

XPF–ERCC1 Blocker Improves the Therapeutic Efficacy of 5-FU- and Oxaliplatin-Based Chemoradiotherapy in Colorectal Cancer
 , , , ,
, , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Cells Lines and Mice
2.2. ERCC1 shRNA, XPF–ERCC1 Blocker (NSC130813), Chemotherapeutic Drug Treatment, Cell Viability Assay
2.3. Irradiation Expose and Colony Formation Assay
2.4. Western Blotting
2.5. Immunofluorescence Staining
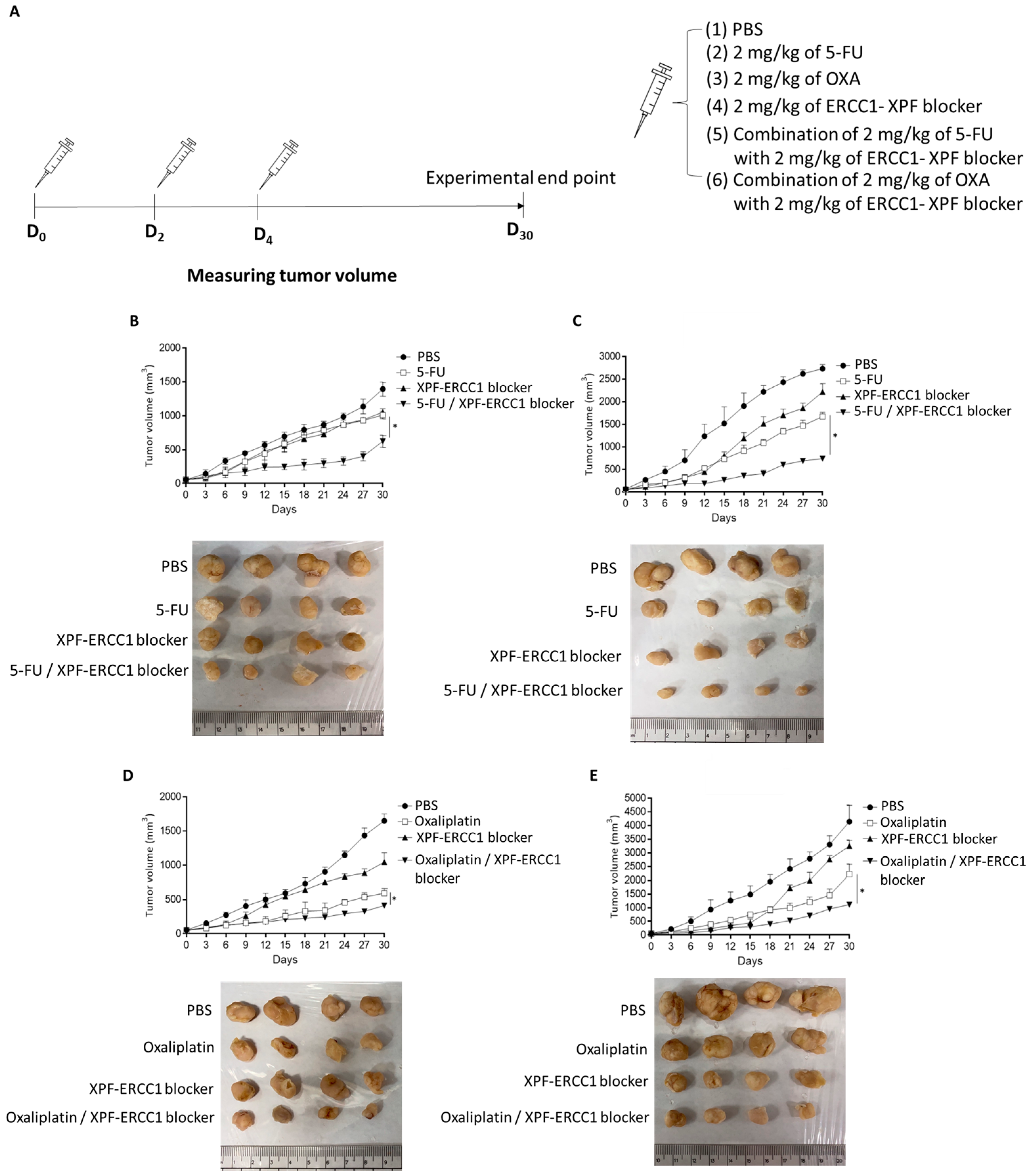
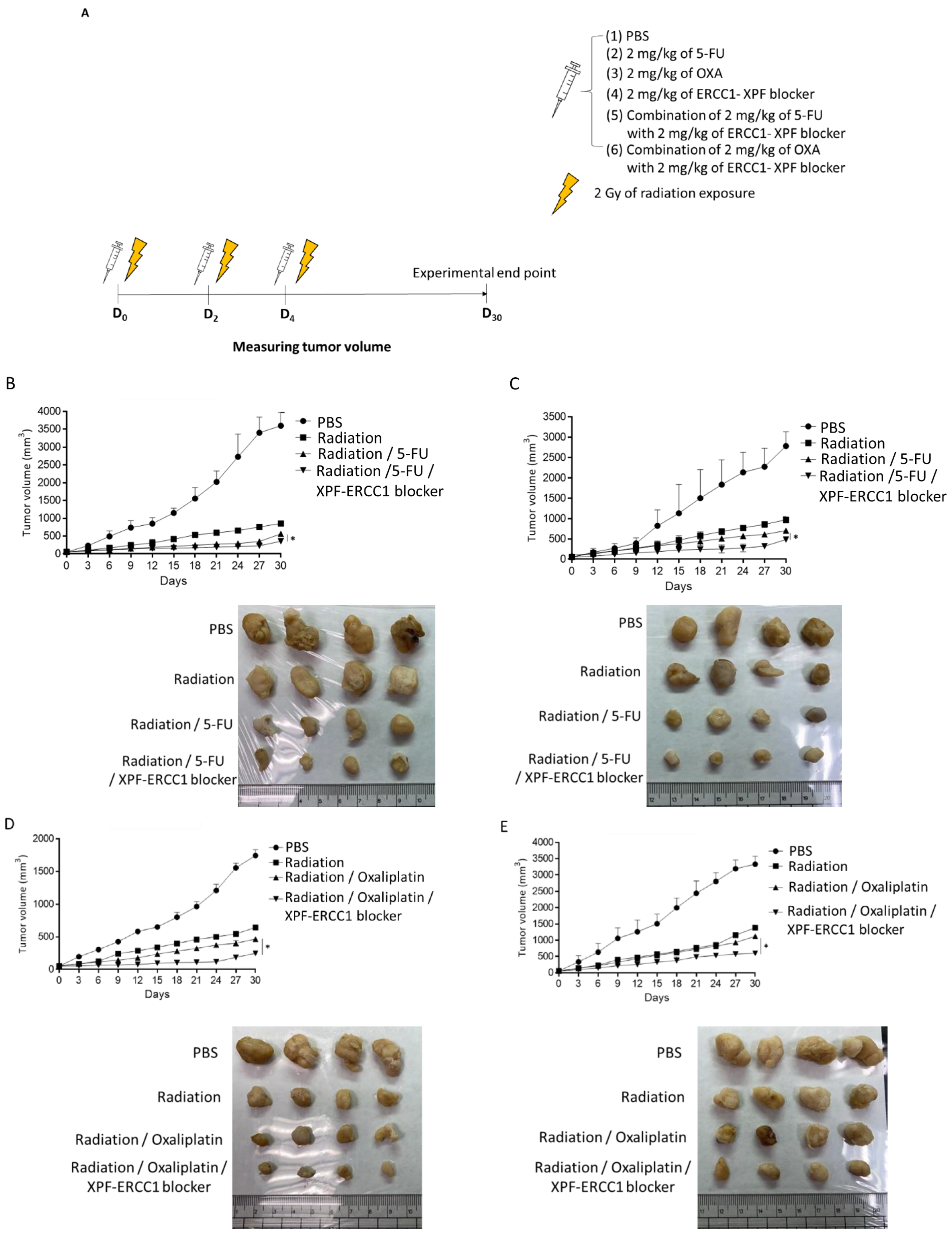
2.6. Xenograft Animal Model, Chemotherapy Treatment Schedule and Chemoradiotherapy Treatment Schedule
2.7. Immunohistochemical Staining and Tunel Assay
2.8. Statistical Analysis
3. Results
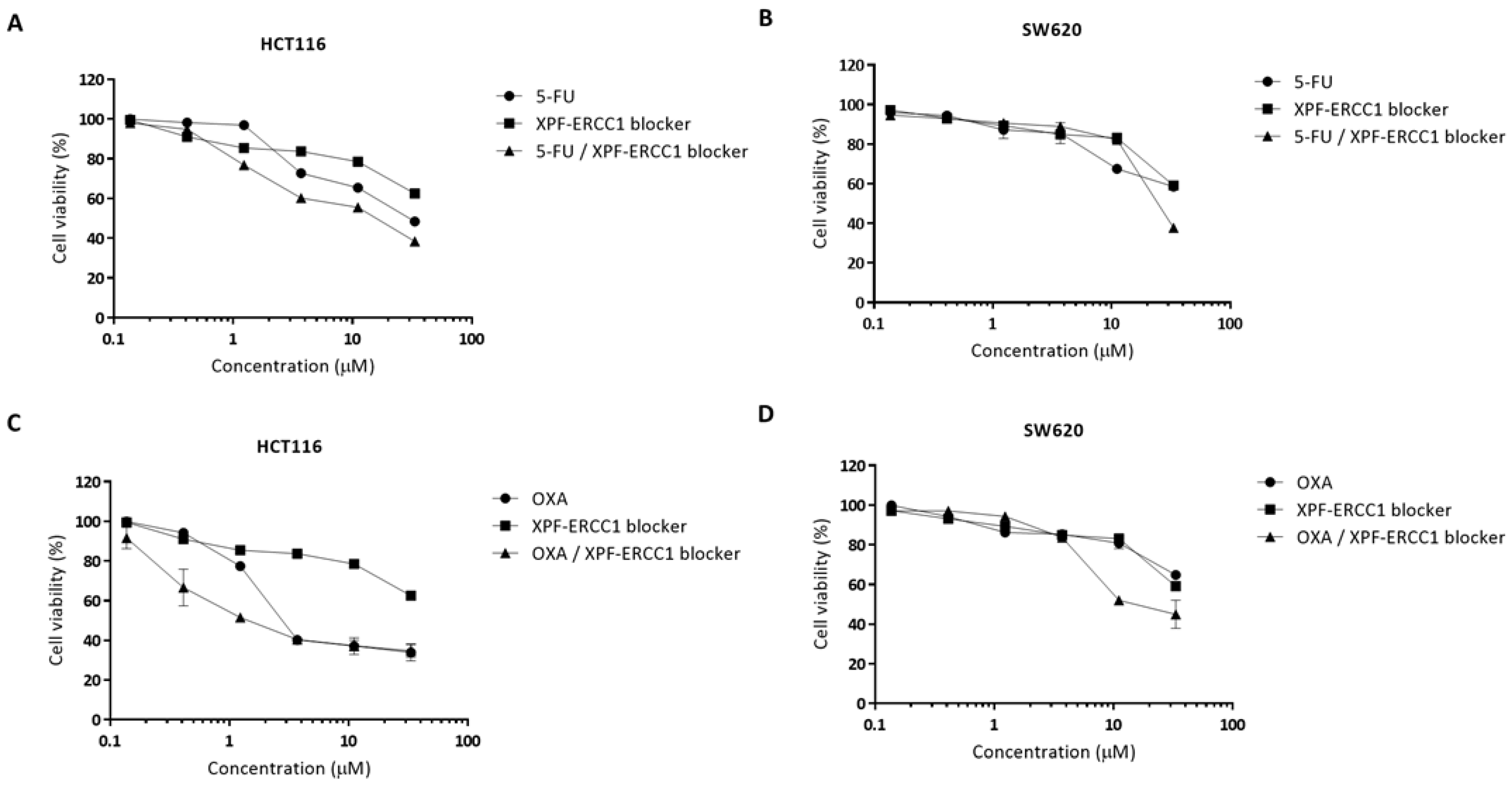
3.1. XPF–ERCC1 Blockers Synergistically Enhance the Cytotoxicity of 5-FU or Oxaliplatin in Colorectal Cells
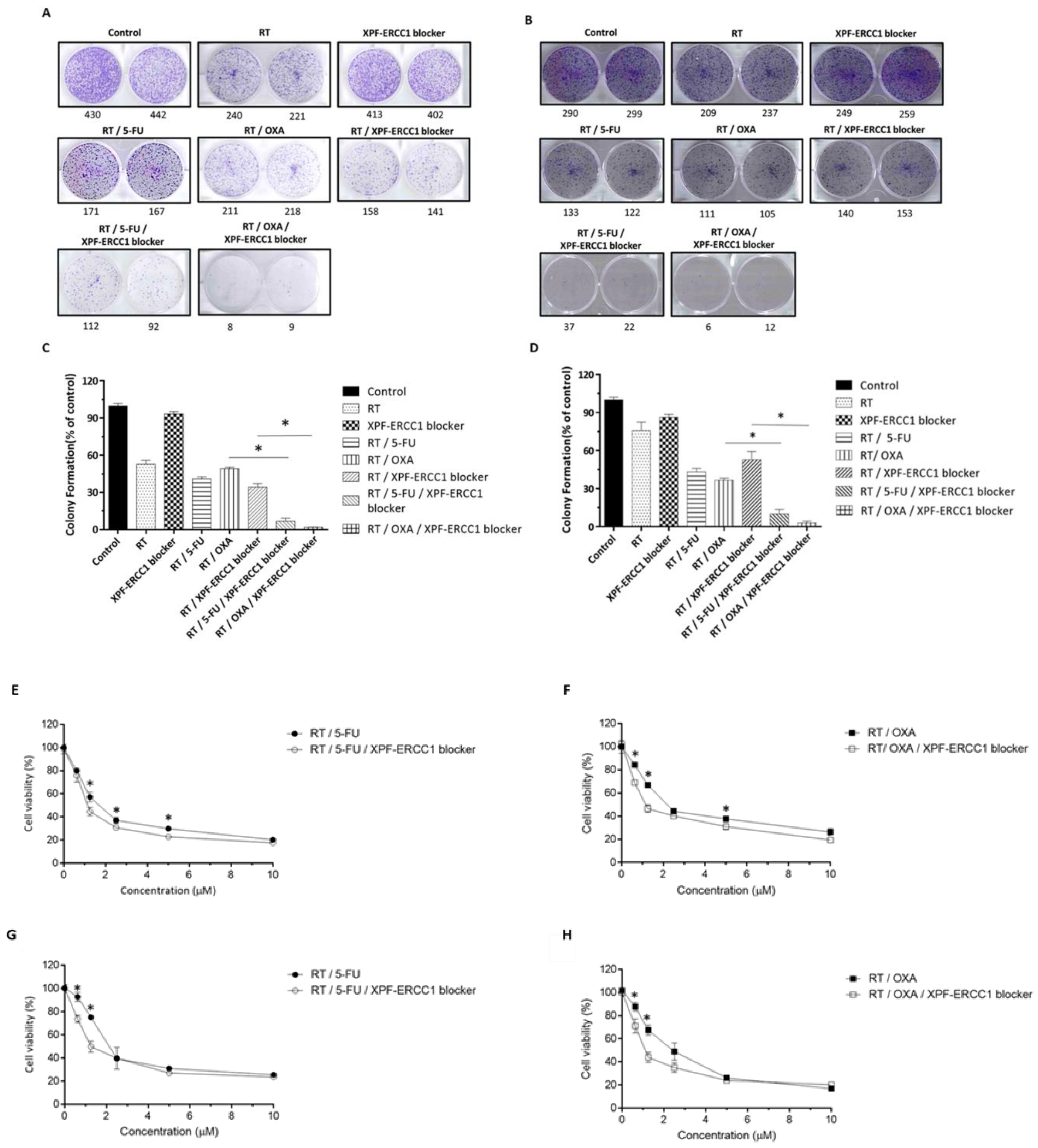
3.2. XPF–ERCC1 Blocker Increases the Efficacy of 5-FU-Based CRT and OXA-Based CRT In Vitro
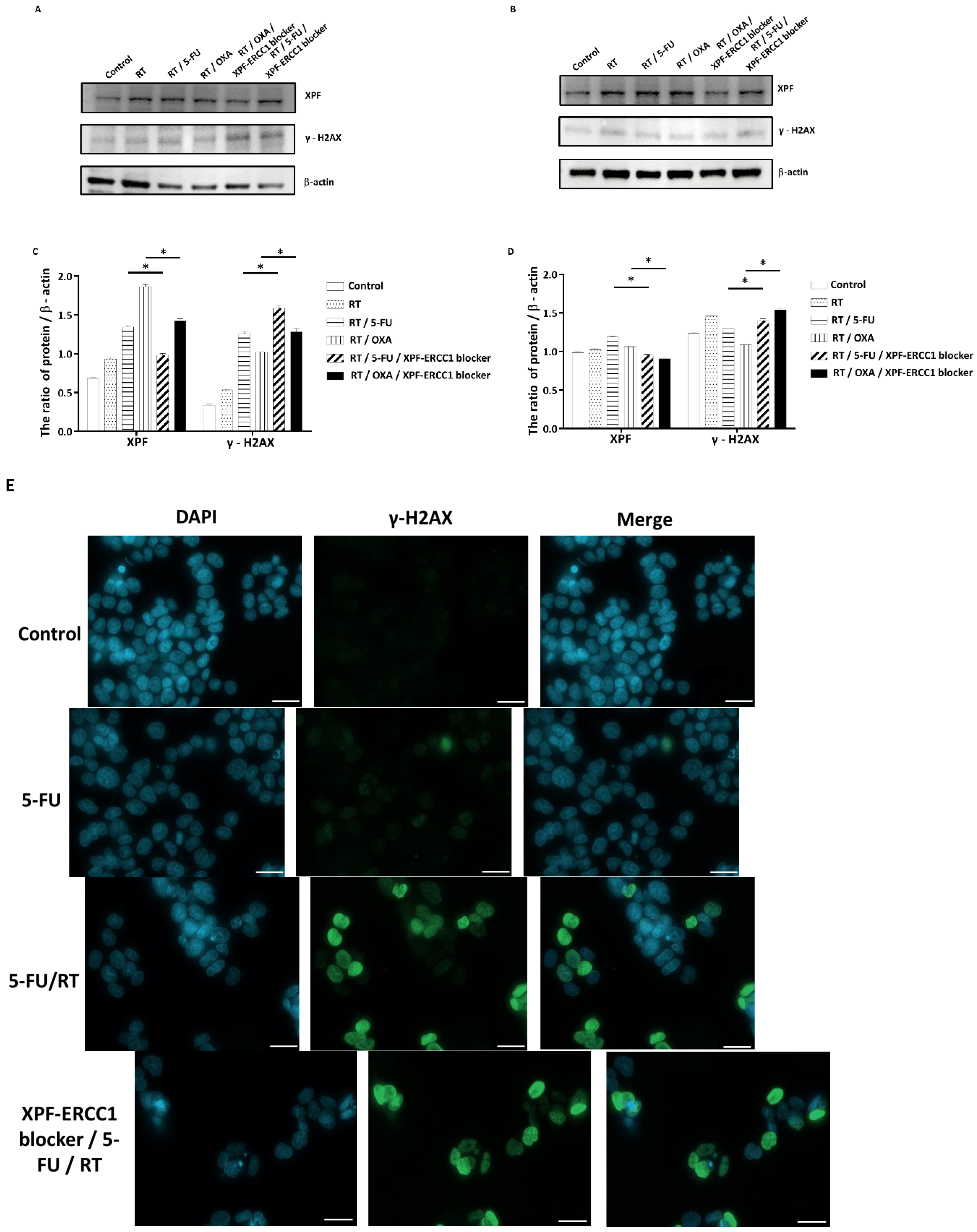
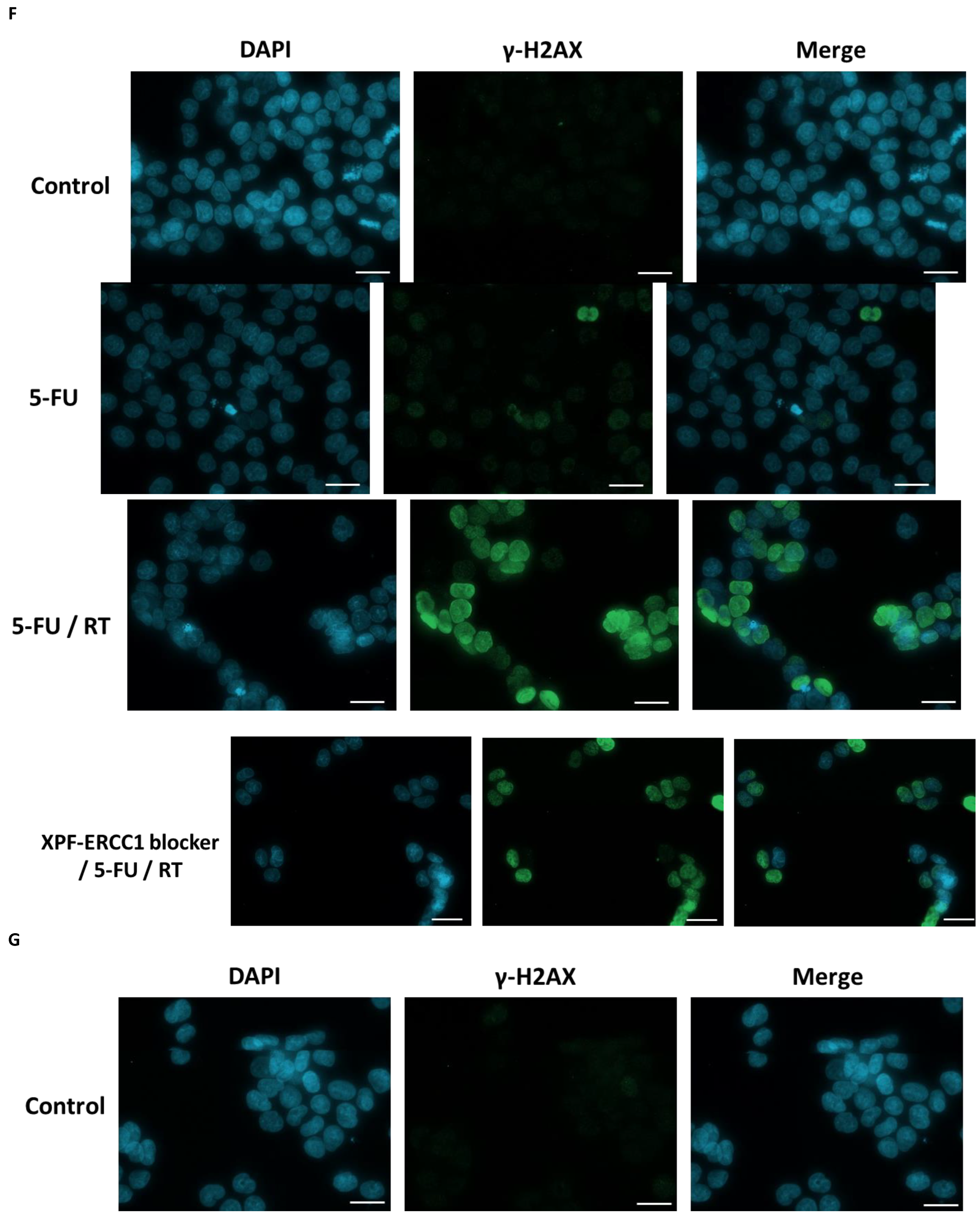
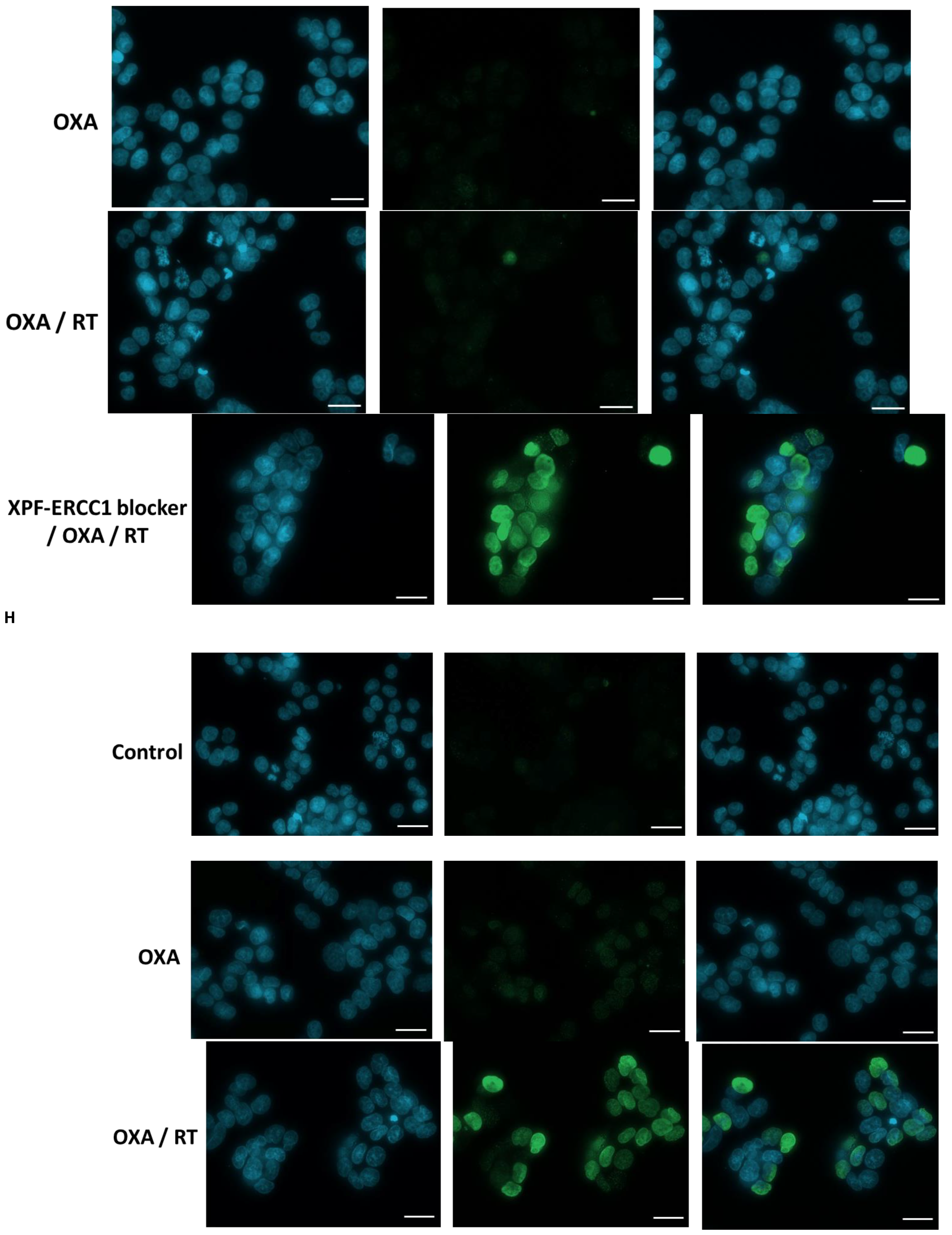
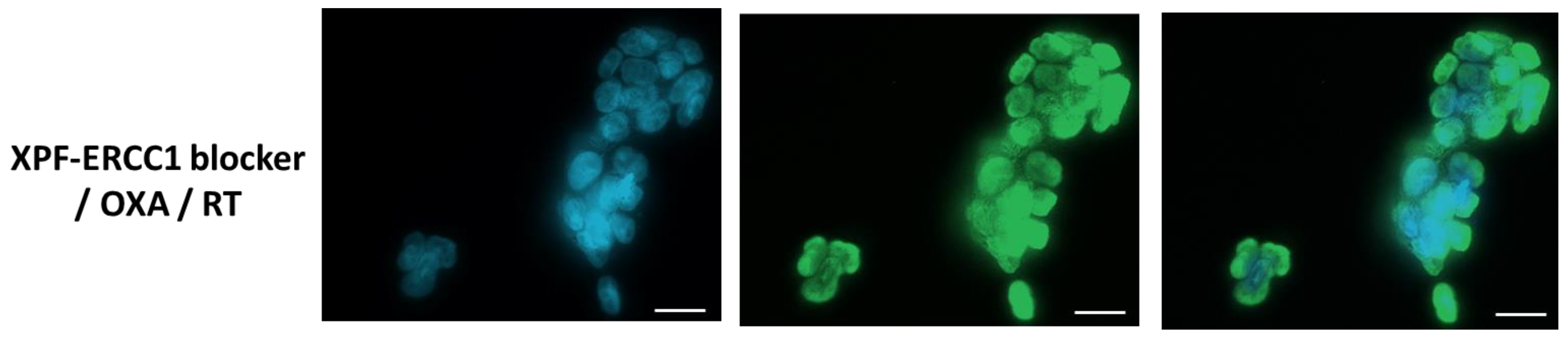
3.3. Inhibition of DNA Repair by XPF–ERCC1 Blocker Leads to Radio-Chemosensitization
3.4. XPF–ERCC1 Blocker Increases Chemotherapeutic Efficacy In Vivo
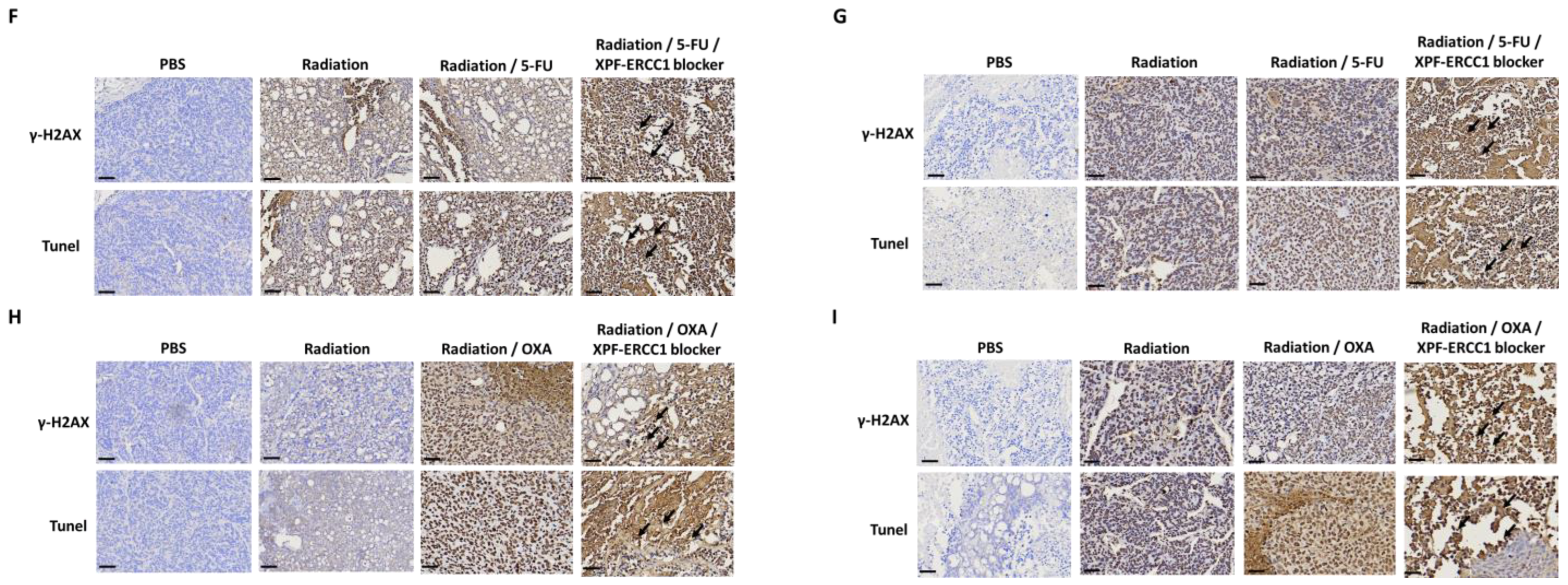
3.5. XPF–ERCC1 Blocker Increases the Efficacy of Combined Radiochemotherapy In Vivo
