
C-Reactive Protein Level and the Genetic Variant rs1130864 in the CRP Gene as Prognostic Factors for 10-Year Cardiovascular Outcome
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. CV Patients
2.2.1. Baseline Investigations
2.2.2. Ten-Year Follow-Up Period
2.3. Genetic Investigations
2.4. Statistical Procedures
3. Results
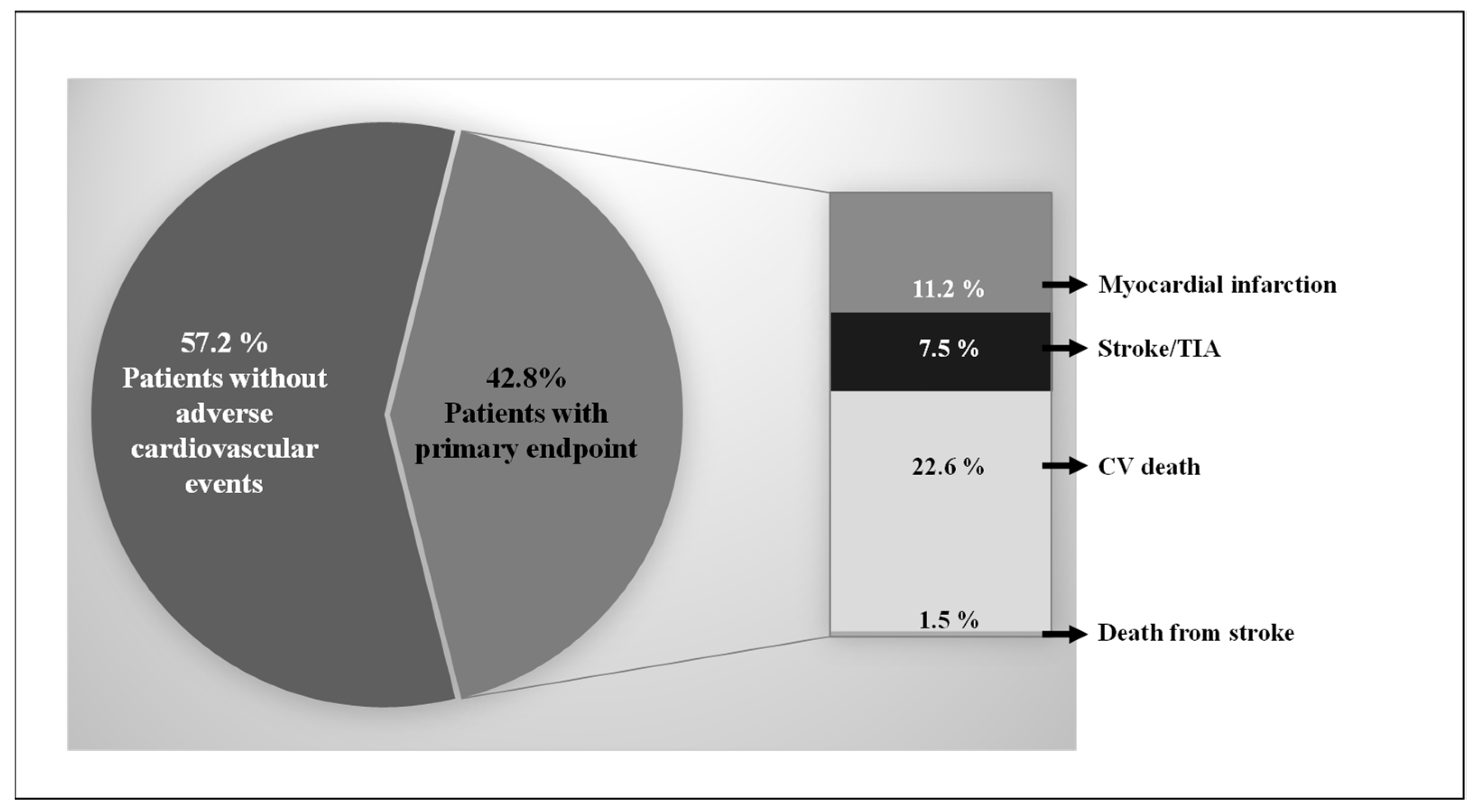
3.1. Clinical Characterisation of CV Patients
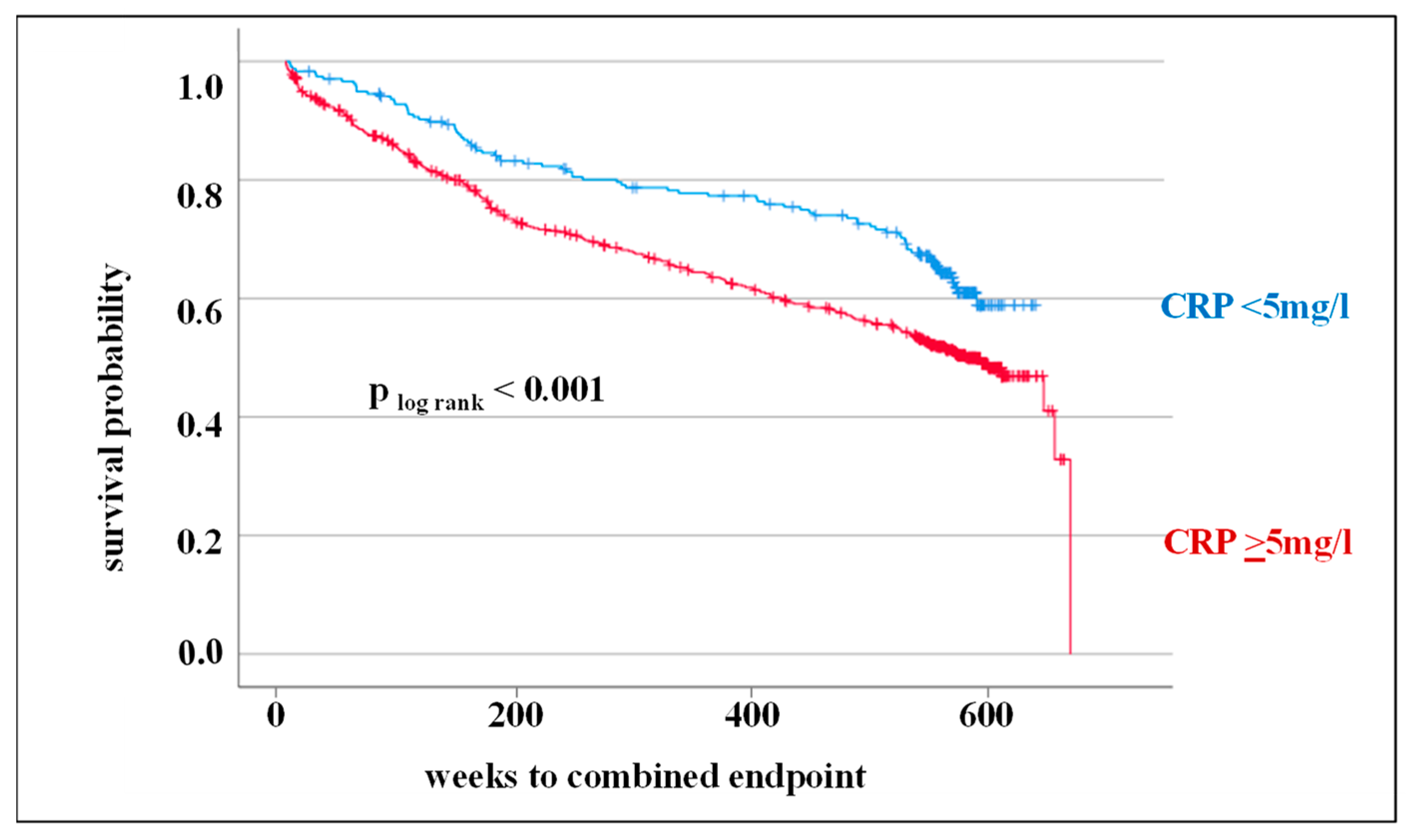
3.2. Circulating CRP Level as Prognostic Markers for Adverse CV Outcome
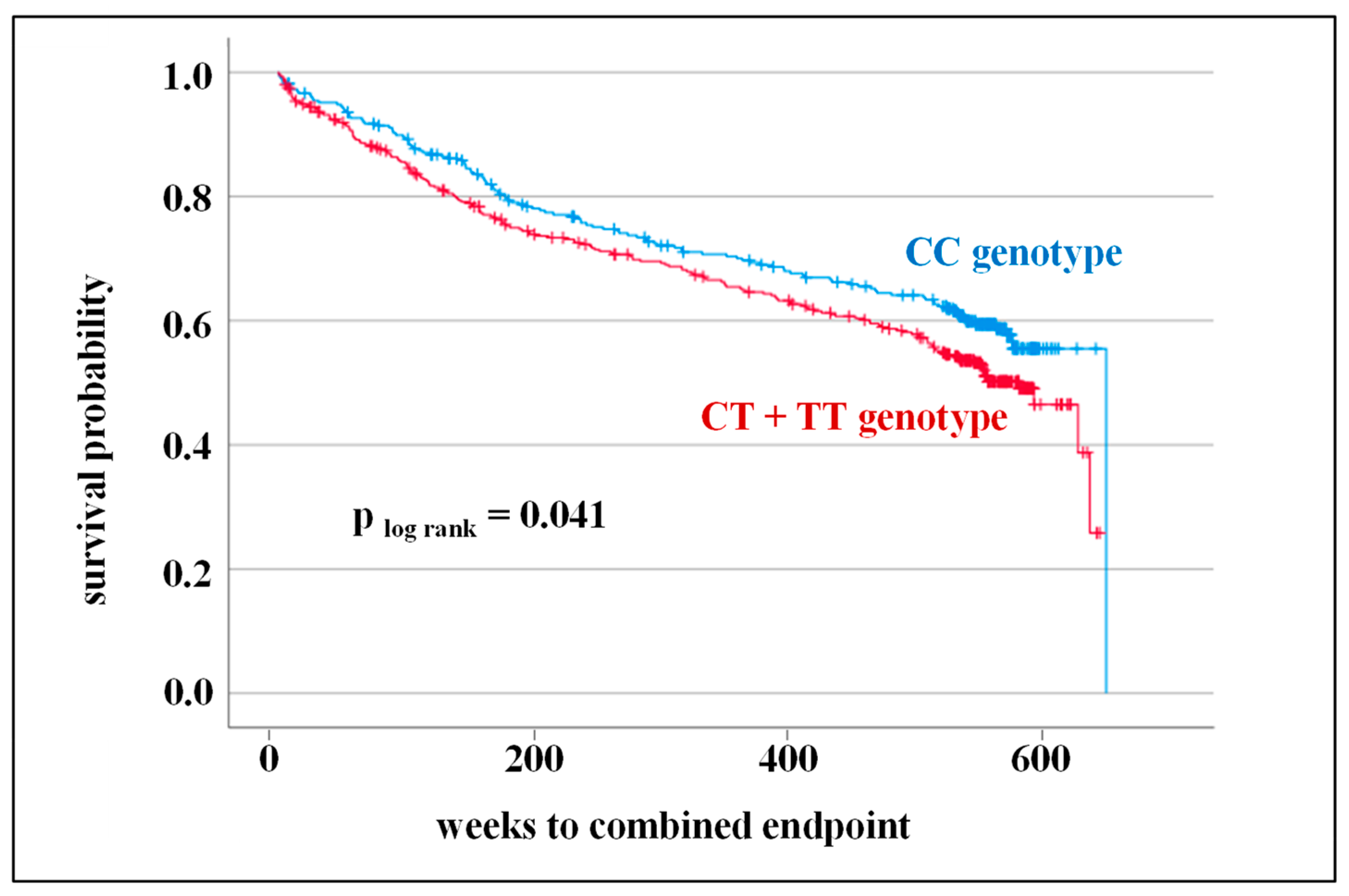
3.3. SNPs in the CRP Gene as Prognostic Markers for Adverse CV Outcome
4. Discussion
4.1. Circulating CRP Level as Prognostic Markers for Adverse CV Outcome
4.2. SNPs in the CRP Gene as Prognostic Markers for Adverse CV Outcome
4.3. Further Prognostic Markers for Adverse CV Outcome
4.4. Limitation of This Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aday, W.A.; Ridker, P.M. Targeting residual inflammatory risk: A shift paradigm for atherosclerotic disease. Front. Cardiovasc. Med. 2019, 28, 16. [Google Scholar] [CrossRef] [Green Version]
- Banait, T.; Wanjari, A.; Danade, V.; Banait, S.; Jain, J. Role of High-Sensitivity C-reactive Protein (Hs-CRP) in Non-communicable Diseases: A Review. Cureus 2022, 14, e30225. [Google Scholar] [CrossRef]
- Ridker, P.M. A test in context: High-sensitivity C-reactive protein. JACC 2016, 67, 712–723. [Google Scholar] [CrossRef]
- Koenig, W. High-sensitive C-reactive protein and atherosclerotic disease: From improved risk prediction to risk-guided therapy. J. Cardiol. 2013, 168, 5126–5134. [Google Scholar]
- He, L.P.; Tang, X.Y.; Ling, W.H.; Chen, W.Q.; Chen, Y.M. Early C-reactive protein in the prediction of long-term outcomes after acute coronary syndromes: A meta-analysis of longitudinal studies. Heart 2010, 96, 339–346. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M. Clinician’s Guide to Reducing Inflammation to Reduce Atherothrombotic Risk: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2018, 72, 3320–3331. [Google Scholar] [CrossRef]
- Libby, P. Inflammation in atherosclerosis—No longer a theory. Clin. Chem. 2021, 67, 131–142. [Google Scholar] [CrossRef]
- Denegri, A.; Boriani, G. High Sensitivity C-reactive Protein (hsCRP) and its Implications in Cardiovascular Outcomes. Curr. Pharm. Des. 2021, 27, 263–275. [Google Scholar] [CrossRef]
