
Circulating miR-451a Expression May Predict Recurrence in Atrial Fibrillation Patients after Catheter Pulmonary Vein Ablation
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. AF Assessment
2.3. Description of the Surgery Intervention and Sample Collection
2.4. Ablation Procedure, Definition of Scar Percentage and Patient Follow-Up
2.5. RNA Extraction and miRNA Quantification
2.6. MicroRNA Pathway Analysis and Target Prediction
2.7. Statistical Analysis
3. Results
3.1. Baseline Characteristics
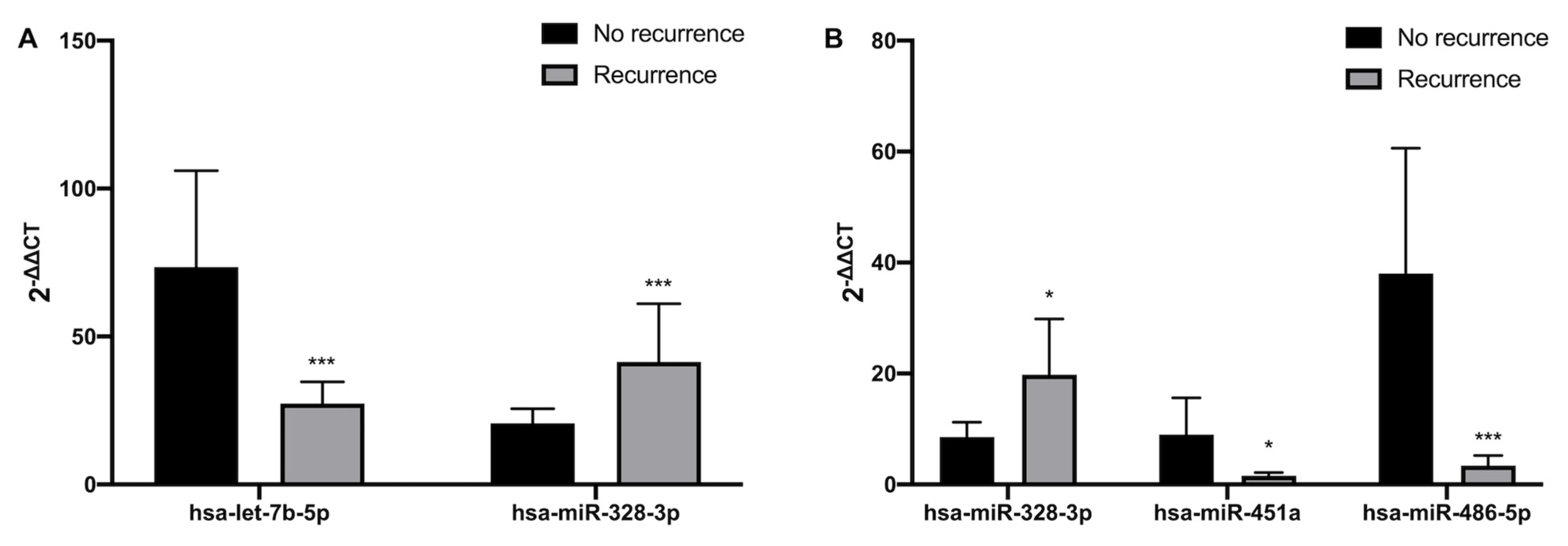
3.2. Differential Expression of microRNAs in No-Recurrence vs. Recurrence Patients
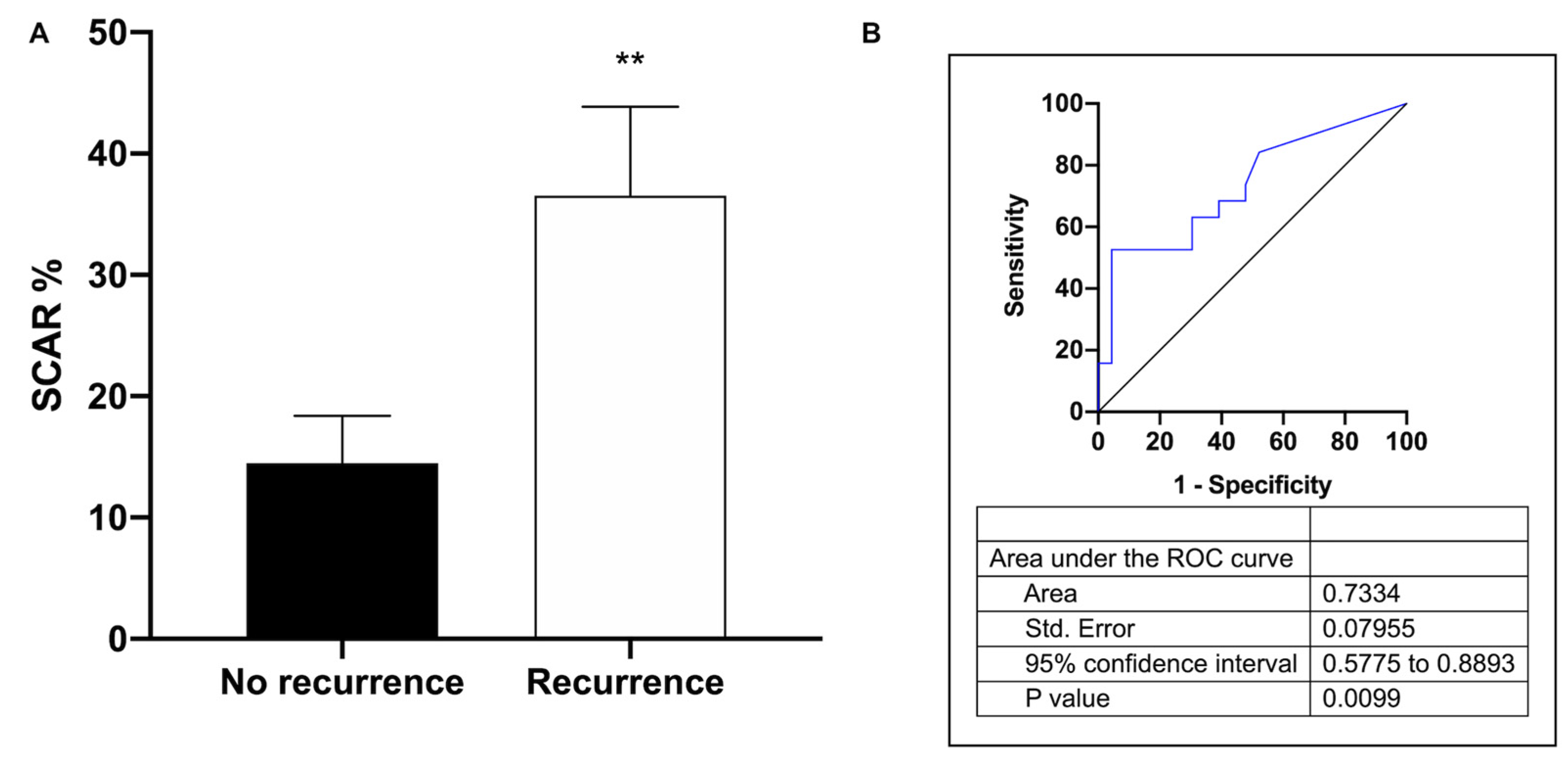
3.3. Association between miR-451a Expression, Scar Percentage and AF Recurrence
3.4. KEGG Pathways and Prediction Targets
4. Discussion
4.1. Background
4.2. AF Patients
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Go, A.S.; Hylek, E.M.; Phillips, K.A.; Chang, Y.; Henault, L.E.; Selby, J.V.; Singer, D.E. Prevalence of Diagnosed Atrial Fibrillation in Adults: National Implications for Rhythm Management and Stroke Prevention: The AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA 2001, 285, 2370–2375. [Google Scholar] [CrossRef] [PubMed]
- Heeringa, J.; van der Kuip, D.A.M.; Hofman, A.; Kors, J.A.; van Herpen, G.; Stricker, B.H.C.; Stijnen, T.; Lip, G.Y.H.; Witteman, J.C.M. Prevalence, Incidence and Lifetime Risk of Atrial Fibrillation: The Rotterdam Study. Eur. Heart J. 2006, 27, 949–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Michaud, G.F.; Stevenson, W.G. Atrial Fibrillation. N. Engl. J. Med. 2021, 384, 353–361. [Google Scholar] [CrossRef] [PubMed]
- Kotalczyk, A.; Lip, G.Y.; Calkins, H. The 2020 ESC Guidelines on the Diagnosis and Management of Atrial Fibrillation. Arrhythm. Electrophysiol. Rev. 2021, 10, 65–67. [Google Scholar] [CrossRef]
- Benjamin, E.J.; Wolf, P.A.; D’Agostino, R.B.; Silbershatz, H.; Kannel, W.B.; Levy, D. Impact of Atrial Fibrillation on the Risk of Death: The Framingham Heart Study. Circulation 1998, 98, 946–952. [Google Scholar] [CrossRef] [Green Version]
- Conen, D.; Chae, C.U.; Glynn, R.J.; Tedrow, U.B.; Everett, B.M.; Buring, J.E.; Albert, C.M. Risk of Death and Cardiovascular Events in Initially Healthy Women with New-Onset Atrial Fibrillation. JAMA 2011, 305, 2080–2087. [Google Scholar] [CrossRef] [Green Version]
- Soliman, E.Z.; Safford, M.M.; Muntner, P.; Khodneva, Y.; Dawood, F.Z.; Zakai, N.A.; Thacker, E.L.; Judd, S.; Howard, V.J.; Howard, G.; et al. Atrial Fibrillation and the Risk of Myocardial Infarction. JAMA Int. Med. 2014, 174, 107–114. [Google Scholar] [CrossRef]
- Chamberlain, A.M.; Gersh, B.J.; Alonso, A.; Chen, L.Y.; Berardi, C.; Manemann, S.M.; Killian, J.M.; Weston, S.A.; Roger, V.L. Decade-Long Trends in Atrial Fibrillation Incidence and Survival: A Community Study. Am. J. Med. 2015, 128, 260–267.e1. [Google Scholar] [CrossRef] [Green Version]
- Cambeiro, G.; Cristina, M.; Mañero, R.; Moisés; Roubin, R.; Assi, A.; Emad; Sergio; Juanatey, G.; Ramón, J. Review Of Obesity And Atrial Fibrillation: Exploring The Paradox. J. Atr. Fibrillation 2015, 8, 1259. [Google Scholar] [CrossRef]
- Kornej, J.; Börschel, C.S.; Benjamin, E.J.; Schnabel, R.B. Epidemiology of Atrial Fibrillation in the 21st Century: Novel Methods and New Insights. Circ. Res. 2020, 127, 4–20. [Google Scholar] [CrossRef]
- El-Battrawy, I.; Lang, S.; Ansari, U.; Behnes, M.; Hillenbrand, D.; Schramm, K.; Fastner, C.; Zhou, X.; Bill, V.; Hoffmann, U.; et al. Impact of Concomitant Atrial Fibrillation on the Prognosis of Takotsubo Cardiomyopathy. Europace 2017, 19, 1288–1292. [Google Scholar] [CrossRef] [PubMed]
