Scholar] [CrossRef]
- Krishnamoorthy, B.; Critchley, W.R.; Thompson, A.J.; Payne, K.; Morris, J.; Venkateswaran, R.V.; Caress, A.L.; Fildes, J.E.; Yonan, N. Study comparing vein integrity and clinical outcomes in open vein harvesting and 2 types of endoscopic vein harvesting for coronary artery bypass grafting: The VICO randomized clinical trial (vein integrity and clinical outcomes). Circulation 2017, 136, 1688–1702. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Souza, D. A new no-touch preparation technique: Technical notes. Scand. J. Thorac. Cardiovasc. Surg. 1996, 30, 41–44. [Google Scholar] [CrossRef] [PubMed]
- De Vries, M.R.; Simons, K.H.; Jukema, J.W.; Braun, J.; Quax, P.H. Vein graft failure: From pathophysiology to clinical outcomes. Nat. Rev. Cardiol. 2016, 13, 451–470. [Google Scholar] [CrossRef] [PubMed]
- Dreifaldt, M.; Souza, D.S.; Loesch, A.; Muddle, J.R.; Karlsson, M.G.; Filbey, D.; Bodin, L.; Norgren, L.; Dashwood, M.R. The “no-touch” harvesting technique for vein grafts in coronary artery bypass surgery preserves an intact vasa vasorum. J. Thorac. Cardiovasc. Surg. 2011, 141, 145–150. [Google Scholar] [CrossRef] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Study Design | Patient Population | Total Number of Vein Samples Studied | LSV Harvest Method | Control Solution | Intervention Solution(s) | Additional Intervention(s) | Assessing | Primary Outcome(s) | Secondary Outcome |
|---|---|---|---|---|---|---|---|---|---|---|
| Chen et al. [11] | Single centre, randomised cohort study | 21 | 162 | Open and endoscopic | Normal saline | Heparinized whole blood | Time of solution exposure | Endothelial integrity | Staining of endothelial dependent markers | Oxidative stress |
| Dumanski et al. [12] | Single centre, prospective cohort study | 48 | 144 | No information provided. | Normal saline | Heparinized whole blood | Distention pressure | Endothlial integrity | Staining of endothelial dependent markers | Nil |
| Evans et al. [13] | Single centre, prospective cohort study | 14 | 70 | Open | Normal saline | Eurocollins, University of Wisconsin, Pyruvate | Nil | Endothelial integrity | Endothelial apoptosis | Nil |
| Gundry et al. [14] | Single centre, prospective cohort study | 30 | 35 | “Gentle dissection” | Heparinized Normal saline | Heparinized whole blood | Temperature and distention pressure | Endothelial integrity | Composite score of endothelial morphology | Nil |
| Hickethier et al. [15] | Single centre, prospective cohort study | 6 | Unknown | Open, no-touch | Normal saline | Buffered cell culture solution with albumin | Nil | Endothelial integrity | Endothelail monolayer integrity | Staining of endothelial dependent markers |
| Kocailik et al. [16] | Single centre, randomised cohort study | 80 | 80 | Open, no-touch | Normal saline | Papaverine | Time of solution exposure | Endothelial function | Endothelial dependent wall relaxation | Nil |
| Kurusz et al. [17] | Single centre, prospective cohort study | 5 | 25 | No information provided. | Normal saline | Heparinized whole blood, Custom cardioplegia solution | Temperature and distention pressure | Endothelial integrity | Endothelail monolayer integrity | Nil |
| Perrault et al. [18] | Multi centre, blinded, randomised control trial | 125 | 250 | Open and endoscopic | Heparinized Normal saline | Duragraft | Proximal vs. distal position in vessel | Endothelial integrity | Wall thickness | Nil |
| Pimentel et al. [19] | Single centre, prospective cohort study | 12 | 42 | Open | Normal saline | Heparinized whole blood | Distention Pressure | Endothelial integrity | Composite score of endothelial morphology | Nil |
| Tekin et al. [20] | Single centre, prospective cohort study | 50 | 150 | “Standard hospital protocol” | Normal saline | Heparinized whole blood, Duragraft | Nil | Endothelial integrity | Oxidative stress index and total antioxidant status | Nil |
| Toto et al. [21] | Single centre, prospective cohort study | 12 | 72 | Open | Normal saline | Heparinized whole blood, Duragraft | Time of solution exposure | Endothelial integrity | Endothelial cell apoptosis | Nil |
| Wilbring et al. (2011) [22] | Single centre, prospective cohort study | Unknown | 19 | Open | Normal saline | TiProtec | Nil | Endothelial function | Endothelial dependent wall relaxation | Vasodilation |
| Wilbring et al. (2013) [23] | Single centre, prospective cohort study | 19 | 38 | Open | Normal saline | TiProtec | Time of solution exposure | Endothelial function | Endothelial dependent wall relaxation | Nil |
| Solution | Components | Additive Concentration(s) [mmol/L] if Applicable | Osmolality |