- Ridker, P.M.; Rifai, N.; Pfeffer, M.A.; Sacks, F.M.; Moye, L.A.; Goldman, S.; Flaker, G.C.; Braunwald, E. Inflammation, pravastatin, and the risk of coronary events after myocardial infarction in patients with average cholesterol levels. Cholesterol and Recurrent Events (CARE) Investigators. Circulation 1998, 98, 839–844. [Google Scholar] [CrossRef]
- Ridker, P.M.; Danielson, E.; Fonseca, F.A.; Genest, J.; Gotto, A.M.; Kastelein, J.J.; Koenig, W.; Libby, P.; Lorenzatti, A.J.; MacFadyen, J.G.; et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N. Engl. J. Med. 2008, 359, 2195–2207. [Google Scholar] [CrossRef] [Green Version]
- Ridker, P.M. From CANTOS to CIRT to COLCOT to Clinic: Will All Atherosclerosis Patients Soon Be Treated with Combination Lipid-Lowering and Inflammation-Inhibiting Agents? Circulation 2020, 141, 787–789. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G.; Chang, W.H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig, W.; Anker, S.D.; et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M. Testing the inflammatory hypothesis of atherothrombosis: Scientific rationale for the cardiovascular inflammation reduction trial (CIRT). J. Thromb. Haemost. 2009, 7 (Suppl. S1), 332–339. [Google Scholar] [CrossRef] [PubMed]
- Nidorf, S.M.; Fiolet, A.T.L.; Eikelboom, J.W.; Schut, A.; Opstal, T.S.J.; Bax, W.A.; Budgeon, C.A.; Tijssen, J.G.P.; Mosterd, A.; Cornel, J.H.; et al. The effect of low-dose colchicine in patients with stable coronary artery disease: The LoDoCo2 trial rationale, design, and baseline characteristics. Am. Heart J. 2019, 218, 46–56. [Google Scholar] [CrossRef]
- Tardif, J.C.; Kouz, S.; Waters, D.D.; Bertrand, O.F.; Diaz, R.; Maggioni, A.P.; Pinto, F.J.; Ibrahim, R.; Gamra, H.; Kiwan, G.S.; et al. Efficacy and Safety of Low-Dose Colchicine after Myocardial Infarction. N. Engl. J. Med. 2019, 381, 2497–2505. [Google Scholar] [CrossRef]
- Carlson, C.S.; Aldred, S.F.; Lee, P.K.; Tracy, R.P.; Schwartz, S.M.; Rieder, M.; Liu, K.; Williams, O.D.; Iribarren, C.; Lewis, E.C.; et al. Polymorphisms within the C-reactive protein (CRP) promoter region are associated with plasma CRP levels. Am. J. Hum. Genet. 2008, 77, 64–77. [Google Scholar] [CrossRef] [Green Version]
