
Diagnostic Value and Prognostic Significance of Nucleated Red Blood Cells (NRBCs) in Selected Medical Conditions
 , ,
, ,
Abstract
:1. Introduction
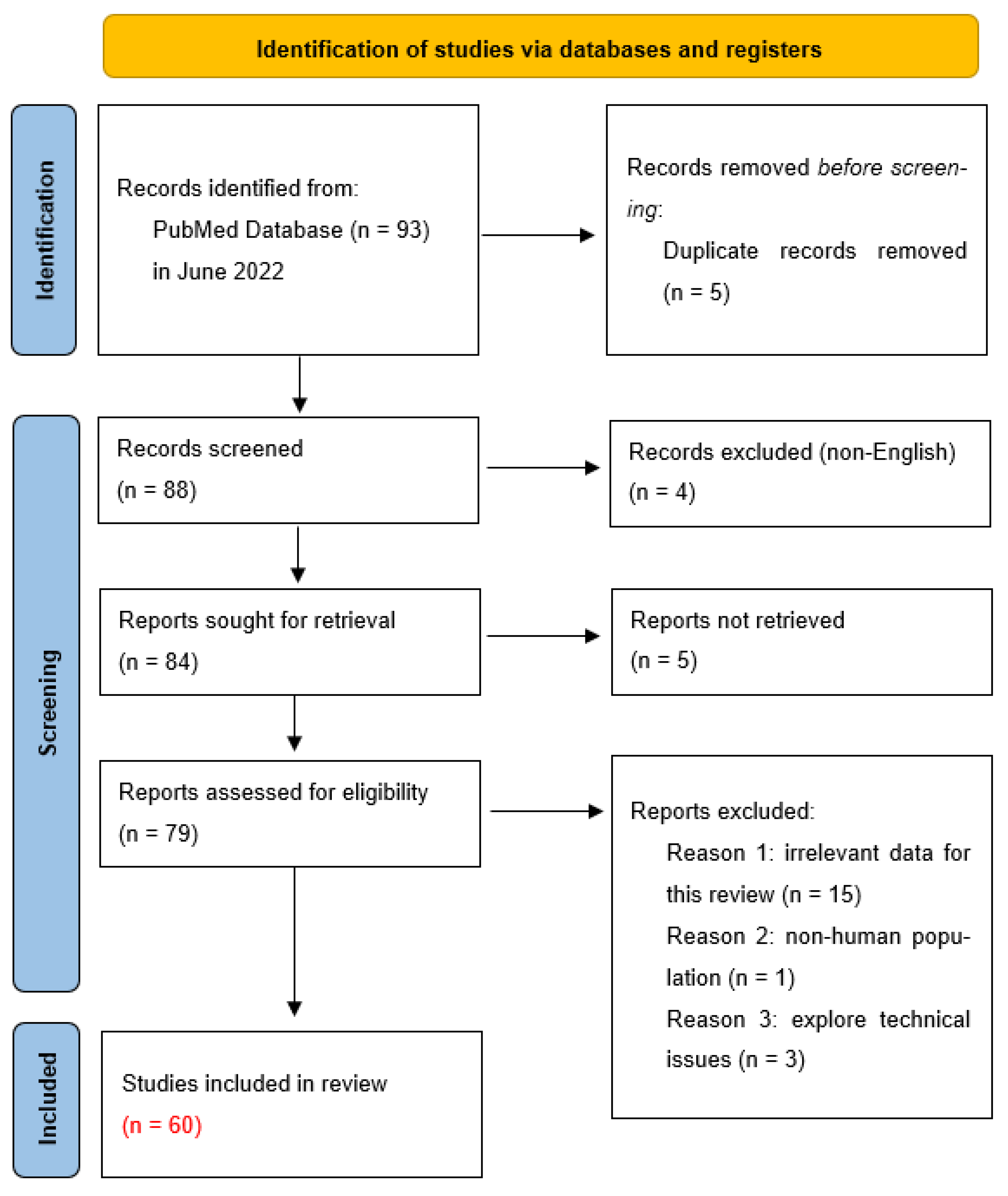
2. Materials and Methods
3. NRBCs as a Biomarker in Neonatology
3.1. NRBCs as an Indicator of Hypoxia among Neonates
3.2. NRBCs as a Marker of Infant Mortality
3.3. NRBCs as a Prognostic and Diagnostic Factor in Perinatal Asphyxia
4. NRBCs in Hematological Conditions
5. NRBCs as a Marker of Bad Prognosis and Mortality in Severely Ill Patients
6. NRBCs as a Diagnostic Method for Thalassemia
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chinudomwong, P.; Khongjaroensakun, N.; Chatachote, B.; Chaothai, N.; Paisooksantivatana, K. Improving the efficiency of the autoverification workflow for nucleated red blood cell reporting in the hematology laboratory. Int. J. Lab. Hematol. 2021, 43, 1373–1378. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, S.J.; Chok, R.; McKillop, S.; Rojas-Vasquez, M.; Duff, J.P.; Szkotak, A.; Bruce, A.A. Peripheral Nucleated Red Blood Cells and Mortality in Critically Ill Children. J. Pediatr. Hematol. Oncol. 2021, 44, 79–83. [Google Scholar] [CrossRef] [PubMed]
- Bergens, M.A.; Pittman, G.S.; Thompson, I.J.B.; Campbell, M.R.; Wang, X.; Hoyo, C.; Bell, D.A. Smoking-associated AHRR demethylation in cord blood DNA: Impact of CD235a+ nucleated red blood cells. Clin. Epigenetics 2019, 11, 87. [Google Scholar] [CrossRef] [PubMed]
- Poryo, M.; Wissing, A.; Aygün, A.; Geisel, J.; Wagenpfeil, S.; Zemlin, M.; Meyer, S. Reference values for nucleated red blood cells and serum lactate in very and extremely low birth weight infants in the first week of life. Early Hum. Dev. 2017, 105, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Nandakumar, S.K.; Ulirsch, J.C.; Sankaran, V.G. Advances in understanding erythropoiesis: Evolving perspectives. Br. J. Haematol. 2016, 173, 206–218. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsiftsoglou, A.S. Erythropoietin (EPO) as a Key Regulator of Erythropoiesis, Bone Remodeling and Endothelial Transdifferentiation of Multipotent Mesenchymal Stem Cells (MSCs): Implications in Regenerative Medicine. Cells 2021, 10, 2140. [Google Scholar] [CrossRef]
- Morton, S.U.; Brettin, K.; Feldman, H.A.; Leeman, K.T. Association of nucleated red blood cell count with mortality among neonatal intensive care unit patients. Pediatr. Neonatol. 2020, 61, 592–597. [Google Scholar] [CrossRef]
- Hebbar, S.; Misha, M.; Rai, L. Significance of Maternal and Cord Blood Nucleated Red Blood Cell Count in Pregnancies Complicated by Preeclampsia. J. Pregnancy 2014, 2014, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Kovalak, E.E.; Dede, F.S.; Gelisen, O.; Dede, H.; Haberal, A. Nonreassuring fetal heart rate patterns and nucleated red blood cells in term neonates. Arch. Gynecol. Obstet. 2010, 283, 1005–1009. [Google Scholar] [CrossRef]