- El-Battrawy, I.; Cammann, V.L.; Kato, K.; Szawan, K.A.; di Vece, D.; Rossi, A.; Wischnewsky, M.; Hermes-Laufer, J.; Gili, S.; Citro, R.; et al. Impact of Atrial Fibrillation on Outcome in Takotsubo Syndrome: Data From the International Takotsubo Registry. J. Am. Heart Assoc. 2021, 10, e014059. [Google Scholar] [CrossRef]
- Mitrić, G.; Udy, A.; Bandeshe, H.; Clement, P.; Boots, R. Variable Use of Amiodarone Is Associated with a Greater Risk of Recurrence of Atrial Fibrillation in the Critically Ill. Crit. Care 2016, 20, 90. [Google Scholar] [CrossRef] [Green Version]
- Zhou, S.S.; Jin, J.P.; Wang, J.Q.; Zhang, Z.G.; Freedman, J.H.; Zheng, Y.; Cai, L. MiRNAS in Cardiovascular Diseases: Potential Biomarkers, Therapeutic Targets and Challenges. Acta. Pharmacol. Sin. 2018, 39, 1073–1084. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marfella, R.; di Filippo, C.; Potenza, N.; Sardu, C.; Rizzo, M.R.; Siniscalchi, M.; Musacchio, E.; Barbieri, M.; Mauro, C.; Mosca, N.; et al. Circulating MicroRNA Changes in Heart Failure Patients Treated with Cardiac Resynchronization Therapy: Responders vs. Non-Responders. Eur. J. Heart Fail. 2013, 15, 1277–1288. [Google Scholar] [CrossRef] [PubMed]
- Noszczyk-Nowak, A.; Zacharski, M.; Michałek, M. Screening for Circulating MiR-208a and -b in Different Cardiac Arrhythmias of Dogs. J. Vet. Res. 2018, 62, 359–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiao, G.; Xia, D.; Cheng, Z.; Zhang, G. MiR-132 in Atrial Fibrillation Directly Targets Connective Tissue Growth Factor. Mol. Med. Rep. 2017, 16, 4143–4150. [Google Scholar] [CrossRef] [Green Version]
- Viereck, J.; Thum, T. Circulating Noncoding RNAs as Biomarkers of Cardiovascular Disease and Injury. Circ. Res. 2017, 120, 381–399. [Google Scholar] [CrossRef] [Green Version]
- Sygitowicz, G.; Maciejak-Jastrzębska, A.; Sitkiewicz, D. A Review of the Molecular Mechanisms Underlying Cardiac Fibrosis and Atrial Fibrillation. J. Clin. Med. 2021, 10, 4430. [Google Scholar] [CrossRef]
- Zhang, L.; Wang, X.; Huang, C. A Narrative Review of Non-Coding RNAs in Atrial Fibrillation: Potential Therapeutic Targets and Molecular Mechanisms. Ann. Transl. Med. 2021, 9, 1486. [Google Scholar] [CrossRef]
- Kiyosawa, N.; Watanabe, K.; Morishima, Y.; Yamashita, T.; Yagi, N.; Arita, T.; Otsuka, T.; Suzuki, S. Exploratory Analysis of Circulating MiRNA Signatures in Atrial Fibrillation Patients Determining Potential Biomarkers to Support Decision-Making in Anticoagulation and Catheter Ablation. Int. J. Mol. Sci. 2020, 21, 2444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhou, Q.; Maleck, C.; von Ungern-Sternberg, S.N.I.; Neupane, B.; Heinzmann, D.; Marquardt, J.; Duckheim, M.; Scheckenbach, C.; Stimpfle, F.; Gawaz, M.; et al. Circulating MicroRNA-21 Correlates with Left Atrial Low-Voltage Areas and Is Associated With Procedure Outcome in Patients Undergoing Atrial Fibrillation Ablation. Circ. Arrhythm. Electrophysiol. 2018, 11, e006242. [Google Scholar] [CrossRef]
- Van Tran, K.; Majka, J.; Sanghai, S.; Sardana, M.; Lessard, D.; Milstone, Z.; Tanriverdi, K.; Freedman, J.E.; Fitzgibbons, T.P.; McManus, D. Micro-RNAs Are Related to Epicardial Adipose Tissue in Participants with Atrial Fibrillation: Data From the MiRhythm Study. Front. Cardiovasc. Med. 2019, 6, 115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hao, H.; Dai, C.; Han, X.; Li, Y. A Novel Therapeutic Strategy for Alleviating Atrial Remodeling by Targeting Exosomal MiRNAs in Atrial Fibrillation. Biochim. Biophys. Acta Mol. Cell Res. 2022, 1869, 119365. [Google Scholar] [CrossRef] [PubMed]