- MacGregor, A.J.; Gallimore, J.R.; Spector, T.D.; Pepys, M.B. Genetic effects on baseline values of C-reactive protein and serum amyloid a protein: A comparison of monozygotic and dizygotic twins. Clin. Chem. 2004, 50, 130–134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wörns, M.A.; Victor, A.; Galle, P.R.; Höhler, T. Genetic and environmental contributions to plasma C-reactive protein and interleukin-6 levels—A study in twins. Genes Immun. 2006, 7, 600–605. [Google Scholar] [CrossRef] [Green Version]
- Ligthart, S.; Vaez, A.; Võsa, U.; Stathopoulou, M.G.; de Vries, P.S.; Prins, B.P.; Van der Most, P.J.; Tanaka, T.; Naderi, E.; Rose, L.M.; et al. Genome Analyses of >200,000 Individuals Identify 58 Loci for Chronic Inflammation and Highlight Pathways that Link Inflammation and Complex Disorders. Am. J. Hum. Genet. 2018, 103, 691–706. [Google Scholar] [CrossRef] [Green Version]
- Said, S.; Pazoki, R.; Karhunen, V.; Võsa, U.; Ligthart, S.; Bodinier, B.; Koskeridis, F.; Welsh, P.; Alizadeh, B.Z.; Chasman, D.I.; et al. Genetic analysis of over half a million people characterises C-reactive protein loci. Nat. Commun. 2022, 13, 2198. [Google Scholar] [CrossRef]
- Schulz, S.; Lüdike, H.; Lierath, M.; Schlitt, A.; Werdan, K.; Hofmann, B.; Gläser, C.; Schaller, H.G.; Reichert, S. C-reactive protein levels and genetic variants of CRP as prognostic markers for combined cardiovascular endpoint (cardiovascular death, death from stroke, myocardial infarction, and stroke/TIA). Cytokine 2016, 88, 71–76. [Google Scholar] [CrossRef] [PubMed]
- Wensley, F.; Gao, P.; Burgess, S.; Kaptoge, S.; Di Angelantonio, E.; Shah, T.; Engert, J.C.; Clarke, R.; Davey-Smith, G.; C Reactive Protein Coronary Heart Disease Genetics Collaboration (CCGC); et al. Association between C reactive protein and coronary heart disease: Mendelian randomisation analysis based on individual participant data. BMJ 2011, 342, d548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fransén, K.; Pettersson, C.; Hurtig-Wennlöf, A. CRP levels are significantly associated with CRP genotype and estrogen use in The Lifestyle, Biomarker and Atherosclerosis (LBA) study. BMC Cardiovasc. Disord. 2022, 22, 170. [Google Scholar] [CrossRef] [PubMed]
- Zacho, J.; Tybjaerg-Hansen, A.; Jensen, J.S.; Grande, P.; Sillesen, H.; Nordestgaard, B.G. Genetically elevated C-reactive protein and ischemic vascular disease. N. Engl. J. Med. 2008, 359, 1897–1908. [Google Scholar] [CrossRef]
