
Placental Changes and Neuropsychological Development in Children—A Systematic Review

Abstract
:1. Introduction
2. Material and Methods
2.1. Eligibility Criteria
2.2. Information Sources and Search Strategy
2.3. Selection Process
2.4. Data Collection Process and Items Extracted
2.5. Study Risk of Bias Assessment
2.6. Effect Measures
2.7. Synthesis Methods
2.8. Reporting Bias Assessment
3. Results
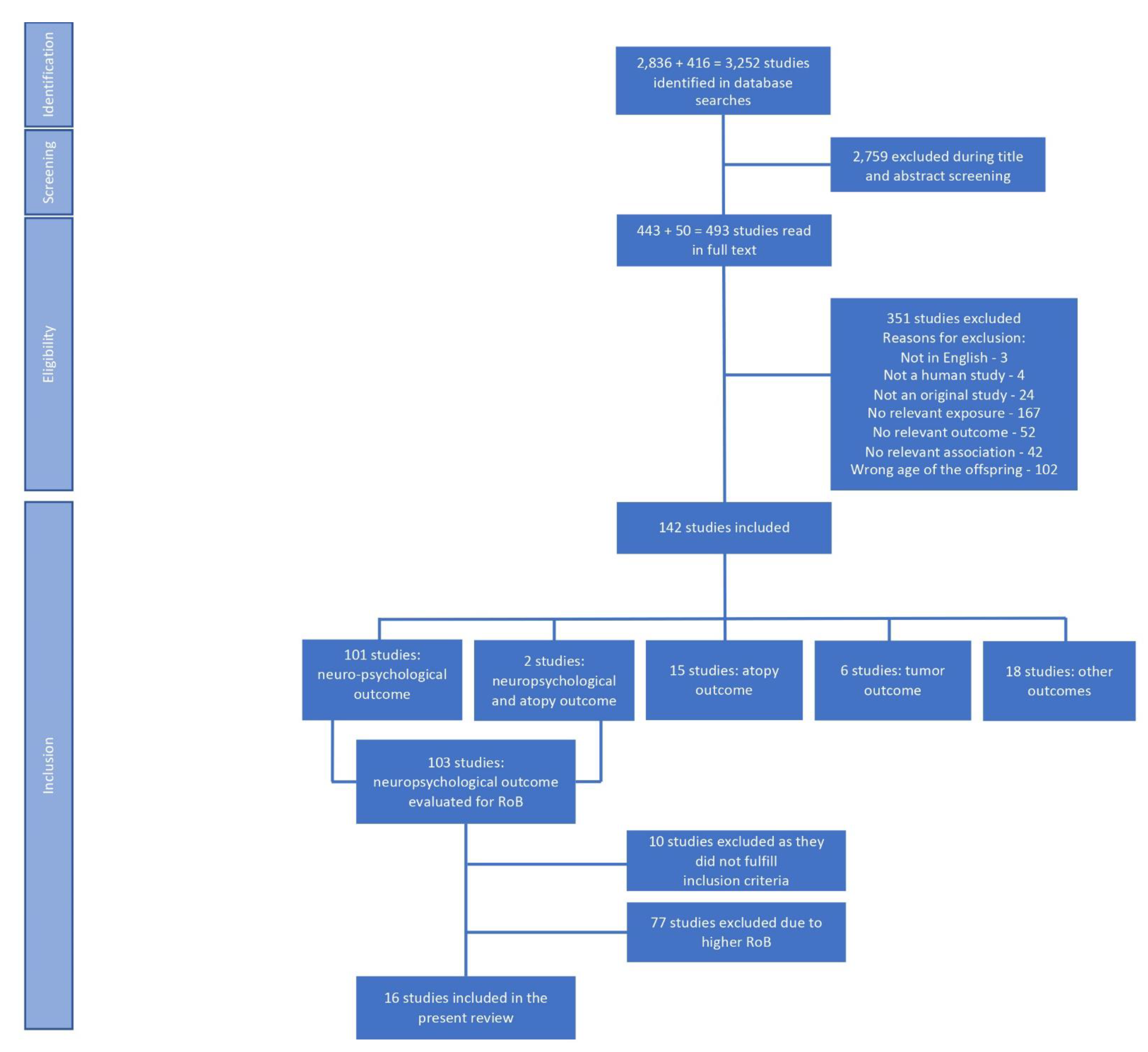
3.1. Study Selection
3.2. Study Characteristics and Their Risks of Bias
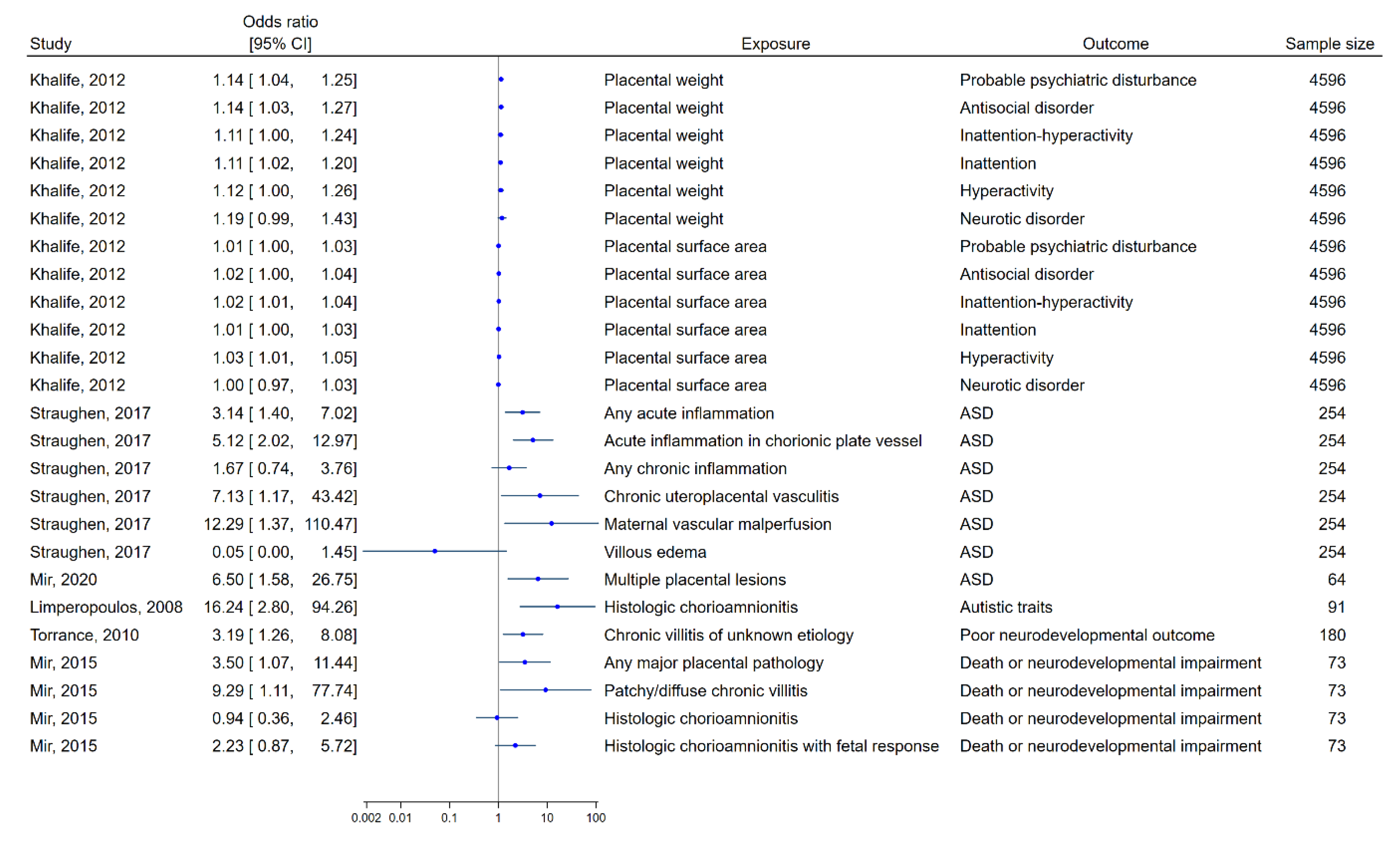
3.3. Results of Individual Studies

{kind=link}
{kind=link}
| Source | Study Type | Setting | Primary Aim To Study: | Study Population | Primary Outcome |
|---|---|---|---|---|---|
| Hendson, 2011 [68] | Cohort | Canada Births 1997–2004 | Survival and neuro- development outcome in VLBW infants exposed to HC | 628 infants HC group: GA: 26.1 w +/− 0.1 BW: 899.3 g +/− 11.9 47% males Non-HC group: GA: 27.6 w +/− 1.0 BW: 958.7 g +/− 11.2 48% males | HC was associated with a lower risk of death after adjustment for perinatal variables, aOR = 0.44 (95% CI = 0.24–0.80) |
| Kaukola, 2005 [70] | Case-control | Finland Births 1998–2002 | Doppler ultrasonographic parameters of fetal cardiovascular hemodynamics associated with poorer neurodevelopment | Cases: 7 infants with signs of PI and suboptimal outcome. GA: 29.1 w +/− 1.6 BW = 796 g +/− 376 Controls: 10 infants with signs of PI and normal outcome. GA: 29.4 w +/− 1.7 BW: 918 g +/− 249 | 6 of 9 Doppler ultrasonographic parameters differed between cases and controls |
| Khalife, 2012 [63] | Cohort | Finland, from the Northern Finland Birth Cohort. Births 1985–1986 | Associations between placental size and psychopathology in childhood | 8954 children 51% males GA: 39.4 w +/− 1.6 BW: 3575 g +/− 534 | Placental size was associated with mental health outcomes in 8 years old boys |
| Limperopoulos, 2008 [67] | Cohort | Northern America Years of birth not stated | Prevalence of and risk factors for autistic features in children born preterm | 91 children 60% males GA: 26 w (range 23–30 BW: 890 g (range 460–1490) | 25% screened positive. Risk factors were GA, BW, chorioamnionitis, sex, and SNAP-II score |
| Meakin, 2018 [76] | Case-control | USA, drawn from the ELGAN study. Births 2002–2004 | Associations between CpG methylation at HPA axis genes in placenta and cognitive impairment at 10 years of age | Cases: 70 children with moderate/severe cognitive impairment. Controls: 158 children with normal/low cognitive function. For all 228 children, GA: 25.7 w (range 23.0–27.6). 60% males | 41 of 237 tested probes associated with moderate/severe impaired cognitive function |
| Mir, 2015 [72] | Cohort | USA Births 2006–2011 | Associations between placental pathology and severity of NE and, in infants requiring hypothermia, neurodevelopmental outcome | 120 neonates with NE 73 of them received hypothermia and were followed up. Their mean GA was 39 w +/− 2. BW: 3384 g +/− 607 | 9 infants receiving hypothermia died before 2 years of age. Placental pathologic findings were more common with increasing severity of the NE |
| Mir, 2021 [64] | Case-control | USA Births 2012–2015 | Placental pathological lesions in children with ASD | Cases: 16 children with ASD GA: 26 w (25–75th centile: 25–29) Controls: 48 matched children GA: 26 w (26–29) | LGA placentas were more prevalent in the ASD group (31% vs. 4 %) |
| Nomura, 2021 [74] | Cohort | USA, enrolled 2010–2013 to the Stress in pregnancy study | Placental transcriptome in relation to natural disaster stress during pregnancy and child behavioral outcome | 131 children. 38 of them were exposed prenatally to a storm. Mean GA: 39.2 w in both groups. Exposed group: BW: 3548 g +/− 577.5 52% males Unexposed group: BW: 3249 g +/− 649 44% males | 221 genes were DE between exposed and unexposed placentas after FDR adjustment and when requiring a FC > 2 |
| Soullane, 2022 [66] | Case-control | Canada Births 2000–2017 | Associations between placental gross morphology and pathology and ASD | Cases: 107 children with ASD 78% males GA: 39.3 w (IQR: 38.6–40.1) BW: 3380 g (2995–3755) Controls: 526 matched children 52% males GA: 39.6 w (38.6–40.3) BW: 3370 g (3050–3675) | 18% of children in both groups had at least one placental pathology. Gross morphology did not differ between groups |
| Spinillo, 2021 [71] | Cohort | Italy Births 2007–2015 | Associations between placental pathological lesions, neonatal mortality and neuro- developmental outcome in VLBW infants | 574 newborns Sex distribution not stated GA: 29.4 w (IQR 27–31.3) BW: 1100 g (IQR 854–1354) | Neonatal mortality: 14%. Four lesions associated with neonatal death |
| Straughen, 2017 [65] | Case-control | USA Births 2007–2014 | Associations between placental pathology and ASD | Cases: 55 children with ASD 76% males GA: 37.4 w +/− 4.0 BW: 2996 g +/− 910.6 Controls: 199 matched children 75% males GA: 37.7 w +/− 3.7 BW: 3148.7 g +/− 833.6 | Five of 18 lesions differed in prevalence between cases and controls |
| Thebault-Dagher, 2021 [75] | Case-control | Canada, enrolled 2010–2012 to the 3D cohort study | Placental expression of 14 genes in children with FS | Cases: 28 children with FS GA: 38.9 w +/− 1.6 BW: 3.3 kg +/− 0.4 Controls: 84 PSM children GA: 39.0 w +/− 1.2 BW: 3.5 kg +/− 0.4 64% males in both groups | Cases had DE of NR3C1-β, SLC6A4, HTR2B, GJA1 and TPJ1 in placenta |