- Shin, S.; Lee, H.R.; Yoon, J.H.; Kim, B.J.; Kim, N.; Park, H.; Roh, E.Y. Increased Nucleated RBCs in Cord Blood: Not an Exclusion Criterion but a Quality Indicator for Hematopoietic Progenitor Cell Transplantation. Transfus. Med. Rev. 2021, 35, 53–59. [Google Scholar] [CrossRef]
- Griffiths, R.E.; Kupzig, S.; Cogan, N.; Mankelow, T.J.; Betin, V.M.S.; Trakarnsanga, K.; Massey, E.J.; Lane, J.D.; Parsons, S.F.; Anstee, D.J. Maturing reticulocytes internalize plasma membrane in glycophorin A–containing vesicles that fuse with autophagosomes before exocytosis. Blood 2012, 119, 6296–6306. [Google Scholar] [CrossRef] [Green Version]
- Gunay, N.E.; Çakır, I.; Çelik, T. Is there clinical value in counting nucleated red blood cells and platelet indices in primary immunodeficiency disease? Turk. J. Pediatr. 2017, 59, 657–663. [Google Scholar] [CrossRef]
- Davari-Tanha, F.; Kaveh, M.; Nemati, S.; Javadian, P.; Salmanian, B. Nucleated Red Blood Cells Count in Pregnancies with Idiopathic Intra-Uterine Growth Restriction. J. Fam. Reprod. Health 2014, 8, 77–81. [Google Scholar]
- Lippi, G.; Pavesi, F.; Cattabiani, C.; Avanzini, P.; Pipitone, S. Influence of in vitro hemolysis on nucleated red blood cells and reticulocyte counts. Int. J. Lab. Hematol. 2012, 35, 225–228. [Google Scholar] [CrossRef]
- Christensen, R.D.; Henry, E.; Andres, R.L.; Bennett, S.T. Reference Ranges for Blood Concentrations of Nucleated Red Blood Cells in Neonates. Neonatology 2010, 99, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Christensen, R.D.; Lambert, D.K.; Richards, D.S. Estimating the nucleated red blood cell ‘emergence time’ in neonates. J. Perinatol. 2013, 34, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Goel, M.; Dwivedi, R.; Gohiya, P.; Hegde, D. Nucleated red blood cell in cord blood as a marker of perinatal asphyxia. J. Clin. Neonatol. 2013, 2, 179–182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cremer, M.; Roll, S.; Gräf, C.; Weimann, A.; Bührer, C.; Dame, C. Nucleated red blood cells as marker for an increased risk of unfavorable outcome and mortality in very low birth weight infants. Early Hum. Dev. 2015, 91, 559–563. [Google Scholar] [CrossRef] [PubMed]
- Boskabadi, H.; Pourbadakhshan, N.; Pishghadam, E.; Zakerihamidi, M. Comparing Nucleated Red Blood Cells in Neonates with and without Retinopathy. Curr. Pediatr. Rev. 2021, 17, 1. [Google Scholar] [CrossRef]
- Hu, G.; Guan, R.; Li, L. Nucleated Red Blood Cell Count in Maternal Peripheral Blood and Hypertensive Disorders in Pregnant Women. Am. J. Med. Sci. 2016, 351, 140–146. [Google Scholar] [CrossRef] [PubMed]
- Ballantine, J.D.; Kwon, S.; Liem, R.I. Nucleated Red Blood Cells in Children with Sickle Cell Disease Hospitalized for Pain. J. Pediatr. Hematol. Oncol. 2019, 41, e487–e492. [Google Scholar] [CrossRef] [PubMed]
- Narcı, H.; Oktay, M.M.; Ayrık, C.; Çimen, M.B.Y. Nucleated red blood cells as predictor of all-cause mortality in emergency department. Am. J. Emerg. Med. 2020, 46, 335–338. [Google Scholar] [CrossRef] [PubMed]
