
Vasoactive Soluble Endoglin: A Novel Biomarker Indicative of Reperfusion after Cerebral Large-Vessel Occlusion
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients, Blood Samples and Neuroradiological Scoring
2.2. Enzyme-Linked Immunosorbent Assay
2.3. Statistics
3. Results
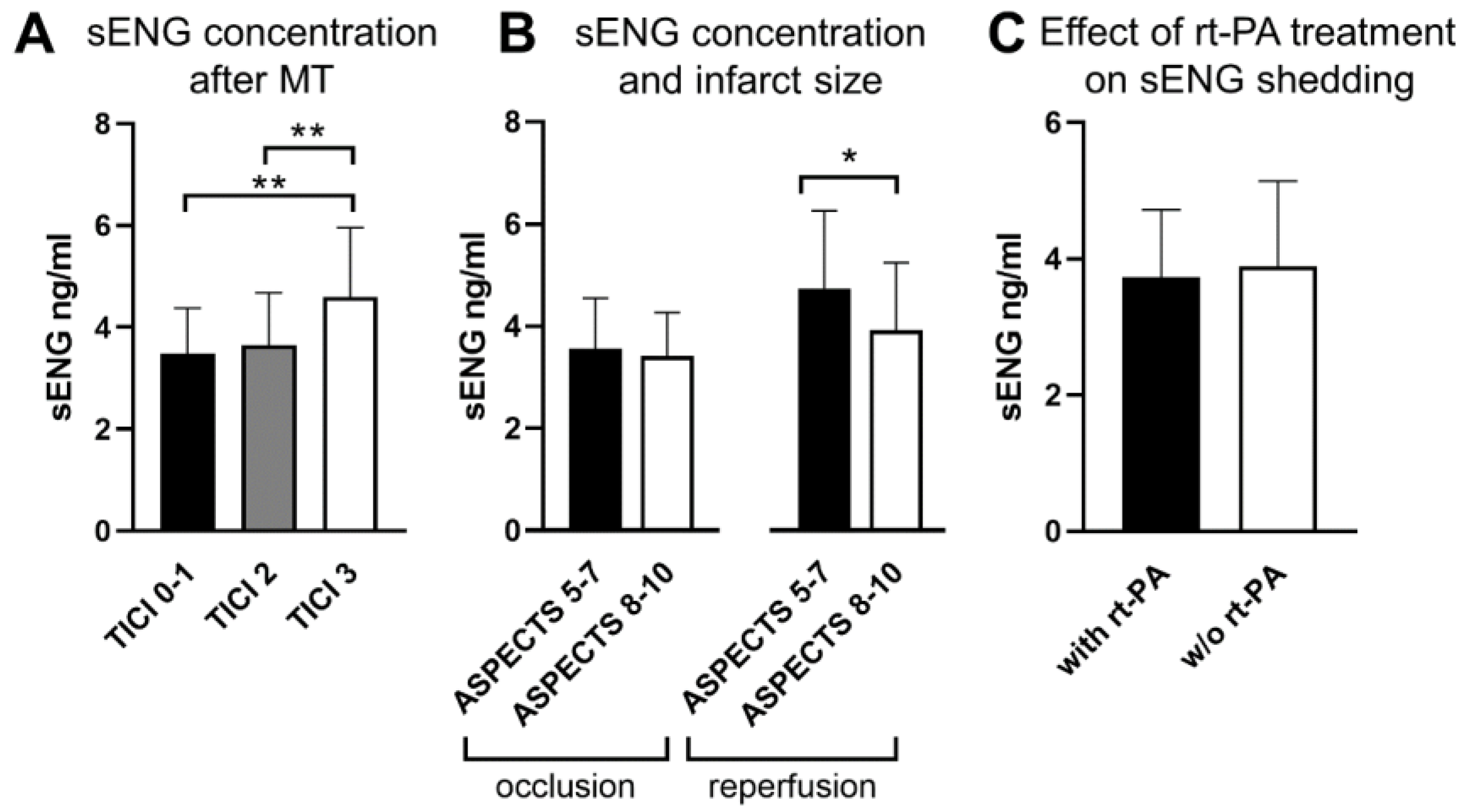
3.1. Elevated Systemic sENG Concentrations Indicate Successful Reperfusion and Reflect Infarct Volume
3.2. Recombinant Tissue Plasminogen Activator Treatment Does Not Change sENG Release in LVO Stroke Patients
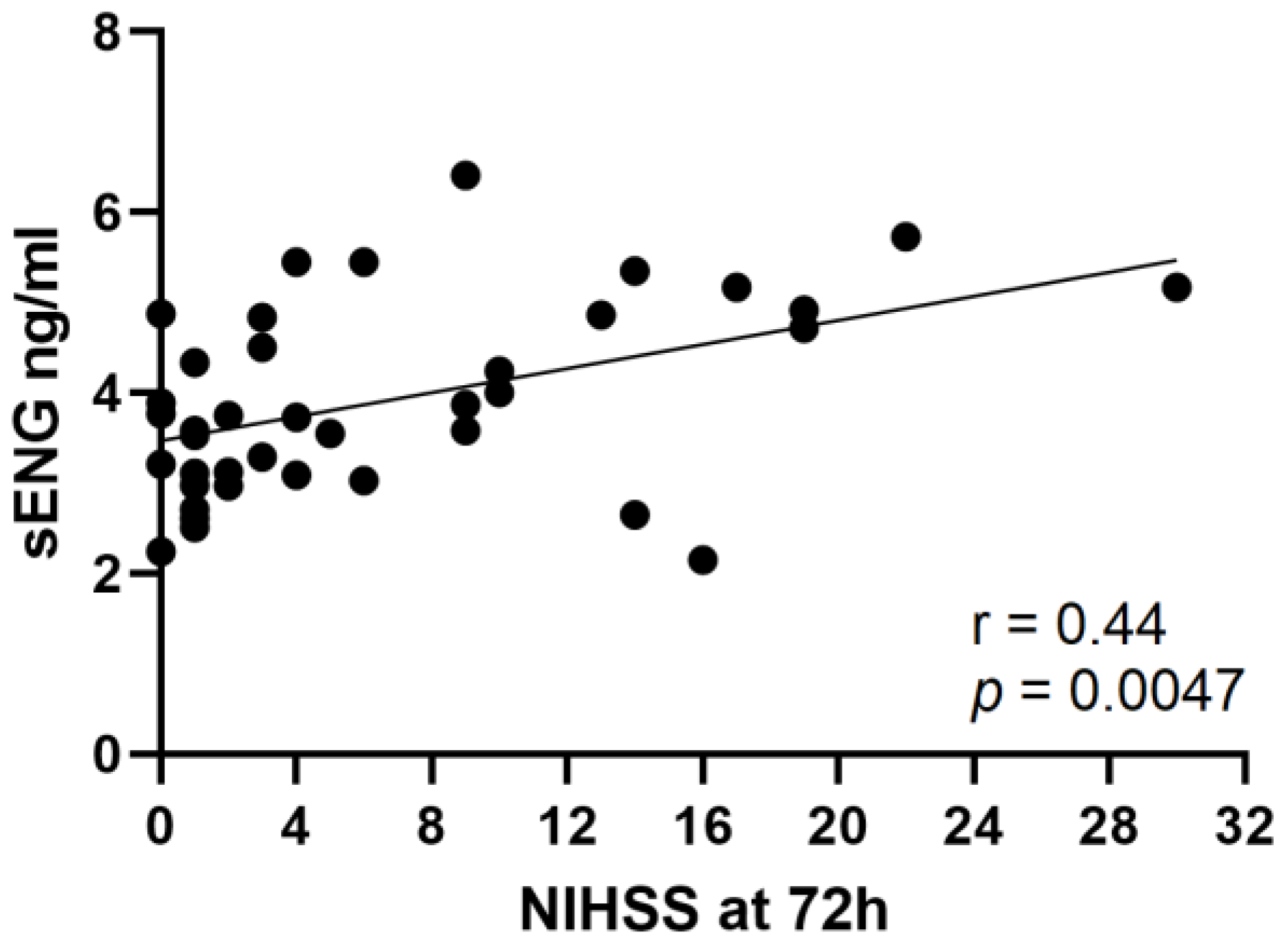
3.3. Concentrations of sENG Positively Correlate with NIHSS after 72 h
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Stoll, G.; Nieswandt, B. Thrombo-inflammation in acute ischaemic stroke—Implications for treatment. Nat. Rev. Neurol. 2019, 15, 473–481. [Google Scholar] [CrossRef] [PubMed]
- Dagonnier, M.; Donnan, G.A.; Davis, S.M.; Dewey, H.M.; Howells, D.W. Acute Stroke Biomarkers: Are We There Yet? Front. Neurol. 2021, 12, 619721. [Google Scholar] [CrossRef] [PubMed]
- Haarmann, A.; Zimmermann, L.; Bieber, M.; Silwedel, C.; Stoll, G.; Schuhmann, M.K. Regulation and Release of Vasoactive Endoglin by Brain Endothelium in Response to Hypoxia/Reoxygenation in Stroke. Int. J. Mol. Sci. 2022, 23, 7085. [Google Scholar] [CrossRef] [PubMed]
- Kollikowski, A.M.; Schuhmann, M.K.; Nieswandt, B.; Mullges, W.; Stoll, G.; Pham, M. Local Leukocyte Invasion during Hyperacute Human Ischemic Stroke. Ann. Neurol. 2020, 87, 466–479. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Barber, P.A.; Demchuk, A.M.; Zhang, J.; Buchan, A.M. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score. Lancet 2000, 355, 1670–1674. [Google Scholar] [CrossRef] [PubMed]