| Torrance, 2010 [69] | Cohort | Netherlands Births 1997–2004 | Prognosis and predictors of outcome in preterm IUGR children | 180 children. 56% males GA: 30.2 w (26–33.9) BW: 875 g (440–1470) | Neonatal mortality: 9% Severe neonatal complications: 28% |
| Ueda, 2022 [73] | Cohort | Japan, drawn from the HBC study Births 2007–2011 | Associations between placental pathology and neurodevelopment | 258 children. 52% males GA: 38.4 w +/− 1.9 BW: 2793 g +/− 552 | Three lesions were associated with lower scores and four lesions were associated with higher scores |
| Vilahur, 2014 [62] | Cohort | Spain, drawn from the INMA study Enrolled 2003–2008 | Associations between prenatal exposure to xenoestrogens and neuropsychological development | 489 children. 52% males GA: 40.0 w (IQR: 39.0–40.7) | TEXB-α tertiles were not associated with any outcome at 1–2 years of age |
| Zhu, 2021 [61] | Cohort | China, drawn from the MABC study Enrolled 2013–2014 | Associations between prenatal exposure to GDM and autistic traits and ADHD symptoms, and whether placental cytokines play a mediating role | 3260 children 13% prenatally exposed to GDM. GA: approx. 39 w 50% of the children that did not develop autistic traits nor ADHD was males | GDM exposure was associated with an increased risk of autistic traits but not ADHD symptoms |
| Study | Bias Due to or in: | ||||||
|---|---|---|---|---|---|---|---|
| Confounding | Selection of Participants | Classification of Exposure | Missing Data | Measurements of Outcomes | Selection of the Reported Result | Overall Bias Risk | |
| Hendson, 2011 [68] | Serious | Low | Low | Low | Low | Moderate | Serious |
| Kaukola, 2005 [70] | Serious | Low | Low | Low | Low | Moderate | Serious |
| Khalife, 2012 [63] | Serious | Low | Low | Low | Low | Moderate | Serious |
| Limperopoulos, 2008 [67] | Moderate | Moderate | Low | Low | Low | Moderate | Moderate |
| Meakin, 2018 [76] | Serious | Low | Low | Low | Low | Moderate | Serious |
| Mir, 2015 [72] | Serious | Low | Low | Low | Low | Moderate | Serious |
| Mir, 2021 [64] | Serious | Low | Low | Low | Low | Moderate | Serious |
| Nomura, 2021 [74] | Serious | Low | Low | Low | Low | Moderate | Serious |
| Soullane, 2022 [66] | Serious | Low | Low | Low | Low | Moderate | Serious |
| Spinillo, 2021 [71] | Serious | Low | Low | Low | Low | Moderate | Serious |
| Straughen, 2017 [65] | Serious | Low | Low | Low | Low | Moderate | Serious |
| Thebault-Dagher, 2021 [75] | Moderate | Low | Low | Low | Low | Moderate | Moderate |
| Torrance, 2010 [69] | Moderate | Low | Low | Low | Low | Moderate | Moderate |
| Ueda, 2022 [73] | Serious | Low | Low | Low | Low | Moderate | Serious |
| Vilahur, 2014 [62] | Serious | Low | Low | Low | Low | Moderate | Serious |
| Zhu, 2021 [61] | Serious | Low | Low | Low | Low | Moderate | Serious |
| Source | Placental Change | Outcome | Age | Associations Found | Confounders Controlled for |
|---|---|---|---|---|---|
| Straughen, 2017 [65] | Histopathological findings (MVM, chronic inflammation, chronic uteroplacental vasculitis, dysmaturity, chronic obstructive vascular lesions, FVM, acute inflammation (=HC)) | ASD | Not specified | aOR (95% CI) for Any acute inflammation: 3.14 (1.39–6.95) Acute inflammation in the chorionic plate vessels: 5.12 (2.02–12.96) Any chronic inflammation: 1.67 (0.74–3.75) Chronic uteroplacental vasculitis: 7.13 (1.17–43.38) MVM: 12.29 (1.37–110.69) Villous edema: 0.05 (0.0005–0.42) | Sex, GA, BW |
| Soullane, 2022 [66] | Histopathological findings (inflammation, vasculitis, degree of maturity, other abnormalities (meconium staining, ischemic infarct, single umbilical artery, chorioangioma, subchorionic fibrin deposition, Tenny-Parker changes)) Gross morphology | ASD | Not specified | Placental hyper maturity: ASD group 4.7% vs. control group 0.4% (p < 0.0001), but the degree of placental maturity was only assessed in 26% of cases and 19% of controls. No other differences were found. No differences were found between groups. | None |
| Mir, 2021 [64] | Histopathological findings (HC, VUE, MVM, fetal thrombotic vasculopathy, villous edema, SGA or LGA placentas) | ASD | Approx. 4 years | > 1 placental lesion: ASD group 69% vs. control group 33% (p = 0.01) Presence of LGA placenta + HC: 25% vs. 2% (p = 0.01) Presence of LGA placenta: 31% vs. 4% (p < 0.01) aOR for presence of multiple lesions: 6.5 (1.6–27.1) | Sex, GA, GDM, maternal age |
| Limperopoulos, 2008 [67] | Histopathological findings (HC, placental abruption, or infarction) | Autistic traits | 22 months corrected age | aOR for HC: 16.240 (2.798–94.270) | Sex, GA, BW, SNAP-II score |
| Hendson, 2011 [68] | Histopathological finding (HC) | NDI 1 | 18 months corrected age | HC associated with MDI, adjusted regression coefficient: −3.93 (−7.52 to −0.33) HC was not associated with NDI after adjustments | PROM, intrapartum antibiotic exposure, antenatal corticosteroids, mode of delivery, GA, sex, singleton vs. multiple birth |
| Torrance, 2010 [69] | Histopathological findings (infarction, VUE) | Mental development | 2 years | Chronic VUE associated with poor neurodevelopmental outcome, aOR: 3.19 (1.26–8.09) | Sex, GA, BW, BW <2.3 percentile, UA pH <7.0, primiparity, hypertensive disease, ROP, RDS |
| Kaukola, 2005 [70] | Histopathological findings (HC, perfusion defect) | Psychomotor development | 1 year corrected age | No differences or associations found | None |