- Holmes, M.V.; Ala-Korpela, M.; Smith, G.D. Mendelian randomization in cardiometabolic disease: Challenges in evaluating causality. Nat. Rev. Cardiol. 2017, 14, 577–590. [Google Scholar] [CrossRef] [Green Version]
- Reynoso-Villalpando, G.L.; Casillas-Muñoz, F.A.; Padilla-Gutiérrez, J.R.; Sevillano-Collantes, C.; Moreno-Ruiz, I.; Del Cañizo-Gómez, F.J.; Valdez-Haro, A.; Martínez-Fernández, D.E.; Valle, Y. The Genetic Variants -717T>C (rs2794521), 1444G>A (rs1130864), and 1846 C>T (rs1205) of CRP Gene, Their Haplotypes, and Their Association with Serum CRP Levels, Acute Coronary Syndrome, and Diabetes in Patients from Western Mexico. Metab. Syndr. Relat. Disord. 2021, 19, 127–136. [Google Scholar] [CrossRef]
- Hermann, M.; Fischer, D.; Hoffmann, M.M.; Gasser, T.; Quitzau, K.; Meinertz, T.; Münzel, T.; Lüscher, T.F. CRP and CD14 polymorphisms correlate with coronary plaque volume in patients with coronary artery disease—IVUS substudy of the ENCORE trials. Atherosclerosis 2012, 220, 172–176. [Google Scholar] [CrossRef]
- Zhu, Y.; Liu, T.; He, H.; Sun, Y.; Zhuo, F. C-reactive protein gene polymorphisms and myocardial infarction risk: A meta-analysis and meta-regression. Genet. Test. Mol. Biomark. 2013, 17, 873–880. [Google Scholar] [CrossRef]
- Lange, L.A.; Carlson, C.S.; Hindorff, L.A.; Lange, E.M.; Walston, J.; Durda, J.P.; Cushman, M.; Bis, J.C.; Zeng, D.; Lin, D.; et al. Association of polymorphisms in the CRP gene with circulating C-reactive protein levels and cardiovascular events. JAMA 2006, 296, 2703–2711. [Google Scholar] [CrossRef] [Green Version]
- Sukhinina, T.S.; Shakhnovich, R.M.; Barsova, R.M.; Matveeva, N.A.; Titov, B.V.; Sudomoina, M.A.; Favorova, O.O.; Ruda, M.I. Value of allele gene polymorphism of the inflammation system for prognosis of patients with myocardial infarction. Kardiologiia 2012, 52, 15–21. [Google Scholar]
- Rizzello, V.; Liuzzo, G.; Giannuario, G.D.; Trabetti, E.; Brugaletta, S.; Santamaria, M.; Piro, M.; Pignatti, P.F.; Maseri, A.; Biasucci, L.M.; et al. 1059G/C polymorphism within the exon 2 of the C-reactive protein gene: Relationship to C-reactive protein levels and prognosis in unstable angina. Coron. Artery Dis. 2007, 18, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Miller, D.T.; Zee, R.Y.; Danik, S.J.; Kozlowski, P.; Chasman, D.I.; Lazarus, R.; Cook, N.R.; Ridker, P.M.; Kwiatkowski, D.J. Association of common CRP gene variants with CRP levels and cardiovascular events. Ann. Hum. Genet. 2005, 69 Pt 6, 623–638. [Google Scholar] [CrossRef]