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kao, P.-S.; Chang, S.-C.; Wang, L.-W.; Lee, R.-C.; Liang, W.-Y.; Lin, T.-C.; Chen, W.-S.; Jiang, J.-K.; Yang, S.-H.; Wang, H.-S.; et al. The impact of preoperative chemoradiotherapy on advanced low rectal cancer. J. Surg. Oncol. 2010, 102, 771–777. [Google Scholar] [CrossRef]
- Zha, L.T.; Zheng, Q.; Li, L. Whether Patients with Stage/Colorectal Cancer Benefit from Adjuvant Chemotherapy: A Modeling Analysis of Literature Aggregate Data. Front. Pharm. 2022, 13, 826785. [Google Scholar] [CrossRef]
- Feeney, G.; Sehgal, R.; Sheehan, M.; Hogan, A.; Regan, M.; Joyce, M.; Kerin, M. Neoadjuvant radiotherapy for rectal cancer management. World J. Gastroenterol. 2019, 25, 4850–4869. [Google Scholar] [CrossRef]
- Papaccio, F.; Rosello, S.; Huerta, M.; Gambardella, V.; Tarazona, N.; Fleitas, T.; Roda, D.; Cervantes, A. Neoadjuvant Chemotherapy in Locally Advanced Rectal Cancer. Cancers 2020, 12, 3611. [Google Scholar] [CrossRef] [PubMed]
- Bahadoer, R.R.; Dijkstra, E.A.; van Etten, B.; Marijnen, C.A.M.; Putter, H.; Kranenbarg, E.M.; Roodvoets, A.G.H.; Nagtegaal, I.D.; Beets-Tan, R.G.H.; Blomqvist, L.K.; et al. investigators. Short-course radiotherapy followed by chemotherapy before total mesorectal excision (TME) versus preoperative chemoradiotherapy, TME, and optional adjuvant chemotherapy in locally advanced rectal cancer (RAPIDO): A randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 29–42. [Google Scholar]
- Conroy, T.; Bosset, J.F.; Etienne, P.L.; Rio, E.; Francois, E.; Mesgouez-Nebout, N.; Vendrely, V.; Artignan, X.; Bouche, O.; Gargot, D.; et al. Neoadjuvant chemotherapy with FOLFIRINOX and preoperative chemoradiotherapy for patients with locally advanced rectal cancer (UNICANCER-PRODIGE 23): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2021, 22, 702–715. [Google Scholar] [CrossRef]