| Spinillo, 2021 [71] | Histopathological findings (HC, VUE, FVM, MVM, intravillous hemorrhage) | Psychomotor development | 24 months corrected age | aOR for survival with normal neurodevelopmental outcome: MVM: 0.45 (0.22–0.92) FVM: 0.46 (0.22–0.45) HC: 0.75 (0.43–1.29) Loss of placental integrity: 0.73 (0.44–1.21) Intravillous hemorrhage: 0.38 (0.22–0.62) VUE: 1.54 (0.86–2.75) | Sex, GA, BW, type of delivery |
| Mir, 2015 [72] | Histopathological findings (HC, VUE, fetal vascular thromboocclusive disease, maternal placental underperfusion, retroplacental hemorrhage/infarction, SGA or LGA placentas) | Death or NDI 2 | 18–24 months | OR for death or NDI: Any major placental pathology: 3.50 (1.07–11.44) Patchy/diffuse chronic villitis: 9.29 (1.11–77.73) HC: 0.94 (0.36–2.47) HC with fetal response: 2.23 (0.87–5.73) | None |
| Ueda, 2022 [73] | Histopathological findings (11 lesions, see the column “Associations found”) | Psychomotor development | 10–40 months | Total MSEL composite scores associated with: Accelerated villous maturation: -2.46 (−4.30 to −0.61) Thrombosis or intramural fibrin deposition: 3.07 (1.36 to 4.79) Avascular villi: 2.68 (0.15 to 5.21) Delayed villous maturation: −2.62 (−4.59 to -0.64 Fetal inflammatory response: 2.26 (0.25 to 4.28) MVM: −2.09 (−3.69 to −0.50) FVM: 3.41 (1.74 to 5.07) But not with decidual arteriopathy, HC, VUE, or deciduitis. | Sex, BW, parity |
| Nomura, 2021 [74] | Gene expression: Transcriptome | Behavior | 4 years | 28 of 221 DEG between prenatally storm-exposed and unexposed children were found to mediate child aggression and 5 DEG were found to mediate child anxiety | Maternal age, drug use, education, marital status, fetal sex, BW |
| Thebault-Dagher, 2021 [75] | Gene expression: 14 genes 3 | FS and age at first seizure | Up to 2 years | FS group had (with medium effect size) increased expression of SLC6A4, GJA1 and TPJ1, and decreased expression of NR3C1-β and HTR2B Increased SLC6A4 expression predicted younger age at first FS (large effect size) | Sex, GA, labor prior to delivery, complications at birth |
| Zhu, 2021 [61] | Gene expression: cytokines 4 | Autistic traits | 18 months | None of the investigated mRNAs associated with autistic traits after FDR corrections | Maternal age, prepregnancy BMI, HDCP, place of residence, educational level, average monthly income, parity, smoking history, fetal sex, BW, delivery mode, GA, the other cytokine mRNA levels |
| Meakin, 2018 [76] | CpG methylation 5 | Cognitive and executive function | 10 years | 41 probes showed methylation differences by cognitive functioning Highest OR was 1.876 (1.067–3.298) found for the TSS200 region near NR3C1 | Race, public insurance, maternal education, fetal sex, GA |
| Vilahur, 2014 [62] | Total effective xenoestrogen burden | Mental and psychomotor development | 11–22 months | No significant association between TEXB-α values and MDI or PDI scores was found | MDI: geographical area of origin, sex, parental social class, maternal age, CS, maternal height, GWG, passive smoking and log transformed TEXB-β values PDI: geographical area of origin, sex, maternal BMI, breastfeeding, parental social class, maternal height, marital status, and log transformed TEXB-β values |
| Khalife, 2012 [63] | Weight and surface | Psychiatric disturbance | 8 years | For boys: aOR for placental weight Probable psychiatric disturbance: 1.14 (1.04–1.25) Antisocial disorder: 1.14 (1.03–1.27) Inattention-hyperactivity: 1.11 (1.00–1.24) Inattention: 1.11 (1.02–1.20) Hyperactivity: 1.12 (1.00–1.26) Neurotic disorder: 1.19 (0.99–1.42) For boys: aOR for surface area Probable psychiatric disturbance: 1.01 (1.00–1.03) Antisocial disorder: 1.02 (1.00–1.04) Inattention-hyperactivity: 1.02 (1.01–1.04) Inattention: 1.01 (1.00–1.03) Hyperactivity: 1.03 (1.01–1.05) Neurotic disorder: 1.00 (0.97–1.03) For girls: No associations were found | GA, BW, maternal age, family structure, education, social class, smoking during pregnancy, parity, pre-pregnancy BMI, GWG |
3.4. Results of Synthesis
3.5. Reporting Biases
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ADHD | attention deficit hyperactivity disorder |
| ASD | autism spectrum disorders |
| CI | confidence interval |
| DHA | docosahexaenoic acid |
| DOHaD | developmental origins of health and disease |
| FVM | fetal vascular malperfusion |
| GA | gestational age |
| GDM | gestational diabetes mellitus |
| HC | histological chorioamnionitis |
| HPA | hypothalamic–pituitary–adrenal |
| IL | interleukin |
| IUGR | intra-uterine growth restriction |
| LGA | large for gestational age |
| MeSH | medical subject headings |
| MSEL | Mullen scale of early learning |
| MVM | maternal vascular malperfusion |
| NE | neonatal encephalopathy |
| RoB | risk of bias |
References
- Barker, D.J.; Winter, P.D.; Osmond, C.; Margetts, B.; Simmonds, S.J. Weight in infancy and death from ischaemic heart disease. Lancet 1989, 2, 577–580. [Google Scholar] [CrossRef] [PubMed]
- Barker, D.J. The developmental origins of adult disease. J. Am. Coll. Nutr. 2004, 23, 588s–595s. [Google Scholar] [CrossRef] [PubMed]
- Wadhwa, P.D.; Buss, C.; Entringer, S.; Swanson, J.M. Developmental origins of health and disease: Brief history of the approach and current focus on epigenetic mechanisms. Semin. Reprod. Med. 2009, 27, 358–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arima, Y.; Fukuoka, H. Developmental origins of health and disease theory in cardiology. J. Cardiol. 2020, 76, 14–17. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, D.J.; Powell, T.L.; Barrett, E.S.; Hardy, D.B. Developmental origins of metabolic diseases. Physiol. Rev. 2021, 101, 739–795. [Google Scholar] [CrossRef]