- Zee, R.Y.; Hegener, H.H.; Fernandez-Cruz, A.; Lindpaintner, K. C-reactive protein gene polymorphisms and the incidence of post-angioplasty restenosis. Atherosclerosis 2004, 176, 393–396. [Google Scholar] [CrossRef] [PubMed]
- Reichert, S.; Schlitt, A.; Beschow, V.; Lutze, A.; Lischewski, S.; Seifert, T.; Dudakliewa, T.; Gawe, R.; Werdan, K.; Hofmann, B.; et al. Use of floss/interdental brushes is associated with lower risk for new cardiovascular events among patients with coronary heart disease. J. Periodontal. Res. 2015, 50, 180–188. [Google Scholar] [CrossRef] [PubMed]
- Ruiz-Ramie, J.J.; Barber, J.L.; Lloyd-Jones, D.M.; Gross, M.D.; Rana, J.S.; Sidney, S.; Jacobs, D.R.; Lane-Cordova, A.D.; Sarzynski, M.A. Cardiovascular Health Trajectories and Elevated C-Reactive Protein: The CARDIA Study. J. Am. Heart Assoc. 2021, 10, e019725. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M. High-sensitivity C-reactive protein and cardiovascular risk: Rationale for screening and primary prevention. Am. J. Cardiol. 2003, 92, 17K–22K. [Google Scholar] [CrossRef] [PubMed]
- Ndrepepa, G.; Braun, S.; Tada, T.; King, L.; Cassese, S.; Fusaro, M.; Keta, D.; Kastrati, A.; Schmidt, R. Comparative prognostic value of C-reactive protein & fibrinogen in patients with coronary artery disease. Indian J. Med. Res. 2014, 140, 392–400. [Google Scholar]
- Sinning, J.M.; Bickel, C.; Messow, C.M.; Schnabel, R.; Lubos, E.; Rupprecht, H.J.; Espinola-Klein, C.; Lackner, K.J.; Tiret, L.; Münzel, T.; et al. Impact of C-reactive protein and fibrinogen on cardiovascular prognosis in patients with stable angina pectoris: The AtheroGene study. Eur. Heart J. 2006, 27, 2962–2968. [Google Scholar] [CrossRef] [Green Version]
- Tzoulaki, I.; Murray, G.D.; Lee, A.J.; Rumley, A.; Lowe, G.D.; Fowkes, F.G. Relative value of inflammatory, hemostatic, and rheological factors for incident myocardial infarction and stroke: The Edinburgh Artery Study. Circulation 2007, 115, 2119–2127. [Google Scholar] [CrossRef] [Green Version]