- McManus, D.D.; Lin, H.; Tanriverdi, K.; Quercio, M.; Yin, X.; Larson, M.G.; Ellinor, P.T.; Levy, D.; Freedman, J.E.; Benjamin, E.J. Relations between Circulating MicroRNAs and Atrial Fibrillation: Data from the Framingham Offspring Study. Heart Rhythm 2014, 11, 663–669. [Google Scholar] [CrossRef] [Green Version]
- Luo, X.; Yang, B.; Nattel, S. MicroRNAs and Atrial Fibrillation: Mechanisms and Translational Potential. Nat. Rev. Cardiol. 2015, 12, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Barwari, T.; Joshi, A.; Mayr, M. MicroRNAs in Cardiovascular Disease. J. Am. Coll. Cardiol. 2016, 68, 2577–2584. [Google Scholar] [CrossRef] [Green Version]
- Shaihov-Teper, O.; Ram, E.; Ballan, N.; Brzezinski, R.Y.; Naftali-Shani, N.; Masoud, R.; Ziv, T.; Lewis, N.; Schary, Y.; Levin-Kotler, L.P.; et al. Extracellular Vesicles From Epicardial Fat Facilitate Atrial Fibrillation. Circulation 2021, 143, 2475–2493. [Google Scholar] [CrossRef]
- Gryshkova, V.; Lushbough, I.; Palmer, J.; Burrier, R.; Delaunois, A.; Donley, E.; Valentin, J.P. MicroRNAs Signatures as Potential Biomarkers of Structural Cardiotoxicity in Human-Induced Pluripotent Stem-Cell Derived Cardiomyocytes. Arch. Toxicol. 2022, 96, 2033–2047. [Google Scholar] [CrossRef]
- Esfandyari, D.; Idrissou, B.M.G.; Hennis, K.; Avramopoulos, P.; Dueck, A.; El-Battrawy, I.; Grüter, L.; Meier, M.A.; Näger, A.C.; Ramanujam, D.; et al. MicroRNA-365 Regulates Human Cardiac Action Potential Duration. Nat. Commun. 2022, 13, 220. [Google Scholar] [CrossRef]
- da Silva, A.M.G.; de Araújo, J.N.G.; de Freitas, R.C.C.; Silbiger, V.N. Circulating MicroRNAs as Potential Biomarkers of Atrial Fibrillation. Biomed Res Int 2017, 2017, 7804763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marques, F.Z.; Vizi, D.; Khammy, O.; Mariani, J.A.; Kaye, D.M. The Transcardiac Gradient of Cardio-MicroRNAs in the Failing Heart. Eur. J. Heart Fail. 2016, 18, 1000–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Rosa, S.; Eposito, F.; Carella, C.; Strangio, A.; Ammirati, G.; Sabatino, J.; Abbate, F.G.; Iaconetti, C.; Liguori, V.; Pergola, V.; et al. Transcoronary Concentration Gradients of Circulating MicroRNAs in Heart Failure. Eur. J. Heart Fail. 2018, 20, 1000–1010. [Google Scholar] [CrossRef] [PubMed]
- Estephan, L.E.; Genuardi, M.V.; Kosanovich, C.M.; Risbano, M.G.; Zhang, Y.; Petro, N.; Watson, A.; al Aaraj, Y.; Sembrat, J.C.; Rojas, M.; et al. Distinct Plasma Gradients of MicroRNA-204 in the Pulmonary Circulation of Patients Suffering from WHO Groups I and II Pulmonary Hypertension. Pulm. Circ. 2019, 9, 2045894019840646. [Google Scholar] [CrossRef] [Green Version]
- Soeki, T.; Matsuura, T.; Bando, S.; Tobiume, T.; Uematsu, E.; Ise, T.; Kusunose, K.; Yamaguchi, K.; Yagi, S.; Fukuda, D.; et al. Relationship between Local Production of MicroRNA-328 and Atrial Substrate Remodeling in Atrial Fibrillation. J. Cardiol. 2016, 68, 472–477. [Google Scholar] [CrossRef] [Green Version]
- López-Canoa, J.N.; Couselo-Seijas, M.; Baluja, A.; González-Melchor, L.; Rozados, A.; Llorente-Cortés, V.; de Gonzalo-Calvo, D.; Guerra, J.M.; Vilades, D.; Leta, R.; et al. Sex-Related Differences of Fatty Acid-Binding Protein 4 and Leptin Levels in Atrial Fibrillation. Europace 2021, 23, 682–690. [Google Scholar] [CrossRef]