- Ganguly, E.; Hula, N.; Spaans, F.; Cooke, C.M.; Davidge, S.T. Placenta-targeted treatment strategies: An opportunity to impact fetal development and improve offspring health later in life. Pharmacol. Res. 2020, 157, 104836. [Google Scholar] [CrossRef] [PubMed]
- Fisher, D.; Baird, J.; Payne, L.; Lucas, P.; Kleijnen, J.; Roberts, H.; Law, C. Are infant size and growth related to burden of disease in adulthood? A systematic review of literature. Int. J. Epidemiol. 2006, 35, 1196–1210. [Google Scholar] [CrossRef] [Green Version]
- Burton, G.J.; Fowden, A.L. The placenta: A multifaceted, transient organ. Philos. Trans. R. Soc. Lond. B Biol. Sci. 2015, 370, 20140066. [Google Scholar] [CrossRef] [Green Version]
- Rosenfeld, C.S. The placenta-brain-axis. J. Neurosci. Res. 2021, 99, 271–283. [Google Scholar] [CrossRef]
- Al-Haddad, B.J.S.; Oler, E.; Armistead, B.; Elsayed, N.A.; Weinberger, D.R.; Bernier, R.; Burd, I.; Kapur, R.; Jacobsson, B.; Wang, C.; et al. The fetal origins of mental illness. Am. J. Obstet. Gynecol. 2019, 221, 549–562. [Google Scholar] [CrossRef]
- Vorherr, H. Factors influencing fetal growth. Am. J. Obstet. Gynecol. 1982, 142, 577–588. [Google Scholar] [CrossRef]
- Burton, G.J.; Jauniaux, E. Pathophysiology of placental-derived fetal growth restriction. Am. J. Obstet. Gynecol. 2018, 218, S745–S761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Derricott, H.; Jones, R.L.; Heazell, A.E. Investigating the association of villitis of unknown etiology with stillbirth and fetal growth restriction-a systematic review. Placenta 2013, 34, 856–862. [Google Scholar] [CrossRef]
- Balayla, J.; Desilets, J.; Shrem, G. Placenta previa and the risk of intrauterine growth restriction (IUGR): A systematic review and meta-analysis. J. Perinat. Med. 2019, 47, 577–584. [Google Scholar] [CrossRef]
- de Knegt, V.E.; Hedley, P.L.; Kanters, J.K.; Thagaard, I.N.; Krebs, L.; Christiansen, M.; Lausten-Thomsen, U. The Role of Leptin in Fetal Growth during Pre-Eclampsia. Int. J. Mol. Sci. 2021, 22, 4569. [Google Scholar] [CrossRef]
- Thornburg, K.L.; Marshall, N. The placenta is the center of the chronic disease universe. Am. J. Obstet. Gynecol. 2015, 213, S14–S20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burton, G.J.; Fowden, A.L.; Thornburg, K.L. Placental Origins of Chronic Disease. Physiol. Rev. 2016, 96, 1509–1565. [Google Scholar] [CrossRef] [Green Version]
- Bastek, J.A.; Weber, A.L.; McShea, M.A.; Ryan, M.E.; Elovitz, M.A. Prenatal inflammation is associated with adverse neonatal outcomes. Am. J. Obstet. Gynecol. 2014, 210, 450.e1–450.e10. [Google Scholar] [CrossRef] [PubMed]
- Backes, C.H.; Markham, K.; Moorehead, P.; Cordero, L.; Nankervis, C.A.; Giannone, P.J. Maternal preeclampsia and neonatal outcomes. J. Pregnancy 2011, 2011, 214365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collins, K.A.; Popek, E. Birth Injury: Birth Asphyxia and Birth Trauma. Acad. Forensic Pathol. 2018, 8, 788–864. [Google Scholar] [CrossRef]
- Saigal, S.; Doyle, L.W. An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet 2008, 371, 261–269. [Google Scholar] [CrossRef] [PubMed]
- Vuillermin, P.J.; Macia, L.; Nanan, R.; Tang, M.L.; Collier, F.; Brix, S. The maternal microbiome during pregnancy and allergic disease in the offspring. Semin. Immunopathol. 2017, 39, 669–675. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heck, J.E.; He, D.; Janzen, C.; Federman, N.; Olsen, J.; Ritz, B.; Hansen, J. Fetal programming and Wilms tumor. Pediatr. Blood Cancer 2019, 66, e27461. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, J.A.; Gallagher, K.; Beck, C.; Kumar, R.; Gernand, A.D. Maternal-Fetal Inflammation in the Placenta and the Developmental Origins of Health and Disease. Front. Immunol. 2020, 11, 531543. [Google Scholar] [CrossRef] [PubMed]
- Medsker, B.; Forno, E.; Simhan, H.; Celedón, J.C. Prenatal Stress, Prematurity, and Asthma. Obstet. Gynecol. Surv. 2015, 70, 773–779. [Google Scholar] [CrossRef] [Green Version]
- Mohamad Zainal, N.H.; Mohd Nor, N.H.; Saat, A.; Clifton, V.L. Childhood allergy susceptibility: The role of the immune system development in the in-utero period. Hum. Immunol. 2022, 83, 437–446. [Google Scholar] [CrossRef]
- Ozen, M.; Aghaeepour, N.; Marić, I.; Wong, R.J.; Stevenson, D.K.; Jantzie, L.L. Omics approaches: Interactions at the maternal-fetal interface and origins of child health and disease. Pediatr. Res. 2022, 1–10. [Google Scholar] [CrossRef]
- Tarui, T.; Rasool, A.; O’Tierney-Ginn, P. How the placenta-brain lipid axis impacts the nutritional origin of child neurodevelopmental disorders: Focus on attention deficit hyperactivity disorder and autism spectrum disorder. Exp. Neurol. 2022, 347, 113910. [Google Scholar] [CrossRef]
- Wu, W.L.; Hsiao, E.Y.; Yan, Z.; Mazmanian, S.K.; Patterson, P.H. The placental interleukin-6 signaling controls fetal brain development and behavior. Brain. Behav. Immun. 2017, 62, 11–23. [Google Scholar] [CrossRef] [Green Version]
- Novak, C.M.; Lee, J.Y.; Ozen, M.; Tsimis, M.E.; Kucirka, L.M.; McLane, M.W.; Xie, L.; Kelleher, M.; Xie, H.; Jia, B.; et al. Increased placental T cell trafficking results in adverse neurobehavioral outcomes in offspring exposed to sub-chronic maternal inflammation. Brain. Behav. Immun. 2019, 75, 129–136. [Google Scholar] [CrossRef]