- Rosello, S.; Papaccio, F.; Roda, D.; Tarazona, N.; Cervantes, A. The role of chemotherapy in localized and locally advanced rectal cancer: A systematic revision. Cancer Treat. Rev. 2018, 63, 156–171. [Google Scholar] [CrossRef]
- Huang, M.Y.; Huang, J.J.; Huang, C.M.; Lin, C.H.; Tsai, H.L.; Huang, C.W.; Chai, C.Y.; Lin, C.Y.; Wang, J.Y. Relationship Between Expression of Proteins ERCC1, ERCC2, and XRCC1 and Clinical Outcomes in Patients with Colorectal Cancer Treated with FOLFOX-Based Preoperative Chemoradiotherapy. World J. Surg. 2017, 41, 2884–2897. [Google Scholar] [CrossRef]
- Vaezi, A.; Feldman, C.H.; Niedernhofer, L.J. ERCC1 and XRCC1 as biomarkers for lung and head and neck cancer. Pharmgenomics Pers. Med. 2011, 4, 47–63. [Google Scholar] [CrossRef]
- Mendoza, J.; Martínez, J.; Hernández, C.; Pérez-Montiel, D.; Castro, C.; Fabián-Morales, E.; Santibáñez, M.; González-Barrios, R.; Díaz-Chávez, J.; Andonegui, M.A.; et al. Association between ERCC1 and XPA expression and polymorphisms and the response to cisplatin in testicular germ cell tumours. Br. J. Cancer 2013, 109, 68–75. [Google Scholar] [CrossRef]
- Hubner, R.A.; Riley, R.D.; Billingham, L.J.; Popat, S. Excision repair cross-complementation group 1 (ERCC1) status and lung cancer outcomes: A meta-analysis of published studies and recommendations. PLoS ONE 2011, 6, e25164. [Google Scholar] [CrossRef]