|---|---|---|---|
| Normal saline | Salt solution | 154 sodium chloride | 308 [mosmol/L] |
| Heparinized whole blood | Autologous whole blood with heparin sodium | Variable heparin sodium dosage dependent on local preferences | 289 ± 3–302 ± 5 [mmol/kg] |
| DuraGraft (Somahlution Inc., Jupiter, FL, USA) | Physiological salt solution with additives | Not reported publically. | Not reported publically. |
| TiProtec (Kohler Chemie, Germany) | Salt solution with additives | 14 sodium chloride, 73 potassium chloride, 8 magnesium chloride, 1 Disodium hydrogen phosphate, 0.05 Calcium chloride • 2 H2O, 30 N-acetyl histidine • H2O, 2 Tryptophan, 2 α-Ketuglutaric acid, 5 Asparagine acid, 10 Glycine, 5 Alanine, 20 Sucrose, 10 Glucose monohydrate, 0.1 Deferoxamine mesylate, 0.02 3,4-Dimethoxy-N-methylbenzohydroxamic acid | 307 [mosmol/L] |
| EuroCollins (Baxter Healthcare, Old Toongabbie NSW, Australia) | Physiological salt solution with additives | 0.11 potassium dihydrogen phosphate, 0.54 Dipotassium hydrogen phosphate trihydrate, 0.06 potassium chloride, 0.05 sodium bicarbonate, 0.006 procaine hydrochloride, 195 glucose, | 375 [mosmol/L] |
| University of Wisconsin (Belzer UW, Bridge to Life, Northbrook, IL, USA) | Salt solution with additives | Pentafraction, 1.99 Lactobionic Acid (as Lactone), 0.19 Potassium Phosphate monobasic, 0.07 Magnesium Sulfate heptahydrate, 0.97 Raffinose pentahydrate, 0.07 Adenosine, 0.01 Allopurinol, 0.05 Total Glutathione, 0.31 Potassium Hydroxide, Sodium Hydroxide/Hydrochloric Acid to adjust to pH 7.4 | 320 [mosmol/L] |
| Pyruvate | Supplement for cell culture medium | 100 Sodium Pyruvate | 165–205 [mosmol/L] |
| Medium 199 with HEPES (Thermo Fisher Scientific, Inc., Waltham, MA, USA) | Buffered cell culture medium | 0.67 Glycine, 0.28 L-Alanine, 0.33 L-Arginine hydrochloride, 0.23 L-Aspartic acid, 5.68 L-Cysteine hydrochloride-H2O, 0.11 L-Cystine 2HCl, 0.51 L-Glutamic Acid, 0.68 L-Glutamine, 0.10 L-Histidine hydrochloride-H2O, 0.08 L-Hydroxyproline, 0.31 L-Isoleucine, 0.46 L-Leucine, 0.38 L-Lysine hydrochloride, 0.10 L-Methionine, 0.15 L-Phenylalanine, 0.35 L-Proline, 0.24 L-Serine, 0.25 L-Threonine, 0.05 L-Tryptophan, 0.22 L-Tyrosine disodium salt dihydrate, 0.21 L-Valine, 2.84 × 10−4 Ascorbic Acid, 4.09 × 10−5 Biotin, 0.003 Choline chloride, 2.1 × 10−5 D-Calcium pantothenate, 2.27 Folic Acid, 5.81 Menadione (Vitamin K3), 2.05 Niacinamide, 2.03 Nicotinic acid (Niacin), 3.65 × 10−4 Para-Aminobenzoic Acid, 1.23 × 10−4 Pyridoxal hydrochloride, 1.21 × 10−4 Pyridoxine hydrochloride, 2.66 × 10−5 Riboflavin, 2.97 × 10−5 Thiamine hydrochloride, 3.05 × 10−4 Vitamin A (acetate), 2.52 × 10−4 Vitamin D2 (Calciferol), 1.80 alpha Tocopherol phos. Na salt, 2.78 × 10−4 i-Inositol, 1.80 Calcium Chloride (CaCl2) (anhyd.), 0.001 Ferric nitrate (Fe(NO3)-9H2O), 0.81 Magnesium Sulfate (MgSO4) (anhyd.), 5.33 Potassium Chloride (KCl), 26.19 Sodium Bicarbonate (NaHCO3), 105.17 Sodium Chloride (NaCl), 1.01 Sodium Phosphate monobasic (NaH2PO4) anhydrous, 0.003 2-deoxy-D-ribose, 0.02 Adenine sulfate, 5.76 Adenosine 5′-phosphate, 0.001 Adenosine 5′-triphosphate, 5.17 × 10−4 Cholesterol, 5.56 D-Glucose (Dextrose), 1.63 Glutathione (reduced), 0.001 Guanine hydrochloride, 25.04 HEPES, 0.002 Hypoxanthine Na, 0.05 Phenol Red, 0.003 Ribose, 0.61 odium Acetate, 0.002 Thymine, Tween 80®, 0.002 Uracil, 0.002 Xanthine-Na | 270–330 [mmol/kg] |
| Customised cardiplegia | 140 sodium, 25 potassium, 3 magnesium, 104 chlorine, 27 acetate, 23 gluconate, 1.36 calcium, 23 bicarbonate radical | 300 [mosmol/L] | |
| Papaverine | Papaverine in 0.9% sodium chloride | 2.95 × 10−6 Papaverine, 154 Sodium chloride | Unknown |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Layton, G.R.; Ladak, S.S.; Abbasciano, R.; McQueen, L.W.; George, S.J.; Murphy, G.J.; Zakkar, M. The Role of Preservation Solutions upon Saphenous Vein Endothelial Integrity and Function: Systematic Review and UK Practice Survey. Cells 2023, 12, 815. https://doi.org/10.3390/cells12050815
Layton GR, Ladak SS, Abbasciano R, McQueen LW, George SJ, Murphy GJ, Zakkar M. The Role of Preservation Solutions upon Saphenous Vein Endothelial Integrity and Function: Systematic Review and UK Practice Survey. Cells. 2023; 12(5):815. https://doi.org/10.3390/cells12050815
Chicago/Turabian StyleLayton, Georgia R., Shameem S. Ladak, Riccardo Abbasciano, Liam W. McQueen, Sarah J. George, Gavin J. Murphy, and Mustafa Zakkar. 2023. "The Role of Preservation Solutions upon Saphenous Vein Endothelial Integrity and Function: Systematic Review and UK Practice Survey" Cells 12, no. 5: 815. https://doi.org/10.3390/cells12050815