- Bronson, S.L.; Chan, J.C.; Bale, T.L. Sex-Specific Neurodevelopmental Programming by Placental Insulin Receptors on Stress Reactivity and Sensorimotor Gating. Biol. Psychiatry 2017, 82, 127–138. [Google Scholar] [CrossRef]
- Yu, P.; Chen, Y.; Ge, C.; Wang, H. Sexual dimorphism in placental development and its contribution to health and diseases. Crit. Rev. Toxicol. 2021, 51, 555–570. [Google Scholar] [CrossRef] [PubMed]
- Mikaelsson, M.A.; Constância, M.; Dent, C.L.; Wilkinson, L.S.; Humby, T. Placental programming of anxiety in adulthood revealed by Igf2-null models. Nat. Commun. 2013, 4, 2311. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Illa, M.; Eixarch, E.; Muñoz-Moreno, E.; Batalle, D.; Leal-Campanario, R.; Gruart, A.; Delgado-García, J.M.; Figueras, F.; Gratacós, E. Neurodevelopmental Effects of Undernutrition and Placental Underperfusion in Fetal Growth Restriction Rabbit Models. Fetal Diagn. Ther. 2017, 42, 189–197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuringer, M.; Connor, W.E.; Lin, D.S.; Barstad, L.; Luck, S. Biochemical and functional effects of prenatal and postnatal omega 3 fatty acid deficiency on retina and brain in rhesus monkeys. Proc. Natl. Acad. Sci. USA 1986, 83, 4021–4025. [Google Scholar] [CrossRef] [Green Version]
- Zhu, Y.; Mordaunt, C.E.; Yasui, D.H.; Marathe, R.; Coulson, R.L.; Dunaway, K.W.; Jianu, J.M.; Walker, C.K.; Ozonoff, S.; Hertz-Picciotto, I.; et al. Placental DNA methylation levels at CYP2E1 and IRS2 are associated with child outcome in a prospective autism study. Hum. Mol. Genet. 2019, 28, 2659–2674. [Google Scholar] [CrossRef]
- Ley, D.; Marsal, K.; Dahlgren, J.; Hellstrom, A. Abnormal retinal optic nerve morphology in young adults after intrauterine growth restriction. Pediatr. Res. 2004, 56, 139–143. [Google Scholar] [CrossRef] [Green Version]
- Ohara, N.; Tsujino, T.; Maruo, T. The role of thyroid hormone in trophoblast function, early pregnancy maintenance, and fetal neurodevelopment. J. Obstet. Gynaecol. Can. 2004, 26, 982–990. [Google Scholar] [CrossRef]
- Chen, Y.; Xue, F. The impact of gestational hypothyroxinemia on the cognitive and motor development of offspring. J. Matern. Fetal Neonatal Med. 2020, 33, 1940–1945. [Google Scholar] [CrossRef]
- Henrichs, J.; Ghassabian, A.; Peeters, R.P.; Tiemeier, H. Maternal hypothyroxinemia and effects on cognitive functioning in childhood: How and why? Clin. Endocrinol. 2013, 79, 152–162. [Google Scholar] [CrossRef] [PubMed]
- Morton, A.; Teasdale, S. Physiological changes in pregnancy and their influence on the endocrine investigation. Clin. Endocrinol. 2022, 96, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Freemark, M. Regulation of maternal metabolism by pituitary and placental hormones: Roles in fetal development and metabolic programming. Horm. Res. 2006, 65 (Suppl. 3), 41–49. [Google Scholar] [CrossRef] [PubMed]
- Maric, C. Mechanisms of fetal programming of adult hypertension: Role of sex hormones. Hypertension 2007, 50, 605–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maranella, E.; Mareri, A.; Nardi, V.; Di Natale, C.; Di Luca, L.; Conte, E.; Pannone, V.; Catalucci, A.; Di Fabio, S. Severe neurologic and hepatic toxicity in a newborn prenatally exposed to methamphetamine. A case report. Brain Dev. 2019, 41, 191–194. [Google Scholar] [CrossRef]
- Felix, A.; Hallet, E.; Favre, A.; Kom-Tchameni, R.; Defo, A.; Fléchelles, O.; Rosenthal, J.M.; Douine, M.; Nacher, M.; Elenga, N. Cerebral injuries associated with Zika virus in utero exposure in children without birth defects in French Guiana: Case report. Medicine 2017, 96, e9178. [Google Scholar] [CrossRef] [PubMed]
- Squier, W.; Cowan, F.M. The value of autopsy in determining the cause of failure to respond to resuscitation at birth. Semin Neonatol. 2004, 9, 331–345. [Google Scholar] [CrossRef]
- Steinlin, M. Cerebellar disorders in childhood: Cognitive problems. Cerebellum 2008, 7, 607–610. [Google Scholar] [CrossRef] [Green Version]
- Roescher, A.M.; Timmer, A.; Erwich, J.J.; Bos, A.F. Placental pathology, perinatal death, neonatal outcome, and neurological development: A systematic review. PLoS ONE 2014, 9, e89419. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Ives, C.W.; Sinkey, R.; Rajapreyar, I.; Tita, A.T.N.; Oparil, S. Preeclampsia-Pathophysiology and Clinical Presentations: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2020, 76, 1690–1702. [Google Scholar] [CrossRef]
- Downes, K.L.; Grantz, K.L.; Shenassa, E.D. Maternal, Labor, Delivery, and Perinatal Outcomes Associated with Placental Abruption: A Systematic Review. Am. J. Perinatol. 2017, 34, 935–957. [Google Scholar] [CrossRef] [PubMed]
- Mosquera, C.; Miller, R.S.; Simpson, L.L. Twin-twin transfusion syndrome. Semin. Perinatol. 2012, 36, 182–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Addy, D.P. Letter: “Neonatal” is the first 28 days of life. Pediatrics 1975, 55, 571–572. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [Green Version]
- Sterne, J.A.C.; Higgins, J.P.T.; Elbers, R.G.; Reeves, B.C.; The development group for ROBINS-I. Risk of Bias in Non-Randomized Studies of Interventions (ROBINS-I): Detailed Guidance. Available online: https://sites.google.com/site/riskofbiastool/welcome/home/current-version-of-robins-i/robins-i-detailed-guidance-2016 (accessed on 15 August 2022).