- Phan, T.T.; Vy, H.T.; Ho, T.T.; Tran, V.T.; Tran, T.T.; Pho, S.P.; Pham, T.T.B.; Le, T.T.; Nguyen, S.T. Emergence role of nucleated red blood cells in molecular response evaluation for chronic myeloid leukemia. Int. J. Gen. Med. 2019, 12, 333–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matarraz, S.; Teodosio, C.; Fernandez, C.; Albors, M.; Jara-Acevedo, M.; López, A.; Gonzalez-Gonzalez, M.; Gutierrez, M.L.; Flores-Montero, J.; Cerveró, C.; et al. The Proliferation Index of Specific Bone Marrow Cell Compartments from Myelodysplastic Syndromes Is Associated with the Diagnostic and Patient Outcome. PLoS ONE 2012, 7, e44321. [Google Scholar] [CrossRef] [Green Version]
- Stachon, A.; Segbers, E.; Holland-Letz, T.; Kempf, R.; Hering, S.; Krieg, M. Nucleated red blood cells in the blood of medical intensive care patients indicate increased mortality risk: A prospective cohort study. Crit. Care 2007, 11, R62. [Google Scholar] [CrossRef] [Green Version]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Millar, L.J.; Shi, L.; Hoerder-Suabedissen, A.; Molnár, Z. Neonatal Hypoxia Ischaemia: Mechanisms, Models, and Therapeutic Challenges. Front. Cell. Neurosci. 2017, 11, 78. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, M.H.; Moustafa, A.N.; Saedii, A.A.F.; Hassan, E.E. Cord blood erythropoietin and cord blood nucleated red blood cells for prediction of adverse neonatal outcome associated with maternal obesity in term pregnancy: Prospective cohort study. J. Matern. Fetal. Neonatal Med. 2016, 30, 2237–2242. [Google Scholar] [CrossRef]
- Schödel, J.; Ratcliffe, P.J. Mechanisms of hypoxia signalling: New implications for nephrology. Nat. Rev. Nephrol. 2019, 15, 641–659. [Google Scholar] [CrossRef]
- Haase, V.H. Regulation of erythropoiesis by hypoxia-inducible factors. Blood Rev. 2013, 27, 41–53. [Google Scholar] [CrossRef] [Green Version]
- Nitzan, I.; Roberts, C.T.; Bhatia, R.; Mimouni, F.B.; Sehgal, A. Nucleated Red Blood Cells as Markers of Perinatal Adaptation in Preterm Neonates Receiving Minimally Invasive Surfactant Therapy. Am. J. Perinatol. 2021, 39, 1792–1795. [Google Scholar] [CrossRef]
- Walsh, B.; Boylan, G.; Dempsey, E.; Murray, D. Association of nucleated red blood cells and severity of encephalopathy in normothermic and hypothermic infants. Acta Paediatr. 2012, 102, e64–e67. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Kobata, K.; Kamei, Y.; Okazaki, Y.; Nishihara, M.; Wada, H.; Tamai, H.; Funato, M.; Jenkin, G. Nucleated red blood cell counts: An early predictor of brain injury and 2-year outcome in neonates with hypoxic–ischemic encephalopathy in the era of cooling-based treatment. Brain Dev. 2014, 36, 472–478. [Google Scholar] [CrossRef] [PubMed]
- Walsh, B.; Boylan, G.; Murray, D. Nucleated Red Blood Cells and early EEG: Predicting Sarnat stage and two year outcome. Early Hum. Dev. 2011, 87, 335–339. [Google Scholar] [CrossRef]