- Yang, J.; Li, C.; Zheng, Y.; Gao, J.; Liu, Y.P.; Wang, J.J.; Song, J.J.; Zhou, Q.; Meng, X.; Zhang, K.; et al. The association between high-sensitivity C-reactive protein/albumin ratio and cardiovascular prognosis in patients undergoing percutaneous coronary intervention. Angiology 2022, 73, 818–826. [Google Scholar] [CrossRef]
- Yuan, D.; Wang, P.; Jia, S.; Zhang, C.; Zhu, P.; Jiang, L.; Liu, R.; Xu, J.; Tang, X.; Song, Y.; et al. Lipoprotein(a), high-sensitivity C-reactive protein, and cardiovascular risk in patients undergoing percutaneous coronary intervention. Atherosclerosis 2022, 363, 109–116. [Google Scholar] [CrossRef]
- Nimptsch, K.; Aleksandrova, K.; Boeing, H.; Janke, J.; Lee, Y.A.; Jenab, M.; Bueno-de-Mesquita, H.B.; Jansen, E.H.; Tsilidis, K.K.; Trichopoulou, A.; et al. Association of CRP genetic variants with blood concentrations of C-reactive protein and colorectal cancer risk. Int. J. Cancer 2015, 136, 1181–1192. [Google Scholar] [CrossRef] [Green Version]
- Nimptsch, K.; Aleksandrova, K.; Fedirko, V.; Jenab, M.; Gunter, M.J.; Siersema, P.D.; Wu, K.; Katzke, V.; Kaaks, R.; Panico, S.; et al. Pre-diagnostic C-reactive protein concentrations, CRP genetic variation and mortality among individuals with colorectal cancer in Western European populations. BMC Cancer 2022, 22, 695. [Google Scholar] [CrossRef]
- Si, S.; Li, J.; Tewara, M.A.; Xue, F. Genetically Determined Chronic Low-Grade Inflammation and Hundreds of Health Outcomes in the UK Biobank and the FinnGen Population: A Phenome-Wide Mendelian Randomization Study. Front. Immunol. 2021, 12, 720876. [Google Scholar] [CrossRef] [PubMed]
- Prasad, K. Current Status of Primary, Secondary, and Tertiary Prevention of Coronary Artery Disease. Int. J. Angiol. 2021, 30, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Lolley, R.; Forman, D.E. Cardiac Rehabilitation and Survival for Ischemic Heart Disease. Curr. Cardiol. Rep. 2021, 23, 184. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| SNP | Primer 3′–5′ | Restriction Enzyme |
|---|---|---|
| rs1130864 | Forward: cac gtc tct gtc tct ggt acct cc cgc | Mae II |
| Reverse: caa aac acct ca aat tct gat tct ttt gga ac | ||
| rs1417938 | Forward: acc ccc at acct cag atc gaa | Tfi I |
| Reverse: gac gtg acc atg gag aag ct | ||
| rs1800947 | Forward: cag ttt tac agt ggg tgg gtc | BsiHKAI |