- Bellut, M.; Raimondi, A.T.; Haarmann, A.; Zimmermann, L.; Stoll, G.; Schuhmann, M.K. NLRP3 Inhibition Reduces rt-PA Induced Endothelial Dysfunction under Ischemic Conditions. Biomedicines 2022, 10, 762. [Google Scholar] [CrossRef] [PubMed]
- Essig, F.; Kollikowski, A.M.; Mullges, W.; Stoll, G.; Haeusler, K.G.; Schuhmann, M.K.; Pham, M. Local Cerebral Recombinant Tissue Plasminogen Activator Concentrations During Acute Stroke. JAMA Neurol. 2021, 78, 615–617. [Google Scholar] [CrossRef] [PubMed]
- Tian, F.; Zhou, A.X.; Smits, A.M.; Larsson, E.; Goumans, M.J.; Heldin, C.H.; Boren, J.; Akyurek, L.M. Endothelial cells are activated during hypoxia via endoglin/ALK-1/SMAD1/5 signaling in vivo and in vitro. Biochem. Biophys. Res. Commun. 2010, 392, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Kallmann, B.A.; Hummel, V.; Lindenlaub, T.; Ruprecht, K.; Toyka, K.V.; Rieckmann, P. Cytokine-induced modulation of cellular adhesion to human cerebral endothelial cells is mediated by soluble vascular cell adhesion molecule-1. Brain 2000, 123 Pt 4, 687–697. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Haarmann, A.; Nowak, E.; Deiss, A.; van der Pol, S.; Monoranu, C.M.; Kooij, G.; Muller, N.; van der Valk, P.; Stoll, G.; de Vries, H.E.; et al. Soluble VCAM-1 impairs human brain endothelial barrier integrity via integrin alpha-4-transduced outside-in signalling. Acta Neuropathol. 2015, 129, 639–652. [Google Scholar] [CrossRef] [PubMed]
- Stoll, G.; Schuhmann, M.K.; Nieswandt, B.; Kollikowski, A.M.; Pham, M. An intravascular perspective on hyper-acute neutrophil, T-cell and platelet responses: Similarities between human and experimental stroke. J. Cereb. Blood Flow Metab. 2022, 42, 1561–1567. [Google Scholar] [CrossRef] [PubMed]