- López-Canoa, J.N.; Couselo-Seijas, M.; González-Ferrero, T.; Almengló, C.; Álvarez, E.; González-Maestro, A.; González-Melchor, L.; Martínez-Sande, J.L.; García-Seara, J.; Fernández-López, J.; et al. The Role of Fatty Acid-Binding Protein 4 in the Characterization of Atrial Fibrillation and the Prediction of Outcomes after Catheter Ablation. Int. J. Mol. Sci. 2022, 23, 11107. [Google Scholar] [CrossRef] [PubMed]
- Moscoso, I.; Cebro-Márquez, M.; Martínez-Gómez, Á.; Abou-Jokh, C.; Martínez-Monzonís, M.A.; Martínez-Sande, J.L.; González-Melchor, L.; García-Seara, J.; Fernández-López, X.A.; Moraña-Fernández, S.; et al. Circulating MiR-499a and MiR-125b as Potential Predictors of Left Ventricular Ejection Fraction Improvement after Cardiac Resynchronization Therapy. Cells 2022, 11, 271. [Google Scholar] [CrossRef] [PubMed]
- Ahmed-Jushuf, F.; Murgatroyd, F.; Dhillon, P.; Scott, P.A. The Impact of the Presence of Left Atrial Low Voltage Areas on Outcomes from Pulmonary Vein Isolation. J. Arrhythm. 2019, 35, 205–214. [Google Scholar] [CrossRef]
- McManus, D.D.; Tanriverdi, K.; Lin, H.; Esa, N.; Kinno, M.; Mandapati, D.; Tam, S.; Okike, O.N.; Ellinor, P.T.; Keaney, J.F.; et al. Plasma MicroRNAs Are Associated with Atrial Fibrillation and Change after Catheter Ablation (the MiRhythm Study). Heart Rhythm 2015, 12, 3–10. [Google Scholar] [CrossRef] [Green Version]
- van den Berg, N.W.E.; Kawasaki, M.; Berger, W.R.; Neefs, J.; Meulendijks, E.; Tijsen, A.J.; de Groot, J.R. MicroRNAs in Atrial Fibrillation: From Expression Signatures to Functional Implications. Cardiovasc. Drugs Ther. 2017, 31, 345–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Geurts, S.; Mens, M.M.J.; Bos, M.M.; Arfan Ikram, M.; Ghanbari, M.; Kavousi, M. Circulatory MicroRNAs in Plasma and Atrial Fibrillation in the General Population: The Rotterdam Study. Genes 2021, 13, 11. [Google Scholar] [CrossRef]
- Komal, S.; Yin, J.J.; Wang, S.H.; Huang, C.Z.; Tao, H.L.; Dong, J.Z.; Han, S.N.; Zhang, L.R. MicroRNAs: Emerging Biomarkers for Atrial Fibrillation. J. Cardiol. 2019, 74, 475–482. [Google Scholar] [CrossRef]
- Zhang, X.; Xiao-Ping, X.; Xu-Ai, R.; Cui, T. Plasma MiRNA-155 Levels Predict Atrial Fibrillation Recurrence after Cardioversion. Heart Surg. Forum 2019, 22, E140–E148. [Google Scholar] [CrossRef] [Green Version]
- Xu, L.; Tian, L.; Yan, Z.; Wang, J.; Xue, T.; Sun, Q. Diagnostic and Prognostic Value of MiR-486-5p, MiR-451a, MiR-21-5p and Monocyte to High-Density Lipoprotein Cholesterol Ratio in Patients with Acute Myocardial Infarction. Heart Vessel. 2022, 38, 318–331. [Google Scholar] [CrossRef] [PubMed]
- Wang, B.; Duan, X.; Xu, Q.; Li, Y. Diagnostic and Prognostic Significance of MiR-451a in Patients with Atherosclerosis. Vascular, 2021; online ahead of print. [Google Scholar] [CrossRef]
- Zeng, Z.; Wang, K.; Li, Y.; Xia, N.; Nie, S.; Lv, B.; Zhang, M.; Tu, X.; Li, Q.; Tang, T.; et al. Down-Regulation of MicroRNA-451a Facilitates the Activation and Proliferation of CD4+ T Cells by Targeting Myc in Patients with Dilated Cardiomyopathy. J. Biol. Chem. 2017, 292, 6004–6013. [Google Scholar] [CrossRef] [Green Version]
- Kuwabara, Y.; Horie, T.; Baba, O.; Watanabe, S.; Nishiga, M.; Usami, S.; Izuhara, M.; Nakao, T.; Nishino, T.; Otsu, K.; et al. MicroRNA-451 Exacerbates Lipotoxicity in Cardiac Myocytes and High-Fat Diet-Induced Cardiac Hypertrophy in Mice through Suppression of the LKB1/AMPK Pathway. Circ. Res. 2015, 116, 279–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, L.; Su, M.; Wang, S.; Zou, Y.; Wang, X.; Wang, Y.; Cui, H.; Zhao, P.; Hui, R.; Wang, J. MiR-451 Is Decreased in Hypertrophic Cardiomyopathy and Regulates Autophagy by Targeting TSC1. J. Cell Mol. Med. 2014, 18, 2266–2274. [Google Scholar] [CrossRef]