- Gohir, W.; Kennedy, K.M.; Wallace, J.G.; Saoi, M.; Bellissimo, C.J.; Britz-McKibbin, P.; Petrik, J.J.; Surette, M.G.; Sloboda, D.M. High-fat diet intake modulates maternal intestinal adaptations to pregnancy and results in placental hypoxia, as well as altered fetal gut barrier proteins and immune markers. J. Physiol. 2019, 597, 3029–3051. [Google Scholar] [CrossRef]
- Åmark, H.; Sirotkina, M.; Westgren, M.; Papadogiannakis, N.; Persson, M. Is obesity in pregnancy associated with signs of chronic fetal hypoxia? Acta Obstet. et Gynecol. Scand. 2020, 99, 1649–1656. [Google Scholar] [CrossRef]
- Persson, M.; Johansson, S.; Villamor, E.; Cnattingius, S. Maternal Overweight and Obesity and Risks of Severe Birth-Asphyxia-Related Complications in Term Infants: A Population-Based Cohort Study in Sweden. PLoS Med. 2014, 11, e1001648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mendes, R.F.P.; Martinelli, S.; Bittar, R.E.; Francisco, R.P.V.; Zugaib, M. Relation between Nucleated Red Blood Cell Count in Umbilical Cord and the Obstetric and Neonatal Outcomes in Small for Gestational Age Fetuses and with Normal Doppler Velocimetry of Umbilical Artery. Rev. Bras. Ginecol. Obstet. 2015, 37, 455–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jahromi, B.N.; Ahmadi, N.; Cohan, N.; Jahromi, M.R.N. Comparison of the umbilical artery blood gas, nucleated red blood cell, C-reactive protein, and white blood cell differential counts between neonates of diabetic and nondiabetic mothers. Taiwan. J. Obstet. Gynecol. 2011, 50, 301–305. [Google Scholar] [CrossRef] [Green Version]
- Elsokkary, M.; Mamdouh, A.; Nossair, W.; El Fattah, O.A.; Hemeda, H.; Sallam, S.; Taema, M.; Hussain, M.; Shafik, A.; Nawara, M.; et al. Significance of assay of nucleated RBCs in umbilical cord blood in neonates with meconium-stained amniotic fluid. J. Matern. Neonatal Med. 2017, 32, 483–487. [Google Scholar] [CrossRef]
- Schaer, C.; Schmugge, M.; Frey, B. Prognostic value of nucleated red blood cells in critically ill children. Swiss. Med. Wkly. 2014, 144, w13944. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Romero, R.; Savasan, Z.A.; Chaiworapongsa, T.; Berry, S.M.; Kusanovic, J.P.; Hassan, S.S.; Yoon, B.H.; Edwin, S.; Mazor, M. Hematologic profile of the fetus with systemic inflammatory response syndrome. J. Périnat. Med. 2011, 40, 19–32. [Google Scholar] [CrossRef] [PubMed]
- Gasparović, V.E.; Ahmetasević, S.G.; Colić, A. Nucleated red blood cells count as first prognostic marker for adverse neonatal outcome in severe preeclamptic pregnancies. Coll. Antropol. 2012, 36, 853–857. [Google Scholar] [PubMed]
- Piggott, K.D.; Norlin, C.; Laviolette, C.; Turner, J.; Lewis, L.; Soliman, A.; Hebert, D.; Pettitt, T. Nucleated red blood cells as a biomarker for mortality in infants and neonates requiring veno-arterial extracorporeal membrane oxygenation for cardiac disease. Perfusion 2021, 38, 299–304. [Google Scholar] [CrossRef]
- Piggott, K.D.; Maqsood, S.; Warner, C.L.; Pettitt, T.; Yang, S.; Turner, J.; Soliman, A.; Norlin, C.; Lewis, L.; Bhatia, A. Nucleated red blood cells as a biomarker for mortality in neonates following cardiac surgery. Cardiol. Young 2021, 32, 1048–1052. [Google Scholar] [CrossRef]