- Vilmar, A.; Sorensen, J.B. Excision repair cross-complementation group 1 (ERCC1) in platinum-based treatment of non-small cell lung cancer with special emphasis on carboplatin: A review of current literature. Lung Cancer 2009, 64, 131–139. [Google Scholar] [CrossRef]
- Li, W.; Jie, Z.; Li, Z.; Liu, Y.; Gan, Q.; Mao, Y.; Wang, X. ERCC1 siRNA ameliorates drug resistance to cisplatin in gastric carcinoma cell lines. Mol. Med. Rep. 2014, 9, 2423–2428. [Google Scholar] [CrossRef]
- Jun, H.J.; Ahn, M.J.; Kim, H.S.; Yi, S.Y.; Han, J.; Lee, S.K.; Ahn, Y.C.; Jeong, H.S.; Son, Y.I.; Baek, J.H. ERCC1 expression as a predictive marker of squamous cell carcinoma of the head and neck treated with cisplatin-based concurrent chemoradiation. Br. J. Cancer 2008, 99, 167–172. [Google Scholar] [CrossRef]
- Kim, M.K.; Cho, K.J.; Kwon, G.Y.; Park, S.I.; Kim, Y.H.; Kim, J.H.; Song, H.Y.; Shin, J.H.; Jung, H.Y.; Lee, G.H.; et al. ERCC1 predicting chemoradiation resistance and poor outcome in oesophageal cancer. Eur. J. Cancer 2008, 44, 54–60. [Google Scholar] [CrossRef]
- Huang, Y.J.; Huang, M.Y.; Cheng, T.L.; Kuo, S.H.; Ke, C.C.; Chen, Y.T.; Hsieh, Y.C.; Wang, J.Y.; Cheng, C.M.; Chuang, C.H. ERCC1 Overexpression Increases Radioresistance in Rectal Cancer Cells. Cancers 2022, 14, 4798. [Google Scholar] [CrossRef]
- Huang, Y.J.; Chen, Y.T.; Huang, C.M.; Kuo, S.H.; Liao, Y.Y.; Jhang, W.Y.; Wang, S.H.; Ke, C.C.; Huang, Y.H.; Cheng, C.M.; et al. HIF-1alpha Expression Increases Preoperative Concurrent Chemoradiotherapy Resistance in Hyperglycemic Colorectal Cancer. Cancers 2022, 14, 4053. [Google Scholar] [CrossRef]