- Gan, M.; Zheng, T.; Shen, L.; Tan, Y.; Fan, Y.; Shuai, S.; Bai, L.; Li, X.; Wang, J.; Zhang, S.; et al. Genistein Reverses Isoproterenol-Induced Cardiac Hypertrophy by Regulating MiR-451/TIMP2. Biomed. Pharmacother. 2019, 112, 108618. [Google Scholar] [CrossRef]
- Scrimgeour, N.R.; Wrobel, A.; Pinho, M.J.; Høydal, M.A. MicroRNA-451a Prevents Activation of Matrix Metalloproteinases 2 and 9 in Human Cardiomyocytes during Pathological Stress Stimulation. Am. J. Physiol. Cell Physiol. 2020, 318, C94–C102. [Google Scholar] [CrossRef]
- Li, J.; Wan, W.; Chen, T.; Tong, S.; Jiang, X.; Liu, W. MiR-451 Silencing Inhibited Doxorubicin Exposure-Induced Cardiotoxicity in Mice. Biomed. Res. Int. 2019, 2019, 1528278. [Google Scholar] [CrossRef]
- Deng, H.Y.; He, Z.Y.; Dong, Z.C.; Zhang, Y.L.; Han, X.; Li, H.H. MicroRNA-451a Attenuates Angiotensin II-Induced Cardiac Fibrosis and Inflammation by Directly Targeting T-Box1. J. Physiol. Biochem. 2022, 78, 257–269. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.; Hu, X.; Yi, C.; Hu, G.; Zhou, X.; Jiang, H. MicroRNA-451 Protects against Cardiomyocyte Anoxia/Reoxygenation Injury by Inhibiting High Mobility Group Box 1 Expression. Mol. Med. Rep. 2016, 13, 5335–5341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Wang, X.; Zhu, H.; Zhu, C.; Wang, Y.; Pu, W.T.; Jegga, A.G.; Fan, G.C. Synergistic Effects of the GATA-4-Mediated MiR-144/451 Cluster in Protection against Simulated Ischemia/Reperfusion-Induced Cardiomyocyte Death. J. Mol. Cell Cardiol. 2010, 49, 841–850. [Google Scholar] [CrossRef] [Green Version]
- Li, S.; Lee, C.; Song, J.; Lu, C.; Liu, J.; Cui, Y.; Liang, H.; Cao, C.; Zhang, F.; Chen, H. Circulating MicroRNAs as Potential Biomarkers for Coronary Plaque Rupture. Oncotarget 2017, 8, 48145–48156. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiedmann, F.; Kraft, M.; Kallenberger, S.; Büscher, A.; Paasche, A.; Blochberger, P.L.; Seeger, T.; Jávorszky, N.; Warnecke, G.; Arif, R.; et al. MicroRNAs Regulate TASK-1 and Are Linked to Myocardial Dilatation in Atrial Fibrillation. J. Am. Heart Assoc. 2022, 11, e023472. [Google Scholar] [CrossRef]
- Girmatsion, Z.; Biliczki, P.; Bonauer, A.; Wimmer-Greinecker, G.; Scherer, M.; Moritz, A.; Bukowska, A.; Goette, A.; Nattel, S.; Hohnloser, S.H.; et al. Changes in MicroRNA-1 Expression and IK1 up-Regulation in Human Atrial Fibrillation. Heart Rhythm 2009, 6, 1802–1809. [Google Scholar] [CrossRef]
- Harada, M.; Luo, X.; Murohara, T.; Yang, B.; Dobrev, D.; Nattel, S. MicroRNA Regulation and Cardiac Calcium Signaling: Role in Cardiac Disease and Therapeutic Potential. Circ. Res. 2014, 114, 689–705. [Google Scholar] [CrossRef] [Green Version]
- Luo, X.; Pan, Z.; Shan, H.; Xiao, J.; Sun, X.; Wang, N.; Lin, H.; Xiao, L.; Maguy, A.; Qi, X.-Y.; et al. MicroRNA-26 Governs Profibrillatory Inward-Rectifier Potassium Current Changes in Atrial Fibrillation. J. Clin. Investig. 2013, 123, 1939–1951. [Google Scholar] [CrossRef]
- Lu, Y.; Zhang, Y.; Wang, N.; Pan, Z.; Gao, X.; Zhang, F.; Zhang, Y.; Shan, H.; Luo, X.; Bai, Y.; et al. MicroRNA-328 Contributes to Adverse Electrical Remodeling in Atrial Fibrillation. Circulation 2010, 122, 2378–2387. [Google Scholar] [CrossRef]