- Rossi, E.; Pericacho, M.; Bachelot-Loza, C.; Pidard, D.; Gaussem, P.; Poirault-Chassac, S.; Blanco, F.J.; Langa, C.; Gonzalez-Manchon, C.; Novoa, J.M.L.; et al. Human endoglin as a potential new partner involved in platelet-endothelium interactions. Cell. Mol. Life Sci. 2018, 75, 1269–1284. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Variable | % | Mean | 95% CI | min.–max. | n |
|---|---|---|---|---|---|
| Age (y) | 76.2 | 74.1–78.2 | 22–99 | 148 | |
| Female sex | 54.7 | 81 | |||
| Subjected to MT | 87.0 | 129 | |||
| Received i.v. rt-PA | 40.5 | 60 | |||
| ASPECTS | 7.4 | 7.1–7.6 | 1–10 | 148 | |
| sENG concentration i.v. (ng/mL) | 3.77 | 3.6–3.9 | 1.9–8.0 | 148 | |
| sENG concentration i.a. cerebral (ng/mL) | 2.2 | 1.9–2.5 | 0.9–4.1 | 31 | |
| sENG concentration i.a. systemic (ng/mL) | 2.1 | 1.8–2.4 | 0.6–4.1 | 31 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Haarmann, A.; Vollmuth, C.; Kollikowski, A.M.; Heuschmann, P.U.; Pham, M.; Stoll, G.; Neugebauer, H.; Schuhmann, M.K. Vasoactive Soluble Endoglin: A Novel Biomarker Indicative of Reperfusion after Cerebral Large-Vessel Occlusion. Cells 2023, 12, 288. https://doi.org/10.3390/cells12020288
Haarmann A, Vollmuth C, Kollikowski AM, Heuschmann PU, Pham M, Stoll G, Neugebauer H, Schuhmann MK. Vasoactive Soluble Endoglin: A Novel Biomarker Indicative of Reperfusion after Cerebral Large-Vessel Occlusion. Cells. 2023; 12(2):288. https://doi.org/10.3390/cells12020288
Chicago/Turabian StyleHaarmann, Axel, Christoph Vollmuth, Alexander M. Kollikowski, Peter U. Heuschmann, Mirko Pham, Guido Stoll, Hermann Neugebauer, and Michael K. Schuhmann. 2023. "Vasoactive Soluble Endoglin: A Novel Biomarker Indicative of Reperfusion after Cerebral Large-Vessel Occlusion" Cells 12, no. 2: 288. https://doi.org/10.3390/cells12020288