- Elmenoufy, A.H.; Gentile, F.; Jay, D.; Karimi-Busheri, F.; Yang, X.; Soueidan, O.M.; Weilbeer, C.; Mani, R.S.; Barakat, K.H.; Tuszynski, J.A.; et al. Targeting DNA Repair in Tumor Cells via Inhibition of ERCC1-XPF. J. Med. Chem. 2019, 62, 7684–7696. [Google Scholar] [CrossRef]
- Jordheim, L.P.; Barakat, K.H.; Heinrich-Balard, L.; Matera, E.L.; Cros-Perrial, E.; Bouledrak, K.; El Sabeh, R.; Perez-Pineiro, R.; Wishart, D.S.; Cohen, R.; et al. Small molecule inhibitors of ERCC1-XPF protein-protein interaction synergize alkylating agents in cancer cells. Mol. Pharm. 2013, 84, 12–24. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, L.; Mao, P.; Jiang, G.; Liu, L.; Wang, J.; Yang, W.; Owusu, L.; Li, W. Functional characterization of a novel transcript of ERCC1 in chemotherapy resistance of ovarian cancer. Oncotarget 2017, 8, 85759–85771. [Google Scholar] [CrossRef]
- Anuja, K.; Chowdhury, A.R.; Saha, A.; Roy, S.; Rath, A.K.; Kar, M.; Banerjee, B. Radiation-induced DNA damage response and resistance in colorectal cancer stem-like cells. Int. J. Radiat. Biol. 2019, 95, 667–679. [Google Scholar] [CrossRef]
- Manzari, M.T.; Shamay, Y.; Kiguchi, H.; Rosen, N.; Scaltriti, M.; Heller, D.A. Targeted drug delivery strategies for precision medicines. Nat. Rev. Mater. 2021, 6, 351–370. [Google Scholar] [CrossRef]
- McNeil, E.M.; Melton, D.W. DNA repair endonuclease ERCC1-XPF as a novel therapeutic target to overcome chemoresistance in cancer therapy. Nucleic Acids Res. 2012, 40, 9990–10004. [Google Scholar] [CrossRef]