- Fattuoni, C.; Palmas, F.; Noto, A.; Fanos, V.; Barberini, L. Perinatal Asphyxia: A Review from a Metabolomics Perspective. Molecules 2015, 20, 7000–7016. [Google Scholar] [CrossRef]
- Rai, R.; Tripathi, G.; Singh, D.K. Nucleated RBC Count as Predictor of Neurological Outcome in Perinatal Asphyxia Hypoxemic Ischaemic Encephalopathy. Indian Pediatr. 2014, 51, 231–232. [Google Scholar] [CrossRef]
- Christensen, R.D.; Baer, V.L.; Yaish, H.M. Thrombocytopenia in late preterm and term neonates after perinatal asphyxia. Transfusion 2014, 55, 187–196. [Google Scholar] [CrossRef]
- Wirbelauer, J.; Thomas, W.; Speer, C.P. Response of leukocytes and nucleated red blood cells in very low-birth weight preterm infants after exposure to intrauterine inflammation. J. Matern. Fetal Neonatal Med. 2010, 24, 348–353. [Google Scholar] [CrossRef]
- Boskabadi, H.; Zakerihamidi, M.; Sadeghian, M.H.; Avan, A.; Ghayour-Mobarhan, M.; Ferns, G.A. Nucleated red blood cells count as a prognostic biomarker in predicting the complications of asphyxia in neonates. J. Matern. Neonatal Med. 2016, 30, 2551–2556. [Google Scholar] [CrossRef] [Green Version]
- Jiang, H.; Yang, L.; Guo, L.; Cui, N.; Zhang, G.; Liu, C.; Xing, L.; Shao, Z.; Wang, H. Impaired Mitophagy of Nucleated Erythroid Cells Leads to Anemia in Patients with Myelodysplastic Syndromes. Oxidative Med. Cell. Longev. 2018, 2018, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Júnior, J.G.d.M.M.; Torres, D.d.O.C.; da Silva, M.C.F.C.; Ramos, T.M.d.B.; Alves, M.L.; Filho, W.J.N.; Damasceno, E.P.; Brunet, A.F.; Bittencourt, M.S.; Pedrosa, R.P.; et al. Nucleated Red Blood Cells as Predictors of All-Cause Mortality in Cardiac Intensive Care Unit Patients: A Prospective Cohort Study. PLoS ONE 2015, 10, e0144259. [Google Scholar] [CrossRef] [Green Version]
- Menk, M.; Giebelhäuser, L.; Vorderwülbecke, G.; Gassner, M.; Graw, J.A.; Weiss, B.; Zimmermann, M.; Wernecke, K.-D.; Weber-Carstens, S. Nucleated red blood cells as predictors of mortality in patients with acute respiratory distress syndrome (ARDS): An observational study. Ann. Intensiv. Care 2018, 8, 42. [Google Scholar] [CrossRef] [PubMed]
- Xu, C.; Wang, J.; Jin, X.; Yuan, Y.; Lu, G. Establishment of a predictive model for outcomes in patients with severe acute pancreatitis by nucleated red blood cells combined with Charlson complication index and APACHE II score. Turk. J. Gastroenterol. 2021, 31, 936–941. [Google Scholar] [CrossRef] [PubMed]
- Desai, S.; Jones, S.L.; Turner, K.L.; Hall, J.; Moore, L.J.; Hwang, D.H.; Dorfman, D.M.; Hwang, D.G.; Senna, P.; Pozdnyakova, O.; et al. Nucleated Red Blood Cells Are Associated with a Higher Mortality Rate in Patients with Surgical Sepsis. Surg. Infect. 2012, 13, 360–365. [Google Scholar] [CrossRef]