- May, T.; Adesina, I.; McGillivray, J.; Rinehart, N.J. Sex differences in neurodevelopmental disorders. Curr. Opin. Neurol. 2019, 32, 622–626. [Google Scholar] [CrossRef]
- Palmeira, P.; Quinello, C.; Silveira-Lessa, A.L.; Zago, C.A.; Carneiro-Sampaio, M. IgG placental transfer in healthy and pathological pregnancies. Clin. Dev. Immunol. 2012, 2012, 985646. [Google Scholar] [CrossRef] [PubMed]
- Ream, M.A.; Lehwald, L. Neurologic Consequences of Preterm Birth. Curr. Neurol. Neurosci. Rep. 2018, 18, 48. [Google Scholar] [CrossRef]
- Bakhuizen, S.E.; de Haan, T.R.; Teune, M.J.; van Wassenaer-Leemhuis, A.G.; van der Heyden, J.L.; van der Ham, D.P.; Mol, B.W. Meta-analysis shows that infants who have suffered neonatal sepsis face an increased risk of mortality and severe complications. Acta Paediatr. 2014, 103, 1211–1218. [Google Scholar] [CrossRef]
- Sterne, J.A.; Egger, M.; Smith, G.D. Systematic reviews in health care: Investigating and dealing with publication and other biases in meta-analysis. BMJ 2001, 323, 101–105. [Google Scholar] [CrossRef]
- Zhu, B.; Deng, F.; Yan, S.; Huang, K.; Wu, X.; Tao, X.; Wang, S.; Tao, F. Gestational diabetes mellitus, autistic traits and ADHD symptoms in toddlers: Placental inflammatory and oxidative stress cytokines do not play an intermediary role. Psychoneuroendocrinology 2021, 134, 105435. [Google Scholar] [CrossRef]
- Vilahur, N.; Fernández, M.F.; Bustamante, M.; Ramos, R.; Forns, J.; Ballester, F.; Murcia, M.; Riaño, I.; Ibarluzea, J.; Olea, N.; et al. In utero exposure to mixtures of xenoestrogens and child neuropsychological development. Environ. Res. 2014, 134, 98–104. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khalife, N.; Glover, V.; Hartikainen, A.L.; Taanila, A.; Ebeling, H.; Järvelin, M.R.; Rodriguez, A. Placental size is associated with mental health in children and adolescents. PLoS ONE 2012, 7, e40534. [Google Scholar] [CrossRef] [PubMed]
- Mir, I.N.; White, S.P.; Steven Brown, L.; Heyne, R.; Rosenfeld, C.R.; Chalak, L.F. Autism spectrum disorders in extremely preterm infants and placental pathology findings: A matched case-control study. Pediatr. Res. 2021, 89, 1825–1831. [Google Scholar] [CrossRef] [PubMed]
- Straughen, J.K.; Misra, D.P.; Divine, G.; Shah, R.; Perez, G.; VanHorn, S.; Onbreyt, V.; Dygulska, B.; Schmitt, R.; Lederman, S.; et al. The association between placental histopathology and autism spectrum disorder. Placenta 2017, 57, 183–188. [Google Scholar] [CrossRef]
- Soullane, S.; Spence, A.R.; Abenhaim, H.A. Association of placental pathology and gross morphology with autism spectrum disorders. Autism Res. 2022, 15, 531–538. [Google Scholar] [CrossRef]
- Limperopoulos, C.; Bassan, H.; Sullivan, N.R.; Soul, J.S.; Robertson, R.L., Jr.; Moore, M.; Ringer, S.A.; Volpe, J.J.; du Plessis, A.J. Positive screening for autism in ex-preterm infants: Prevalence and risk factors. Pediatrics 2008, 121, 758–765. [Google Scholar] [CrossRef] [Green Version]
- Hendson, L.; Russell, L.; Robertson, C.M.; Liang, Y.; Chen, Y.; Abdalla, A.; Lacaze-Masmonteil, T. Neonatal and neurodevelopmental outcomes of very low birth weight infants with histologic chorioamnionitis. J. Pediatr. 2011, 158, 397–402. [Google Scholar] [CrossRef]
- Torrance, H.L.; Bloemen, M.C.; Mulder, E.J.; Nikkels, P.G.; Derks, J.B.; de Vries, L.S.; Visser, G.H. Predictors of outcome at 2 years of age after early intrauterine growth restriction. Ultrasound Obstet. Gynecol. 2010, 36, 171–177. [Google Scholar] [CrossRef]
- Kaukola, T.; Räsänen, J.; Herva, R.; Patel, D.D.; Hallman, M. Suboptimal neurodevelopment in very preterm infants is related to fetal cardiovascular compromise in placental insufficiency. Am. J. Obstet. Gynecol. 2005, 193, 414–420. [Google Scholar] [CrossRef]
- Spinillo, A.; Dominoni, M.; Caporali, C.; Olivieri, I.; La Piana, R.; Longo, S.; Cesari, S.; Fiandrino, G.; Orcesi, S.; Gardella, B. Placental Histological Features and Neurodevelopmental Outcomes at Two Years in Very-Low-Birth-Weight Infants. Pediatr. Neurol. 2021, 120, 63–70. [Google Scholar] [CrossRef]
- Mir, I.N.; Johnson-Welch, S.F.; Nelson, D.B.; Brown, L.S.; Rosenfeld, C.R.; Chalak, L.F. Placental pathology is associated with severity of neonatal encephalopathy and adverse developmental outcomes following hypothermia. Am. J. Obstet. Gynecol. 2015, 213, 849.e1–849.e7. [Google Scholar] [CrossRef] [PubMed]
- Ueda, M.; Tsuchiya, K.J.; Yaguchi, C.; Furuta-Isomura, N.; Horikoshi, Y.; Matsumoto, M.; Suzuki, M.; Oda, T.; Kawai, K.; Itoh, T.; et al. Placental pathology predicts infantile neurodevelopment. Sci. Rep. 2022, 12, 2578. [Google Scholar] [CrossRef] [PubMed]
- Nomura, Y.; Rompala, G.; Pritchett, L.; Aushev, V.; Chen, J.; Hurd, Y.L. Natural disaster stress during pregnancy is linked to reprogramming of the placenta transcriptome in relation to anxiety and stress hormones in young offspring. Mol. Psychiatry 2021, 26, 6520–6530. [Google Scholar] [CrossRef] [PubMed]
- Thébault-Dagher, F.; Robles, M.; Herba, C.M.; St-Pierre, J.; Brochen, C.; Muckle, G.; Lupien, S.J.; Séguin, J.R.; Fraser, W.D.; Vaillancourt, C.; et al. Febrile seizure incidence and age at first occurrence are associated with changes in placental normalized gene expression: The ‘3D’ pregnancy cohort study. J. Neuroendocrinol. 2021, 33, e13046. [Google Scholar] [CrossRef]
- Meakin, C.J.; Martin, E.M.; Santos, H.P., Jr.; Mokrova, I.; Kuban, K.; O’Shea, T.M.; Joseph, R.M.; Smeester, L.; Fry, R.C. Placental CpG methylation of HPA-axis genes is associated with cognitive impairment at age 10 among children born extremely preterm. Horm. Behav. 2018, 101, 29–35. [Google Scholar] [CrossRef]
- Polanczyk, G.; de Lima, M.S.; Horta, B.L.; Biederman, J.; Rohde, L.A. The worldwide prevalence of ADHD: A systematic review and metaregression analysis. Am. J. Psychiatry 2007, 164, 942–948. [Google Scholar] [CrossRef]