- McNeil, E.M.; Astell, K.R.; Ritchie, A.M.; Shave, S.; Houston, D.R.; Bakrania, P.; Jones, H.M.; Khurana, P.; Wallace, C.; Chapman, T.; et al. Inhibition of the ERCC1-XPF structure-specific endonuclease to overcome cancer chemoresistance. DNA Repair. 2015, 31, 19–28. [Google Scholar] [CrossRef]
- Kirschner, K.; Melton, D.W. Multiple roles of the ERCC1-XPF endonuclease in DNA repair and resistance to anticancer drugs. Anticancer. Res. 2010, 30, 3223–3232. [Google Scholar]
- Faridounnia, M.; Folkers, G.E.; Boelens, R. Function and Interactions of ERCC1-XPF in DNA Damage Response. Molecules 2018, 23, 3205. [Google Scholar] [CrossRef]
- Ferry, K.V.; Hamilton, T.C.; Johnson, S.W. Increased nucleotide excision repair in cisplatin-resistant ovarian cancer cells: Role of ERCC1-XPF. Biochem. Pharm. 2000, 60, 1305–1313. [Google Scholar] [CrossRef]
- Rosell, R.; Taron, M.; Barnadas, A.; Scagliotti, G.; Sarries, C.; Roig, B. Nucleotide excision repair pathways involved in Cisplatin resistance in non-small-cell lung cancer. Cancer Control. 2003, 10, 297–305. [Google Scholar] [CrossRef]
- Blondy, S.; David, V.; Verdier, M.; Mathonnet, M.; Perraud, A.; Christou, N. 5-Fluorouracil resistance mechanisms in colorectal cancer: From classical pathways to promising processes. Cancer Sci. 2020, 111, 3142–3154. [Google Scholar] [CrossRef]