- Ling, T.-Y.; Wang, X.-L.; Chai, Q.; Lau, T.-W.; Koestler, C.M.; Park, S.J.; Daly, R.C.; Greason, K.L.; Jen, J.; Wu, L.-Q.; et al. Regulation of the SK3 Channel by MicroRNA-499--Potential Role in Atrial Fibrillation. Heart Rhythm 2013, 10, 1001–1009. [Google Scholar] [CrossRef] [Green Version]
- Ellinor, P.T.; Lunetta, K.L.; Glazer, N.L.; Pfeufer, A.; Alonso, A.; Chung, M.K.; Sinner, M.F.; de Bakker, P.I.W.; Mueller, M.; Lubitz, S.A.; et al. Common Variants in KCNN3 Are Associated with Lone Atrial Fibrillation. Nat. Genet. 2010, 42, 240–244. [Google Scholar] [CrossRef]
- Adam, O.; Löhfelm, B.; Thum, T.; Gupta, S.K.; Puhl, S.-L.; Schäfers, H.-J.; Böhm, M.; Laufs, U. Role of MiR-21 in the Pathogenesis of Atrial Fibrosis. Basic Res. Cardiol. 2012, 107, 278. [Google Scholar] [CrossRef] [PubMed]
- Cardin, S.; Guasch, E.; Luo, X.; Naud, P.; le Quang, K.; Shi, Y.; Tardif, J.-C.; Comtois, P.; Nattel, S. Role for MicroRNA-21 in Atrial Profibrillatory Fibrotic Remodeling Associated with Experimental Postinfarction Heart Failure. Circ. Arrhythm. Electrophysiol. 2012, 5, 1027–1035. [Google Scholar] [CrossRef] [Green Version]
- Dawson, K.; Wakili, R.; Ordög, B.; Clauss, S.; Chen, Y.; Iwasaki, Y.; Voigt, N.; Qi, X.Y.; Sinner, M.F.; Dobrev, D.; et al. MicroRNA29: A Mechanistic Contributor and Potential Biomarker in Atrial Fibrillation. Circulation 2013, 127, 1466–1475. [Google Scholar] [CrossRef] [Green Version]
- Shan, H.; Zhang, Y.; Lu, Y.; Zhang, Y.; Pan, Z.; Cai, B.; Wang, N.; Li, X.; Feng, T.; Hong, Y.; et al. Downregulation of MiR-133 and MiR-590 Contributes to Nicotine-Induced Atrial Remodelling in Canines. Cardiovasc. Res. 2009, 83, 465–472. [Google Scholar] [CrossRef] [PubMed]
- Mun, D.; Kim, H.; Kang, J.; Park, H.; Park, H.; Lee, S.; Yun, N.; Joung, B. Expression of MiRNAs in Circulating Exosomes Derived from Patients with Persistent Atrial Fibrillation. FASEB J. 2019, 33, 5979–5989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huang, H.; Chen, H.; Liang, X.; Chen, X.; Chen, X.; Chen, C. Upregulated MiR-328-3p and Its High Risk in Atrial Fibrillation: A Systematic Review and Meta-Analysis with Meta-Regression. Medicine 2022, 101, e28980. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Meng, X.; Han, J.; Li, Y.; Luo, T.; Wang, J.; Xin, M.; Xi, J. Differential Expressions of MiRNAs in Patients with Nonvalvular Atrial Fibrillation. Zhonghua Yi Xue Za Zhi 2012, 92, 1816–1819. [Google Scholar] [PubMed]
- Liu, Y.; Luo, D.; Liu, E.; Liu, T.; Xu, G.; Liang, X.; Yuan, M.; Zhang, Y.; Chen, X.; Chen, X.; et al. MiRNA21 and IL-18 Levels in Left Atrial Blood in Patients with Atrial Fibrillation Undergoing Cryoablation and Their Predictive Value for Recurrence of Atrial Fibrillation. J. Interv. Card. Electrophysiol. 2022, 64, 111–120. [Google Scholar] [CrossRef]
- Nattel, S.; Harada, M. Atrial Remodeling and Atrial Fibrillation: Recent Advances and Translational Perspectives. J. Am. Coll. Cardiol. 2014, 63, 2335–2345. [Google Scholar] [CrossRef] [Green Version]
- Nattel, S. Molecular and Cellular Mechanisms of Atrial Fibrosis in Atrial Fibrillation. JACC Clin. Electrophysiol. 2017, 3, 425–435. [Google Scholar] [CrossRef]
- Friedrichs, K.; Baldus, S.; Klinke, A. Fibrosis in Atrial Fibrillation—Role of Reactive Species and MPO. Front. Physiol. 2012, 3, 214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Anné, W.; Willems, R.; Roskams, T.; Sergeant, P.; Herijgers, P.; Holemans, P.; Ector, H.; Heidbüchel, H. Matrix Metalloproteinases and Atrial Remodeling in Patients with Mitral Valve Disease and Atrial Fibrillation. Cardiovasc. Res. 2005, 67, 655–666. [Google Scholar] [CrossRef] [Green Version]