- Wang, T.; Liu, K.; Li, Z.; Xu, Y.; Liu, Y.; Shi, W.; Chen, L. Prevalence of attention deficit/hyperactivity disorder among children and adolescents in China: A systematic review and meta-analysis. BMC Psychiatry 2017, 17, 32. [Google Scholar] [CrossRef] [Green Version]
- Engström, K.; Mandakh, Y.; Garmire, L.; Masoumi, Z.; Isaxon, C.; Malmqvist, E.; Erlandsson, L.; Hansson, S.R. Early Pregnancy Exposure to Ambient Air Pollution among Late-Onset Preeclamptic Cases Is Associated with Placental DNA Hypomethylation of Specific Genes and Slower Placental Maturation. Toxics 2021, 9, 338. [Google Scholar] [CrossRef]
- Allbrand, M.; Eklund, D.; Cao, Y.; Nilsson, K.; Lodefalk, M. Gene expression of leptin, leptin receptor isoforms and inflammatory cytokines in placentas of obese women-Associations to birth weight and fetal sex. Placenta 2022, 117, 64–71. [Google Scholar] [CrossRef]
- Schalekamp-Timmermans, S.; Cornette, J.; Hofman, A.; Helbing, W.A.; Jaddoe, V.W.; Steegers, E.A.; Verburg, B.O. In utero origin of sex-related differences in future cardiovascular disease. Biol. Sex Differ. 2016, 7, 55. [Google Scholar] [CrossRef]
- Morsing, E.; Lundgren, P.; Hård, A.L.; Rakow, A.; Hellström-Westas, L.; Jacobson, L.; Johnson, M.; Nilsson, S.; Smith, L.E.H.; Sävman, K.; et al. Neurodevelopmental disorders and somatic diagnoses in a national cohort of children born before 24 weeks of gestation. Acta Paediatr. 2022, 111, 1167–1175. [Google Scholar] [CrossRef] [PubMed]
- Morsing, E.; Asard, M.; Ley, D.; Stjernqvist, K.; Marsál, K. Cognitive function after intrauterine growth restriction and very preterm birth. Pediatrics 2011, 127, e874–e882. [Google Scholar] [CrossRef] [PubMed]
- van Abeelen, A.F.M.; de Rooij, S.R.; Osmond, C.; Painter, R.C.; Veenendaal, M.V.E.; Bossuyt, P.M.M.; Elias, S.G.; Grobbee, D.E.; van der Schouw, Y.T.; Barker, D.J.P.; et al. The sex-specific effects of famine on the association between placental size and later hypertension. Placenta 2011, 32, 694–698. [Google Scholar] [CrossRef]
- Kalisch-Smith, J.I.; Simmons, D.G.; Pantaleon, M.; Moritz, K.M. Sex differences in rat placental development: From pre-implantation to late gestation. Biol. Sex Differ. 2017, 8, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, S.; Isotani, A.; Mise, N.; Yamamoto, M.; Fujihara, Y.; Kaseda, K.; Nakanishi, T.; Ikawa, M.; Hamada, H.; Abe, K.; et al. Comparison of gene expression in male and female mouse blastocysts revealed imprinting of the X-linked gene, Rhox5/Pem, at preimplantation stages. Curr. Biol. 2006, 16, 166–172. [Google Scholar] [CrossRef] [Green Version]
- Bermejo-Alvarez, P.; Rizos, D.; Rath, D.; Lonergan, P.; Gutierrez-Adan, A. Epigenetic differences between male and female bovine blastocysts produced in vitro. Physiol Genomics 2008, 32, 264–272. [Google Scholar] [CrossRef] [PubMed]
- Bermejo-Alvarez, P.; Rizos, D.; Rath, D.; Lonergan, P.; Gutierrez-Adan, A. Sex determines the expression level of one third of the actively expressed genes in bovine blastocysts. Proc. Natl. Acad. Sci. USA 2010, 107, 3394–3399. [Google Scholar] [CrossRef] [Green Version]
- Syrett, C.M.; Sierra, I.; Berry, C.L.; Beiting, D.; Anguera, M.C. Sex-Specific Gene Expression Differences Are Evident in Human Embryonic Stem Cells and During In Vitro Differentiation of Human Placental Progenitor Cells. Stem Cells Dev. 2018, 27, 1360–1375. [Google Scholar] [CrossRef]
- Sood, R.; Zehnder, J.L.; Druzin, M.L.; Brown, P.O. Gene expression patterns in human placenta. Proc. Natl. Acad. Sci. USA 2006, 103, 5478–5483. [Google Scholar] [CrossRef] [Green Version]
- Buckberry, S.; Bianco-Miotto, T.; Bent, S.J.; Dekker, G.A.; Roberts, C.T. Integrative transcriptome meta-analysis reveals widespread sex-biased gene expression at the human fetal-maternal interface. Mol. Hum. Reprod. 2014, 20, 810–819. [Google Scholar] [CrossRef]
- Sciberras, E.; Mulraney, M.; Silva, D.; Coghill, D. Prenatal Risk Factors and the Etiology of ADHD-Review of Existing Evidence. Curr. Psychiatry Rep. 2017, 19, 1. [Google Scholar] [CrossRef] [PubMed]
- Marks-Anglin, A.; Chen, Y. A historical review of publication bias. Res. Synth. Methods 2020, 11, 725–742. [Google Scholar] [CrossRef] [PubMed]
- Shi, Z.; Ma, L.; Luo, K.; Bajaj, M.; Chawla, S.; Natarajan, G.; Hagberg, H.; Tan, S. Chorioamnionitis in the Development of Cerebral Palsy: A Meta-analysis and Systematic Review. Pediatrics 2017, 139, e20163781. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kratimenos, P.; Penn, A.A. Placental programming of neuropsychiatric disease. Pediatr. Res. 2019, 86, 157–164. [Google Scholar] [CrossRef]
- Gardener, H.; Spiegelman, D.; Buka, S.L. Prenatal risk factors for autism: Comprehensive meta-analysis. Br. J. Psychiatry 2009, 195, 7–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gardener, H.; Spiegelman, D.; Buka, S.L. Perinatal and neonatal risk factors for autism: A comprehensive meta-analysis. Pediatrics 2011, 128, 344–355. [Google Scholar] [CrossRef]
- Wang, C.; Geng, H.; Liu, W.; Zhang, G. Prenatal, perinatal, and postnatal factors associated with autism: A meta-analysis. Medicine 2017, 96, e6696. [Google Scholar] [CrossRef]
- Monset-Couchard, M.; de Bethmann, O.; Kastler, B. Mid- and long-term outcome of 89 premature infants weighing less than 1000 g at birth, all appropriate for gestational age. Biol. Neonate 1996, 70, 328–338. [Google Scholar] [CrossRef]
- Lorenz, J.M. The outcome of extreme prematurity. Semin. Perinatol. 2001, 25, 348–359. [Google Scholar] [CrossRef]
- Shah, R.; Harding, J.; Brown, J.; McKinlay, C. Neonatal Glycaemia and Neurodevelopmental Outcomes: A Systematic Review and Meta-Analysis. Neonatology 2019, 115, 116–126. [Google Scholar] [CrossRef]