- Wang, T.; Wang, L.; Qian, X.; Yu, L.; Ding, Y.; Liu, B. Relationship between gene expression of 5-fluorouracil metabolic enzymes and 5-fluorouracil sensitivity in primary cancer cells isolated from malignant ascites. Cancer Invest. 2011, 29, 130–136. [Google Scholar] [CrossRef]
- Douillard, J.Y.; Cunningham, D.; Roth, A.D.; Navarro, M.; James, R.D.; Karasek, P.; Jandik, P.; Iveson, T.; Carmichael, J.; Alakl, M.; et al. Irinotecan combined with fluorouracil compared with fluorouracil alone as first-line treatment for metastatic colorectal cancer: A multicentre randomised trial. Lancet 2000, 355, 1041–1047. [Google Scholar] [CrossRef]
- Johnston, P.G.; Kaye, S. Capecitabine: A novel agent for the treatment of solid tumors. Anticancer. Drugs 2001, 12, 639–646. [Google Scholar] [CrossRef]
- Blagosklonny, M.V. Analysis of FDA approved anticancer drugs reveals the future of cancer therapy. Cell Cycle 2004, 3, 1035–1042. [Google Scholar] [CrossRef]
- Wiseman, L.R.; Adkins, J.C.; Plosker, G.L.; Goa, K.L. Oxaliplatin: A review of its use in the management of metastatic colorectal cancer. Drugs Aging 1999, 14, 459–475. [Google Scholar] [CrossRef]
- Culy, C.R.; Clemett, D.; Wiseman, L.R. Oxaliplatin. A review of its pharmacological properties and clinical efficacy in metastatic rectal cancer and its potential in other malignancies. Drugs 2000, 60, 895–924. [Google Scholar] [CrossRef]
- Simpson, D.; Dunn, C.; Curran, M.; Goa, K.L. Oxaliplatin: A review of its use in combination therapy for advanced metastatic rectal cancer. Drugs 2003, 63, 2127–2156. [Google Scholar] [CrossRef]