- Lewkowicz, J.; Knapp, M.; Tankiewicz-Kwedlo, A.; Sawicki, R.; Kamińska, M.; Waszkiewicz, E.; Musiał, W.J. MMP-9 in Atrial Remodeling in Patients with Atrial Fibrillation. Ann. Cardiol. Angeiol. 2015, 64, 285–291. [Google Scholar] [CrossRef]
- Li, M.; Yang, G.; Xie, B.; Babu, K.; Huang, C. Changes in Matrix Metalloproteinase-9 Levels during Progression of Atrial Fibrillation. J. Int. Med. Res. 2014, 42, 224–230. [Google Scholar] [CrossRef]
- Pan, D.; Zhou, Y.; Xiao, S.; Hu, Y.; Huan, C.; Wu, Q.; Wang, X.; Pan, Q.; Liu, J.; Zhu, H. Identification of Differentially Expressed Genes and Pathways in Human Atrial Fibrillation by Bioinformatics Analysis. Int. J. Gen. Med. 2022, 15, 103–114. [Google Scholar] [CrossRef]
- Ebana, Y.; Sun, Y.; Yang, X.; Watanabe, T.; Makita, S.; Ozaki, K.; Tanaka, T.; Arai, H.; Furukawa, T. Pathway Analysis with Genome-Wide Association Study (GWAS) Data Detected the Association of Atrial Fibrillation with the MTOR Signaling Pathway. Int. J. Cardiol. Heart Vasc. 2019, 24, 100383. [Google Scholar] [CrossRef]
- Harada, M.; Melka, J.; Sobue, Y.; Nattel, S. Metabolic Considerations in Atrial Fibrillation—Mechanistic Insights and Therapeutic Opportunities. Circ. J. 2017, 81, 1749–1757. [Google Scholar] [CrossRef] [Green Version]
- Hulsurkar, M.M.; Lahiri, S.K.; Moore, O.; Moreira, L.M.; Abu-Taha, I.; Kamler, M.; Dobrev, D.; Nattel, S.; Reilly, S.; Wehrens, X.H.T. Atrial-Specific LKB1 Knockdown Represents a Novel Mouse Model of Atrial Cardiomyopathy with Spontaneous Atrial Fibrillation. Circulation 2021, 144, 909–912. [Google Scholar] [CrossRef]
- Zheng, L.; Jia, X.; Zhang, C.; Wang, D.; Cao, Z.; Wang, J.; Du, X. Angiotensin II in Atrial Structural Remodeling: The Role of Ang II/JAK/STAT3 Signaling Pathway. Am. J. Transl. Res. 2015, 7, 1021–1031. [Google Scholar] [PubMed]
- Wang, H.; Xu, Y.; Xu, A.; Wang, X.; Cheng, L.; Lee, S.; Tse, G.; Li, G.; Liu, T.; Fu, H. PKCβ/NF-ΚB Pathway in Diabetic Atrial Remodeling. J. Physiol. Biochem. 2020, 76, 637–653. [Google Scholar] [CrossRef] [PubMed]
- Scott, L.; Li, N.; Dobrev, D. Role of Inflammatory Signaling in Atrial Fibrillation. Int. J. Cardiol. 2019, 287, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Pretorius, L.; Du, X.-J.; Woodcock, E.A.; Kiriazis, H.; Lin, R.C.Y.; Marasco, S.; Medcalf, R.L.; Ming, Z.; Head, G.A.; Tan, J.W.; et al. Reduced Phosphoinositide 3-Kinase (P110alpha) Activation Increases the Susceptibility to Atrial Fibrillation. Am. J. Pathol. 2009, 175, 998–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wolke, C.; Antileo, E.; Lendeckel, U. WNT Signaling in Atrial Fibrillation. Exp. Biol. Med. 2021, 246, 1112–1120. [Google Scholar] [CrossRef]
- Rusnak, J.; Behnes, M.; Saleh, A.; Fastner, C.; Sattler, K.; Barth, C.; Wenke, A.; Sartorius, B.; Mashayekhi, K.; Hoffmann, U.; et al. Interventional Left Atrial Appendage Closure May Affect Metabolism of Essential Amino Acids and Bioenergetic Efficacy. Int. J. Cardiol. 2018, 268, 125–131. [Google Scholar] [CrossRef]
- Akoum, N.; Wilber, D.; Hindricks, G.; Jais, P.; Cates, J.; Marchlinski, F.; Kholmovski, E.; Burgon, N.; Hu, N.; Mont, L.; et al. MRI Assessment of Ablation-Induced Scarring in Atrial Fibrillation: Analysis from the DECAAF Study. J. Cardiovasc. Electrophysiol. 2015, 26, 473–480. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Total (n = 42) | w/o Recurrence (n = 23) | Recurrence (n = 19) | p Value |
|---|---|---|---|---|
| Age (years) | 59.4 ± 9.1 | 57.4 ± 8.8 | 60.8 ± 8.9 | 0.078 |