- Shah, R.; Reddy, S.; Horst, H.M.; Stassinopoulos, J.; Jordan, J.; Rubinfeld, I. Getting back to zero with nucleated red blood cells: Following trends is not necessarily a bad thing. Am. J. Surg. 2012, 203, 343–346. [Google Scholar] [CrossRef]
- Kuert, S.; Holland-Letz, T.; Friese, J.; Stachon, A. Association of nucleated red blood cells in blood and arterial oxygen partial tension. Clin. Chem. Lab. Med. 2010, 49, 257–263. [Google Scholar] [CrossRef]
- Cao, A.; Galanello, R. Beta-thalassemia. Orphanet J. Rare Dis. 2010, 5, 11. [Google Scholar] [CrossRef] [Green Version]
- Shafei, N.; Hakhamaneshi, M.S.; Houshmand, M.; Gerayeshnejad, S.; Fathi, F.; Sharifzadeh, S. Diagnostic Value of Non-Invasive Prenatal Screening of β-thalassemia by Cell Free Fetal DNA and Fetal NRBC. Curr. Mol. Med. 2019, 19, 105–111. [Google Scholar] [CrossRef]
- Wei, H.Y.; Long, G.; Lin, W.X.; Li, S.Q. Noninvasive Prenatal Diagnosis of β-Thalassaemia Using Individual Fetal Erythroblasts Isolated from Maternal Blood after Enrichment. Zhonghua Er Ke Za Zhi 2007, 917–921. [Google Scholar] [CrossRef]
- Karakukcu, M.; Karakukcu, C.; Unal, E.; Ozturk, A.; Ciraci, Z.; Patiroglu, T.; Ozdemir, M.A. The Importance of Nucleated Red Blood Cells in Patients with Beta Thalassemia Major and Comparison of Two Automated Systems with Manual Microscopy and Flow Cytometry. Clin. Lab. 2015, 61, 1289–1295. [Google Scholar] [CrossRef] [PubMed]
- Danise, P.; Amendola, G.; Di Concilio, R.; Cillari, E.; Gioia, M.; Di Palma, A.; Avino, D.; Rigano, P.; Maggio, A. Nucleated red blood cells and soluble transferrin receptor in thalassemia syndromes: Relationship with global and ineffective erythropoiesis. Clin. Chem. Lab. Med. 2009, 47, 1539–1542. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| ↑NRBC | |
|---|---|
| Group | Disorders |
| Neonatal conditions | Hypoxia [16,29,30,31] |
| Asphyxia [17,47,48,50] | |
| Mortality [18,41,43,44,45] | |
| Hematological diseases | Chronic myeloid leukemia [23] |
| Myelodysplastic syndromes [51] | |
| Thalassemia [59,60,61,62] | |
| Critical conditions | Trauma [22,56] |
| Sepsis [55] | |
| Acute pancreatitis [54] | |
| ARDS [53] | |
| Hypoxemia [57] | |
| Hospitalization in the ICU [52] | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pikora, K.; Krętowska-Grunwald, A.; Krawczuk-Rybak, M.; Sawicka-Żukowska, M. Diagnostic Value and Prognostic Significance of Nucleated Red Blood Cells (NRBCs) in Selected Medical Conditions. Cells 2023, 12, 1817. https://doi.org/10.3390/cells12141817
Pikora K, Krętowska-Grunwald A, Krawczuk-Rybak M, Sawicka-Żukowska M. Diagnostic Value and Prognostic Significance of Nucleated Red Blood Cells (NRBCs) in Selected Medical Conditions. Cells. 2023; 12(14):1817. https://doi.org/10.3390/cells12141817
Chicago/Turabian StylePikora, Katarzyna, Anna Krętowska-Grunwald, Maryna Krawczuk-Rybak, and Małgorzata Sawicka-Żukowska. 2023. "Diagnostic Value and Prognostic Significance of Nucleated Red Blood Cells (NRBCs) in Selected Medical Conditions" Cells 12, no. 14: 1817. https://doi.org/10.3390/cells12141817