- Jia, Y.; Sun, S.; Gao, X.; Cui, X. Expression levels of TUBB3, ERCC1 and P-gp in ovarian cancer tissues and adjacent normal tissues and their clinical significance. J. BUON 2018, 23, 1390–1395. [Google Scholar]
- Wang, S.; Liu, F.; Zhu, J.; Chen, P.; Liu, H.; Liu, Q.; Han, J. DNA Repair Genes ERCC1 and BRCA1 Expression in Non-Small Cell Lung Cancer Chemotherapy Drug Resistance. Med. Sci. Monit. 2016, 22, 1999–2005. [Google Scholar] [CrossRef]
- Hu, Q.; Li, H.; Wang, L.; Gu, H.; Fan, C. DNA Nanotechnology-Enabled Drug Delivery Systems. Chem. Rev. 2019, 119, 6459–6506. [Google Scholar] [CrossRef]









Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, M.-Y.; Huang, Y.-J.; Cheng, T.-L.; Jhang, W.-Y.; Ke, C.-C.; Chen, Y.-T.; Kuo, S.-H.; Lin, I.-L.; Huang, Y.-H.; Chuang, C.-H. XPF–ERCC1 Blocker Improves the Therapeutic Efficacy of 5-FU- and Oxaliplatin-Based Chemoradiotherapy in Colorectal Cancer. Cells 2023, 12, 1475. https://doi.org/10.3390/cells12111475
Huang M-Y, Huang Y-J, Cheng T-L, Jhang W-Y, Ke C-C, Chen Y-T, Kuo S-H, Lin I-L, Huang Y-H, Chuang C-H. XPF–ERCC1 Blocker Improves the Therapeutic Efficacy of 5-FU- and Oxaliplatin-Based Chemoradiotherapy in Colorectal Cancer. Cells. 2023; 12(11):1475. https://doi.org/10.3390/cells12111475
Chicago/Turabian StyleHuang, Ming-Yii, Yi-Jung Huang, Tian-Lu Cheng, Wun-Ya Jhang, Chien-Chih Ke, Yi-Ting Chen, Shih-Hsun Kuo, I-Ling Lin, Yu-Hsiang Huang, and Chih-Hung Chuang. 2023. "XPF–ERCC1 Blocker Improves the Therapeutic Efficacy of 5-FU- and Oxaliplatin-Based Chemoradiotherapy in Colorectal Cancer" Cells 12, no. 11: 1475. https://doi.org/10.3390/cells12111475