| Reverse: ccc gcc agt tca gga cat tag | ||
| rs3093077 | Forward: caa aag tga ggc tgg gac ctg | Mnl I |
| Reverse: gac agg gag ctg aa gaga agg |
| Characteristics | All Patients (n = 792) | Without Combined Endpoint (n = 453) | With Combined Endpoint (n = 339) | p-Value |
|---|---|---|---|---|
| Demographic and anamnestic parameters | ||||
| Age, years (median; 25/75 IQR) | 69.2 (60.7/74.8) | 68.2 (59.3/72.9) | 70.9 (62.7/77.4) | <0.001 |
| Female gender (%) | 26.5 | 28.7 | 23.6 | 0.127 * |
| Current smoking (%) | 10.4 | 11.5 | 8.8 | 0.278 * |
| Body mass index, kg/m2 (median; 25/75 IQR) | 28.1 (25.3/30.7) | 28.1 (25.3/30.9) | 28.2 (25.4/30.7) | 0.691 |
| History of | ||||
| Diabetes mellitus (%) | 35.6 | 29.4 | 44.0 | <0.001 * |
| Hypertension (%) | 87.6 | 86.1 | 89.7 | 0.160 * |
| MI (%) | 39.3 | 32.5 | 48.4 | <0.001 * |
| Stroke/TIA (%) | 12.2 | 9.7 | 15.6 | 0.016 * |
| Peripheral artery disease (%) | 10.2 | 7.3 | 14.2 | 0.002 * |
| Hyperlipoproteinemia (%) | 59.0 | 59.2 | 58.7 | 0.955 * |
| Biochemical parameters (median; 25/75 IQR) | ||||
| C-reactive protein (mg/L), | 8.6 (3.6/32.8) | 6.2 (2.8/27.9) | 11.4 (5.0/39.0) | 0.001 |
| Leukocytes (Gpt/L), | 7.8 (6.4/9.6) | 7.8 (6.4/9.8) | 7.7 (6.2/9.5) | 0.397 |
| Interleukin 6 (pg/mL), | 7.8 (3.8/15.9) | 7.2 (3.4/13.9) | 8.7 (4.3/18.5) | 0.017 |
| Uric acid (µmol/L) | 5.7 (4.3/7.9) | 5.4 (4.3/6.8) | 6.3 (4.5/9.4) | <0.001 |
| Creatinine (mmol/L), | 87 (73/109) | 83 (71/97) | 97 (78/130) | <0.001 |
| Total cholesterol (mmol/L), | 4.3 (3.7/6.3) | 4.4 (3.8/5.3) | 4.2 (3.5/5.2) | 0.030 |
| HDL cholesterol (mmol/L), | 1.0 (0.8/1.2) | 1.0 (0.8/1.3) | 0.9 (0.8/1.2) | 0.002 |
| LDL cholesterol (mmol/L), | 2.5 (2.0/3.3) | 2.6 (2.1/3.3) | 2.5 (2.0/3.2) | 0.055 |
| Triglycerides (mmol/L), | 1.4 (1.0/1.9) | 1.4 (0.9/1.8) | 1.3 (1.0/1.9) | 0.394 |
| Regression Coefficient | Standard Error | p-Value | Hazard Ratio | 95% CI | ||
|---|---|---|---|---|---|---|
| Upper | Lower | |||||
| CRP level ≥5 mg/L | 0.397 | 0.129 | 0.002 | 1.49 | 1.16 | 1.91 |
| Age | 0.041 | 0.007 | <0.001 | 1.04 | 1.03 | 1.06 |
| Male gender | 0.325 | 0.130 | 0.012 | 1.38 | 1.07 | 1.78 |
| BMI | −0.008 | 0.014 | 0.534 | 0.99 | 0.97 | 1.02 |
| smoking | 0.317 | 0.209 | 0.128 | 1.37 | 0.91 | 2.07 |
| Diabetes mellitus | 0.540 | 0.118 | <0.001 | 1.72 | 1.36 | 2.16 |