- Cai, S.; Thompson, D.K.; Anderson, P.J.; Yang, J.Y. Short- and Long-Term Neurodevelopmental Outcomes of Very Preterm Infants with Neonatal Sepsis: A Systematic Review and Meta-Analysis. Children 2019, 6, 131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burton, G.J.; Jauniaux, E. What is the placenta? Am. J. Obstet. Gynecol. 2015, 213, S6.e1–S6.e4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wojczakowski, W.; Kimber-Trojnar, Ż.; Dziwisz, F.; Słodzińska, M.; Słodziński, H.; Leszczyńska-Gorzelak, B. Preeclampsia and Cardiovascular Risk for Offspring. J. Clin. Med. 2021, 10, 3154. [Google Scholar] [CrossRef]
- McKinnon, K.; Huertas-Ceballos, A. Developmental follow-up of children and young people born preterm, NICE guideline 2017. Arch. Dis. Child. Educ. Pract. Ed. 2019, 104, 221–223. [Google Scholar] [CrossRef] [PubMed]
- Appleton, A.A.; Murphy, M.A.; Koestler, D.C.; Lesseur, C.; Paquette, A.G.; Padbury, J.F.; Lester, B.M.; Marsit, C.J. Prenatal Programming of Infant Neurobehaviour in a Healthy Population. Paediatr. Perinat. Epidemiol. 2016, 30, 367–375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jaddoe, V.W.; van Duijn, C.M.; Franco, O.H.; van der Heijden, A.J.; van Iizendoorn, M.H.; de Jongste, J.C.; van der Lugt, A.; Mackenbach, J.P.; Moll, H.A.; Raat, H.; et al. The Generation R Study: Design and cohort update 2012. Eur. J. Epidemiol. 2012, 27, 739–756. [Google Scholar] [CrossRef] [Green Version]
- Janssen, B.G.; Madhloum, N.; Gyselaers, W.; Bijnens, E.; Clemente, D.B.; Cox, B.; Hogervorst, J.; Luyten, L.; Martens, D.S.; Peusens, M.; et al. Cohort Profile: The ENVIRonmental influence ON early AGEing (ENVIRONAGE): A birth cohort study. Int. J. Epidemiol. 2017, 46, 1386–1387m. [Google Scholar] [CrossRef]
- Redline, R.W.; Heller, D.; Keating, S.; Kingdom, J. Placental diagnostic criteria and clinical correlation—A workshop report. Placenta 2005, 26 (Suppl. A), S114–S117. [Google Scholar] [CrossRef]
- Khong, T.Y.; Mooney, E.E.; Ariel, I.; Balmus, N.C.; Boyd, T.K.; Brundler, M.A.; Derricott, H.; Evans, M.J.; Faye-Petersen, O.M.; Gillan, J.E.; et al. Sampling and Definitions of Placental Lesions: Amsterdam Placental Workshop Group Consensus Statement. Arch. Pathol. Lab. Med. 2016, 140, 698–713. [Google Scholar] [CrossRef] [Green Version]
- Thiese, M.S. Observational and interventional study design types; an overview. Biochem. Med. 2014, 24, 199–210. [Google Scholar] [CrossRef]
- Fewell, Z.; Davey Smith, G.; Sterne, J.A. The impact of residual and unmeasured confounding in epidemiologic studies: A simulation study. Am. J. Epidemiol. 2007, 166, 646–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinheiro, T.V.; Brunetto, S.; Ramos, J.G.; Bernardi, J.R.; Goldani, M.Z. Hypertensive disorders during pregnancy and health outcomes in the offspring: A systematic review. J. Dev. Orig. Health Dis. 2016, 7, 391–407. [Google Scholar] [CrossRef] [PubMed]
- Jansen, M.A.; Pluymen, L.P.; Dalmeijer, G.W.; Groenhof, T.K.J.; Uiterwaal, C.S.; Smit, H.A.; van Rossem, L. Hypertensive disorders of pregnancy and cardiometabolic outcomes in childhood: A systematic review. Eur. J. Prev. Cardiol. 2019, 26, 1718–1747. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McPhee, P.G.; Singh, S.; Morrison, K.M. Childhood Obesity and Cardiovascular Disease Risk: Working Toward Solutions. Can. J. Cardiol. 2020, 36, 1352–1361. [Google Scholar] [CrossRef]


| Name of the Instrument | Outcome Measured | Studies Using the Instrument |
|---|---|---|
| Bayley Scales of Infant Development II or III | Mental developmental index | Hendson, 2011 [68], Torrance, 2010 [69], Vilahur, 2014 [62], Mir, 2015 [72], Mir, 2021 [64] |
| Griffiths Mental Development Scale | Developmental quotient | Torrance, 2010 [69], Kaukola, 2005 [70], Spinillo, 2021 [71] |
| Mullen Scales of Early Learning | Gross and fine motor, visual reception, receptive and expressive language | Ueda, 2022 [73] |
| School-Age Differential Ability Scales-II Verbal and Non-verbal reasoning scales | General cognitive ability (IQ), executive function, and working memory | Meakin, 2018 [76] |
| NEPSY-II | Executive function, auditory attention, set switching, concept generation, mental flexibility, and inhibition | Meakin, 2018 [76] |
| Vineland Adaptive Behavior Scale | Communication, daily living, socialization, and motor skills | Limperopoulos, 2008 [67] |
| Child Behavior Checklist | Behavioral and emotional problems | Limperopoulos, 2008 [67] |
| Behavior Assessment System for Children-2 | Behavioral and emotional problems | Nomura, 2021 [74] |
| Rutter B2 scale | Psychiatric disturbance, especially ADHD symptoms | Khalife, 2012 [63] |
| CHAT-23 | Autistic traits | Zhu, 2021 [61] |
| M-CHAT | Autistic traits | Limperopoulos, 2008 [67], Mir, 2021 [64] |
| Autism Diagnostics Observation Schedule-II | Assessment for diagnosing ASD | Mir, 2021 [64] |
| Childhood Autism Rating Scale-II | Assessment for diagnosing ASD | Mir, 2021 [64] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lodefalk, M.; Chelslín, F.; Patriksson Karlsson, J.; Hansson, S.R. Placental Changes and Neuropsychological Development in Children—A Systematic Review. Cells 2023, 12, 435. https://doi.org/10.3390/cells12030435
Lodefalk M, Chelslín F, Patriksson Karlsson J, Hansson SR. Placental Changes and Neuropsychological Development in Children—A Systematic Review. Cells. 2023; 12(3):435. https://doi.org/10.3390/cells12030435
Chicago/Turabian StyleLodefalk, Maria, Felix Chelslín, Johanna Patriksson Karlsson, and Stefan R. Hansson. 2023. "Placental Changes and Neuropsychological Development in Children—A Systematic Review" Cells 12, no. 3: 435. https://doi.org/10.3390/cells12030435