| Male | 29 (69%) | 16 (69.6%) | 13 (68.4%) | 0.936 |
| Female | 13 (31%) | 7 (30.4%) | 6 (31,6%) | 0.936 |
| BMI | 29.3 ± 5 | 29.7 ± 5.2 | 29 ± 4.7 | 0.807 |
| Pre-existing Conditions | ||||
| Hypertension | 23 (54.8%) | 12 (52.2%) | 11 (57.9%) | 0.711 |
| Diabetes | 5 (11.9%) | 2 (8.7%) | 3 (15.8%) | 0.480 |
| Smoking | 12 (28.6%) | 6 (26.1%) | 6 (31.6%) | 0.695 |
| Scar % | 24.7 ± 27.9 | 14.5 ± 18.7 | 36.4 ± 32.1 *** | 0.008 |
| Tachycardiomyopathy | 8 (19%) | 4 (17.4%) | 4 (21.1%) | 0.763 |
| Statines | 19 (45.2%) | 8 (34.8%) | 11 (57.9%) | 0.134 |
| ACEi | 9 (21.4%) | 6 (26.1%) | 3 (15.8%) | 0.418 |
| ARB | 12 (28.6%) | 4 (17.4%) | 8 (42.1%) | 0.078 |
| DHP Ca channel blockers | 5 (11.9%) | 2 (8.7%) | 3 (15.8%) | 0.480 |
| Acenocoumarol | 17 (40.5%) | 9 (39.1%) | 8 (42.1%) | 0.845 |
| NOAG | 25 (59.5%) | 14 (60.9%) | 11 (57.9%) | 0.845 |
| Class I ADT | 14 (33.3%) | 10 (43.5%) | 4 (21.1%) | 0.125 |
| Class II ADT | 32 (76.2%) | 17 (53.1%) | 15 (46.9%) | 0.703 |
| Class III ADT | 13 (30.9%) | 7 (30.4%) | 6 (46.2%) | 0.936 |
| Class IV ADT | 4 (9.5%) | 1 (4.4%) | 3 (15.8%) | 0.209 |
| Cholesterol | 191.5 ± 39.1 | 195.9 ± 36.4 | 185.8 ± 56.2 | 0.711 |
| LDLc | 112.3 ± 29.3 | 118.3 ± 30 | 104.6 ± 33.5 | 0.276 |
| HDLc | 54.8 ± 17.8 | 55.2 ± 19.2 | 54.4 ± 18.2 | 0.710 |
| TG | 119.9 ± 52.5 | 129.5 ± 60.6 | 107.6 ± 38.1 | 0.242 |
| AF type | ||||
| Type 1 | 12 (28.6%) | 11 (47.8%) | 1 (5.3%) *** | 0.002 |
| Type 2 | 17 (40.5%) | 8 (34.8%) | 9 (47.4%) | 0.903 |
| Type 3 | 13 (30.9%) | 4 (17.4%) | 9 (47.4%) ** | 0.013 |
| Echocardiographic Parameters | ||||
| LVEF (%) | 59.1 ± 10.6 | 61.3 ± 8.4 | 56.2 ± 16.7 | 0.195 |
| LA Area | 19.6 ± 6.0 | 18.7 ± 5.5 | 20.5 ± 7.7 | 0.424 |
| LA Vol | 91.2 ± 46.1 | 86.8 ± 44.9 | 96.2 ± 49.8 | 0.413 |
| LVEDV | 62.3 ± 33.6 | 62.8 ± 32 | 61.8 ± 38 | 0.944 |
| LVESV | 25 ± 19 | 23.5 ± 11.4 | 27 ± 26.7 | 0.783 |
| LVTDD | 40 ± 8.6 | 40.5 ± 9 | 39.3 ± 11 | 0.748 |
| LVTSD | 28 ± 6.6 | 28.9 ± 6.9 | 26.8 ± 8.3 | 0.376 |
| EAT Vol | 80.6 ± 52.8 | 80.5 ± 49.4 | 80.9 ± 58.7 | 0.738 |
| ECG Parameters | ||||
| HR | 74.2 ± 21.5 | 72.3 ± 24.3 | 76.5 ± 21.7 | 0.136 |
| PR | 157.7 ± 25 | 156.9 ± 28.0 | 160.2 ± 55.8 | 0.877 |
| QRS | 95 ± 12.5 | 93.3 ± 11.1 | 97.2 ± 25.0 | 0.480 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lage, R.; Cebro-Márquez, M.; Vilar-Sánchez, M.E.; González-Melchor, L.; García-Seara, J.; Martínez-Sande, J.L.; Fernández-López, X.A.; Aragón-Herrera, A.; Martínez-Monzonís, M.A.; González-Juanatey, J.R.; et al. Circulating miR-451a Expression May Predict Recurrence in Atrial Fibrillation Patients after Catheter Pulmonary Vein Ablation. Cells 2023, 12, 638. https://doi.org/10.3390/cells12040638
Lage R, Cebro-Márquez M, Vilar-Sánchez ME, González-Melchor L, García-Seara J, Martínez-Sande JL, Fernández-López XA, Aragón-Herrera A, Martínez-Monzonís MA, González-Juanatey JR, et al. Circulating miR-451a Expression May Predict Recurrence in Atrial Fibrillation Patients after Catheter Pulmonary Vein Ablation. Cells. 2023; 12(4):638. https://doi.org/10.3390/cells12040638
Chicago/Turabian StyleLage, Ricardo, María Cebro-Márquez, Marta E. Vilar-Sánchez, Laila González-Melchor, Javier García-Seara, José Luis Martínez-Sande, Xesús Alberte Fernández-López, Alana Aragón-Herrera, María Amparo Martínez-Monzonís, José Ramón González-Juanatey, and et al. 2023. "Circulating miR-451a Expression May Predict Recurrence in Atrial Fibrillation Patients after Catheter Pulmonary Vein Ablation" Cells 12, no. 4: 638. https://doi.org/10.3390/cells12040638