| Hypertension | 0.135 | 0.186 | 0.466 | 1.14 | 0.80 | 1.65 |
| Hyperlipoproteinemia | −0.043 | 0.116 | 0.711 | 0.96 | 0.76 | 1.20 |
| SNPs in CRP Gene | All Patients (n = 792) | Without Combined Endpoint (n = 453) | With Combined Endpoint (n = 339) | p-Value |
|---|---|---|---|---|
| rs1130864 | ||||
| CC genotype | 44.4 | 47.2 | 40.6 | |
| CT + TT genotype | 55.6 | 52.8 | 59.4 | 0.089 * |
| rs1417938 | ||||
| TT genotype | 43.4 | 45.8 | 40.3 | |
| AA + AT genotype | 56.6 | 54.2 | 59.7 | 0.162 * |
| rs1800947 | ||||
| GG genotype | 86.5 | 85.4 | 87.9 | |
| CG + CC genotype | 13.5 | 14.6 | 12.1 | 0.370 * |
| rs3093077 | ||||
| TT genotype | 87.7 | 88.3 | 87.0 | |
| GG + GT genotype | 12.3 | 11.7 | 13.0 | 0.681 * |
| Regression Coefficient | Standard Error | p-Value | Hazard Ratio | 95% CI | ||
|---|---|---|---|---|---|---|
| Upper | Lower | |||||
| CT + TT genotype | 0.188 | 0.116 | 0.103 | 1.21 | 0.96 | 1.51 |
| Age | 0.042 | 0.007 | <0.001 | 1.04 | 1.03 | 1.06 |
| Male gender | 0.320 | 0.134 | 0.017 | 1.38 | 1.06 | 1.79 |
| BMI | −0.007 | 0.014 | 0.062 | 0.99 | 0.97 | 1.02 |
| Smoking | 0.344 | 0.218 | 0.115 | 1.41 | 0.92 | 2.16 |
| Diabetes mellitus | 0.546 | 0.122 | <0.001 | 1.73 | 1.36 | 2.19 |
| Hypertension | 0.102 | 0.192 | 0.597 | 1.11 | 0.76 | 1.61 |
| Hyperlipoproteinemia | −0.114 | 0.119 | 0.339 | 0.89 | 0.71 | 1.13 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schulz, S.; Rehm, S.; Schlitt, A.; Lierath, M.; Lüdike, H.; Hofmann, B.; Bitter, K.; Reichert, S. C-Reactive Protein Level and the Genetic Variant rs1130864 in the CRP Gene as Prognostic Factors for 10-Year Cardiovascular Outcome. Cells 2023, 12, 1775. https://doi.org/10.3390/cells12131775
Schulz S, Rehm S, Schlitt A, Lierath M, Lüdike H, Hofmann B, Bitter K, Reichert S. C-Reactive Protein Level and the Genetic Variant rs1130864 in the CRP Gene as Prognostic Factors for 10-Year Cardiovascular Outcome. Cells. 2023; 12(13):1775. https://doi.org/10.3390/cells12131775
Chicago/Turabian StyleSchulz, Susanne, Selina Rehm, Axel Schlitt, Madlen Lierath, Henriette Lüdike, Britt Hofmann, Kerstin Bitter, and Stefan Reichert. 2023. "C-Reactive Protein Level and the Genetic Variant rs1130864 in the CRP Gene as Prognostic Factors for 10-Year Cardiovascular Outcome" Cells 12, no. 13: 1775. https://doi.org/10.3390/cells12131775